Article Text

Abstract
The COVID-19 pandemic will not be the last of its kind. As the world charts a way towards an equitable and resilient recovery, Public Health and Social Measures (PHSMs) that were implemented since the beginning of the pandemic need to be made a permanent feature of health systems that can be activated and readily deployed to tackle sudden surges in infections going forward. Although PHSMs aim to blunt the spread of the virus, and in turn protect lives and preserve health system capacity, there are also unintended consequences attributed to them. Importantly, the interactions between PHSMs and their accompanying key indicators that influence the strength and duration of PHSMs are elements that require in-depth exploration. This research employs case studies from six Asian countries, namely Indonesia, Singapore, South Korea, Thailand, the Philippines and Vietnam, to paint a comprehensive picture of PHSMs that protect the lives and livelihoods of populations. Nine typologies of PHSMs that emerged are as follows: (1) physical distancing, (2) border controls, (3) personal protective equipment requirements, (4) transmission monitoring, (5) surge health infrastructure capacity, (6) surge medical supplies, (7) surge human resources, (8) vaccine availability and roll-out and (9) social and economic support measures. The key indicators that influence the strength and duration of PHSMs are as follows: (1) size of community transmission, (2) number of severe cases and mortality, (3) health system capacity, (4) vaccine coverage, (5) fiscal space and (6) technology. Interactions between PHSMs can be synergistic or inhibiting, depending on various contextual factors. Fundamentally, PHSMs do not operate in silos, and a suite of PHSMs that are complementary is required to ensure that lives and livelihoods are safeguarded with an equity lens. For that to be achieved, strong governance structures and community engagement are also required at all levels of the health system.
- COVID-19
- Health policy
- Health systems
- Public Health
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The COVID-19 pandemic had driven countries to implement an array of Public Health and Social Measures (PHSMs), which aim to mitigate the spread of the virus and minimise economic fallout. Most modelling studies highlight the effectiveness of one PHSM as a standalone measure but do not emphasise the interplay between PHSMs and the key indicators that determine their overall effectiveness.
WHAT THIS STUDY ADDS
We have derived nine typologies of PHSMs and their accompanying six key indicators. The dynamic interplay between PHSMs and key indicators dictates the strength and duration of PHSMs.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
We found that for PHSMs be effective, national responses will need to place the most vulnerable first by centring PHSMs around an equity lens with strong governance and community engagement as key tenets at all levels of the health system.
As the world moves towards living with the virus endemically, coupled with waning vaccine immunities, newer variant strains and the reopening of economies, health systems need to be made resilient and nimble to readily redeploy PHSMs. Such policy actions will help curb any spike in infections in order to protect the lives and livelihoods of populations.
Introduction
COVID-19, caused by SARS-CoV-2, which first emerged in 2019, has thrown the world into turmoil. At the end of May 2022, there were approximately 6.2 million deaths and 520 million cases globally.1 However, WHO estimated 14.9 million excess deaths (directly and indirectly associated with COVID-19) in 2020 and 2021 globally.2 With the emergence of more transmissible variants such as Delta and Omicron and COVID-19 vaccine inequities across countries, the virus is forecasted to stay with newer strains expected to surface.3 As seen in most countries since the start of the pandemic, Public Health and Social Measures (PHSMs) were implemented at varying intensities and durations to interrupt community transmission and mitigate the unintended consequences that PHSMs brought to the population.4 5
PHSMs had become commonplace in peoples’ lives since 2020, with countries that took decisive action suffering from fewer cases and mortalities and a more contained economic decline.6 As the crisis persists, certain countries have tapered off PHSMs and resumed the economy, despite the emergence of more transmissible strains.7 In fact, countries that lifted PHSMs prematurely had experienced a swell in caseloads, overwhelming of health systems and unwarranted mortalities, while others have reinstated targeted lockdowns that hinder economic recovery.8 9 Notably, vulnerable groups suffer from greater mortality and morbidity. Coupled with the absence of adequate social support, the pandemic has widened social inequities and reversed the course of many social and health indicators.10
However, the goals of PHSMs remain to prevent infection, contain outbreaks and blunt peak epidemic size so that healthcare systems are not overwhelmed at every step of the pandemic trajectory.11 To achieve this, PHSMs need to be commensurate with the intensity of contagion transmission and PHSMs safely adapted to ensure feasibility, sustainability and congruence to the local context.12 In fact, simulation models have investigated the efficacy of some PHSMs over others, but more importantly, no standalone PHSM can function effectively, but a comprehensive set is needed to curb local transmission.13 Notably, health systems that are resilient and can effectively and equitably implement PHSMs are postulated to be better positioned to protect the health and livelihoods of the population.14 15
In the face of newly emerging strains, breakthrough infections and reinfections among third dose vaccinated individuals, waning of vaccine immunity and pressure to resume the economy, prospects of living with SARS-CoV-2 endemically will necessitate agile adaptations of PHSMs with concurrent strengthening of health systems.16 To our knowledge, however, there is a paucity of data on the interactions among different types of PHSMs and between PHSMs and their key indicators that influence the strength and duration of their deployment. Therefore, this study aims to address this gap by analysing PHSMs implemented in six Asian countries through an in-depth case study analysis and provide insights into their interactions with each other and how key indicators directly impact the stringency and effectiveness of PHSMs. This study also contributes to an evidence-informed framework related to the strategic application of PHSMs.
METHODS
Country selection criteria
This study focuses on six countries in Asia that introduced different levels of PHSMs at different stretches of the pandemic. Although this study has a Asian regional focus, the selected countries differed in terms of income status, level of devolution and centralisation of governance, population density, mortality rates from COVID-19, health systems attributes, Universal Health Coverage Service Coverage Index and Global Health Security Index which give us a comprehensive picture of how PHSMs evolved and impacted national responses in a variety of six Asian countries. Table 1 provides a backdrop of country profiles, including key country indicators.
Summary of key characteristics of six Asian countries
Literature search and case studies
The team of researchers from the six countries performed desk reviews of literatures relevant to PHSMs applied by their home countries. To that end, we used the literature review methodology set by Webster and Watson by harnessing scientific online data bases such as PubMed, EMBASE and Scopus as a starting point.17 Keywords during the initial search included ‘national responses to COVID-19’, ‘Public Health Measures’, ‘Social Support Measures’ and names of individual countries. We also performed a deeper dive into each PHSMs by repeating certain searches with the relevant PHSMs that we have identified after the initial thematic analysis. After the relevant articles have been sieved out, we selectively performed a backwards review of the pertinent citations from the articles to help address any missing data which we thought were applicable to our area of research.17 We also performed searches for national health accounts, government reports and policy executive summaries on the topic through digital government domains, mainly from ministries of health websites. To plug any remaining gaps, we performed a search of university databases where permitted, the websites of international development organisations and traditional and non-traditional media outlets (primarily through Google search). This provided us with a relatively complete census of the relevant literature made publicly available on PHSMs in the six countries. Data extracted in the local languages and English were included. Snapshots of the key PHSMs implemented from 2020 to 2022 are summarised in the results section and detailed in tables 2–10.
Snapshot of physical distancing measures implemented in six Asian countries
Snapshot of border control measures implemented in six Asian countries
Snapshot of personal protective equipment requirements implemented in six Asian countries
Snapshot of transmission monitoring measures implemented in six Asian countries
Snapshot of surging health infrastructure capacity measures implemented in six Asian countries
Snapshot of surging health supply measures implemented in six Asian countries
Snapshot of surging human resource capacity measures implemented in six Asian countries
Snapshot of vaccine availability and roll-out implemented in six Asian countries
Snapshot of social and economic support measures implemented in six Asian countries
Data analysis and presentation
The research team extracted key themes from the literature obtained from countries by performing an inductive thematic analysis whereby theoretical insights are generated from data,18 and thereafter drew comparisons across case studies which include all salient themes as typologies of PHSMs.19 Multiple rounds of iterative feedback between team members were performed to ensure the typologies correctly represented the themes that surfaced from the data to ensure reliability and accuracy. Any disagreement was resolved through discussions till a consensus was reached. Thematic saturation was reached when no new themes emerged.
Results
The inductive thematic analysis applied by this study emerged nine PHSM typologies, which include (1) physical distancing, (2) border controls, (3) personal protective equipment (PPE) requirements, (4) transmission monitoring, (5) surge health infrastructure capacity, (6) surge medical supplies, (7) surge human resources, (8) vaccine availability and roll-out and (9) social and economic support measures. We analysed how these nine PHSMs interacted among themselves.
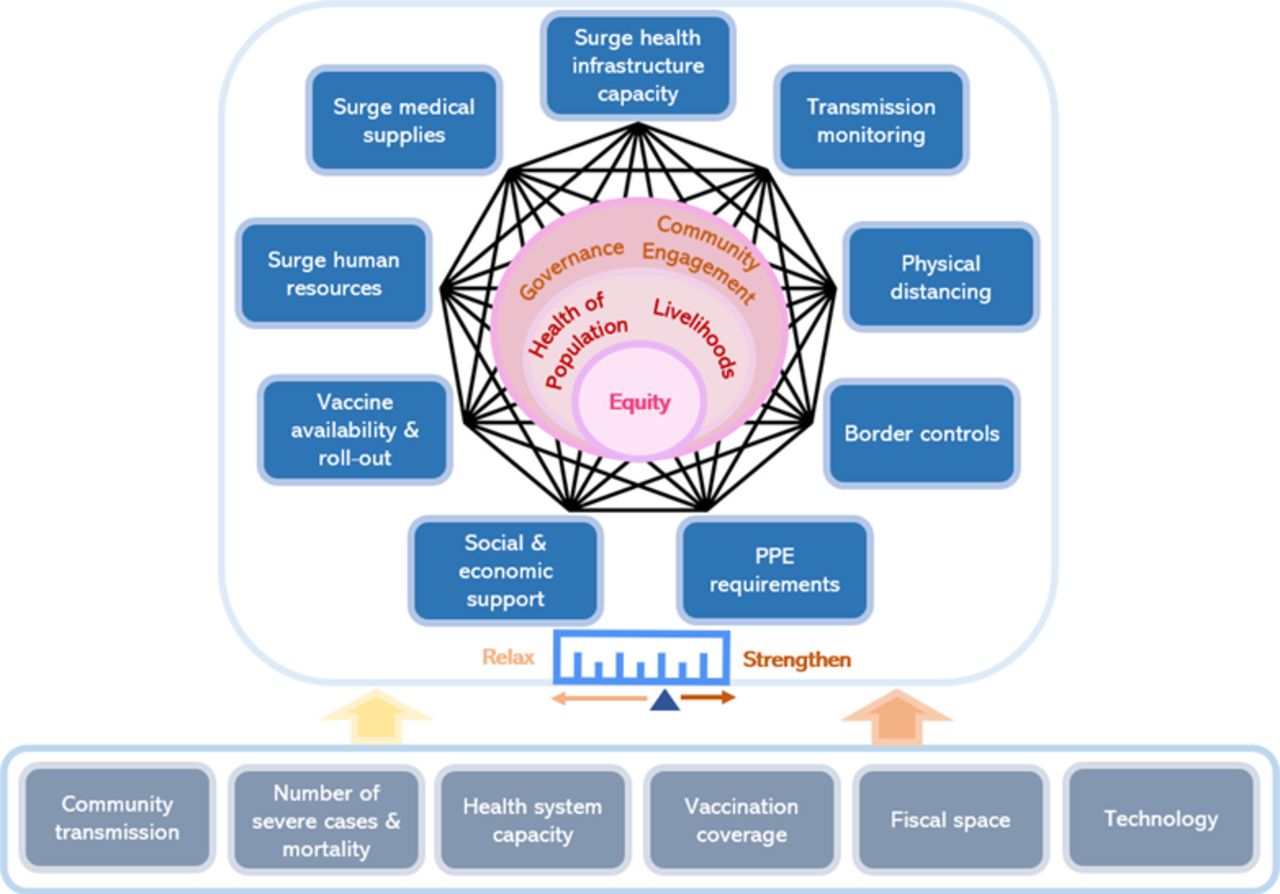
In addition, we identified six key indicators influencing the scaling up or down of PHSMs, including (1) size of community transmission, (2) number of severe cases and mortality, (3) health system capacity, (4) vaccine coverage, (5) fiscal space and (6) technology. Thereafter, we expand on the nine overarching PHSM typologies and analyse how the six key indicators shape the strengthening or relaxing of PHSMs, with reference to the synthesised framework in figure 1.
{kind=link}
Framework of interactions among nine PHSMs and six key indicators that influence the scaling up and down of PHSMs. PHSMs, Public Health and Social Measures.
Physical distancing
All countries reviewed implemented physical distancing measures to prevent viral transmission between people in close proximity. Common methods include school closures, work from home (WFH) arrangements or limitations applied to public gatherings. School closures vary in duration and intensity, with countries such as Indonesia, Thailand, the Philippines and Vietnam facing challenges of remote learning due to limited internet coverage and availability of learning devices. Similarly, despite digital challenges when shifting to WFH arrangements, all countries pushed for minimal office presence if offsite options were available. In addition, all countries reviewed introduced restrictions on public gatherings, most commonly implemented by controlling the size of group gatherings based on a tiered system, with lockdowns implemented only as a last resort. Singapore, for example, initiated its Circuit Breaker lockdown in response to massive outbreaks within foreign worker dormitories and to rapidly suppress community transmission. In larger countries, stringency of physical distancing differs based on epidemiological performance at sub-national levels, such as the Community Activity Restrictions (known as ‘PPKM’) in Indonesia, which tailored these restrictions based on local hospital capacity and caseloads.
Border controls
The imposition of travel bans to stem the inflow of infections by countries was commonplace after the WHO declared a public health emergency of international concern. For inbound travellers, strict quarantine at designated facilities was required, with the need to monitor health status through various applications. South Korea, for example, mandated inbound travellers to quarantine in dedicated facilities while a Global Positioning System tracking function was used to monitor compliance. As the pandemic continued into its second year, countries relying heavily on tourism trialled calibrated reopening of their borders to the fully vaccinated through sandbox pilots such as the Phuket Sandbox in Thailand and Phu Quoc Island in Vietnam. By the end of 2021, certain countries had shifted from a static close all borders approach to a more dynamic one based on epidemiology in sending and receiving countries, vaccination statuses and to some extent, reciprocity. As vaccination coverage expanded, countries such as Singapore and South Korea commenced vaccinated travel lanes (VTLs), with vaccination and negative test requirements for inbound travellers. However, with the resurgence of more virulent strains such as Delta and Omicron, these countries retightened their borders iteratively.
PPE requirements
Countries reviewed adjusted their requirements for mask-wearing based on the stage of the pandemic that they are in. For example, in the early stages of the pandemic in Singapore, mask-wearing was only for the unwell, but subsequently, everyone was required by law to wear one. Eventually, all countries implemented mandatory mask-wearing, with penalties imposed for non-compliance, such as in Indonesia, where police and military personnel meted out fines to those who flouted these mandates. However, amid increasing vaccine coverage, South Korea altered their masking requirements such that vaccinated people need not wear a mask outdoors by July 2021, but this was suspended amid a spike in numbers, while the Philippines had mandated everyone to wear both face shields and masks while in public. In some Western countries, mask-wearing had been a point of contention between policymakers and citizenry.20 However, this was not the case in countries reviewed due to cultural and environmental factors, such as in Vietnam, where wearing face masks was common due to air pollution in the cities.
Transmission monitoring
Countries reviewed implemented extensive testing, surveillance and contact tracing strategies since the beginning of the pandemic to detect and isolate potential and confirmed cases quickly. PCR testing remains the gold standard for diagnosing COVID-19. Chiefly, PCR testing is coupled with other more efficient testing methods such as rapid antigen tests (RAT) when laboratory testing capacities became overwhelmed by high caseloads brought about by multiple epidemic waves and testing requirements.
Testing strategies are in tandem with contact tracing protocols which aim to identify cases to break transmission chains. Contact tracing teams were rapidly mobilised in all countries, embarking on a manual tracing process initially. As transmissions intensified, digital tools were used to accelerate the tracing process. In Singapore, the TraceTogether mobile application and Safe Entry QR code were created by the government technology office and adopted by the population to aid in contact tracing, while South Korea leveraged CCTV footage, cellular geolocation and credit card histories for the same purpose. However, uptake of such digital strategies faced challenges due to privacy concerns. For the Philippines, an additional hurdle was the parallel development of multiple information systems and digital platforms that were not immediately interoperable. Generally, passive surveillance was already in place for most countries with a system to detect underlying infectious diseases prior to COVID-19, and since 2020, was augmented with active and sentinel surveillance protocols through healthcare providers, routine rostered testing for workers or wastewater testing.
Surge health infrastructure capacity
Health infrastructure such as laboratories, isolation facilities and negative pressure rooms in medical facilities are needed to identify and care for patients and suspected cases as well as parameterise them from the community to reduce transmission. Countries expanded laboratory testing capacities by setting up new laboratories or authorising private laboratories to provide testing services. In South Korea, novel testing protocols such as drive-through and walk-through testing were deployed in car park spaces. In Vietnam and Thailand, the distribution of testing laboratories proliferated across the country in order to reach all provinces. This was done by expediting accreditation of government and private laboratories, commonly under a national laboratory network system. Nonetheless, as more transmissible variants emerged, even this expanded capacity faced difficulties with the swelling demand, making RATs an acceptable means to triage patients for RT-PCR tests. As for quarantine and isolation facilities, countries partnered with the private sector and converted hotels and other large public facilities such as convention centres into quarantine or isolation facilities. Designated hospitals were also retrofitted to serve as respiratory split hospitals to segregate prospective COVID-19 patients from the general patient pool, such as those in South Korea. Initially, the focus was on the quarantine of contacts and isolation of cases in dedicated facilities resulting in a large emphasis on creating such facilities. However, countries such as Singapore and South Korea which had high population vaccination coverage had progressively moved towards a more home-based quarantine and isolation approach for patients with milder symptoms to be managed at home to preserve hospital capacity for more severe cases.
Surging health supplies
At the early stages of the pandemic, countries preserved health supplies by easing import regulations while restricting the export of certain medical products, which were subsequently lifted after domestic production was increased through the use of innovative technologies and approaches. For example, garment factories in Thailand, the Philippines and Vietnam were retrofitted to manufacture PPEs while approvals for manufacturing or sale of certain health products were expedited. For instance, Thailand reclassified hand sanitisers as medical products to prevent production delays. Price controls and regulations to deter hoarding were implemented to ensure the population had access to available stocks. South Korea had initially limited weekly masks sales by retailers, while hoarders faced imprisonment and financial penalties. In addition, countries such as Singapore and South Korea maintained a national stockpile of medical supplies that could be rapidly deployed in times of health emergencies.
Human resource capacity
Having a sufficient and healthy healthcare workforce is imperative to treating, isolating, testing and contact tracing during a pandemic. Across reviewed countries, healthcare workers were overburdened as case numbers increased while taking on heightened risks when managing COVID-19 patients, at times with uncertain access to PPE necessary to provide care safely. To mobilise more human resources, some countries activated their ‘reserves’ which predominantly came from former or retired healthcare workers, medically or non-medically trained volunteers, medical and paramedical students, or the military. In countries such as Vietnam, the military and public security forces were rapidly mobilised and trained to perform contact tracing. In Singapore, nursing students answered the call for volunteers by joining mobile serology teams, while Thailand successfully mobilised their pool of village health volunteers for public education activities and community surveillance.
Vaccine availability and roll-out
Mass vaccination has been touted as a key exit strategy from this pandemic. However, vaccine supply chains must be secured, high-risk groups prioritised and distribution plus access within communities ensured through robust cold chains. Vaccine drives commenced at the beginning of 2021 for countries reviewed. As Singapore ramped up its vaccination drive, it unveiled its VacciNationSG Campaign to address misconceptions, debunk misinformation about vaccinations and promote uptake. Other strategies to promote vaccine uptake are allocation and affordability. In terms of allocation, all countries reviewed had prioritised high-risk groups such as the elderly and front-line workers for vaccination, with the costs of vaccination borne by the government. However, access to vaccines at the country level posed a hurdle for countries failing to secure sufficient advance purchase agreements with pharmaceutical companies. Donations from other countries and the COVAX facility had provided vaccine doses to countries such as the Philippines, Indonesia and Vietnam, although only for a marginal proportion of their population, while others such as Indonesia and Thailand produced their own. Most countries also implemented vaccine differentiated measures, such as Singapore, South Korea and Vietnam, which necessitate a digital vaccination certificate to be presented for entry into certain venues. As more transmissible variants circulated, countries began recommending booster doses, with Singapore only considering those with a booster dose as fully vaccinated.
Social and economic support measures
All countries had provided support packages to the vulnerable groups and businesses, but the level and type of support for the general population varied. These included financial relief packages, skills upgrading to increase employability, measures that cover basic necessities, insurance premium waivers and utility subsidies. To revitalise the economy, Singapore issued vouchers to the general public to spend on local businesses, while Indonesia, Philippines and Vietnam provided tax incentives and reductions in corporate tax for selected businesses. Vulnerable groups such as low income and migrant workers were supported with cash transfers, unemployment protection and free COVID-19 treatment services. Some countries such as the Philippines saw the emergence of ground-up initiatives like food pantries, and Indonesia expanded its cash transfer initiative under Programme Keluarga Harapan for low-income households. Support packages were reportedly extended due to poor economic outlook and prolonging of PHSMs in the face of new waves of infection.
Discussion
In each country, the nine typologies of PHSMs were introduced at different stages and intensities, adapted and influenced by key indicators in order to respond effectively as the pandemic unfolded. The types of PHSMs implemented, though similar in their fundamental policy structure and objectives, were enacted either at national or subnational levels depending on viral transmission, feasibility, fiscal capacity, health systems readiness and economic implications based on local context. The discussion section offers insight into the dynamic interplay among PHSMs and their effects on each other. This is followed by the key indicators that determine the strengthening or relaxing of PHSMs.
The dynamic interplay among PHSMs
PHSMs cannot function alone and must be implemented strategically and synergistically to maximise the protection of the health of populations and livelihoods. Synergies across different PHSMs can achieve their intended outcomes and withstand unintended consequences. Three nested interactions that emerged from this study will be discussed.
First, transmission monitoring through testing and contact tracing must be followed by citizens’ compliance with quarantine and isolation to stem community transmission. Ringfencing cases and contacts require alignment with social and economic support measures so that these individuals possess the resources to remain temporarily segregated from the rest of the community.21 This may come in the form of food delivery services as seen performed by village health volunteers in Thailand and allowances or income replacement given to isolated individuals in Singapore. This is especially integral for informal economy workers or daily waged earners, who are disproportionately affected by these quarantine measures, making physical distancing measures difficult to adhere to.22 The need for such support is more evident in low-income and middle-income countries (LMICs), where a large proportion of their population belongs to informal sector and is impoverished.23 24 However, vulnerable groups also exist in upper-middle-income and high-income countries, which are disproportionately affected by COVID-19 who also need government support. This dilemma further adds to the complexities between the protection of the health of the population and livelihoods.
Second, a more complex interaction network between various PHSMs entails interactions between health worker capacity, health infrastructure, border controls, vaccination roll-out and testing requirements, to name a few. To elaborate, human resources are needed to expand health services provision capacities to respond to the pandemic and to maintain other essential routine services at health facilities, which can be accomplished by mobilising military personnel and volunteers to refurbish non-clinical facilities and erect field hospitals and vaccination centres. During vaccination roll-out, human resources are required for inoculation services and facilitation of the cold chain. Private sector providers are commonly engaged to augment government service personnel to conduct laboratory tests, treatment and quarantine services. In Thailand, public and private healthcare providers were contracted on the same terms, conditions and fees, which had to an extent, prevented patient denials by private facilities.25 26 To that end, hotels were also converted into isolation amenities for returning travellers and close contacts during the initial peaks. Closely related are sandbox pilots for travel, where vaccine campaigns were accelerated to reach a certain level of population coverage before reopening of borders, which was determined by the availability of vaccines, manpower capacity to vaccinate and relevant supporting infrastructure.
Third, the availability of PPE, medical supplies and human resources also need to complement one another to maximise their effectiveness. Specifically, in certain countries with initial supply shortfalls, mask coverage for the general population was low during the early stages of the pandemic. These mismatches between PHSM objectives and medically related supplies were alleviated after rapid market approvals were authorised and domestic manufacturing capacities bolstered. Similarly, adequate PPEs for healthcare workers must be preserved to safeguard essential workforces to render COVID-19 related services while maintaining other essential health services. The severe lack of PPEs had endangered the lives of health workers and, in some cases, precipitated into healthcare worker mortality, further straining the countries’ test, trace and test capabilities.27 28
The list of interlinkages, complementation and synergies between different PHSMs are non-exhaustive, as depicted in the framework by the different permutations represented by the intersecting black lines in figure 1. Fundamentally, the mantra that PHSMs do not operate in silos and one PHSM should not substitute but complement another must be amplified at all levels of the health system.29
Key indicators influencing the dynamism of PHSMs
As the pandemic wore on, vaccines became more available and with the emergence of the more virulent strains in 2021, most countries adjusted their PHSM based on these emerging contexts as well as the impact of prolonged PHSMs on the economy. Policies had to balance between the health of the population and livelihoods. In general, the key indicators that govern the scale and duration of PHSMs are similar across the six countries. For example, Vietnam had used five explicit metrics to achieve this. Specifically, during the early stages of vaccination roll-out, a proportion of the population over the age of 50 fully inoculated was the most important indicator, as older persons were more predisposed to severe symptoms and overburden the health system, followed by the percentage of people over 18 who receive at least one vaccine dose. Next, the health system capacity indicator was predicated on the number of oxygen tanks at commune health stations to be used as a precaution for managing milder cases in the community along with the districts’ plan of deploying mobile health stations to provide care for hard-to-reach populations. Another indicator existed during the peak of demand for critical services, where the government earmarked ICU beds for the most severe COVID-19 cases based on an estimation of the percentage of total COVID-19 cases as potential demand. The number of community infections was also incorporated when calibrating the magnitude of PHSMs. Broadly, in all countries reviewed, parameters for decision-making towards scaling up PHSM include: community spread (indicator 1), number of severe cases and mortality (indicator 2) and health system capacity (indicator 3). For most countries, excluding Singapore, decisions were also made at the subnational level, and PHSMs tailored based on subnational key indicators.
n addition, a country’s fiscal capacity (indicator 4) and vaccination coverage (indicator 5) also act as important indicators (25). Countries that depend heavily on tourism, with large informal economies or insufficient budget reserves, might find themselves reopening their economy prematurely.30 Countries such as Thailand whose economy relies on tourism cautiously reopened borders at selected destinations, contingent on high vaccination coverage. Moreover, of the total government debt, 59.5% of GDP in 2022, 98.14% were internal borrows and were used to finance social and economic support and recovery from the pandemic.31 In 2022, vaccine policy changes were influenced by demand for booster doses in the light of waning vaccine immunity, breakthrough infections, new vaccines and existing fiscal space. When Omicron circulated towards the end of 2021, huge waves of infections threatened to overwhelm health systems. As a result, Thailand recommended a fourth dose to health workers, while Singapore mandated a booster dose to be considered fully vaccinated.32 33 However, despite high vaccination rates in countries such as Singapore, increased community transmission resulted in reclosing of borders in December 2021 and January 2022, with the temporary ceasing of VTLs to preserve hospital capacity.34 Concomitantly, these policy decisions and the prolonging of PHSMs require an enlarged fiscal space for health.35
The availability of technology (indicator 6) is a quintessential element to guide the intensity and duration of PHSMs. This is evident in countries such as Indonesia, Thailand, the Philippines and Vietnam, whereby a large proportion of their student population might not have access to the internet for remote online learning. Despite having measures to support students, it is reportedly insufficient to meet the immense demand. The long-term closure of schools and the digital divide threaten the quality of education and exacerbate inequity gaps.36 Access to technology can determine a population’s capacity to maintain physical distancing measures such as WFH arrangements and provision of telehealth services.37 38 Furthermore, leveraging digital technologies such as mobile applications to perform check-ins at locations by scanning QR codes and generating proximity notifications when in close contact to a suspected or positive case using Bluetooth technology in addition to alerting individuals and authorities for contact tracing and follow-up management proved vital to reducing the transmission in countries such as Singapore, South Korea and Thailand.21 39 40
PHSMs centred on equity require governance and community engagement to balance the protection of health of population and livelihoods
The phasing introduction of PHSM, either sequentially or concurrently in a comprehensive manner, synergise and complement each other, reflects the decision-making agility of the government based on evidence from the field of what works and vice versa. The up-scaling and down-scaling of PHSMs are mostly guided by epidemiological evidence, the effectiveness of interventions and unintended consequences of policies, reflecting the governments’ adaptability. Therefore, governance structures need to take into account key indicators to derive a plan of action which involves the evaluation of the effects of PHSMs on health of population vs incomes. On another level, strong and coordinated governance is imperative at subnational levels, where local governments are devolved the authority to make decisions while maintaining a coordinated national response at all levels of government.41 Instrumentally, governments need to emulate transparency and uphold political accountability regarding decision-making processes, which can come in the form of community engagement as populations need to understand the rationale behind PHSMs, their stringency and duration due to PHSMs’ impacts on their health and livelihoods.42 43 Effective and transparent community engagement strategies can help mobilise the general public to action, such as mobilising volunteers to augment the health workforce or to educate and advocate for behavioural changes that promote adherence to PHSMs. This can be achieved through engaging community leaders to promote compliance with physical distancing and mask-wearing measures, leveraging on pre-existing trust fostered within the community.44 This is seen in Vietnam, where community COVID-19 supervision groups comprising village health workers, youth or women union volunteers were responsible for sharing information and promoting compliance to PHSMs.45 In Singapore, the government also launched both WhatsApp and Telegram chat groups to directly engage the public and provide accurate updates on the evolving situation, modifications to regulations and dispel misinformation.46 Notably, there is a need for clear communication channels by the government to clarify vaccine efficacy and safety, and timely management of vaccine misinformation in the Philippines, where vaccine hesitancy was spreading during the initial stages of vaccination roll-out.47 Chiefly, community engagement can strengthen governance by providing feedback channels to understand the local sociocultural context, enabling iterative tailoring and cocreation of PHSMs that fit the needs of the population.48
All PHSMs seek similar objectives of curbing onward transmission, reducing mortality and preserving livelihoods. The unintended consequences of PHSMs can be seen through widening income gaps, increased gender-based violence and forecasted lowering of educational attainment, among other social and health indices.49–51 These inequities and inflictions on population health outcomes will not only impact the present but future health of a population and its national economy. Hence, PHSMs need to place equity at the core at all stages of the pandemic and can only be achieved when governance structures put the most vulnerable first while simultaneously balancing the dichotomous trade-offs between the health of population and livelihoods.52 53
Charting an equitable and resilient recovery
As more variants and subvariants such as Omicron BA.1 and BA.2 continue to emerge, the need for contextually appropriate PHSMs that will augment vaccines due to waning of immunity in the population remains.54–56 Henceforth, governments must remain vigilant and steadfast by executing regular risk assessments through surveillance strategies and reintroducing evidence-based and cost-effective PHSMs.53 Although PHSMs serve to safeguard the lives and livelihoods of all populations, including the vulnerable, governments need to redress the existing vulnerabilities and societal inequities. The pandemic has put a wedge on and expanded the current fissures between the have and have-nots and amplified the inequities in all dimensions, not only in LMICs but in high-income countries as well.57 58 This is observed in countries reviewed, whereby support packages were offered to vulnerable populations such as migrant workers, as most of them are socially marginalised, lack social protection and are more predisposed to getting infected.59 This is also seen in high-income countries such as Singapore, whereby massive outbreaks in crowded foreign worker dormitories led to the implementation of a nationwide Circuit Breaker for 2 months.60 Therefore, countries that do not offer vaccines to migrants and non-residents, might observe a persistence of epidemic waves, dampening the effectiveness of other PHSMs. The instance of such oversight is also reported in other vulnerable groups such as internally displaced people and refugees.61
Essentially, the level of disproportionate impacts on the poor and vulnerable groups is determined by the level of existing structural inequality on the one hand, the size of social capital and resilience on the other hand, calling on national and global solidarity.62 63 In particular, inadequate vaccine coverage and lack of resilient health system pillars can prolong the pandemic as low-income countries continue to fight outbreaks, permitting the emergence of new variants and spread across the world due to international travel.64 Increasingly, as more viable and effective antivirals are developed and authorised for use, their equitable access has also come under scrutiny.65 Therefore, countries need to focus on equitable distribution of vaccines, antivirals and other resources to strengthen health systems globally and narrow the gap between the global North and South.66 67
Lastly, countries must harness this pandemic as an ephemeral window to strengthen health system capacities by investing in three interlocking pillars: (1) capacity to rapidly detect and react to emerging infectious diseases, (2) capacity to absorb infected individuals while maintaining care continuity for routine management of other diseases and (3) foster an enabling climate for the nurturance of healthy lifestyle and behaviours to promote healthier populations resilient towards diseases.68 Only through these steps can populations and health systems become more resilient and steadfast in the face of a prolonged pandemic.
Strengths and limitations
An in-depth analysis of the interlinks and synergies across nine typologies of PHSMs applied by six Asian countries enabled us to rapidly synthesise a framework for PHSMs where key indicators play a significant role in shaping PHSMs as the pandemic unfolds. Importantly, this study confirms a prior study that explores the major negative impacts on social inequity and vulnerability, and that universality principles prevail in the effective containment of the pandemic.69 However, this study captures snapshots of policy responses from January 2020 to January 2022 in the context of data incompleteness. Given the ongoing and rapid changes to contextual environments, it is likely that many of the policies highlighted above may have changed considerably since the time of writing. Certain information on policies might also be unavailable and inaccessible from public domains. It is, however, beyond the scope of this study to assess the full range of PHSMs and ascertain the effectiveness of implementation.
Conclusion
In 2022, as countries are transitioning from acute to recovery phase, where SARS-CoV-2 may become endemic, high levels of vaccine coverage in parallel with the PHSMs explicated in the framework needs to be made permanent features of health system responses. With waning vaccine immunities, newer variant strains and the reopening of economies, health systems need to remain resilient and agile while ensuring that PHSMs can be swiftly reinstated to protect the health of populations and livelihoods with an equity lens.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
References
Footnotes
Handling editor Alberto L Garcia-Basteiro
Twitter @chuande99, @@iamjun10, @timarthias
Contributors CDF, HL-Q, VT and NA-J conceived the manuscript. All other coauthors contributed to the collection and analysis of the data. CDF wrote the manuscript, with intellectual inputs and revisions made by all coauthors. HL-Q and NA-J supervised the entire research project. CDF is the guarantor.
Funding This research is funded through the Singapore Population Health Improvement Centre (SPHERiC) Collaborative Centre Grant from the National Medical Research Council, Singapore (NMRC/CG/C026/2017_NUHS) and the Asia Pacific Observatory on Health Systems and Policies (WHO registration 2021/1118437-0).
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.