Article Text

Abstract
Introduction The Zambian Ministry of Health (MoH) issued COVID-19 mitigation guidance for HIV care immediately after the first COVID-19 case was confirmed in Zambia on 18 March 2020. The Centre for Infectious Disease Research in Zambia implemented MoH guidance by: 1) extending antiretroviral therapy (ART) refill duration to 6 multi-month dispensation (6MMD) and 2) task-shifting communication and mobilisation of those in HIV care to collect their next ART refill early. We assessed the impact of COVID-19 mitigation guidance on HIV care 3 months before and after guidance implementation.
Methods We reviewed all ART pharmacy visit data in the national HIV medical record for PLHIV in care having ≥1 visit between 1 January—30 June 2020 at 59 HIV care facilities in Lusaka Province, Zambia. We undertook a before–after evaluation using mixed-effects Poisson regression to examine predictors and marginal probability of early clinic return (pharmacy visit >7 days before next appointment), proportion of late visit (>7 days late for next appointment) and probability of receiving a 6MMD ART refill.
Results A total of 101 371 individuals (64% female, median age 39) with 130 486 pharmacy visits were included in the analysis. We observed a significant increase in the adjusted prevalence ratio (4.63; 95% CI 4.45 to 4.82) of early return before compared with after guidance implementation. Receipt of 6MMD increased from a weekly mean of 47.9% (95% CI 46.6% to 49.2%) before to 73.4% (95% CI 72.0% to 74.9%) after guidance implementation. The proportion of late visits (8–89 days late) was significantly higher before (18.8%, 95% CI17.2%to20.2%) compared with after (15.1%, 95% CI13.8%to16.4%) guidance implementation .
Conclusions Timely issuance and implementation of COVID-19 mitigation guidance involving task-shifted patient communication and mobilisation alongside 6MMD significantly increased early return to ART clinic, potentially reducing interruptions in HIV care during a global public health emergency.
- HIV
- COVID-19
- epidemiology
- cohort study
Data availability statement
Data are available on reasonable request. The data used to prepare these analyses are not public and are part of the Zambian national electronic HIV medical record data, and as such, are only potentially available on request and with permission from the Zambian Ministry of Health (suggested contact: info@moh.gov.zm). Access to data is subject to restrictions including, but not limited to, deidentification and suppression of small cell sizes.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Limited published reports have described the impact of implementing COVID-19 mitigation efforts for people living with HIV (PLHIV), such as multimonth dispensation (MMD) of antiretroviral therapy (ART), on HIV care during the pandemic in sub-Saharan Africa. Increased frequency of missed visits have been observed in South Africa associated with COVID-19 lockdowns and restrictions. In well-resourced settings, COVID-19 has been associated with unique financial and health stressors, especially among those in HIV care.
What are the new findings?
We present here the impact of implementing national COVID-19 mitigation guidance using 6-month MMD and task-shifting mobilisation of PLHIV receiving ART in Lusaka, Zambia. We observed that individuals in care returned to ART clinic early, effectively reducing clinic patient volumes and ensuring ART possession in preparation for initial waves of COVID-19 in Zambia. Proactive patient communication and 6-month ART scripting resulted in increased early return to ART clinic and potential reduction of interruptions in HIV care during a global public health emergency.
What do the new findings imply?
Quickly responding and implementing COVID-19 mitigation guidance for PLHIV using a combination of MMD and community mobilisation can attenuate the negative effects of external public health shocks, such as the COVID-19 pandemic.
Introduction
The global COVID-19 pandemic has redirected public health funding to fight SARS-CoV-2, running the risk of undermining hard won gains made towards ending the HIV epidemic in sub-Saharan Africa (SSA).1 The COVID-19 pandemic has further stressed already strained health systems and generated widespread concerns that service disruptions will compromise critical health functions addressing tuberculosis (TB), HIV and malaria, among other priority conditions, especially in resource-limited settings.2 3 Health systems have been required to rapidly implement modified supply chain systems and health worker deployments, observing new public health protocols for mitigating the deleterious effects of COVID-19. On 24 March 2020, 6 days after the first confirmed COVID-19 case in Zambia, the national Ministry of Health (MoH) issued COVID-19 mitigation guidance to HIV care facilities to prevent treatment interruption for people living with HIV (PLHIV).2–4 This context provides an opportunity to assess the flexibility, nimbleness and resilience of health systems to sustain HIV treatment services in the context of external disruptions from the COVID-19 pandemic.
To date, relatively little data have emerged from high-burden HIV settings, including those in SSA, to demonstrate the effects of the COVID-19 pandemic on the functioning of HIV treatment programmes. In South Africa, it has been observed that 19.6% of those in HIV care missed an HIV care appointment during the national lockdown beginning 24 March 2020.5 There is also evidence that PLHIV are at increased risk of COVID-19 related morbidity and mortality, highlighting the critical importance of minimising COVID-19 exposure in this population.6 Though there has been much modelling to predict how the pandemic will impact PLHIV, there has been commensurately little empirical data to show how HIV treatment programmes have responded to COVID-19 in SSA.7–9 In programmatic settings throughout the region, including in the southern African country of Zambia, changes to HIV care were implemented, including introduction, adaptation and scale up of differentiated service delivery (DSD) models, with the intent to decongest health facilities and minimise disruptions to HIV treatment and care for PLHIV.3 10
In Zambia, access to one DSD model, multimonth dispensing (MMD) of antiretroviral therapy (ART), has increased since 2016. Refill intervals for ART in Zambia have been increasing over time as ART supply chains have become more stable and retention advantages of longer ART refill intervals have been demonstrated.11 First, the refill interval was extended from a standard of 1–3 months, and prior to COVID-19, the Zambian MoH had issued national recommendations for providing 6-month refills for stable patients (ie, PLHIV in care ≥6 months, virally suppressed and with minimal missed appointments). However, scale-up of this 6MMD model had been sluggish due to limited ART stocks, differing definitions of MMD eligibility, and other operational challenges.12 With the emergence of COVID-19, MoH mitigation guidance included recommendations for strengthening 6MMD implementation, potentially increasing the probability that an individual would receive a 6-month ART refill. Given the high prevalence of HIV in Zambia, estimated to be 11.5% of the adult (15–49 years old) population, there is an urgent need to understand how COVID-19 mitigation guidance, including strengthened 6MMD, impacted HIV care and treatment nationally.13 14
In this pre–post quasiexperimental analysis, we leveraged Zambia’s national HIV electronic medical record (EMR) to evaluate the effect of the new COVID-19 mitigation recommendations on HIV care visits at public health facilities supported by the President’s Emergency Plan for AIDS Relief (PEPFAR), which provides approximately 97% of the HIV care funding in Zambia.15 Here, we report changes in HIV care visits, including incidence of early patient return, late visits and incidence of 6MMD ART refill to estimate effects of mitigation guidance on HIV treatment interruption during the early COVID-19 pandemic in Zambia.
Methods
Design and patient population
We conducted a before–after cohort study involving routine data from PLHIV in care, defined as having ≥1 documented pharmacy visit(s) between 1 January 2019 and 31 December 2019 and at ≥1 visit between 1 January 2020 and 30 June 2020 at MoH HIV care facilities in Lusaka Province, Zambia. All pharmacy visit records were extracted from SmartCare, which is the national HIV EMR owned by MoH and developed and supported by CDC/PEPFAR and its implementing partners. SmartCare serves as a comprehensive repository of all HIV-related clinical, laboratory and pharmacy data, including visit information, for the study population.
Setting
We included 59 MoH HIV care-providing facilities in Lusaka Province supported by PEPFAR/CDC. Lusaka Province is Zambia’s most densely populated province and includes the capital city of Lusaka. Lusaka Province has an estimated total adult (ages 15–49 years) PLHIV population of 202 823, with an estimated adult HIV prevalence of 11.5% in 2019.13 14
COVID-19 mitigation guidance
Zambian COVID-19 mitigation guidance functioned as an emergent intervention to provide MMD of ART to all PLHIV.4 16 ART provided via MMD was for a supply of 3–6 months. To implement this guidance at health facility level, CIDRZ implementers used a phone-based community outreach strategy to proactively call back patients with an upcoming pharmacy appointment and ask them to present to the facility for an immediate pharmacy refill. CIDRZ-supported lay treatment providers and community liaison officers based at the health facilities used line-lists extracted from the SmartCare EMR, including telephone contact information from a routine patient locator form, to request that a patient return to the clinic earlier than their scheduled appointment to receive ART MMD. Community sensitisation for early clinic return for an extended MMD refill was also accomplished through radio talks and mobile megaphones to reach those who may not have a phone number on file in SmartCare.
Outcomes
We defined an ‘early return’ as a documented return pharmacy visit occurring 8 or more days prior to an appointment date scheduled for between 1 January 2020 and 30 June 2020. A visit was categorised as ‘on-time’ if it occurred in a 15-day window around the next scheduled appointment date, specifically less than 8 days before or less than 8 days after the next scheduled appointment date. Late visit categories were defined on return visit using the first pharmacy visit occurring after the assigned appointment at intervals of: (1) 8–89 days late; (2) 90–180 days late; and (3) >180 days late.17 18 ART refill spacing, especially 6MMD refills, was assessed using the pharmacy appointment interval (ie, next appointment date minus the date of pharmacy visit).
Statistical analysis
We compared the prevalence of early return in the preguidance period from 1 January 2020 to 23 March 2020 to the postguidance period from 24 March 2020 to 30 June 2020. Mixed effects Poisson regression was used to estimate prevalence ratios of early return before (preguidance) and after (postguidance) issuance of COVID-19 mitigation guidance on 24 March 2020. Crude prevalence ratios resulted from univariate models allowing a random effect at the facility and individual level. Adjusted estimates were the result of a model including fixed effects for age, sex, marital status and time in HIV care, which were identified a priori as potential confounders for the outcome of early return, and random effects at the individual and facility levels. Descriptive counts and proportions were illustrated to elucidate trends in the data over the study period. Additionally, we estimated predictive probabilities and associated 95% CIs of early visit receipt of a 6-month MMD ART refill and of late visit.
Ethical statement
Participant consent was not required as all analyses were conducted as part of routine CIDRZ programme monitoring and evaluation.
Patient and public involvement
COVID-19 mitigation guidelines were developed by the Zambian MoH, and implementation of the guidance was conducted as part of routine CIDRZ PEPFAR programming in partnership with the Zambian MOH, CDC/PEPFAR, implementing partners and affected communities, including PLHIV. As we describe observational results from this routine programme activity, patients in the analysis population were not directly involved with the design of the intervention or the analysis presented here. Dissemination of study results is ongoing in consultation with CDC/PEPFAR and the CIDRZ Community Advisory Board.
Results
A total of 130 486 pharmacy visits among 101 371 PLHIV were included in the analytical dataset. Of all individuals included in the analysis, a majority were women (64.7%), had a median age of 38 years (IQR: 30–45 years) and reported being married (55.0%). Sex, age, marital status, and years in HIV care did not differ meaningfully between patients analysed before (1 January 2020–24 March 2020) and after (24 March–30 June 2020) COVID-19 mitigation guidance (issued on 24 March 2020) (table 1).
Characteristics of those with HIV pharmacy visits before (1 January 2020–23 March 2020 and after (24 March 2020–30 June 2020) implementation of COVID-19 mitigation guidance
Early return visits following implementation of modified HIV care recommendations
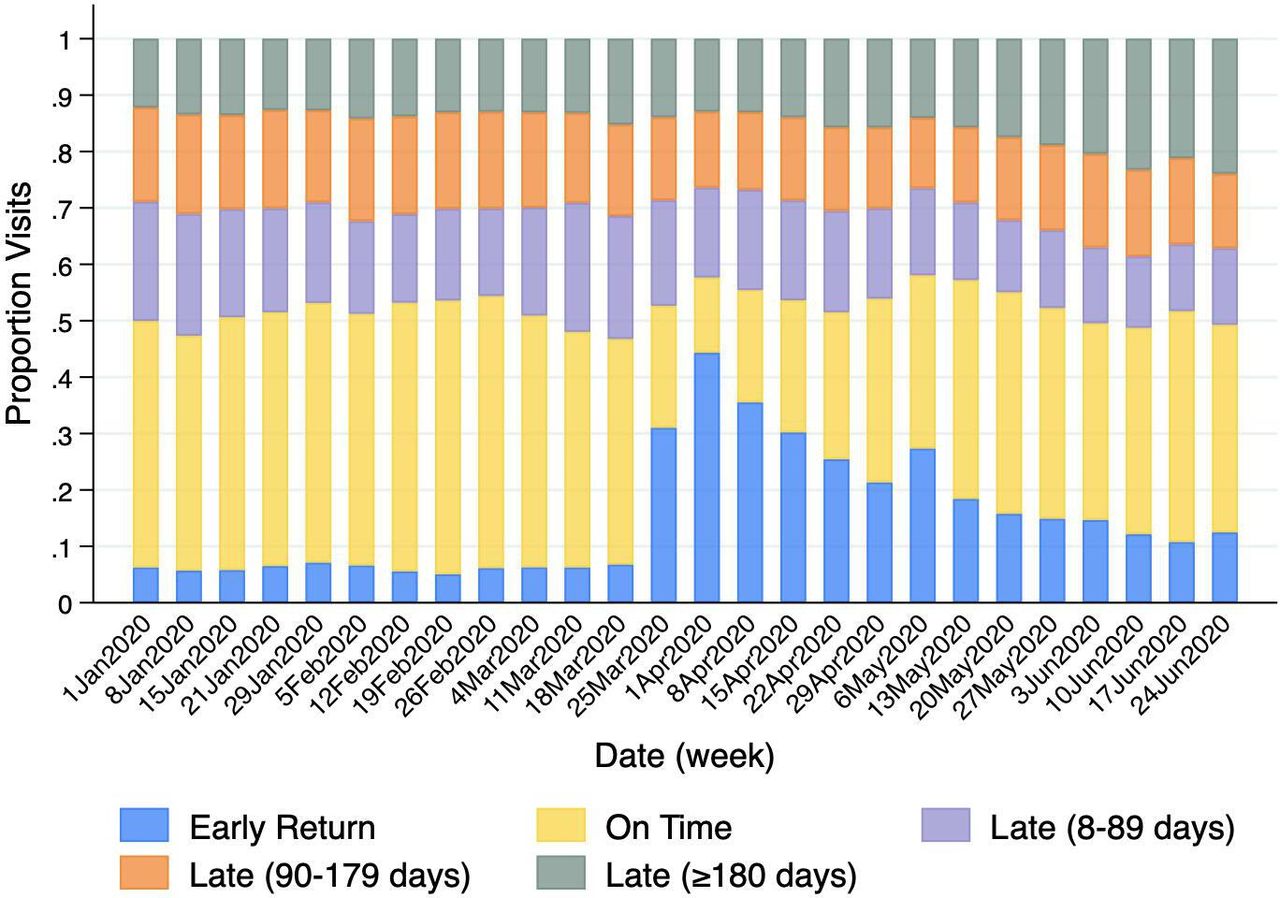
Those accessing HIV services in the period after COVID-19 response guidance (ie, between 24 March and 30 June 2020) returned to clinic early with an adjusted prevalence ratio of 4.63 (95% CI 4.45 to 4.82) times that of those in the preceding 3 month period (table 2). The adjusted prevalence ratio (aPR) for early return was lowest for those 16–24 years old (aPR: 0.81, 95% CI 0.76 to 0.85), followed by those 25–29 years old (aPR: 0.86, 95% CI 0.82 to 0.91). Those who were divorced/widowed (aPR: 0.90, 95% CI 0.85 to 0.95) and those who were married (aPR: 0.94, 95% CI 0.90 to 0.98) had a lower adjusted prevalence ratio for early return compared with those reporting being single. Those in care 6–12 months had a significantly lower adjusted prevalence (aPR: 0.78, 95% CI 0.73 to 0.84) of early return compared with those recently initiating HIV care (table 2). We also found that the mean weekly proportion of early return in the preguidance period was 6.2% (95% CI 5.8% to 6.5%), significantly lower than the postguidance period with a mean weekly proportion of 22.5% (95% CI 16.6% to 28.3%) (p value: <0.001) (figure 2).
Crude and adjusted prevalence ratios for early return (8 or more days from scheduled appointment)
We observed a surge of 25 758 more visits than scheduled appointments, despite relatively stable appointment volumes, in the 4 weeks immediately following COVID-19 mitigation guidance implementation (figure 1 and online supplemental table S1). It is also important to note that in the last 6 weeks of the review timeframe (20 May 2020–30 June 2020), scheduled appointments outnumbered actual visits (figure 1 and online supplemental table S1).
Supplemental material

Area graph of counts for attended visits and appointments by date, before guidance (1 January 2020–23 March 2020) and after guidance (24 March 2020–30 June 2020). Note: dashed line indicates timing of before–after transition (ie, 24 March 2020). Appointments associated with early visits were censored.
Late visits following implementation of COVID-19 mitigation guidance
There was a significant shift in the proportion (Mann-Whitney p value: 0.002) of individuals returning ≥180 days after their scheduled appointment from the preguidance (13.3%, 95% CI 12.8% to 13.8%) to the postguidance period (17.2%, 95% CI 15.0% to 19.3%). The weekly mean proportion for visits where individuals were 8–89 days late (18.8%, 95% CI 17.2% to 20.5%) and 90–179 days late (17.0%, 95% CI to 16.6% to 17.4%) were higher in the preguidance period compared with the postguidance period where 8–89 days late accounted for 15.1% (95% CI 13.8% to 16.4%) of visits and 90–179 days accounted for 14.4% (95% CI 13.8% to 15.0%) of visits (figure 2).
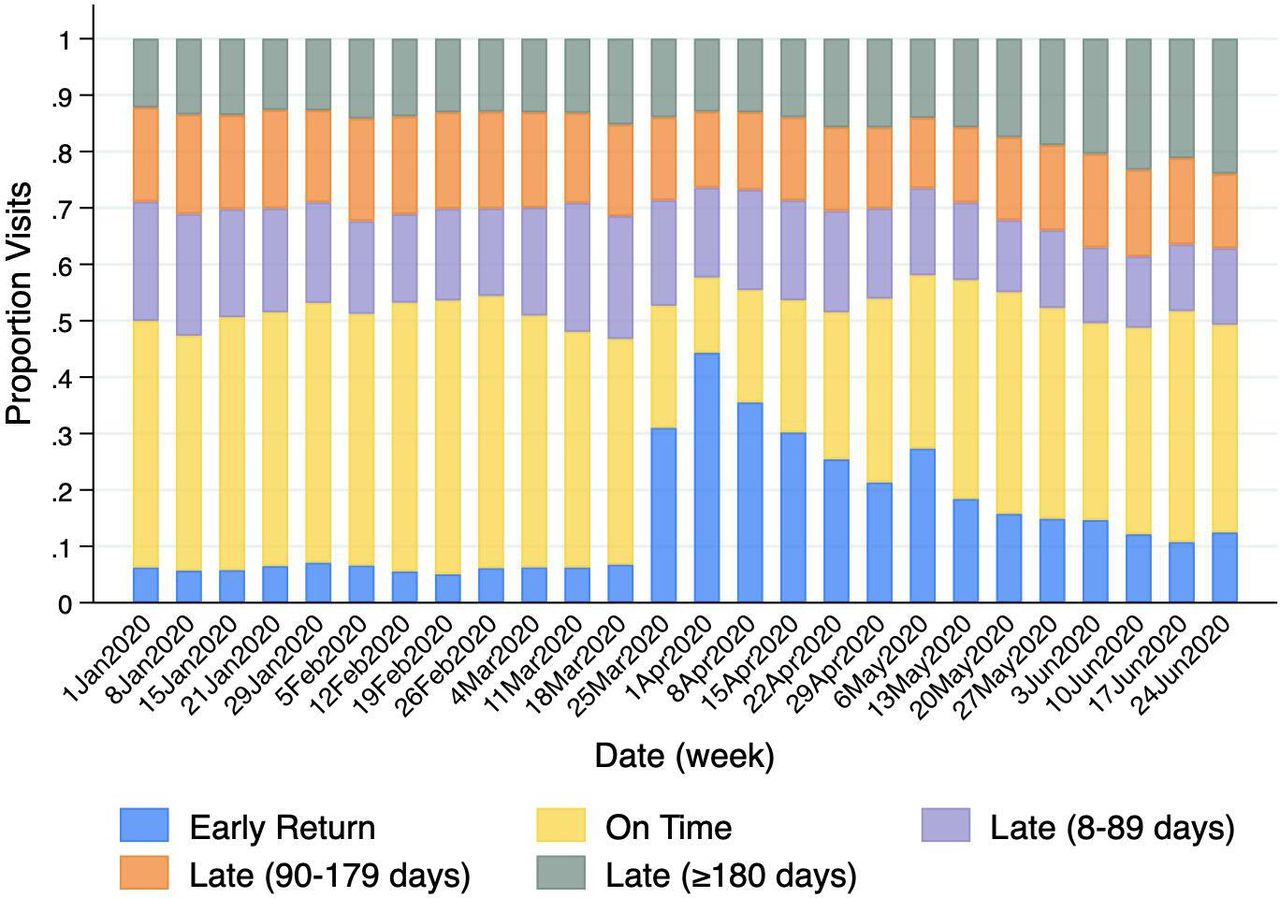
Stacked bar chart of visit status/category among all those with an attending visiting Lusaka Province art clinics by week before (1 January 2020–23 March 2020) and after guidance (24 March 2020–30 June 2020). Note: before–after transition occurred the week of 18 March 2020 (ie, 24 March 2020).
Likelihood of 6-month ART refill visits following implementation of COVID-19 mitigation guidance
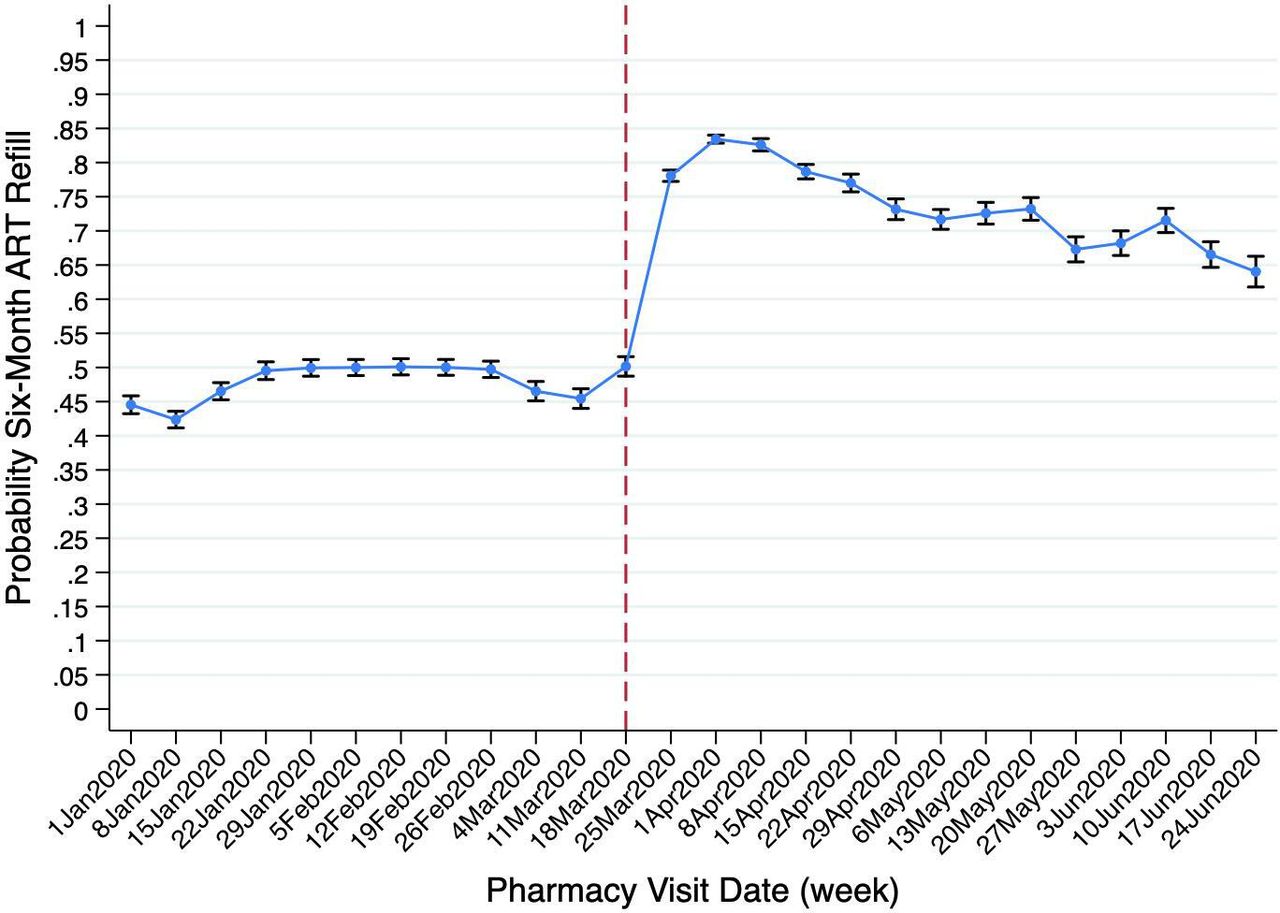
The mean proportion of those receiving a 6MMD ART refill was significantly greater in the period after implementation of COVID-19 mitigation guidance (73.4%, 95% CI 72.0% to 74.9%) compared with the before period (47.9%, 95% CI 46.6% to 49.2%), with a peak probability of 83.4% (95% CI 82.8% to 84.0%), the week of 1 April 2020 (figure 3).

{kind=link}
{kind=link}
{kind=link}
Line graph of predicted probability of receiving a 6-month refill by week before (1 January 2020–23 March 2020) and after (24 March 2020–30 June 2020) guidance with 95% CIs. Note: before–after transition occurred the week of 18 March 2020 (ie, 24 March 2020); predicted probability and 95% CI based on Poisson model adjusted for age, sex, marital status, time in care and facility.
Discussion
We observed a significant increase in the incidence of both early return for ART collection and use of extended 6MMD after implementation of COVID-19 mitigation guidance to prevent HIV treatment interruption in Lusaka, Zambia. Owing to stakeholder coordination and communication, implementation of the guidance, including sensitising health workers, PEPFAR partners, PLHIV and other affected communities, only took 1 week. Collectively, these findings indicate that the HIV treatment programme in Lusaka responded rapidly and adapted effectively to the external shock posed by COVID-19 through a response package involving 6MMD and patient outreach done by lay health providers. Importantly, early return for ART was observed least frequently among adolescents and young adults. This younger demographic represents a priority population that has been, traditionally, hard to reach with HIV services before the COVID-19 pandemic and, based on our data, remain challenging to engage in HIV programmatic innovations during a public health emergency.
Though COVID-19 mitigation guidance appears to have resulted in early return for ART collection for most PLHIV in care, it is unclear if this led to long-term improvements in HIV care retention. It may be that early return simply shifted appointments that would have happened otherwise to an earlier time and reduced the volume of facility visits over the ensuing months. However, this result may be a worthwhile end, in and of itself, for HIV programmes during a pandemic, as it decongests health facilities, minimises risk of nosocomial COVID-19 transmission and helps health workers prioritise patients having the most active HIV care issues, thereby offloading an already overburdened health system in the throes of COVID-19 response.
While we illustrated the successful surge of early clinic return visits immediately following implementation of COVID-19 mitigation guidance, there were distinct shifts in the ratio of attended appointments to scheduled appointment later in the pandemic. Immediately after guidance implementation, there was an early surge when significantly more patients attended visits compared with scheduled visits, but later the ratio shifted to fewer patients attending visits compared with those scheduled. These observations could be due to one or more of the following reasons: 1) patients readily responding to the sensitisation, mitigation guidance and outreach efforts to encourage early return, 2) patients being more affected by COVID-19 and less likely to return for a visit, even for a regularly scheduled visit and/or patients presenting to care shortly after the first reports of COVID-19 motivated by fears of possible facility closure or ART stock outs, among others. It will be important to rigorously evaluate incidence of lost to follow-up and continue efforts to promote HIV care retention as COVID-19 continues to impact HIV and other public health programmes.
Although not conclusive, our data support the concept that telephonic communication can enable programmatic innovation and adaptation when used alongside the following implementation strategies: community outreach and mobilisation; task shifting to lay health providers; and modifying pharmacy appointments . Past research has leveraged phone-based contact with individuals lost to follow-up in Zambia and for improved HIV testing in prevention of mother-to-child transmission studies in Kenya and South Africa.19–21 Mobile network coverage for Zambia was estiamted to be 99.1% in 2019, compared with 74.3% 4 years prior.22 23 This rapid expansion in mobile network operations and increasingly affordable mobile technology has opened the door for improved efficiency and convenience for patient-provider communication, even in settings with limited resources.
It has been noted previously that adolescents and young adults exhibit different healthcare-seeking behaviours compared with older adults, which may have played a role in the uptake of early return for ART collection seen in our study.24–26 We observed age-related differences in our outcomes of interest, with the lowest predictive probability of early return seen among patients ages 16–24 years. One key potential reason that we observed less early return among younger people could be related to higher phone number turnover in this more mobile and economically active population, especially in urban settings like Lusaka.27 It is also possible that young people are at increased risk for mental health stressors associated with the COVID-19 pandemic, school or work schedule interruptions, and/or other psychosocial factors that might impact their ability and/or availability to return early for an ART refill.28 29 Other possible reasons could relate to young people having more exposure to COVID-19 related misinformation on social media, or, in so far as young people in our study lived in informal urban settlements with limited health education infrastructure, they could have been harder to reach with health messaging during our community outreach activities.30
PLHIV recently initiated on ART were significantly more like to have an early return visit than those more established on ART. This observation could be due to the fact that those who initiated HIV care more recently may be more likely to have a current and, thus active, phone number documented in the EMR to enable contact by telephonic outreach efforts. Additionally, it might be possible that those with more treatment experience are more comfortable with set appointments and, thus, less receptive to early return visit because they are less likely to want to change their appointments than patients newer to HIV care.
Our study had several limitations. First, we included a limited follow-up duration in the postguidance period. However, we hypothesised that the effect of guidance implementation would be immediate and that it would be possible to demonstrate that the guidance had its intended effect shortly after implementation. While this limited our ability to assess guidance effects on longer term clinical outcomes like HIV care retention and viral suppression, it likely mitigated against competing secular trends due to the close temporal relationship between guidance implementation and assessment of the frequency of pharmacy visits. It will be important for future evaluations during the COVID-19 pandemic to closely monitor retention and viral suppression metrics to ensure that PLHIV do not experience clinically significant treatment interruptions. Second, our analysis was focused predominately on urban clinics, which may not be generalisable to rural areas in Zambia. Third, we captured only individuals in the EMR for which records were complete, which may have excluded patients with somewhat incomplete or incorrect records. Nonetheless, the data for key variables has previously been found to be highly complete and the quality of such records is frequently audited by CIDRZ and the Zambia MoH to address inaccuracies and update the data on a rolling basis. Fourth, we assume that the primary contributor to the large increase in early return visits and the decrease in actual visits over time was due to implementation of COVID-19 mitigation guidance and greater adoption of 6MMD, though it is possible that several other unknown and/or unmeasured factors, such as fear of ART supply shortages or facility closures or wanting COVID-19 information or clinical evaluation may have played a role. Finally, while our findings support the impact of the COVID-19 mitigation guidance and implementation strategies described, they do not prove causation, which would require confirmation in larger, randomised studies. That said, our pragmatic study design enabled us to quickly estimate the effects of a multilevel intervention using routinely available data during a rapidly evolving public health emergency.
Conclusions
We showed that government COVID-19 mitigation guidance implemented using a multipronged, task-shifted outreach strategy can mitigate HIV care disruption among PLHIV in care at the time of a disruption to the public health system. It is important that patient telephone numbers and other contact details are routinely updated, particularly for adolescents and young adults living with HIV and that HIV programme investments in community platforms, including lay health providers and community sensitisation channels, are maintained to enable their rapid leveraging to mitigate HIV treatment interruptions during times of external shocks, such as that caused by COVID-19.
Data availability statement
Data are available on reasonable request. The data used to prepare these analyses are not public and are part of the Zambian national electronic HIV medical record data, and as such, are only potentially available on request and with permission from the Zambian Ministry of Health (suggested contact: info@moh.gov.zm). Access to data is subject to restrictions including, but not limited to, deidentification and suppression of small cell sizes.
Ethics statements
Patient consent for publication
Ethics approval
The review of existing, deidentified, routinely collected programmatic data was approved by the US Centers for Disease Control & Prevention (2018–381), University of Zambia Biomedical Research Ethics Committee (011–12- 17), University of North Carolina at Chapel Hill, USA Institutional Review Board (18–0854) and the Institutional Review Board at Washington University, St. Louis, USA (2019–11143).
Acknowledgments
We would like to thank the Zambian Ministry of Health for their leadership to ensure those in HIV care continue to receive life-saving HIV treatment. We would also like to thank the healthcare workers who continued to faithfully deliver HIV care in the face of the COVID-19 pandemic.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @Kombatende, @MpandeMwen
JMP and KS contributed equally.
Contributors JMP: guarantor, lead author, conducted all analyses, led data management activities. KS: lead author and field coordination of data. AMo: assisted with analysis. SL: assisted with conceptualisation and data processes. JM: assisted with data extraction. NV: assisted with writing and advised regarding intervention implementation details. TS: lead for underlying data processes and assisted with writing. MWM: lead for underlying data processes and assisted with writing. KM: assisted for underlying data processes. AMw: assisted for underlying data processes. CM: assisted for underlying data processes. MM-M: advised intervention implementation details. ADK: assisted with framing and analysis. IS: lead for underlying data processes and assisted with writing. CBM: lead for underlying data processes and assisted with writing. DM: assisted with writing and advised regarding intervention implementation details. EHG: led conceptualisation and advised on all analyses. MEH: assisted with conceptualisation and manuscript writing.
Funding The US President’s Emergency Plan For AIDS Relief (PEPFAR) through the US Centers for Disease Control and Prevention/Zambia (CDC) and the Centre for Infectious Disease Research in Zambia (funding reference: NU2GGH001920).
Disclaimer The contents of this paper are the sole responsibility of the authors and do not necessarily reflect the views of PEPFAR, USAID, or the United States Government.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.