Article Text

Abstract
Introduction Unlike physiological recovery, return to full functional status following childbirth takes longer than 6 weeks (42 days) of the traditionally defined postnatal period, and women with maternal morbidity usually require a longer period to recover. However, the extent to which this morbidity collectively impacts on women’s functional status is not well investigated in Ethiopia. We aim to determine the distinct trajectories and predictors of functional status among postpartum women in Northwest Ethiopia.
Methods Health facility linked community-based follow-up study was conducted in Northwest Ethiopia from October 2020–March 2021. A sample of 779 delivering women was recruited after childbirth and before discharge using the criteria published by the WHO Maternal Morbidity Working Group. Functional status was measured by the Amharic version of the WHO Disability Assessment Schedule 2.0 (WHODAS 2.0) instrument. The Stata Traj package was used to determine trajectories of functional status using group-based multi-trajectory modelling. The multinomial logistic regression model was used to identify predictors of trajectory group membership.
Results A total of 775 women participated at the first, second and third follow-up of the study (6th week, 12th week and 18th week of postpartum period). Three distinct functional status trajectory groups with different longitudinal patterns were identified across the six domains of WHODAS 2.0. Direct and indirect maternal morbidities, lower educational status, poor social support, vaginal delivery, stress, anxiety, posttraumatic stress disorder and fear of childbirth were found to be predictors of poor functioning trajectories.
Conclusion Early diagnosis and treatment of maternal morbidities and mental health problems, developing encouraging strategies for social support and providing health education or counselling for women with less or no education are essential to improve functioning trajectories of postpartum women.
- epidemiology
- public health
- cohort study
Data availability statement
Data are available upon reasonable request. Extra data are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Experience of non-life-threatening maternal morbidities could negatively affect functional status of women after childbirth.
Most previous studies were cross-sectional, providing limited insights into functional status trajectories and its predictors during postpartum period.
What are the new findings?
Women with vaginal delivery, life threatening event of health risk, direct and indirect maternal morbidities were at risk of belonging to poor and very poor functioning trajectories.
Higher stress, anxiety and posttraumatic stress disorder symptom scores, poor social support and fear of childbirth increase the risk of women to belong to poor and very poor functioning trajectories.
Lower educational status, being government employed, housewife and merchant/student in occupation and lower monthly expenditure were statistically associated with poor and very poor functioning trajectories
What do the new findings imply?
Early diagnosis and treatment of maternal morbidities and mental health problems may contribute to increase functioning among postpartum women.
Developing encouraging strategies for social support and providing health education or counselling for women with less or no education may enable to avert functional impairment among women in the postpartum period.
Introduction
Improving maternal health and reducing related mortality have been key concerns of the international community, as evidenced by being part of the third sustainable development goal.1 However, maternal mortality accounts for only a small fraction of the overall burden of poor maternal health and as a result, less attention has been paid to women who survive maternal morbidity conditions, while there has been a considerable attention to preventing women from dying during pregnancy and childbirth.2 3 As there was a success in defining and measuring maternal near-miss events and reduction in maternal mortality, efforts are now focused on measuring non-life-threatening maternal morbidity.4 By defining maternal morbidity as ‘any health condition attributed to and/or complicating pregnancy and childbirth that has a negative impact on the woman’s well-being and/or functioning’ with three dimensions of maternal morbidity matrix, the WHO emphasises the need for comprehensiveness in the evaluation of the maternal morbidity burden.5
Analogous to the long-term consequences of trauma,6 any maternal morbidity that a woman survives during pregnancy, childbirth or the postpartum period is also likely to modify their short-term and long-term functioning.7 8 The WHO International Classification of Functioning, Disability and Health (ICF) describes functioning and disability in an individual in relation to health conditions. It identifies what a person can or cannot do in daily activities and takes organ and/or system functions and body structures into account as well as activity limitations and social participation in the environment.9 The second version of the WHO Disability Assessment Schedule (WHODAS 2.0) was developed to evaluate the functioning and/or disability of an individual to participate in six main life domains, which include cognition, mobility, self-care, getting along with people, life activities and participation irrespective of their medical diagnosis.10
Functional status describes a person’s ability to perform a task or activity in the environment in which they live and is the result of a dynamic interaction between health conditions and contextual factors, integrating the different dimensions of health (individual, biological and social).11 12 Functional status after childbirth is defined as mother’s ability to resume self-care, household, social, community, occupational and infant care activities.13 14
According to the WHO, the postnatal period begins immediately after the birth of the baby and extends up to 6 weeks (42 days) after birth.15 Postpartum recovery is often focused primarily in relation to physiological changes, whereas the complete functional status of the mother after delivery is often overlooked.13 16 Unlike physiological recovery, return to full functional status following childbirth takes longer than 6 weeks and women who experienced maternal morbidity during childbirth usually require a longer period to achieve complete functional status recovery gradually.7 13 16–18 However, while there is increased focus on describing the levels and patterns of maternal morbidity,19–22 the extent to which this morbidity collectively impacts on women’s functional status is not well investigated in Ethiopia.4 In addition, most study designs on the association of maternal morbidity with functional status were cross-sectional, providing limited insights into functional status trajectories during postpartum period.11 13 18 23 24 Therefore, the aim of this study was to identify the distinct trajectories and predictors of functional status from 6th week to 18th week of postpartum period among women in Northwest Ethiopia by using a group based multi-trajectory modelling.
Methods
Study design and study area
The present study was embedded in the health facility linked community based prospective follow-up study conducted in Northwest Ethiopia to determine the effect of maternal morbidities on maternal health related quality of life, functional status and mental health problems. Briefly, the study was conducted in four hospitals of south Gondar zone, Northwest Ethiopia, from 1 October 2020 to 30 March 2021. South Gondar is located at 650 km Northwest from Addis Ababa, the capital city of Ethiopia.
Study population
The study participants were recruited after childbirth and before the time of discharge. Using the criteria published by the WHO Maternal Morbidity Working Group,25 women diagnosed with any of the direct and indirect maternal morbidities were taken as exposed mothers and included in the study. Women without the direct and indirect maternal morbidities were taken as non-exposed mothers. Mothers were asked for consent to participate in the study and after getting their consent and full address, appointments were made at their home to collect the data for the follow-up study.
Eligibility/inclusion criteria
Postpartum women whose age was 15 years and above, with preterm, term or postterm delivery and with live birth, stillbirth or fetal death were included in the study.
Sample size determination
Calculation of the sample size was done by comparing two proportions using Epi-Info software V.7. Accordingly, a minimum sample size of 753 (251 exposed and 502 non-exposed) was calculated by taking 0.05 α, power of 90%, 1.96 OR, 15.4% of mothers with indirect maternal morbidity having least well-functioning quintile (20% of women in the fifth quantile against the first four quantiles of WHODAS total score) as defined by a previous article,11 1:2 ratio of exposed to non-exposed and by adding 10% non-response rate.11 Based on the number of delivering mothers who visited each hospital during the previous 1 year (annual report of each hospital), proportional allocation of the total sample size was carried out to attain the required sample size in each hospital.
Sampling procedure
Identification of exposed and non-exposed mothers was done in four hospitals of south Gondar zone, Northwest Ethiopia, at the time of childbirth and before discharge. Eligible women were those who presented to delivery service in the four hospitals with and without maternal morbidity. The exposed women were those diagnosed with at least one direct or indirect maternal morbidity based on the criteria published by the WHO maternal morbidity working group. All exposed women with direct or indirect maternal morbidities were included in the study and non-exposed women without direct or indirect maternal morbidities were selected by simple random sampling method using their chart number on daily bases. With 1:2 ratio of exposed mothers to non-exposed mothers, this recruitment procedure continued prospectively until the required sample size was fulfilled.
Patient and public involvement
Patients or members of the public were not involved in the design, conduct, reporting or dissemination plans of the research as it was not appropriate to involve.
Definition of the outcome and independent variables
Functional status was taken as the outcome or dependent variable. The primary independent variables were direct and indirect maternal morbidities. Women were taken as exposed if they were diagnosed with any of the direct and indirect maternal morbidities based on the criteria published by the WHO Maternal Morbidity Working Group.25 The diagnosis of direct and indirect maternal morbidity conditions was ascertained by the health professionals working in gynaecology and obstetrics ward of the study hospitals using the clinical diagnosis on every day.
The WHO Maternal Morbidity Working Group has developed three dimensions of maternal morbidity matrix. The first dimension, which includes the direct and indirect maternal morbidity, is composed of 121 conditions, 58 symptoms, 29 signs, 44 investigations and 35 management strategies.26 The second dimension of the matrix measures functional impact and disability related to pregnancy, as defined in the ICF, and is measured using the WHODAS 2.0.10 14 The third dimension measures maternal history focusing on social and health-related characteristics, which include socioeconomic status, pre-existing health conditions and care seeking during pregnancy, which might help to identify the maternal morbidity as well as influence the risk and severity of the morbidity.26
Among the three dimensions of maternal morbidity criteria, developed by WHO Maternal Morbidity Working Group, the direct and indirect maternal morbidities in the first dimension, were used to identify exposed mothers and non-exposed mothers since they are the most common causes of maternal morbidity conditions.25 The third dimension of the morbidity matrix published by the WHO maternal morbidity working group, which measures maternal history focusing on social and health-related characteristics, including socioeconomic status, pre-existing health conditions and care seeking during pregnancy, was treated as secondary exposure variables (confounders) for the outcome variable—functional status. In addition, socio-demographic variables (age, educational status, marital status, religion, ethnicity, occupation and monthly expenditure), residence, obstetric variables (parity, mode of delivery, gestational age at birth, birth weight, birth interval, fetal death, unwanted pregnancies, antenatal care visit and history of abortion) and psychosocial factors (social support, fear of childbirth (FOC), depression and anxiety) were taken as additional exposure variables.
Measurement tools for the variables
Functional impairment
To measure maternal functional status, the 36-item form of the WHODAS 2.0 instrument was used (the 32-item form was used for participants who were unemployed and no longer in school). The WHODAS has been previously validated and used in Ethiopia.24 27–29 The WHODAS 2.0 is designed to measure activity functioning and participation in daily living activities in the previous 30 days. The instrument provides a common way of measuring the impact of any health condition in terms of functioning. It is not targeted to a specific disease, so it can be used to compare disability due to different conditions. The WHODAS 2.0 consists of six domains: cognition (understanding and communication), mobility, self-care, getting along with people, life activities and participation in society. Results provided a profile of functioning within the domains as well as overall score. Total WHODAS 2.0 scores can range from 0 to 100, with higher numbers indicating greater impairment of day-to-day functioning.10
Depression, anxiety and stress
The short version of Depression, Anxiety and Stress Scale–21 items questionnaire was used to measure depression, anxiety and stress. The instrument has 21 items with three domains. Each domain comprises seven items assessing symptoms of depression, anxiety and stress. In this study, a score of ≥10 was considered for a mother to have a symptom of depression. A cut-off score of ≥8 was considered to have symptoms of anxiety and a score of ≥15 was considered to have symptoms of stress. This instrument was also validated and used previously in Ethiopia.30 31
Fear of childbirth
The Wijma Delivery Expectation/Experience Questionnaire (W-DEQ) was used to measure FOC. The W-DEQ has been designed specially to measure FOC operationalised by the cognitive appraisal of the delivery. This 33-item rating scale has a 6-point Likert scale as a response format, ranging from ‘not at all’ (0) to ‘extremely’ (=5), yielding a score range between 0 and 165. The W-DEQ was validated and previously used in Ethiopia, and its internal consistency and split-half reliability were checked with the Cronbach’s α score of 0.932.32 33 A score of ≥85 was considered to have FOC for this study.32 33
Social support
The 3-items Oslo Social Support Scale with scores ranging from 3 to 14 was used to measure social support. The social support scores were categorised into poor or no social support for scores less than 9. Scores between 9 and 14 were considered moderate to strong support and merged together as ‘yes’ for social support. The 3-items Oslo Social Support Scale was validated and previously used in Ethiopia.34–36
Posttraumatic stress disorder
The Posttraumatic Stress Disorder (PTSD) Checklist for DSM-5 (PCL-5) was used to measure PTSD. The instrument contains 20 items, including 2 new PTSD symptoms (compared with the PCL for DSM-IV): blame, negative emotions and reckless or self-destructive behaviour.37 A total-symptom score of 0–80 can be obtained by summing the items. A score of 31–33 is optimal to determine PTSD symptoms and a score of ≥33 is recommended when further psychometric testing is not available.38 39 Therefore, a score of ≥33 was considered to have symptoms of PTSD for this study. The instrument was validated and used previously in Ethiopia.39
Stressful life events
The List of Threatening Experiences (LTE) was used to measure experience of stressful life events during the 6-month period.40 The 12 items were categorised into 5 categories, namely, health risks, loss of a loved one, relationship difficulties, income instability and legal problems.41 The LTE-12 has been validated and used in population level studies in Ethiopia.42 43
Data collection and quality control
Based on the criteria published by the WHO maternal morbidity working group, the direct and indirect maternal morbidities were diagnosed and collected by health professionals working in the gynaecology and obstetrics wards of four hospitals in the study area. The questionnaires consisted of a patient interview and a record review. The interview was on socioeconomic status, medical and obstetric history and clinical symptoms. In addition, physical examination has been done by a healthcare professional in order to evaluate clinical signs. The record review was intended to extract information on selected laboratory tests and results for haemoglobin, HIV, malaria (rapid diagnostic test or smear) and random blood sugar (glucometer).
Baseline questionnaires were administered by health professionals working in gynaecology and obstetrics ward of each hospital before the mothers were discharged. The 36-item WHODAS 2.0 was administered by health extension workers at the first, second and third home visit (6th week, 12th week and 18th week of postpartum period). Training was given for data collectors and supervision was done by the principal investigator. As part of the training process in each study area, data collectors carefully reviewed each question and conducted pretest in the study area before the study commences since women who gave birth before the study period were not eligible to be included in the actual data collection. The investigator and data collectors have checked the final version of the questionnaire and update as required based on the pretest.
Data processing and analysis
Group-based multi-trajectory modelling was carried out with the Stata Traj package to identify latent clusters of mothers with similar longitudinal functioning trajectories over time across the six domains of WHODAS 2.0: cognitive, mobility, self-care, getting along with people, life activities and participation in society.44 This method assumes that the overall population is made up of distinct, but unobserved (ie, latent), subpopulations with different behavioural phenotypes and then uses the observed data to estimate both the trajectories of these groups and how they are distributed in the population. A distinct trajectory consists of a group of individuals who share a common underlying pattern of functional status change over time.44
Group-based multi-trajectory modelling, a generalisation of univariate group-based trajectory modelling to multiple outcomes,45 aims to identify clusters of individuals with similar trajectories across multiple indicators of an outcome of interest (eg, WHODAS 2.0: six domains). Hence, the latent trajectory subgroups are derived based on multiple trajectories of the individual domains of WHODAS 2.0, and individuals have the same group membership across all the domains. The advantage of multi-trajectory approach is particularly that it incorporates the interrelationships among the WHODAS 2.0 domains, leading to improved clustering of trajectories.45 Trajectories of the overall WHODAS-36 score were also determined by using a group-based trajectory modelling.44
Censored normal finite mixture model was used to estimate trajectories of functional status over the postpartum period (at 6th week, 12th week and 18th week of postpartum period for active data collection) in this cohort of postpartum women. The identification process of appropriate group trajectories was based on the selection and reporting procedures outlined by Nagin and Odgers.46 Statistically, group-based trajectory models use maximum likelihood estimation to estimate both the trajectory of each group (modelled as a function of time using flexible polynomials) and the expected population-level distribution of each group that creates the best fit for the observed data.46 47
Since the number of groups and the order of the trajectory polynomials (ie, linear, quadratic and cubic) are not actually known a priori (but must be prespecified when estimating a model), we systematically tested a series of model specifications. This was done first by varying the number of groups and then the order of the trajectory polynomials in order to select the model most optimised for fit and parsimony.45 46 In the model selection process, the Bayesian Information Criterion (BIC) was used to determine the best model underlying the group selection and functional form. The closer the negative BIC value is to 0, the better is the fit of the model. A difference in the BIC value of at least 10 points between two models indicates that the model with the lower BIC value has a better model fit.46
We have also assessed the posterior probabilities of group membership and required that average posterior probability reached 0.70 or higher to be a distinct classification group. Posterior probabilities represent the average probability that the trajectory group each participant was assigned to is the most appropriate group selection and model fit. Entropy, a statistic that ranges from 0.00 to 1.00, which is a summary indicator of the conditional probabilities of individuals’ group membership, has been also used. High values of entropy (>0.80) indicate that individuals are classified with confidence (ie, the model is generally pretty sure that persons belong to a particular class) and there is adequate separation between the latent classes.48 Additionally, we required at least 10% of the sample to be present in a particular group and all trajectories were distinct from one another by visual assessment of trajectory figures looking for non-overlapping confidence intervals.46 The labelling of each trajectory was based on a previous research work.49
Finally, we have used multinomial logistic regression model to identify factors that were associated with probability of group (trajectory) membership. First, unadjusted bivariable associations between each predictor and trajectory membership were tested in order to identify predictors having a p value of ≤0.2 to enter into the multivariable multinomial logistic regression. Next, multivariable multinomial logistic regression model was fitted to determine factors associated with membership to functional status trajectories. We report the OR of group membership with a 95% CI and a p value of ≤0.05 for statistical significance. Stata V.16 and IBM SPSS Statistics V.26.0 were used for the statistical analyses.
Results
At baseline a total of 779 postpartum mothers were included in this postpartum cohort study. Nearly all (that is, 99.5%) of the mothers participated at the first, second and third follow-up of the study (6th week, 12th week and 18th week of postpartum period). Four mothers were lost to follow-up because of changing their living place and going out of the study area. A total of 775 mothers who completed all the three measurements with functional status data were included in the analyses. The mean age of the study participants was 26.3 (4.36). Almost all of them (774; 99.9%) were Amhara by ethnicity and 742 (95.7%) were followers of orthodox Christianity (see table 1).
Socio-demographic characteristics of postpartum women by functional status trajectory groups across the six domains of WHODAS 2.0 in Northwest Ethiopia, 2021
Overall and domain scores for WHODAS 2.0 by maternal morbidity status
The mean and SD for the overall and domain scores of the WHODAS 2.0 were evaluated by maternal morbidity status. The overall functional status mean score was significantly higher among women with direct maternal morbidities (p<0.01) and with indirect maternal morbidities (p<0.01) than among those with no morbidity throughout the follow-up period. Mean domain scores were significantly higher in women with direct and indirect maternal morbidities for all domains throughout the follow-up period. But, the mean of mobility domain was not significantly different at the second and third follow-up periods. In addition, for the life activity and self-care domains, the difference disappears at the 18th week following childbirth and mean of the participation domain was not significantly different at the third follow-up period in women with and without direct maternal morbidities (see table 2). Results for further comparisons of the overall and domain scores of the WHODAS 2.0 by various maternal morbidity status can be found in online supplemental tables 1–4.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Mean and SD for WHODAS 2.0 domain and total scores by direct and indirect maternal morbidity statuses among postpartum women in Northwest Ethiopia, 2021
Maternal morbidity, obstetrics and psychosocial variables by trajectory group
Table 3 describes the comparison of maternal morbidity, obstetrics and psychosocial variables across trajectory groups. Out of 252 (32.5%) mothers with direct maternal morbidity, 52 (6.7%), 133 (17.2%) and 67 (8.6%) of them were in the trajectory group of persistently well functioning, poor functioning with recovery and very poor functioning with recovery, respectively.
Maternal morbidity, obstetrics and psychosocial variables by functional status trajectory groups across the domains of WHODAS 2.0 in Northwest Ethiopia, 2021
Out of women with FOC, 58 (7.5%), 56 (7.2%) and 131 (16.9%) of them also belongs to the trajectory group of persistently well functioning, poor functioning with recovery and very poor functioning with recovery, respectively (see table 3).
Identification of the overall and domain-specific functional status trajectories
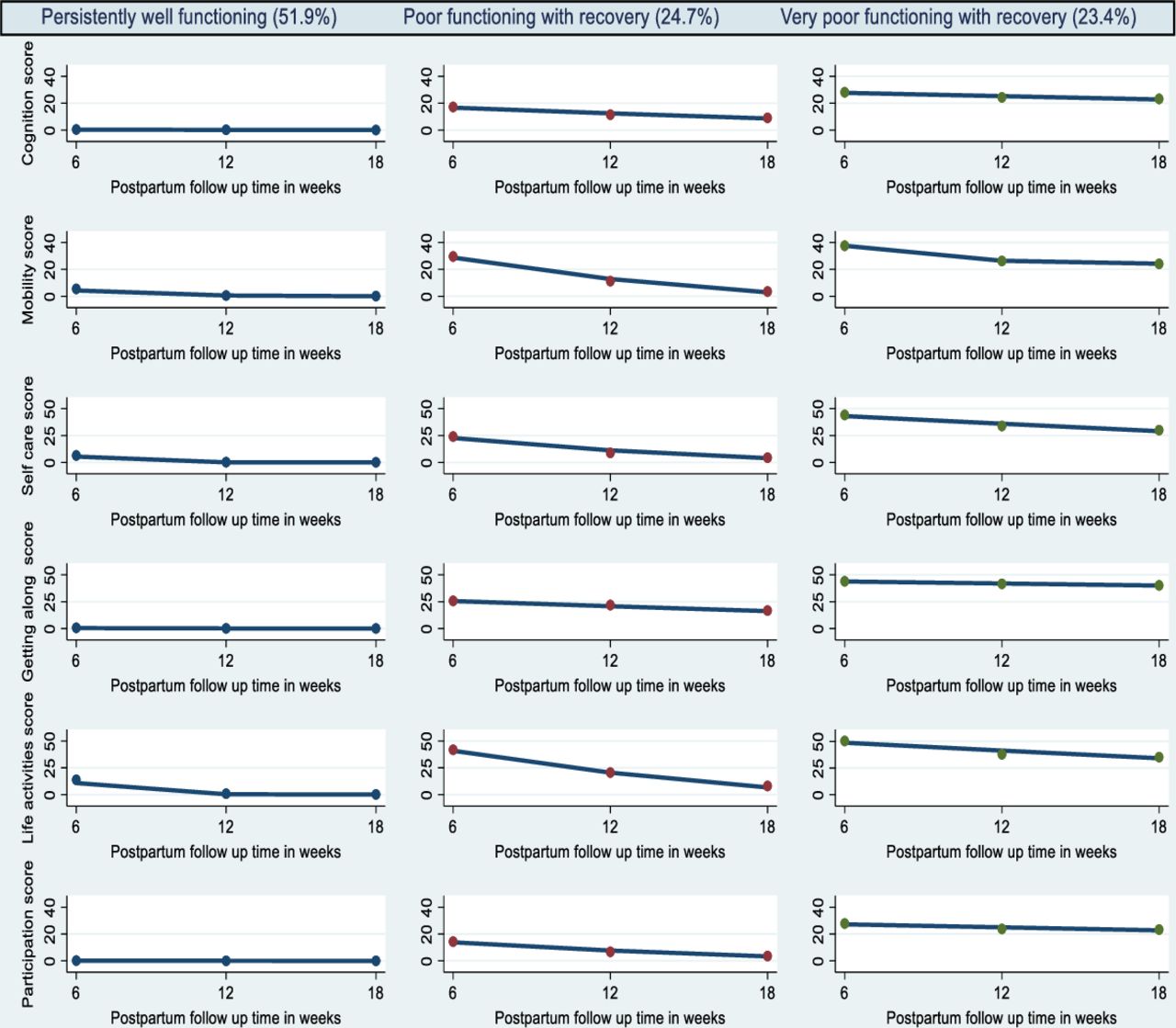
As indicated in table 4, the group-based multi-trajectory analysis indicates that the three latent trajectory class best fitted the data across the six domains of WHODAS 2.0. The three trajectories of functional status were labelled as persistently well functioning, poor functioning with recovery and very poor functioning with recovery.
Fit indices for group-based trajectory and multi-trajectory modelling of WHODAS 2.0 overall and domain scores among postpartum women in Northwest Ethiopia, 2021
The persistently well-functioning group with 52.0% of the total cohort had consistently (stable) high functioning patterns in all the six domains of WHODAS 2.0 throughout the follow-up period.
The poor functioning with recovery trajectory group (24.7% of the cohort) consisted of postpartum women with poor functional status across the six domains. This trajectory group exhibited decreasing patterns (recovery) on trajectories of cognitive functioning, mobility functioning, self-care functioning, life activities functioning and participation functioning domains but relatively flat patterns on getting along with people functioning over the follow-up period.
The third trajectory, labelled as very poor functioning with recovery, consisted of 23.4% of postpartum women with very poor functional status across the six domains. This trajectory group exhibited decreasing patterns (recovery) on trajectories of mobility functioning, self-care functioning and life activities functioning but relatively flat patterns on cognitive functioning, getting along with people functioning and participation functioning domains over the follow-up period (see figure 1).
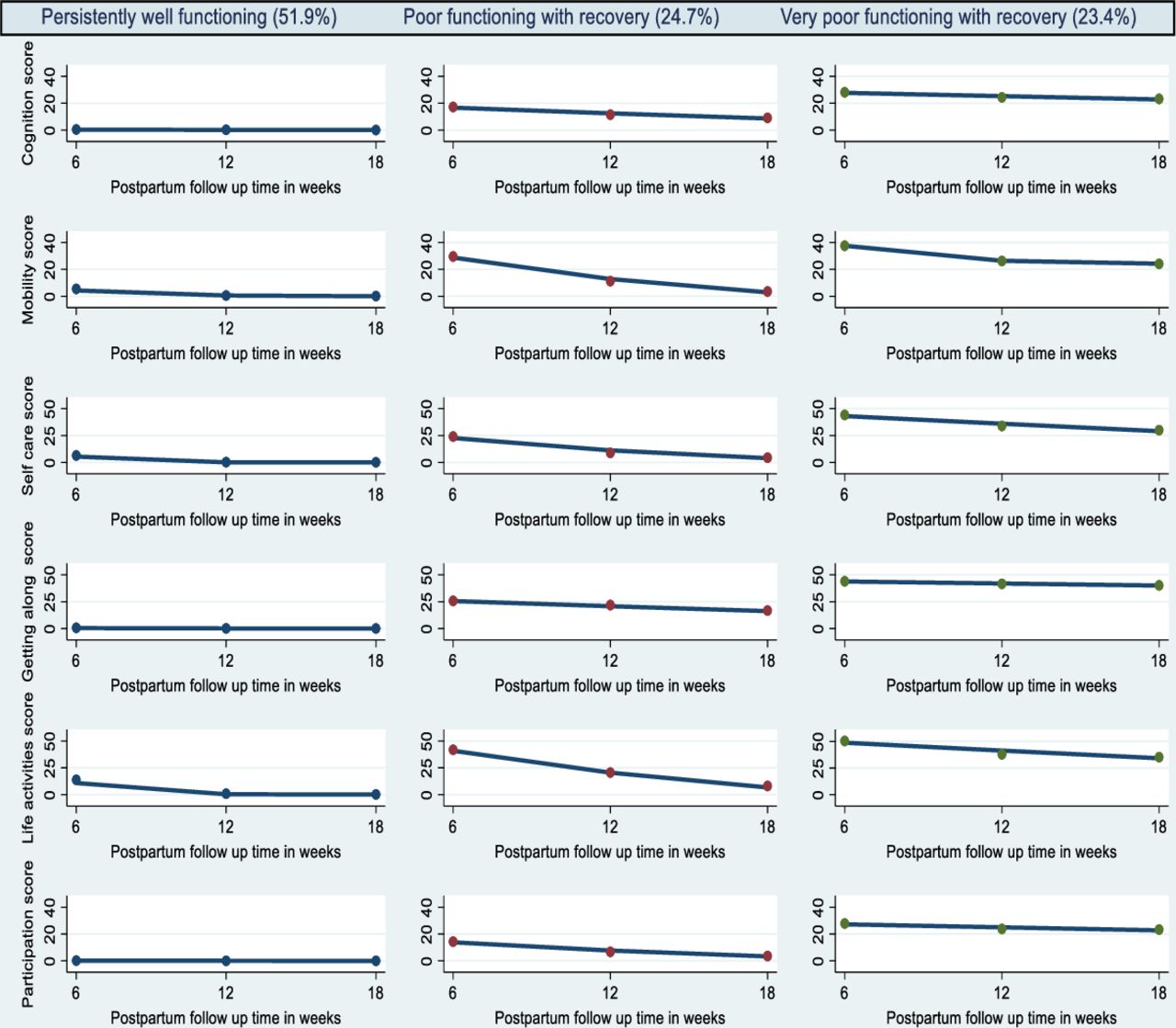
Trajectories of WHO Disability Assessment Schedule 2.0 domains functional status in postpartum women, Northwest Ethiopia, 2021.
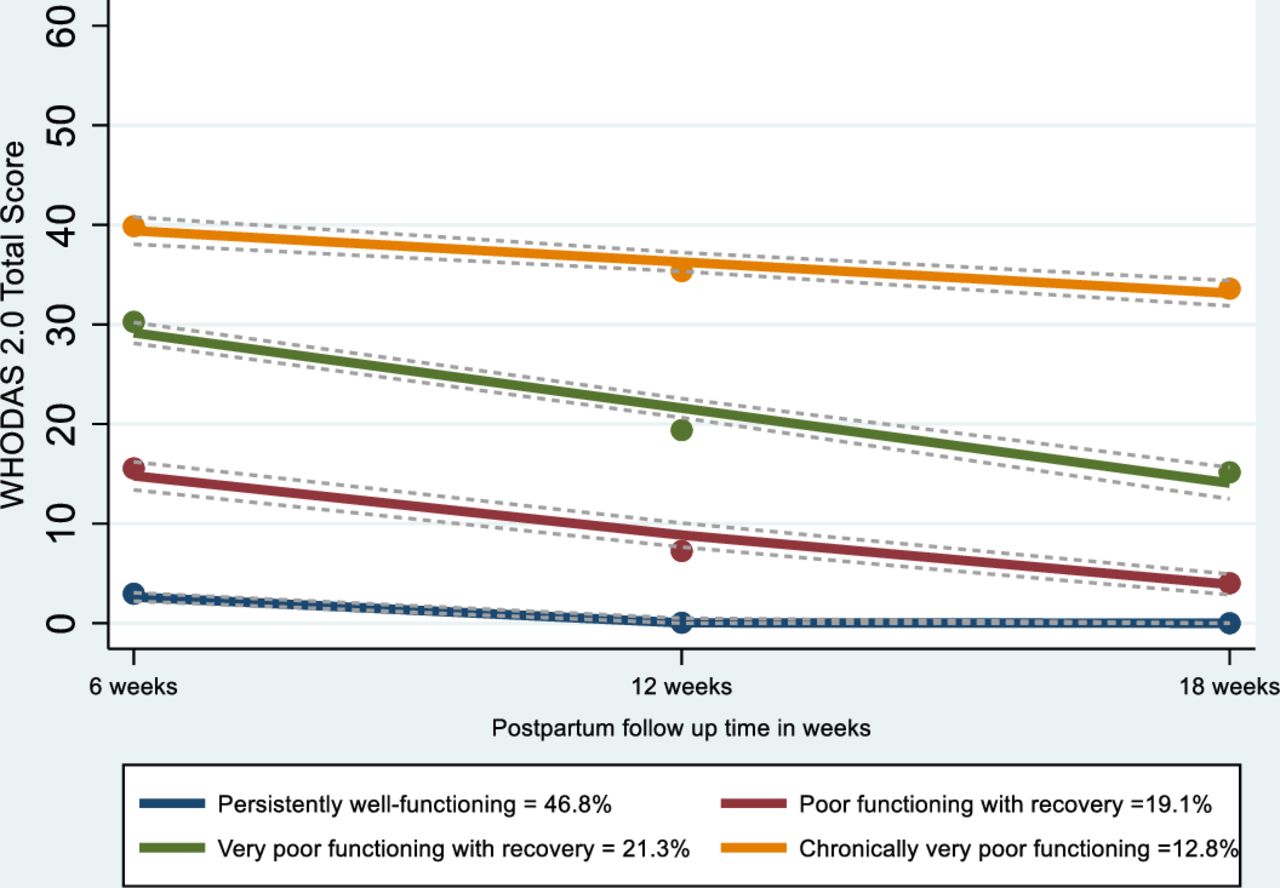
For the overall functional status, four trajectories best fitted the data and were labelled as persistently well functioning, poor functioning with recovery, very poor functioning with recovery and chronically very poor functioning (see table 4). The patterns of persistently well functioning, poor functioning with recovery and very poor functioning with recovery trajectory groups of the overall functional status were similar with the domains’ functional status trajectory group patterns during the follow-up period. However, the fourth trajectory of the overall functional status labelled as chronically very poor functioning exhibited relatively stable patterns of higher functional status scores (worsen disability) throughout the follow-up period (see figure 2).
{kind=link}
{kind=link}
Trajectories of WHODAS 2.0 overall functional status in postpartum women, Northwest Ethiopia, 2021. WHODAS 2.0, WHO Disability Assessment Schedule 2.0.
Predictors of functional status trajectory group membership across the domains of WHODAS 2.0
Predictors of the functional status trajectory group membership, which were found to be statistically significant in the multinomial logistic regression analysis, were presented in table 5.
Significant predictors of functional status trajectories across the domains of WHODAS-36 in postpartum women in Northwest Ethiopia, 2021
Women with a higher anxiety and PTSD score were more likely to belong to the latent class with poor and very poor functioning trajectory compared with participants in the persistently well-functioning trajectory. Similarly, mothers with higher stress score were 1.2 times more likely to belong to the latent class with poor functioning trajectory (OR=1.19; 95% CI 1.02 to 1.39) compared with participants in the persistently well-functioning trajectory.
Mothers with direct maternal morbidity were 7.0 and 6.7 times more likely to belong to the poor and very poor functioning trajectory, respectively (poor: OR=6.98; 95% CI 1.41 to 34.52; very poor: OR=6.65; 95% CI 1.05 to 42.14), relative to the persistently well-functioning trajectory. Also, mothers with indirect maternal morbidity were 10.2 and 7.4 times more likely to belong to the poor and very poor functioning trajectory, respectively (poor: OR=10.15; 95% CI 3.04 to 33.87; very poor: OR=7.42; 95% CI 1.83 to 30.13), relative to the persistently well-functioning trajectory.
Participants with FOC (OR=6.07; 95% CI 2.74 to 13.46) were more likely to belong to the very poor functioning trajectory compared with participants in the persistently well-functioning trajectory. In addition, participants with vaginal delivery (OR=2.57; 95% CI 1.06 to 6.23) were more likely to belong to the poor functioning trajectory compared with participants in the persistently well-functioning trajectory. Finally, mothers with poor social support were 7.8 and 11.3 times more likely to belong to the poor and very poor functioning trajectory, respectively (poor: OR=7.76; 95% CI 3.90 to 15.43; very poor: OR=11.34; 95% CI 5.20 to 24.72), compared with participants in the persistently well-functioning trajectory.
Predictors of WHODAS 2.0 overall functional status trajectory membership
As indicated in table 6, women with higher PTSD score were more likely to belong to the latent class with poor, very poor and chronically very poor functioning trajectory compared with participants in the persistently well-functioning trajectory. Mothers with direct maternal morbidity were 5.6 and 8.1 times more likely to belong to the poor and very poor functioning trajectory, respectively (poor: OR=5.56; 95% CI 1.54 to 20.13; very poor: OR=8.09; 95% CI 1.79 to 36.45), relative to the persistently well-functioning trajectory. Also, mothers with indirect maternal morbidity were 10.9 and 7.3 times more likely to belong to the poor and very poor functioning trajectory, respectively (poor: OR=10.91; 95% CI 3.66 to 32.59; very poor: OR=7.34; 95% CI 2.31 to 23.37), relative to the persistently well-functioning trajectory. In addition, participants with vaginal delivery (OR=2.16; 95% CI 1.06 to 4.42) were more likely to belong to the poor functioning trajectory compared with participants in the persistently well-functioning trajectory. Mothers with poor social support were 3.3, 10.8 and 5.6 times more likely to belong to the poor, very poor and chronically very poor functioning trajectory, respectively (poor: OR=3.31; 95% CI 1.87 to 5.86; very poor: OR=10.83; 95% CI 5.44 to 21.55; chronically very poor: OR=5.56; 95% CI 2.30 to 13.44), compared with participants in the persistently well-functioning trajectory.
Significant predictors of WHODAS 2.0 overall functional status trajectories in postpartum women in Northwest Ethiopia, 2021
Discussion
Our study found that both direct and indirect maternal morbidities negatively impacted the overall postpartum functioning at the 6th week, 12th week and 18th week of postpartum period. Women with direct maternal morbidities (gestational hypertension, pre-eclampsia, postpartum haemorrhage, perineal tear and infection) had a significantly higher mean score (23.73, 13.43 and 10.08) at the first, second and third follow-up periods, respectively, than women with no direct maternal morbidities (12.13, 8.44 and 7.46), respectively, at the same follow-up periods. Similarly, women with indirect maternal morbidities (tuberculosis, asthma, pneumonia, hypertension, anaemia, diabetes mellitus and HIV/AIDS) had a significantly higher mean score (25.48, 14.22 and 10.54) at the first, second and third follow-up periods, respectively, than women with no indirect maternal morbidities (12.37, 8.53 and 7.47), respectively, at the same follow-up periods. The mean scores of this study were comparable to the results of two studies using WHODAS 2.0 among postpartum women in Brazil reporting the overall functioning mean score of 19.04 and 19.00 among women with severe maternal morbidities.18 23
In this study, we also found that women who experienced direct and indirect maternal morbidities had a lower domain-specific functional ability throughout the follow-up period compared with women without direct and indirect maternal morbidities. But, the difference for the mean of mobility domain disappeared at the 12th week and 18th week of postpartum and for the life activity and self-care domains; the difference disappears at the 18th week following childbirth, while the mean difference of participation domain between women with and without direct maternal morbidity also disappears at the 18th week of postpartum period. Another study, conducted in Malaysia using a different psychometric tool, reported an increase in maternal functional ability in subdomains of household, social participation and self-care activities from 1-month to 6 months postpartum, which is in congruent with our finding.13 This study also reported that maternal morbidity conditions did not adversely affect multiple domains of functioning at 6 months indicating that gradual resumption of the activities reflects the normal adjustments of the mothers.13
By using a group-based multi-trajectory analyses of the longitudinal data across the six domains of the WHODAS 2.0, we have also identified three distinct trajectory groups with different longitudinal patterns. The first group, which consists of mothers with persistently well-functioning group across the six domains, exhibited consistently (stable) high functioning patterns in all domains throughout the follow-up period. Mothers in the poor functioning with recovery group exhibited substantial improvements on trajectories of cognitive, mobility, self-care, life activities and participation functioning domains but relatively flat patterns on getting along with people functioning over the follow-up period. Similarly, mothers in the very poor functioning with recovery group demonstrated improvements on trajectories of mobility, self-care and life activities functioning but relatively flat patterns on cognitive, getting along with people and participation functioning domains over the follow-up period.
In this study, life threatening event of health risk, direct maternal morbidities (gestational hypertension, pre-eclampsia, eclampsia, postpartum haemorrhage, perineal tear and infection) and indirect maternal morbidities (tuberculosis, asthma, pneumonia, hypertension, anaemia, diabetes mellitus and HIV/AIDS) were found to be independent risk factors for women to belong to the poor and very poor functioning with recovery trajectories relative to the persistently well-functioning trajectory. Our finding is consistent with previous studies showing women with a clinically diagnosed direct and indirect maternal morbidity were generally more likely to have a lower level of functioning compared with those with no condition.11 18 Another study from Malaysia also showed that women who experienced severe morbidity had lower overall functional ability at 1 month postpartum compared with women without severe morbidity and that the difference between the two groups had disappeared by 6 months postpartum, although most women had not achieved full functional status by this time.13
Among the direct maternal morbidities, hypertension was found to be related to poor functioning in a study from Brazil, as expressed in higher WHODAS- 36 scores.23 It was speculated that women with hypertension may experience acute complications (placental abruption, pulmonary oedema and stroke), which could have an impact on functionality.23 There is also an increased risk of a medically indicated preterm birth among women with hypertension and as a result, women may experience the need to deal with the consequences of premature birth.13 23 In one study, mothers of preterm babies were reported to have higher levels of fatigue in the morning at 6 weeks postpartum because of higher physical demands for caring for preterm babies and fragmented sleep.50
A prospective cohort study in Burkina Faso also showed that women with severe obstetric complications (anaemia, hypertension, haemorrhage, dystocia and infection) generally reported feeling worse than women with uncomplicated deliveries.51 It was suggested that the different patterns of health problems may affect women at different times following severe obstetric complications.51
With a simple functional health status assessment based on three questions on the ability of the women to work, care for their children and perform general household tasks, another study in USA also reported a similar finding that health problems such as fatigue, headaches, backache, abdominal and vaginal pain at 9–12 months postpartum were to be consistently and significantly related to functional health status.52 This study reported increased functional limitation with increased severity of health problems among the women.52
Higher anxiety and PTSD symptom scores were found to be significant predictors of poor and very poor functioning trajectory group membership relative to the well-functioning trajectory. Similarly, while women with higher stress symptom scores were at risk of belonging to the poor functioning trajectory group, women with FOC were at risk of belonging to the very poor functioning trajectory compared with the well-functioning group. Previous researches found a similar relationship between mental health disorders and functional status. The WHO pilot study in Jamaica, Kenya and Malawi found that anxiety and depression were associated with a significant loss of functioning.11 Other studies conducted in the USA and Iran reported that maternal functional status had an inverse significant relationship with postpartum anxiety.53 54
The possible reason might be due to the fact that mental health disorders can lead to a person’s lack of interest in everyday activities, lack of energy to conduct routine activities and manage tasks, and general discomfort. As a result, anxiety and other mental health problems during the postpartum period can lead to the impaired adjustment of mothers, delay their recovery and impede the actions that are necessary to maintain their health resulting in decreased maternal functional status.16 54 This finding points to the importance of screening and treating anxiety and PTSD during postpartum period and continuing to follow mothers postnatally. In addition, our findings suggest that decreasing anxiety and PTSD during postpartum period may be one strategy for closing the functional impairment gap and increasing maternal capability to return to regular social and work activities.
In our study, relative to the well-functioning trajectory, women with lower education level were more likely to belong to the very poor functional trajectory group as compared with women with higher education status. This is in line with the results of previous studies, which reported that high level of education was associated with greater functional status.16 49 55 This might be due to the fact that higher education may enhance resilience and significantly increase likelihood of recovery. Therefore, this finding may be useful when targeting interventions and follow-ups, as women with less or no education may need training packages to convey information to promote their awareness about functional status, thereby improving maternal functional status in the postpartum period.
In addition, being government employed, merchant/student and housewife in occupation were the predictors of belonging to poor and very poor functioning trajectory group relative to the well-functioning trajectory. This might be due to work-related stress, as it has been argued that women who return to work may find their job more challenging with additional task of baby care.56 This increased responsibility and workload might have affected their functional status trajectories negatively.
In our study, having lower monthly expenditure and income instability were found to be protective of belonging to the poor functional status trajectory as compared with women with higher monthly expenditure. However, this result is not in agreement with the majority of the scientific literature, which indicates that increased resources are protective.50 55 Another evidence in Iran reported similar finding with our study that having a low to moderate income was associated with higher maternal functioning.54 The association of lower monthly expenditure with less likelihood of belonging to the poor functional status in the present study might be because of women in this social class may engage more in physical works in order to afford their income. Thus, the more engagement in physical work might have improved their functional status as it has been reported in an evidence that women who are highly physically active at 6 weeks and 12 weeks postpartum were more likely to have higher functional status.57 Another possible explanation might be since infant care, breastfeeding practices and the use of neonatal care standards to improve neonatal and maternal healthcare practices are provided for mothers in health facilities and home visits through health extension programme for free; visiting public health facilities and receiving all these services may lead to better maternal functioning in women with less monthly expenditure.54 58
The results of this study also indicated that poor social support can lead a woman to belong to the poor and very poor functioning trajectories relative to the well-functioning trajectory, which is consistent with previous studies.53 54 Receiving social support is a powerful predictor for postpartum maternal health and functioning since positive social environment and support in the form of provision of resources and assurance can act as a stress buffering mechanism, protecting the mental health and functional status of mothers.54 Considering the fact that receiving support is a predictor of maternal functioning, interventions of social support should be included in programmes for improvement of maternal functioning.
Although other studies have shown different results,59 60 the present study observed that women who gave birth with vaginal delivery were more likely to belong to the poor functional trajectory group compared with those who had a caesarean section. Similar finding was obtained in a study from Turkey that women who had a caesarean section had better functional status in the area of household activities at 6th month of postpartum period, compared with those who gave normal birth.61 This might be due to the fact that women who had caesarean delivery may have received more family support because of their surgery than those women with vaginal delivery. Another justification might be as FOC is linked to vaginal birth,62 women who had vaginal birth might have experienced high levels of FOC, which reduces their level of self-confidence, and in turn decreases their functional status.63
However, other studies which were conducted in Brazil and Turkey found that women who gave birth with vaginal delivery regained their functional status faster than those who had a caesarean section.59 60 This is also true that the pain experienced in the postpartum period because of caesarean section may restrict the daily activities related to mobility, self-care and newborn care.59
Strength and limitation
Strength of this study is the use of group-based multi-trajectory analysis to identify subgroups of longitudinal functional status trajectories based on multiple WHODAS 2.0 domains. Group-based multi-trajectory modelling enables the identification of the distinct underlying trajectories and their predictors. Understanding these distinct trajectory subgroups and the risk factors associated with each trajectory can help to provide prognostic information for mothers and to inform the design of targeted risk factors prevention for women in the postpartum period.
This study is not without limitations. Since the postnatal questionnaire was completed by women around 6th week, 12th week and 18th week after childbirth, recall bias might be one possible limitation of this study. At the time of data collection, since employee mothers were on maternity leave after childbirth, we were unable to assess the occupational subdomain of the functional status questionnaire. Additionally, in Bayesian analysis, there is no correct way to choose a prior and it does not tell us how to select a prior. As a result, if we do not proceed with caution, a misleading result could be generated. However, to minimise this limitation, a priori we hypothesised the labelling and maximum number of trajectory groups based on the suggestion of previous research works on functional status trajectories in postpartum women. Moreover, for multivariate analysis to give meaningful results, they need a large sample of data; otherwise, the results would be meaningless due to high standard errors. Even though the CIs for some variables were relatively wider, our sample size was relatively large enough (775) to minimise the standard errors, which could make the results meaningless for a small sample size in multivariate analysis.
Conclusion
Three distinct functional status trajectory groups with different longitudinal patterns were identified across the six domains of WHODAS 2.0. Life-threatening event of health risk, direct and indirect maternal morbidities was found to be predictors of poor functioning trajectories. Therefore, early diagnosis and treatment of these morbidities are essential to avert the decrease in functioning trajectories of postpartum women.
Lower educational status, poor social support, being government employed, housewife and merchant/student in occupation, vaginal delivery and lower monthly expenditure were also identified to be predictors of poor functioning trajectory. Hence, health professionals should target these issues when developing health interventions or provide health education to help women to cope with these conditions so as to improve their functional status trajectories. Particularly, social support should be encouraged especially for those women who are employed, housewife and merchant/student so as to reduce workload and improve their functional status trajectory. Women with less or no education may need training packages to convey information to promote their awareness about functional status, thereby improving maternal functional status in the postpartum period.
In addition, stress, anxiety, PTSD and FOC were predictors of poor functional status trajectory group membership among the identified latent trajectory groups. Therefore, healthcare providers should be aware of the treatment of postpartum women with mental health problems and providing health education or counselling in order to reduce the potential consequences on maternal functioning.
Data availability statement
Data are available upon reasonable request. Extra data are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Institutional Review Board of Bahir Dar University (reference number: 00225/2020). Participants gave informed consent to participate in the study before taking part. In addition to informed consent from their care givers, assent was also obtained from teenage mothers whose age is less than 18 years, to participate in the study. Using codes, passwords and limiting access to the data only for the investigators were the measures taken to ensure the confidentiality of the data. Data collectors read out and assisted participants to fill out the consent form if participants were unable to read and write.
Acknowledgments
The authors would like to acknowledge the heads of Debre Tabor Hospital, Addis Zemen Hospital, Estie Hospital and Nefas Mewcha Hospital for their cooperation on the data collection of this study. The authors are also grateful to the study participants for their dedicated time and volunteer participation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seema Biswas
Contributors MTM was investigator, involved in proposal writing, designing, recruitment and training of supervisors and data collectors and did analysis and write-up in all stages of the project implementation. GDA and TA contributed in the designing of the methodology, were lead investigators and were involved in designing of project proposal, design of questionnaires, supervision, in giving comments in the progress of the project and final approval of the paper. All authors read and approved the final manuscript.
Funding This study was supported by Bahir Dar University and Debre Tabor University.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.