Article Text

Abstract
Background The National Inuit Strategy on Research focuses on advancing Inuit governance in research, increasing ownership over data and building capacity. Responding to this call for Inuit self-determination in research, academic researchers should consider cultural safety in research and ways to promote Inuit-led methods.
Methods This scoping review collated academic literature on public health research in Inuit communities in Canada between 2010 and 2022. A critical assessment of methods used in public health research in Inuit communities examined cultural safety and the use of Inuit-attuned methods. Descriptive and analytical data were summarised in tables and figures. Knowledge user engagement in the research process was analysed with thematic analysis.
Results 356 articles met the inclusion criteria. Much of the published research was in nutrition and mental health, and few initiatives reported translation into promotion programmes. Almost all published research was disease or deficit focused and based on a biomedical paradigm, especially in toxicology, maternal health and chronic diseases. Recent years saw an increased number of participatory studies using a decolonial lens and focusing on resilience. While some qualitative research referred to Inuit methodologies and engaged communities in the research process, most quantitative research was not culturally safe. Overall, community engagement remained in early stages of co-designing research protocols and interventions. Discussion on governance and data ownership was limited. Recent years saw emerging discussions on these issues. Knowledge user capacity-building was limited to brief training on conventional data collection methods.
Conclusions The last decade of published public health research has not responded to the National Inuit Strategy on Research. Participatory research is gaining ground, but has not reached its full potential. A shift from biomedical to decolonised methods is slowly taking place, and public health researchers who have not yet embraced this paradigm shift should do so.
- Public Health
- Systematic review
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The National Inuit Strategy on Research advocates for self-determination in research.
Most published research on Inuit health has limited community participation through the process.
WHAT THIS STUDY ADDS
A biomedical paradigm was prominent in most areas of Inuit public health research.
Of 356 studies, 76 self-identified some community engagement in the research process.
Few studies referred to Indigenous methodologies.
Discussion on capacity-building, governance and data ownership was limited.
Limited translation of evidence to culturally safe health promotion.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Current health research practices fall short of the National Inuit Strategy on Research.
Quantitative and qualitative research should be decolonised and rooted in Inuit worldviews.
Capacity-building and improving access to funding and aligning it with Inuit priorities would increase self-determination in research and data sovereignty.
There is much room to improve participatory research protocols and engage communities and local stakeholders more efficiently.
Introduction
Public health research has not escaped colonisation’s harm.1 2 In Indigenous settings, public health research has long been associated with western academic exploitation and minimal benefit to communities.3 In the words of the president of Inuit Tapiriit Kanatami, the national Inuit organisation: ‘the term research invokes strong reactions among Inuit, because researchers have historically been and continue to be the primary beneficiaries of research involving our people, wildlife, and environment’.4
The colonial history of public health research and its legacy in Indigenous communities has led Indigenous scholars and policymakers to question partnership modalities between Indigenous communities and academic researchers and to reflect on research methods and practices based on western worldviews. Many of these run counter to principles of Inuit research, which is ‘grounded in relational accountability’.3 While there is recognition that ‘Inuit research approaches need to be revitalised in a modern context due to the ongoing effects of colonialism’,3 Inuit view research as a process towards decolonisation and self-determination, in reclaiming Inuit ways and decision-making power.
Cultural safety has potential leverage to put into practice how Inuit want to see research conducted in their communities. Initially developed by a Māori nurse in response to the negative experience Māori faced with interacting with health services in New Zealand,5 the concept is understood as ‘an environment that is spiritually, socially, emotionally, physically safe and there is no assault challenge or denial of Indigenous identity of who they are, and what they need’.6
Cultural safety goes beyond cultural sensitivity and competence to analyse power imbalances, institutional discrimination, racism, and colonial relationships in health services and policies.7 8 In research, it emerged as a response to the recognition that research may cause more harm than good.8 The intercultural dialogue and exchange promoted by cultural safety ensure that research pivots on respect and recognition of lived experience.8 What is deemed culturally safe or unsafe can only be determined by Inuit themselves.9 10
In 2018, the Inuit Tapiriit Kanatami identified five priorities for respectful and beneficial research for Inuit: (1) advance Inuit governance in research, (2) enhance the ethical conduct of research, (3) align funding with Inuit research priorities, (4) ensure Inuit access, ownership, and control over data and information, and (5) build capacity in Inuit Nunangat research.4
Inuit are among the most studied Indigenous groups worldwide. The number of academic publications and dissertations on Inuit health in Canada has increased more than the Inuit population.4 ‘Between 1996 and 2011, the population of Inuit in Canada increased 48% from 41 080 to 59 440. For the same period, the number of Inuit Nunangat (Inuit homeland) related publications increased by approximately 200%. In 1996, for every seven Inuit, there was one publication or dissertation. Research on Inuit increased with time, so in 2011, there was one publication or dissertation for every three Inuit’.2
Based on these facts, it becomes essential to critically examine the current public health research practices and methods, as reflected in the published literature. We also need to assess how published research evidence demonstrates the priorities set by the Inuit Tapiriit Kanatami and the fundamental principles of Inuit research. This review is the first step in a larger research initiative that engages Inuit communities and knowledge users to clarify Inuit cultural safety in research.
Methods
This scoping review11 used the Arksey and O'Malley framework and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Review to report the methods and results sections.12 13 The objectives were to: (1) describe public health research in Inuit communities in Canada, (2) critically evaluate the reported methods as it relates to studies’ design, implementation, evaluation and knowledge translation, (3) assess how studies incorporate Inuit worldview into research methods, and (4) examine how Inuit stakeholders were engaged throughout research process and outputs.
Identifying relevant documents
With the help of an expert librarian, we designed a search strategy using Medical Subject Headings terms and Boolean operators (And/OR) (online supplemental appendix 1). We searched in the following electronic databases: EMBASE, Medline, EBM reviews, CINAHL, JSTOR and PsycInfo. We completed the search on 4 December 2020. We reran the search for articles and used an accession date limit to identify records added on or after 4 December 2020, up to 24 February 2022 (online supplemental appendix 2). We used the same electronic databases except for the EBM reviews, no longer accessible from the previous first author’s institution. We replaced it with the Cochrane Library. The librarian translated the EBM reviews strategy to the Cochrane Library syntax.
Supplemental material
Supplemental material
Screening and selection of relevant documents
Targeting peer-reviewed publications included articles that had to (1) examine a public health issue, (2) focus on Inuit in Canada, (3) report empirical data from primary and/or secondary data sources, (4) report scholars’ reflection on research or process of engaging Inuit stakeholders, and (5) peer-reviewed publication.
In this paper, public health is ‘the science and art of preventing diseases, prolonging life and improving quality of life through organised efforts and informed choices of society, organisations, communities, and individuals’.14 We used the WHO’s definition of health: ‘a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity’.15 Based on these definitions, we included articles on diverse and broad public health issues such as obesity, cancer, cardiovascular diseases, infectious diseases, mental health conditions, maternal health, environmental health, water safety, physical activity, housing conditions and nutrition.
We included published literature involving Indigenous populations if Inuit communities from Canada were included, and data were disaggregated by ethnicity and when data on Inuit were substantial. We considered the following study designs: quantitative, qualitative and mixed methods. We looked at publications in English and French. We restricted the search from 2010 to 2022 (February) to have an overview of the most recent public health research.
Exclusion criteria were: (1) systematic reviews, including narrative reviews, (2) PhD dissertations, (3) data not disaggregated by ethnicity or the data on Inuit were limited, (4) experimental studies on animals, (5) fauna and flora research, including marine biology and geology, (6) genomic studies and clinical drugs trials, (7) clinical reports, and (8) editorial, opinion, letters, conference abstract and commentary.
Charting data, collation, summary and reporting of the results
We designed a chart to collate data extracted. This included title, year of publication, public health topics, geographical localisation, study designs, sample size, methods and instruments. Figures illustrated geographical localisation, study designs and research health topics. We used a thematic analysis to assess qualitative aspects.16 We designed a coding framework iteratively using a hybrid deductive and inductive analytical approach to critically analyse the reported methods, particularly stakeholder engagement throughout the research. We refined the codebook during coding, then reapplied the final form to included articles. Codes reflected justification, framing issues, partnerships, data collection, methods, instruments, data analysis, governance, data ownership, intervention, dissemination, capacity-building, sustainability, ethics and funding sources. We focused on who was involved and how the activity was designed and implemented (table 1). We did not assess quality or risk of bias of the included studies, consistent with scoping review guidelines.17
Description of data extraction items
Positionality
The first author (LB) is a North African Arab Muslim woman working with communities in Canada (Inuit) and Africa. RB is an Inuk male professor and researcher with Inuit in Nunavik, Labrador, and urban settings. CS is a female Canadian expert librarian. NA is a male non-Inuit professor who has worked with more than 200 Indigenous communities in Canada and Inuit in Quebec. This scoping review is the first step in an initiative to co-design culturally safe health research methods for Inuit communities in Nunavik (Quebec).
Patient and public involvement
This study is a scoping review including only published literature. It did not involve patients. However, this study aims to respond to self-determination in research which is one of Inuit stakeholders’ priorities. The results will be disseminated to Inuit stakeholders through meetings.
Results
A total of 5270 citations between 2000 and 2020 were identified through database searches. After removing duplicates and papers published from 2000 to 2010, we retrieved 2893 references. A total of 313 studies met the inclusion criteria. To this, we added nine articles retrieved manually from JSTOR database. In February 2022, we updated the review with 420 citations. Screened using the same inclusion criteria, we added 34 publications. A total of 356 studies met the inclusion criteria (online supplemental appendices 3 and 4).
Supplemental material
Supplemental material
Temporal, geographical localisation and health topics
Figure 1 shows the articles published in 2010–2022. Years 2010 and 2012 had the greatest number of articles (n=41). We observed a slight reduction of published papers per year throughout the decade, with the lowest number in 2017 (n=19). Figure 2 represents the number of self-identified participatory research or articles describing local stakeholders’ engagement. Year 2020 had the highest number of self-identified participatory research publications on Inuit public health (n=10).

Number of articles published from 2010 to 2022. CIHR, Canadian Institutes of Health Research; ITK, Inuit Tapiriit Kanatami.

Number of articles self-identified as participatory research or described community engagement per year. CBPR, community-based participatory research.
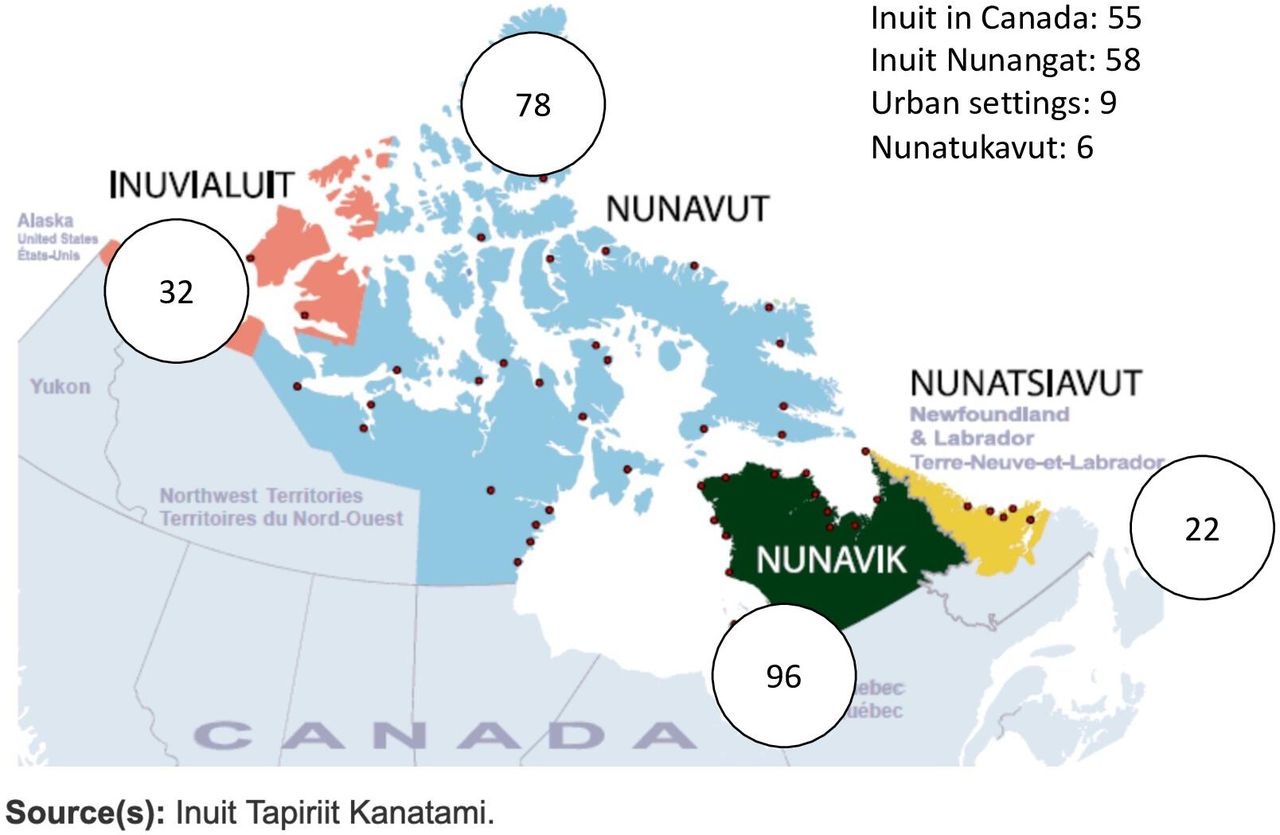
An estimated 65 000 Inuit live in Canada,18 many of them in 53 communities in Inuit Nunangat composed of four regions: Inuvialuit, Nunavut, Nunavik and Nunatsiavut. Most of the published studies occurred in Nunavik (n=96), followed by Nunavut (n=78), Inuvialuit (n=32), Nunatsiavut (n=22) and NunatuKavut (n=6). Nine studies involving Inuit took place in urban settings (Ottawa, Toronto, Montreal). The remaining studies that reported data collected from more than one region were split into two categories. Those covering more than one region in Inuit Nunangat (n=58) and Indigenous populations in Canada worldwide that included Inuit were disaggregated by ethnicity (n=55) (figure 3).
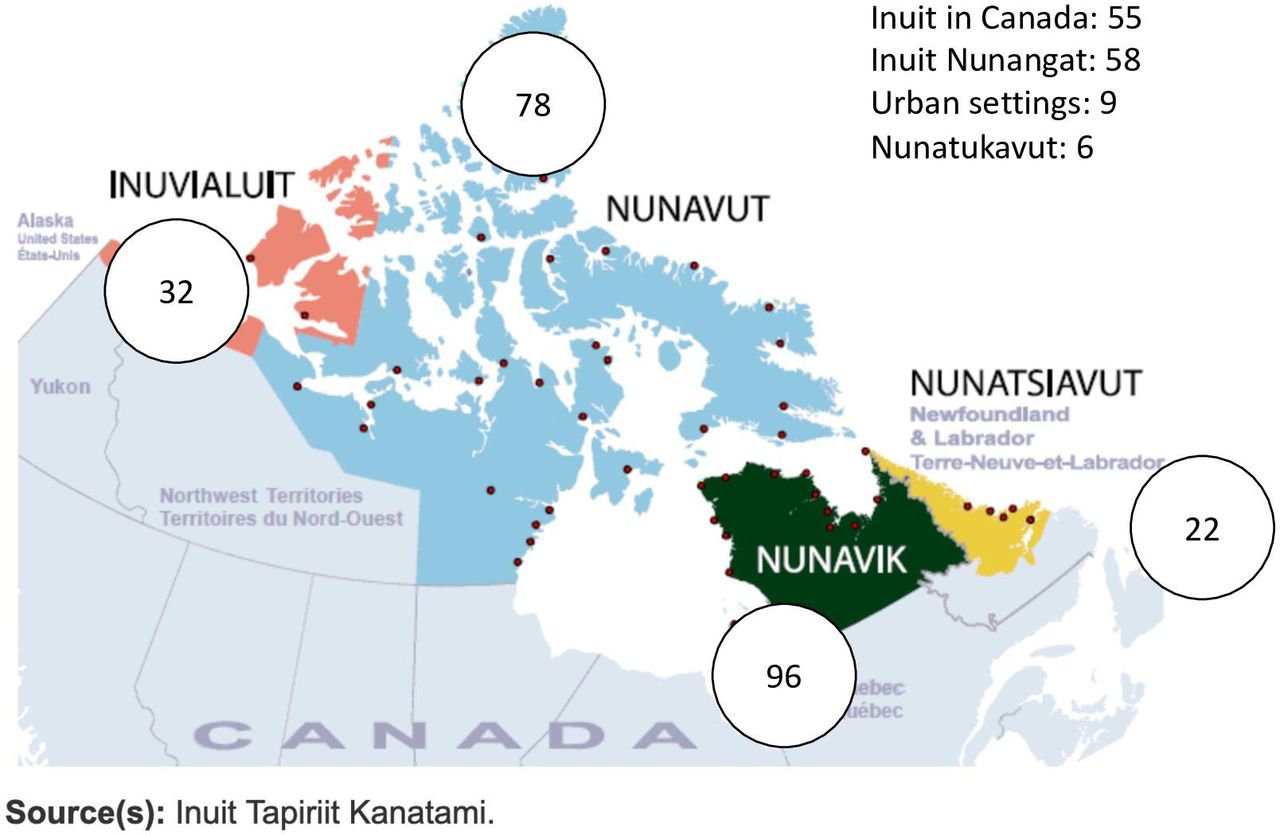
Geographical localisation of health research in Inuit communities from 2010 to 2022.
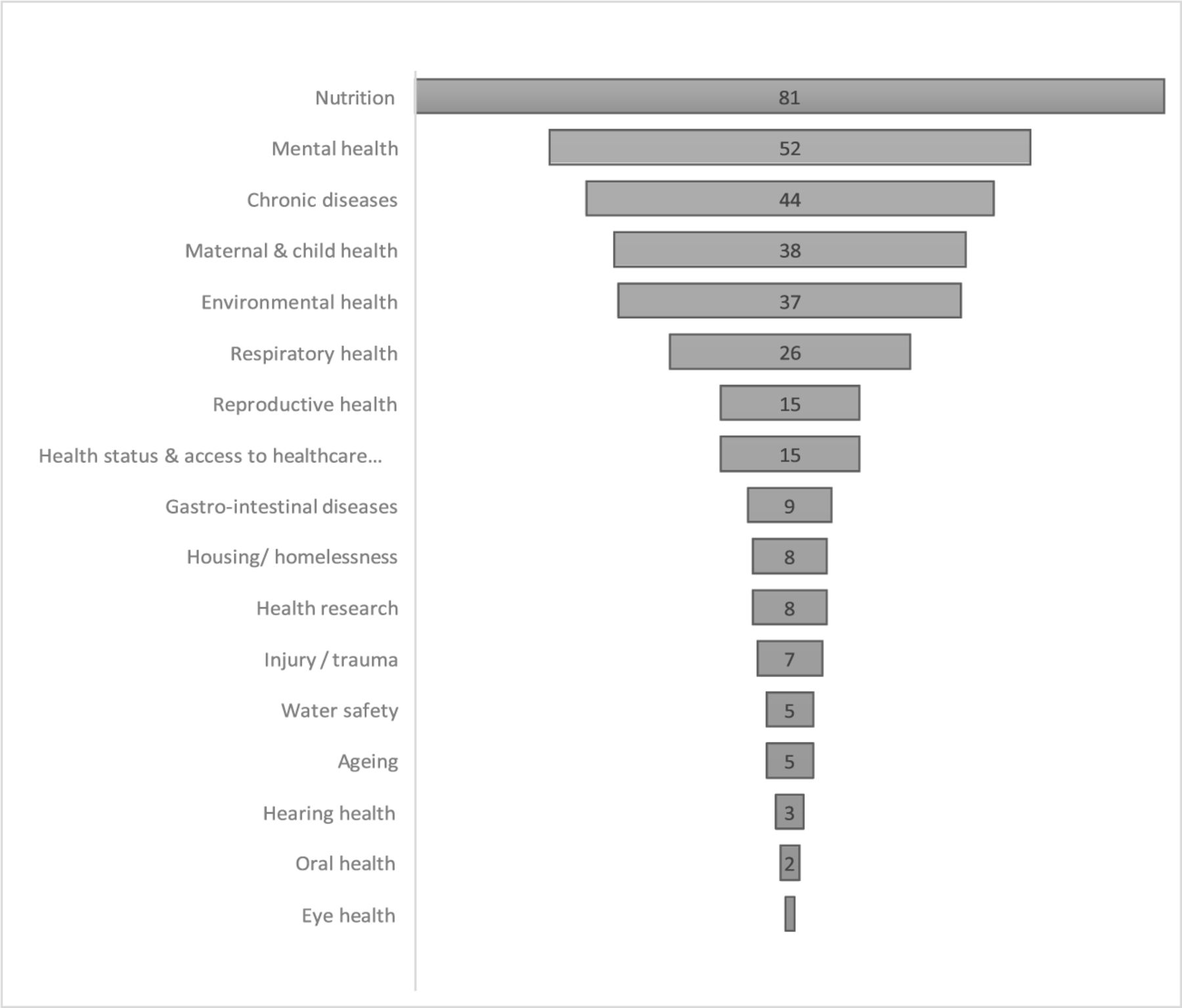
Health topics most studied were nutrition (n=81); mental health (n=52); chronic diseases (including cancer and palliative care) (n=44); maternal and child health (n=38); and environmental health (n=37) (figure 4 and table 2). The nutrition studies focused on the epidemiology and determinants of food insecurity, diet and food programmes. Mental health research involved suicide determinants, youth mental health services and substance use studies. Very little published research focused on psychological distress, anxiety and dementia. The maternal and child health category contained mainly research on maternal and childhood mortality and morbidity. A few studies focused on adolescent sexual and reproductive health, cervical cancer, breastfeeding and Inuit midwifery. Environmental studies examined exposure to environmental contaminants on children’s cognitive, neurodevelopment and behavioural outcomes. Recent studies focused on exploring the impact of climate change on mental health.

Distribution of articles per health topics.
Distribution of articles per health topic addressed
Research on cancer and chronic diseases described the epidemiology and risk factors. Recent cancer research focused on experience of care. Respiratory health research explored tuberculosis, asthma, respiratory infections, pneumococcal diseases and vaccines. The least examined health topics were ageing, housing/homelessness, injury, water safety, gastrointestinal illnesses, hearing, and oral and eye health, also focused on epidemiology and risk factors.
Study designs, data sources and sample size
Of 356 studies, 247 were quantitative, 70 qualitative and 16 mixed methods research, while 23 addressed policy and practice (figure 5). In the latter category, the authors discussed specific issues about the research process, such as ethical issues, challenges and success stories of governance, partnership, participatory process, and knowledge translation activities such as health programming and training (table 3). Some 76 studies self-identified as participatory or described local stakeholders’ engagement throughout the research process (online supplemental appendix 5).
Supplemental material

Distribution of articles per study designs.
Policy and practice studies
Among the 247 quantitative studies, 138 derived data from only five population-based surveys and regional programmes: Aboriginal Peoples Surveys (APS) 2012, Qanuippitaa? National Inuit Health Survey (2004) and the International Polar Year Survey (2007–2008). The 2012 APS included 2614 Inuit adults.19 In the Qanuippitaa? National Inuit Health Survey (2004), 521 households and 1051 individual adults from Nunavik participated.20 The International Polar Year Survey (2007–2008) involved 36 communities from the Inuvialuit Settlement Region, Nunavut and Nunatsiavut, and included 2595 households, 1901 adults and 388 children.21
Nunavik research on environmental health relied on the blood cord monitoring programme (n=286) and the child development study (n=292). The programme involved dyads of mothers and children in three communities.22 The Healthy Foods North Programme was a community-based programme in six Nunavut and Northern Western Territories communities. It involved 332 individuals23 (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Distribution of articles per data source.
Other quantitative research included between 100 and 860 participants using census, random selection using community housing maps and respondent-driven sampling techniques used only in urban settings. Qualitative research study size was between 5 and 120 participants using mainly snowballing, purposive and convenience sampling techniques. Research based on photovoice and storytelling ranged from 5 to 25 participants.
Conceptualisation
Framing health issues and justification
The way authors defined the health issues varied between disciplines and research approaches. Except for climate change research, environmental studies narrowed the health focus to exposure to environmental contaminants. A study on attention deficit hyperactivity disorder recognised a complex aetiology. The authors emphasised the relevance of focusing on the environmental contaminant.24 Apart from some tuberculosis research, respiratory health research viewed health outcomes through a clinical lens.25–27 Nutrition and chronic diseases studies situated health in a nutrition transition paradigm, reporting a shift from traditional Inuit lifestyle to western diets and physical activity.28–31 Studies on childbirth outcomes and infant health addressed health about maternal health risk behaviours (smoking, alcohol).32–34 Across health topics, many studies situated health issues within social, cultural and economic determinants in health. For example, one study examined the impact of age, gender, education, income, employment and cultural variables on diet quality.35
Most recent studies recognised health outcomes as distal determinants of colonialism, the impact of residential schools and systemic racism.36–41 Earlier cancer research focused on the high rates and addressed health system challenges (access to treatment, lack of specific Inuit health data).42 43 More recent cancer research recognised the legacy of colonialism and advocated for culturally safe care.44 45 The same pattern is observed in mental health research. Studies focused more on protective factors, seeking culturally safe services and resilience.39 46–48 The distal determinant recognition was more prominent in studies using a participatory approach.
Authors reported several justifications for their research: (1) overcome knowledge gaps,22 42 49 (2) describe disease burden, risk factors and adverse outcomes,50–57 (3) explore and highlight health disparities,49 58–63 (4) inform development or improvement of health services and programmes,49 64–66 and (5) respond to local public health authorities/community requests and support Inuit-led research and programmes.67–74
Implementation
Inception, protocols and decision-making process
Studies reported involvement of political and health authorities from the different Inuit regions. Researchers engaged also with national and community-based organisations. The most common type of collaboration was between southern-based academic researchers with health and political representatives at the national, regional and local levels (Hamlet, Council) (n=177). Thirty-nine studies21 32 39 41 44 47 48 65 67 71–73 75–98 established an advisory committee to oversee the research and to provide feedback on the research protocols.
Engagement and participation reported in 76 articles spanned all research stages, being more prominent in early stages (design) (online supplemental appendix 5). In one food insecurity study, the author consulted with local stakeholders to identify research priorities, develop the methodology and conduct fieldwork.99 A study on climate change reported collaboratively developed research questions, study design, and resulting interventions engaging researchers, community members, and regional provincial and federal stakeholders.68 Some studies reported that consultations ensured that the research was aligned with community priorities and conducted in a culturally appropriate way.36 70 72 100–103 Two studies reported that the consultations with Inuit organisations and partners ensured that the research is rooted in an Indigenous perspective.104 105
Inuit organisations and scholars also led initiatives. The Fostering Open eXpression Programme was a participatory action research project to promote the health and well-being of Northern and Indigenous youth, focusing on girls’ sexual and mental health and gender-diverse youth. This participatory programme used traditional beading and art-based methods to help teenage girls express their knowledge, opinions, and mental and sexual health questions.106 107
The Qaujigiartiit Health Research Centre and the Nunavut network for Indigenous health research are independent, non-profit community research institutes and community-led organisations that design and implement research projects to address the needs of Nunavut communities.73 74 108 109 These organisations addressed several issues, such as the impact of climate change on health, food insecurity, and sexual and reproductive health. In Rigolet, Nunatsiavut, My Word: Storytelling and Digital Media Lab was a community-driven, participatory storytelling project led by the Rigolet Inuit Community Government. This project mobilised digital media to gather place-based narratives, documenting the impacts of climate change on human health and well-being and sharing adaptation strategies.69 110
One study reported researchers and community researchers undertook all aspects of this research together in a collaborative manner with shared decision-making. Another author reported workshops at key stages in the research to make collective decisions on key aspects.111 A climate change study mentioned that, while formal governance was explicit, informal governance (social status, power relationships) was unclear in their study.69 Authors using a decolonised approach discussed their awareness of their power.47 112 113 Two recent studies discussed power dynamics between researchers and communities.41 103
Design instruments
Most studies used standardised (non-Inuit) questionnaires, scales and classification. Two respiratory studies used the International Study of Asthma and Allergies in Childhood Questionnaire.114 115 Food insecurity studies used the 18-item USDA (The United States Department of Agriculture) food security survey.21 29 30 116 Obesity and overweight studies used the body mass index classification or the International Obesity Task Force.117 118 Researchers used the Rosenberg Self-Esteem Scale or the Psychology Distress Scale40 119 in mental health. The gender-based violence studies used the Conflict Tactics Scales.40 119 Adaptation to Inuit culture, such as it was, amounted to translating instruments into Inuktitut, changing some wording, removing/adding questions or justifying their validity by their use in other Indigenous populations.
Questionnaires focused on risk factors, abnormalities and deprivation, especially studies focused on the impact of environmental contaminants on neurodevelopment and psychological outcomes. For example, a 2019 study based on a longitudinal cohort of Inuit children (n=212) tested direct associations between childhood lead concentrations and adolescent externalising symptoms and substance abuse.120 The authors used the Disruptive Behaviour Disorders Rating Scale, the Child Oppositional Defiant and Conduct Disorder, the Barkley Adult Attention Deficit Hyperactivity Disorder Scale and the Diagnostic Interview Schedule for Children’s Psychiatric Disorders. A grid across these instruments assessed alcohol and drug problems in Inuit adolescents. This questionnaire was designed and tested among Quebec’s French-speaking adolescents.120 A 2020 study used the Screen for Child Anxiety Related Emotional Disorders and the State-Trait Anxiety Inventory to examine the association between anxiety among the at-risk population of Inuit adolescents (n=89) and exposure to environmental chemicals. The authors did not mention whether these questionnaires were adapted to Inuit participants.121 Another study in Nunavik on food insecurity and psychological distress among Inuit adolescents (n=212) used an established child behaviour checklist, the Disruptive Behaviour Disorders Rating Scale and the Achenbach’s Youth Self-Report. The authors recognised none of these questionnaires had been used before in Inuit children and justified their adoption by reporting use among other Indigenous Arctic populations, among whom the internal consistency was either high or moderate.122 A 2021 qualitative study collated views on three psychometric scales used to diagnose depression among adults. The participants considered the measurement scales culturally unsafe. The major components that hindered their acceptance were: numerical rating, self-evaluation (vs supportive interaction) and a focus on symptoms rather than supportive factors. The participants preferred the Growth and Empowerment Measure.39
Studies based on population surveys (APS, Nunavik and Polar Health Surveys) indicated that the design included consultation with Indigenous political and public health authorities. Statistics Canada designed and implemented APS in consultation with Indigenous political and health authorities. Indigenous representatives provided feedback regarding the previous survey, omitted areas of interest, groups not represented and issues unique to each Aboriginal group.123 L’Institut Nationale de Santé Publique and a southern university led the design, implementation and evaluation of the Qanuippitaa? National Inuit Health Survey (2004).124 Two southern universities designed and implemented the International Polar Health Survey in consultation with Inuit territorial health authorities. Authors reported the steering committee discussed survey content.21 One report from the International Polar Survey indicated the indigeneity domain referred to items of interest to Inuit partners. It involved indicators of culture and acculturation, social cohesion and social safety nets among the determinants of Inuit health.125
Several authors questioned the western view underpinning concepts and instruments used in their research.30 77 113 126–130 They recommended more studies to adapt these concepts, variables and instruments to the Inuit worldview. For example, the USDA food security assessment tool remains to be validated in Indigenous populations. Further work is needed to develop definitions of food security relevant to Inuit.30 126 One article reported the question items in the USDA module lack construct validity for Inuit.129
There was also debate among scholars about the measurement of household crowding.130 131 One study criticised the concept as currently measured in Inuit communities.130 The authors reported that the ‘concept’s application tended to obscure the important ways culture mediates the relationship linking material conditions to health outcomes of interest and was at odds with local understandings of the overcrowding’.130 Another study also recognised the lack of cultural relevance of indicators to measure household crowding; they used it because no alternatives had been proposed.132
Some researchers reported alternatives to cultural appropriateness on research instruments. A 2016 study based on cross-sectional data from the 2004 Nunavik Inuit Health Survey aimed to quantify individual and community determinants of Inuit youth mental wellness.133 The authors emphasised factors identified as important to Inuit. They used part of Inuit Tapiriit Kanatami’s definition of mental wellness, measured by a seven-item version of the validated Rosenberg Self-Esteem Scale. The authors converted the original point score to a percentage value for interpretation.133 A 2019 study found the 2012 APS not fully designed in accordance with the vision of Indigenous health research; they attempted to ground their research in Indigenous, culturally appropriate theories.134
Several studies using a participatory approach in surveys reported adaptation to Inuit contexts.36 70 99 135 136 The adaptation varied in scope. Reporting a locally adapted USDA food security survey,99 136 for example, the authors assumed Inuit had already experienced food insecurity and used four locally adapted questions of the standard six items of the questionnaire. Yet, for the coping strategies questions in the same questionnaire, the authors used standardised questions.99 136 The Healthy Foods North Programme used a food frequency questionnaire developed specifically for the Inuit population.135 The adaptation involved traditional foods, food models to assess animal meat consumption and local food lexicon.135 Two studies on access to healthcare services in urban settings used a respectful health assessment survey tool.36 70 Authors reported their survey tool incorporated domains of relevance to Indigenous community identified through concept mapping. After discussions with community partners, they modified the tool, although the unmet health needs item was not adapted. A 2019 ageing study designed an indicator of healthy ageing for Inuit elders through a mapping activity of concepts related to health and well-being.127
In qualitative studies, interview and focus group discussion guides were derived from research objectives and literature. Some studies engaged community members to provide inputs to formulate these guides.68 77 79 137
Data collection and analysis
Most quantitative studies were cross-sectional, historical, or prospective longitudinal studies and secondary analyses of population-based surveys and censuses. Other data collection methods included clinical (anthropometric, neurodevelopment assessments), biological and laboratory assessments, and dietary and psychometric tests. Several studies on maternal and children’s health outcomes relied on vital statistics and national and regional registries. Cancer research used chart reviews.
The most common qualitative data collection methods were interviews and focus groups, followed by participatory tools like photovoice, storytelling, digital storytelling, wisdom circles and concept mapping activity. Interviews and focus groups were semidirective with open questions or in a conversation format. One study on substance use reported that interviews became more directive in covering the essential content sought.96
In three studies, authors incorporated Inuit cultural practices during the data collection.45 48 105 Two recent studies used traditional craft activities like sewing and seal fur earing in focus groups.45 105 In a study on violence prevention among youth, the focus group began with the ceremonial lighting of the qulliq (seal-oil lamp), and an Inuk elder co-facilitated the session.48 Photovoice studies considered their methods culturally appropriate for community-based participatory research in Indigenous settings or justified their use by mentioning that the advisory committees approved them.73 77 99 136 138 139 One study on ageing, including First Nations and Inuit, initially aimed to use photovoice and focus group discussions. The authors changed their data collection strategies based on feedback from First Nations participants who were uncomfortable with the photovoice method. While First Nations participants preferred individual interviews, Inuit participants were more satisfied with focus groups and attended other discussions to hear their peers’ voices.77 We found one study in which researchers reflected on the conventional research methods and sought a complementary data collection method that ‘reflects, preserves, and promotes Inuit culture while avoiding methods that can serve colonial knowledge, power, and truth’.110
Authors used digital recording and note-taking less often to capture data. They offered participants the option of data collection in Inuktitut, English and French. The authors used the following options to conduct the qualitative data collection: (1) only research team members, (2) research team members with the support of local researchers acting as interpreters, (3) only trained local researchers.
Advisory committees provided technical and logistics assistance during the data collection process emphasising the community’s role in recruitment.77 87 In six studies, authors reported that the advisory groups found the interview and focus groups appropriate.65 77 82 87 89 112
In quantitative studies, authors used trained research assistants to administer the questionnaire. The research assistants included graduate students and community members. Studies involving anthropometric measurement, clinical tests and blood sampling relied on nurses and other paramedics/public health staff or graduate studies in psychology (psychometric and neurocognitive tests). The survey format was face-to-face, telephone, self-administered and digital (iPad, computers) with a prominent face-to-face questionnaire. Survey studies considered Inuit languages. Some translated questionnaires, some used data collectors proficient in Inuit languages or they used interpreters.
Qualitative and photovoice studies used thematic analysis variants (content analysis, constant comparative). Authors mostly opted for inductive and hybrid approaches with an iterative process to capture Inuit lived experience, unexpected factors and outcomes related to the health issue. Eight studies applied theoretical approaches and frameworks to guide the data analysis process.39 41 85 113 139–141 One study of barriers and facilitators to implementing human papillomavirus self-sampling in Nunavik, for example, used Purnell’s model for cultural competence to provide a structure for collecting and analysing cultural data.85
In almost half of the qualitative studies (31 of 70), authors reported some engagement of local stakeholders through member checking to validate the preliminary findings or discussion sessions with Inuit partners to review data interpretation. In three photovoice studies, researchers opted for collective data analysis and interpretation to examine meanings; they shared stories, identified themes and grouped photos according to themes.73 99 138 Two used individual interviews with research team members.111 139 One study used a mix of both.142 Five studies reported respecting the principle Iqqaumaqatigiinniq derived from Inuit epistemology and knowledge, whereby knowledge is produced collectively through a ‘coming-together’ of meaning after a cyclical process of dialogue and periods of reflection among knowledge makers.73 91 143–145
A 2020 study evaluating a land-based programme to improve well-being recognised that thematic analysis did not reflect Indigenous ways of making meaning from other people’s stories and experiences.41 In their case, the community advisory board and research team agreed to use this approach for the project.41 In another mental health study, the author expressed discomfort in analysing the data and discussed this bias with Inuit partners who felt it was appropriate and helpful if done in the context of care and dialogue with the community. The author reported this bias that remained an ongoing discussion with partners.89 Another study on intimate partner violence reported that none of the research team were Indigenous, and consequently, interpretation of results could not include Indigenous worldviews.146
While some qualitative research engaged local stakeholders and participants in the data analysis process, quantitative research saw no engagement with Inuit stakeholders, except for four epidemiological studies that used a participatory paradigm that considered Inuit interests in the analysis.71 100 104 147 One study reported exploring ethnicity in Helicobacter pylori and found the infection less frequent among non-Indigenous populations. The authors noted exploration of ethnicity was a community request.71 An epidemiological study of suicide engaged in several round tables with Inuit stakeholders to discuss the results considering the social, cultural and economic contexts.100
Quantitative research used conventional data analysis techniques, and authors used descriptive and analytical statistics. Authors designed statistical models to be tested. The integration or removal of variables depended on literature, expert knowledge or conventional p value threshold.
Knowledge translation
Dissemination and knowledge translation outputs
Dissemination strategies and knowledge translation outputs were not systematically reported in the published articles. When authors described research dissemination, they reported diverse channels: radio shows, community gatherings, potlucks, social media, photo exhibits, newsletters and open houses.69 90 111 139 One study on perceptions of health risks reported participants received photos, posters, and fact sheets information on the study and its primary results during an open house event, as recommended by the community researchers and the regional Inuit government.111 Researchers often used reports to disseminate results.36 73 89 97 139 148 Three studies mentioned presenting results at national and international conferences.76 100 149
Peer-reviewed publications were invariably researcher led. Many studies included local health authorities and Inuit partners as coauthors. Researchers were the first authors of all publications. Only 4 of 356 studies had self-reported Inuit scholars as first authors,45 70 80 87 with three studies published by the director of an Inuit research institution.73 74 109 One study on climate change obtained the approval to publish results with the community name and location.68
Interventions and sustainability
Sixteen of 356 studies translated into tangible interventions that could be scaled up and sustained23 44 67 69 88 90 113 150–157 (table 4). The interventions included preventive and curative activities. One participatory research initiative co-designed, implemented and evaluated a whiteboard video to prevent acute gastro-illnesses.90 Another epidemiology participatory study focused on community screening and offering clinical care for pylori infection.88 Interventions resulting from the studies were diverse in format, scope and scale. In Nunavik, two projects translated into adopting and institutionalising health policies: a policy on a transfat reduction process in Nunavik store-bought foods and a legislation to ban lead-shot ammunition as an intervention to prevent lead exposure.151 152 In these two policies, southern-based researchers disseminated their research to local government, and public health authorities acted.151 152 The study resulted in the transfat reduction policy suggested the strategies to the Nunavik partners.151 An urban study tested the feasibility and acceptability of a CD-ROM delivering messages for midwifery.153 This study engaged two elders to produce the content of the CD-ROM, and 40 individuals were involved in the assessment of the tool.153 A nutrition study piloted six radio dramas to moderate the consumption of soft drinks among youth.67 The development and evaluation of the radio drama engaged six youths.67 A recent study tested an application to increase the cultural safety of short-term providers working in Nunavut.109 The researchers assessed the tool with a questionnaire that 18 participants completed.109
Summary of interventions
The spectrum of engagement of community members varied during the development of these interventions. Community members and local representatives were engaged in developing and implementing the interventions. For example, the Healthy Foods North Programme involved community members in the proposed intervention materials, identifying the best media, choosing key messages and the channels to reach various audiences,135 and community members were trained to deliver the different intervention components. A study trained community members to conduct awareness activities on tuberculosis, and youth developed the messages for the videos.155 156 A mental health study engaged community health workers to conduct outreach activities and deliver appropriate care for youth.154
The studies were proof of concept or implemented on a small scale. Three studies used a quasi-experimental design to measure short-term outcomes.135 152 155 One study used single-centre, randomised controlled trial adherence, and identified barriers to completing treatment among H. pylori-positive participants.71
The published literature offered limited evidence of intervention scale-up and sustainability. One study reached the stage of institutionalisation of a policy to prevent lead exposure in Nunavik.152 Another study, using an eco-health approach in Rigolet, reported the creation of a laboratory dedicated to digital media and storytelling to share information about Inuit culture, history and lifestyle through personal narrative.69
Capacity-building
Seventeen of the 356 articles reported capacity-building.21 41 47 69 73 86 98 111 135 139 155 158–162 The training focused mainly on data collection (administering questionnaires, interview skills and photovoice). A project on climate change provided details on how the project provided capacity-building in research skills (research design, data collection methods), professional writing, presentation, facilitation and digital storytelling techniques.69
A Nunavut study described a cross-cultural research workshop to encourage reciprocity as a basis for research training incorporating western and Inuit approaches. The authors mentioned that the workshop framework integrated taxonomy competencies embedded in the Inuit Qaujimajatuqangit philosophy.161 The International Polar Survey and the Healthy Foods North Programme trained fieldworkers to administer the questionnaires.21 23
Other studies reported specific training related to their interventions (mental health, respiratory health). A Canadian initiative to improve mental health services for youth trained community health workers and clinicians to conduct assessments of mental health problems. The objective of the training was to empower clinicians to function independently as the first point of contact. The researchers used the WHO training material and Indigenous-focused modules.98
One paper described bidirectional learning.41 The study evaluated a land-based programme led by the Inuvialuit Regional Corporation. The researchers learnt from Inuvialuit members about Inuvialuit ways of living, culture, and history to better engage with participants and about land skills such as driving a snow machine and sewing.41
Ethics, data ownership and funding
The included studies obtained ethical approvals from mainly southern universities to conduct their research. They also got licences or letters from local research institutes (ie, Aurora License from Nunavut) and political authorities (Hamlet Council). In Nunatsiavut, studies sought ethical approvals from the Nunatsiavut Government Research Advisory Committee and the NunatuKavut Community Council.139 163–166 The ethical section focused on consent and financial compensation and limited information about privacy, confidentiality and especially benefits/risks of participating in the research. A study led by an Inuk researcher raised the lack of description of how research benefits Inuit communities.80
Researchers used written and, less commonly, oral consent. The study led by the Inuk researcher pointed out how the consent process is complex from an Inuit perspective. It has several implications: (1) community consent through establishing relationships with the community, (2) consent concerning power involves community fears from technical jargon used by the researcher or the blind trust in the researcher, (3) consent in partnership involves community needs to be involved in the research process, (4) consent as dissemination through dissemination and community engagement in data interpretation.80
The International Polar Survey and the Nunavik Health Survey used a DVD to watch before getting the consent of the participants to support oral Inuit traditions.21 124 The researchers who sought verbal approval are self-identified participatory and community-based research.76 83 166 167
Researchers reported that financial compensation was discussed and agreed upon with local partners before the study. The monetary compensation varied from $C20 to $C100, which took the form of gift cards for local groceries and gas stores. Other studies gave an honorarium. The study led by the Inuk researcher pointed to the lack of or inadequate financial compensation at the early stage of the research to establish and build relationships. In her study, elders shared time and knowledge and were not compensated.80
Thirteen studies using a participatory approach referred to the Canadian Institutes of Health Research Guidelines for Health Research Involving Aboriginal People.36 44 45 73 83 87 95 97 134 143 168–170 Thirteen studies mentioned information on data ownership process.21 36 41 47 70 73 100 133 138 139 171–173 Three indicated that they signed a memorandum of understanding with local stakeholders.21 47 100 A Nunavut study on suicide prevention signed a memorandum of understanding with the Hamlet Council in which community members own the data.100 A photovoice project reported that copies of the photo books were donated to school libraries in the 11 NunatuKavut communities to ensure that the knowledge generated from this project remained within the communities.139 Three self-identified participatory research reported that the community-based organisation stored, own and maintained control over the data,36 41 70 and six studies referred to the principles of Ownership, Control, Access and Possession for data management.36 39 65 169 173
Studies received funds mainly from the Canadian Federal Government and its research institutions and agencies (ie, Canadian Institute of Health Research, Public Health Agency Canada), then provincial and Indigenous research institutions and local governments. The funds took the form of research grants, career development, and scholarship. Medical associations, hospitals and a few foundations also offered financial support.
Discussion
While most published research on Inuit health was disease and deficit focused, using biomedical perspectives, we observed an increase in participatory studies using a decolonial lens to focus on resilience. There were very few Inuit-specific research approaches, and few research initiatives reported translation into promotion and prevention programmes. Community engagement focused on the early stages of co-designing research proposals and interventions. Governance, data sovereignty, and capacity-building remained the weakest links of the research process and outputs on Inuit health.
Most studies were rooted in a biomedical perspective, especially in toxicology, maternal and child health and chronic diseases. These focused on risk factors and adverse outcomes and used standardised questionnaires, reflecting what Walter and Suina called 5-D data: difference, disparity, disadvantage, dysfunction and deprivation.174 This emphasises the need for research that contrasts with these ‘deficit narratives and collect data that reflect the embodied social, political, historical and cultural realities of Indigenous people’s lives’.174
While there is a misconception that qualitative research is more culturally appropriate in Indigenous settings than quantitative research,9 174 175 we believe both are relevant and have a place in Inuit public health research; however, both must be culturally safe.9 176 In this review, little qualitative research was rooted in Inuit worldviews. There was also a tendency to see First Nations and Inuit as a homogeneous group, where First Nations perspectives and values predominate. The study on ageing involving First Nations and Inuit in Ottawa illustrated this assumption.77 We only found one study in which authors sought an authentic decolonised qualitative research method.110 The positive note is that things are changing. The recent studies incorporated cultural practices (sewing) within the data collection process.45 105 A qualitative study described the development of a consensus methodology (to contrast with the Delphi method) rooted in Inuit worldviews.177
This review showed how much work is needed to decolonise quantitative research, especially in developing instruments. Like qualitative researchers, quantitative researchers made assumptions that their instruments were valid because they have been used in other Indigenous populations. This shows how authors did not recognise Inuit history or social and cultural context, which is quite different from, for example, First Nations.10 178 A study led by an Inuk researcher pointed out how Inuit communities had concerns about a common misconception that ‘all Aboriginal people are the same and how researchers continue to base their assumptions on an assimilationist perspective’.80
Some studies attempted to adapt their survey instruments to Inuit context and culture. However, the adaptation was limited to ensure that the questionnaire was culturally appropriate (wording, local lexicon, inclusion of Inuit items). This is not enough if researchers aim to respond to community needs and priorities.9 Community members might be interested in exploring causal relationships between an outcome and determinants based on their lived experiences that the researchers have not considered or are unavailable in the literature.9 In addition, this way of developing research instruments is no more acceptable by Indigenous organisations. They no longer advocate incorporating Indigenous knowledge into western research methods but for its recognition based on its scientific merit and inclusion as a distinct knowledge.10 Inuit Tapiriit Kanatami wants to see Inuit-specific and relevant indicators in Inuit health surveys.4
It was also clear from the review that quantitative data analysis was based on western epistemology assumptions. Studies privileged certain variables over others and constructed statistical models without considering Inuit cultural and social contexts10 174 179; however, recent years see an emergence of research to decolonise epidemiology research methods.70 180 181 For instance, Our Health Counts is a research initiative led by First Nations, Inuit and Métis researchers to address the absence of population-based health assessment information in urban settings.182 The Centro de Investigación de Enfermedades Tropicales (CIET) organisation, which works with and for Indigenous communities, uses ‘Bayesian approaches that incorporate pre-existing evidence and beliefs as a prior distribution of probabilities; this allows to connect Inuit and scientific knowledge into statistical analysis formally’.9
Many studies reported that they engaged local stakeholders at each step of the research process; however, the engagement was often reduced to consultations at early stage of designing research protocols and interventions. Local stakeholders provided support for administrative and logistics for recruitment and collecting data. Engagement was inconsistent in qualitative research at the data analysis and interpretation stages and almost absent from quantitative research. The literature we reviewed did not offer a clear picture of how the Inuit worldview might be considered and preserved in the data analysis process. It was, therefore, difficult to assess the extent to which knowledge derived from the studies was co-created with communities. Local stakeholders’ engagement was even less clear at the dissemination stages. Academics led peer-reviewed publications though some included local public and political entities as coauthors. All these findings were consistent with systematic reviews in Canada183 184 and elsewhere.185 186
Capacity-building should be strengthened to respond to the call for Inuit self-determination in research. Researchers should find ways to cultivate and foster community skills from research design to reporting, including the most technical and challenging steps of the research (instruments development, sampling techniques, data analysis and interpretation, scientific and grant writing). Recent years see emerging initiatives for capacity-building. For instance, the Our Health Counts Project is developing applied Indigenous epidemiology, health information, health services, and programme evaluation training and mentorship programme.182 Inuit Tapiriit Kanatami expects more of these initiatives.4 They advocate developing Inuit-specific training and education programmes to foster future generations of Inuit researchers.
While some Indigenous communities are forming their local ethical committees, southern universities continue to provide most of the ethical approvals of the included studies, which might not be suitable for reviewing Inuit research. Southern universities use standardised protocols for reviewing research and might not consider Inuit social and cultural values to research, research question to local priorities, cultural appropriateness of methodologies and other concerns of cultural safety.9 For instance, university ethical review committees might require written consent that might not support oral traditions of Indigenous communities or expect a finalised questionnaire before starting the research, which might not allow researchers to work collaboratively with communities to include their knowledge and experience.9 In this review, limited studies referred to the guidelines outlined in the Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans (Chapter 9). Inuit Tapiriit Kanatami advocates for adherence to this guideline by all universities.4 Therefore, we recommend greater use of Inuit ethics committees and increase Inuit participation or Indigenous experts in southern university committees. We also recommend cultural safety training for southern universities’ ethics committees.
Another key to Inuit research is data sovereignty.4 In this review, few studies used the principles of Ownership, Control, Access and Possession developed by First Nations organisations to fill the gap on community rights and information about them.4 Inuit Tapiriit Kanatami wants to develop Inuit-specific guidelines on data accessibility, ownership and control.4
Academic funding agencies of the Government of Canada were the primary funders of the studies included in this review, which reinforced the privilege of universities to apply for grants and scholarships to the detriment of Inuit organisations, which are excluded from accessing research funding because they are not academic institutions. In addition, currently, there are no specific Inuit health programmes at the Canadian Institute of Health Research, which decrease opportunities for Inuit health research.
At the policy level, the Canadian Federal Government is acting. On 21 April 2022, Inuit representatives and federal ministers announced they had approved the Inuit Nunangat Policy, which recognised the region as geographically, culturally, and politically distinct and aimed to integrate its interests into decisions in Ottawa. The government granted $25 million to cover 5 years. Of this, $20 million will be earmarked for projects to accelerate the implementation of the policy under Inuit priorities. This could be a step forward on the path of Inuit self-determination and reconciliation.187
Limitations
To our knowledge, this is the first review of research methods, practices, participation, and knowledge mobilisation without restriction on health topics and in all Inuit communities in Canada.
We acknowledge several limitations. The review covered articles between 2010 and 2022, excluding earlier relevant articles. Our conclusions are about the current literature, although reviews without date restrictions reached similar findings.183 184 188 Since we focused on Inuit communities in Canada, results cannot be generalised without caution to other Circumpolar regions or Indigenous communities with historical, social contexts and research practices. As happens in systematic reviews that reflect the state of the current published literature, we included multiple articles published by the same research team and/or from the same projects.
Our review explored public health research reported in published academic literature to question how mainstream research might respond to calls for increasing Inuit self-determination. With this focus, we excluded grey literature, including Inuit organisations like Pauktuutit Inuit Women of Canada.183 Our review is an invitation to rethink academic public health research with Inuit communities, adopting a cultural safety paradigm to co-design participatory protocols and methods that increase Inuit self-determination in research.
Our interpretation of community participation in the review required some caution. Most papers did not have participation or community ownership as their research objectives, so they may have made little reference to these dynamics in their methods. The word limits of journals, very few of which place a premium on participation, may have discouraged authors from expansive descriptions of community engagement.
The lead author alone screened the titles and abstracts, which, in some settings, is not as reliable as double screening; it can increase the risk of missing studies. A recent study showed that single screening is appropriate if done by an experienced reviewer,189 which is the case here.
Conclusion
The last decade of published public health research has not responded to the National Inuit Strategy on Research. Public health research on Inuit remained disease and deficit focused using biomedical perspectives. There were limited Inuit-specific research approaches, and few research initiatives have been translated into promotion programmes. Community engagement was not systematic in qualitative and almost absent in quantitative research. Governance, data sovereignty, and capacity-building remained the weakest links of the research process and outputs on Inuit health. However, participatory research is gaining ground, but it has not yet reached its full potential. A shift from biomedical to decolonised methods is slowly taking place. Academic researchers who have not yet embraced this paradigm shift should make it—and those who have already committed to it should strengthen it.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Geneviève Gore for supporting the authors on the search in the electronic databases.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Stephanie M Topp
Twitter @loubna_belaid
Genevieve Gore We are grateful to Genevieve Gore for supporting the team in the design and the search of the articles in the electronic databases.
Contributors NA and LB designed the study. CS designed the search strategies and searched in the electronic databases. LB screened and synthesised the data. NA, RB and LB interpreted the data. NA and LB drafted the manuscript. The authors approved the manuscript. LB is acting as guarantor.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.