Article Text

Abstract
The Improving Global Health (IGH) programme develops leadership capacity within the National Health Service (NHS) in a novel way. NHS employees collaboratively run quality improvement projects within organisations in low-income and middle-income countries with whom long-standing healthcare partnerships have been built. Leadership behaviours are developed through theoretical and experiential learning, alongside induction and mentorship. The health systems of overseas partners are strengthened through projects that align with local priorities. This article develops solutions to two main problems: how reciprocal global health programmes can be designed and how global health programmes based in leadership can attract women and black and minority ethnic groups into leadership. The outcomes of both sides of the IGH programme are described here. The overseas perspective is described using the reflections of two current partners, highlighting improvements in the local healthcare system and demonstrating growth in local team members. The UK perspective is evaluated using two surveys sent to different groups of returned IGH participants. Leadership, global health and quality improvement skills improve, having a significant and long-lasting impact on career trajectory. The IGH programme is attracting women and black and minority ethnic groups into leadership. Through collaboration and reciprocity, the IGH programme is developing a new cadre of NHS leader that is diverse and inclusive. The use of long-standing healthcare partnerships ensures that learning is shared and growth is mutual, creating development within the overseas and UK partner alike.
- health education and promotion
- health economics
- health policy
- health systems evaluation
Data availability statement
All data relevant to the study are included in the article.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Leadership development is needed throughout the National Health Service (NHS) and is known to have a positive effect on the quality of health delivery.
The experience of working internationally is known to improve leadership skills.
The Improving Global Health (IGH) programme is a novel leadership development programme based on experiential learning through overseas placement.
Many returned fellows reported a substantial development in their leadership behaviours. Improved confidence to be a leader, better knowledge of quality improvement methodology and a better understanding of global health were also reported. Completing the fellowship had a substantial and long-standing impact on career trajectory.
IGH in-country partners report healthcare system improvements.
The IGH programme is attracting women and minority ethnic groups into leadership.
Leadership development programmes, such as the IGH programme, must be encouraged and scaled up in order to promote the training of a diverse and inclusive group of NHS leaders of the future.
The success of the IGH programmes’ global health work is due to its focus on reciprocity through mutual learning and development.
Introduction
The Improving Global Health (IGH) programme is a National Health Service (NHS) leadership development programme that, owing to its practice of running projects in low-income or middle-income countries, is unique in its design. Leadership is developed through the experiential learning of an overseas placement while improvements in the local healthcare system are realised, in contrast to other NHS leadership programmes that are based in the UK.1 ,2 Through vertical leadership development,3 the programme creates leaders who are independent of thought, adaptable and are able to face challenges; they are more culturally and emotionally aware (accepted for publishing, ‘a qualitative analysis of vertical leadership development among NHS healthcare workers in low to middle income country settings’, January 2020). These leaders are needed in a fast changing and ever more pressurised NHS.
Women are under-represented in more senior clinical NHS roles4 and fewer senior NHS staff are from black and minority ethnic background.5 The under-representation of women and minority ethnic groups within NHS leadership can be addressed by fostering a culture of inclusivity within leadership development programmes. This article highlights the reciprocal nature of the IGH programme by outlining leadership development in the returned fellow and describing the impact of the programme on the host country’s healthcare system and workers. The IGH programmes’ ethos of ‘co-development and mutual learning’ as a replacement for ‘more outdated ideas of international development’6 is highlighted, and a framework for fostering reciprocity in global health programmes is drawn.
Programme overview
The IGH programme gained recognition as a programme which provides benefit to all participants. Since it began, 254 fellows have completed a placement, each spending on average 6 months overseas. Participants, known as ‘fellows’, work in partnership with in-country health workers to implement projects using quality improvement (QI) methodology. Leadership behaviours are developed through experiential learning,7 using the NHS Healthcare Leadership Model as a framework.8 Fellows do not provide clinical care but act as project coordinators, contributing to local healthcare improvement. Project topics are chosen by the in-country team with the Sustainable Development Goals (SDGs) in mind, ensuring work is aligned with local healthcare priorities.
During the lifetime of the programme, 12 overseas partnerships have been formed with organisations in Cambodia, Myanmar, Tanzania, Kenya, South Africa, Zambia, Lesotho and Uganda. Preplacement, fellows complete 4 days of UK-based induction where they learn concepts of leadership, communication skills and behaviours; project planning, implementation and evaluation; QI methods; peer learning and support; concepts of public health and the wider determinants of health; the SDGs, teaching and learning and cultural preparation for their placement site. There is allocated time to complete and receive feedback regarding their Myers-Briggs Type Indicator (MBTI).
Fellows are each allocated a mentor to support and challenge them and have access to a partnership-link lead (PLL) who supports the relationship with the partnership organisation. Mentors are recruited from IGH alumni. They attend a training day called ‘Coaching Conversations’ which is updated every 2 years. The PLL is a voluntary role, and they all complete 5 days of training to become an MBTI Practitioner (level 1). Postplacement, fellows complete a project report, reflect on their leadership development and present their work and learning to their colleagues.
Leadership and the IGH programme
‘Leadership is becoming less about being the smartest in the room and much more about how we collaborate, work with diverse stakeholders, inspire and bring the best out of others. Being more inclusive and collaborative. It’s about developing our ability to be curious; our ability to explore new approaches, new perspectives, engage different stakeholders and view points and empathise with diverse perspectives’.9
There has been a call for leadership within the NHS at every level that is high quality, inclusive and compassionate.10–12 NHS Improvement outlines that QI and leadership must be embedded within healthcare curricula and revalidation processes, making programmes such as the IGH programme ever more necessary.13 The modern world has been described as increasingly: volatile, uncertain, complex and ambiguous; descriptors that are readily applied to health systems such as the NHS.14 15 There is therefore a need for strong leadership. A review of NHS leadership concludes that properly developed leadership can lead to improvements in patient satisfaction, patient mortality, financial performance, staff well-being, engagement, turnover and overall quality of care.16
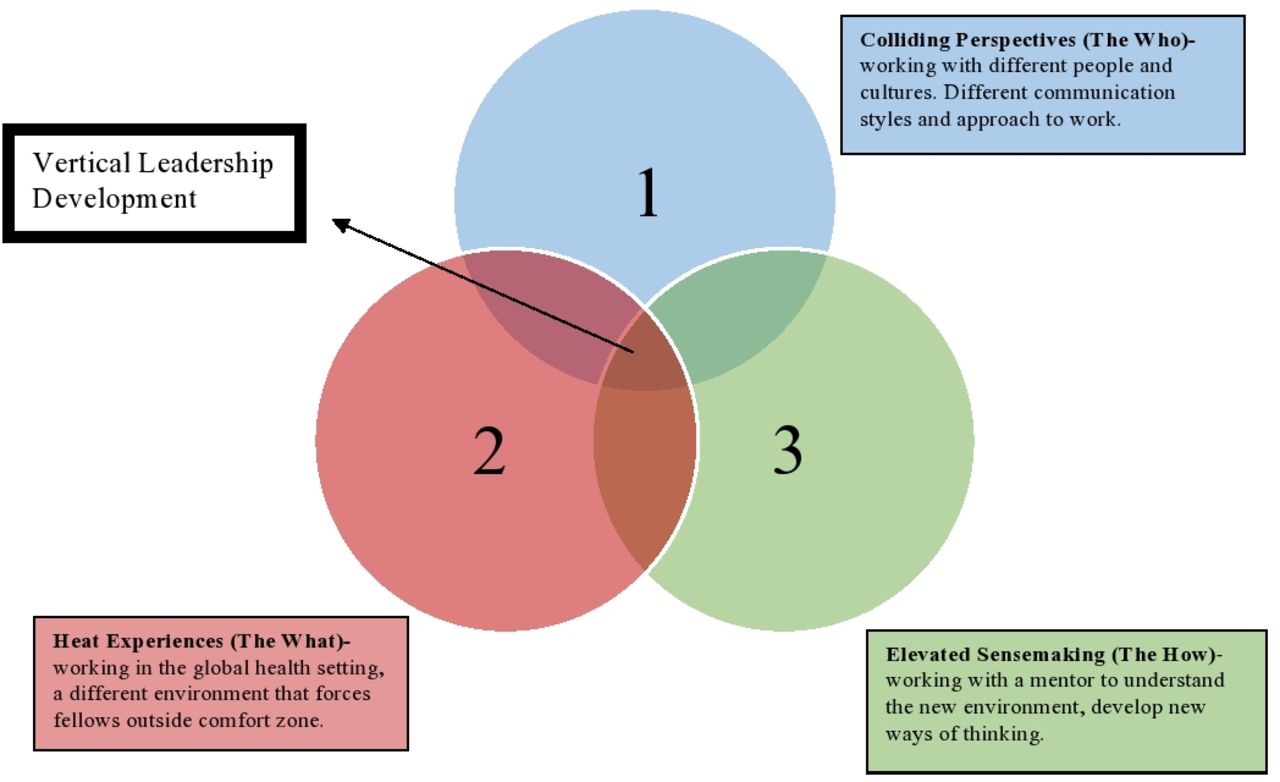
The IGH programme is centred on developing the leadership behaviours described in the NHS Healthcare Leadership Model8 and has evolved to use the framework of vertical and horizontal leadership development3 to support this. Horizontal leadership development is about imparting knowledge and facts, while vertical leadership development is about changing the way you think.3 The structure of the IGH programme fits well with the proposed design of a horizontal and vertical leadership development programme. Vertical leadership development needs a ‘heat experience’, ‘colliding perspectives’ and ‘elevated sensemaking’ (figure 1).

The IGH programme as a vertical leadership development programme. Reproduced and adapted from Petrie (2015).3 IGH, Improving Global Health.
The induction programme provides the horizontal development through classroom learning of theoretical knowledge, while the overseas placement facilitates the vertical development. The placement puts fellows in an unfamiliar environment, within a country and healthcare system that is different from their own. They co-ordinate a project in a specialty or area that they may have little or no prior knowledge or experience. This serves as their ‘heat experience’, and they face a challenging situation where their normal way of operating is inadequate, forcing them to consider new ways of thinking. The fellows work in partnership with people they have only just met, from a different culture and society. Communication, experiences and training are different, producing the ‘colliding perspectives’ element of vertical leadership development. At a time when the fellows are open to new ways of thinking, they are presented with a range of new perspectives to consider and sample. Finally, they are provided with a mentor, an in-country project supervisor and a PLL who work to coach the fellows to establish new thought processes, called ‘elevated sensemaking’.3 The aspiration is to take leaders from the state of the ‘faithful follower’, to ‘independent thinker’ and finally to the ‘interdependent collaborator’ (figure 2). It is in this final state that leaders become better adapted to cope with the uncertainty of a modern health system, such as the NHS.17

Stages of vertical leadership development. Reproduced and adapted from Petrie (2014).17
Global health
The overseas placement is integral to the programme’s design, partly as it contributes to the ‘heat experience’ described above and also in helping participants to understand another health system and develop their cultural intelligence.18 Cultural intelligence is described as building on emotional intelligence.19 ‘A person with high cultural intelligence can somehow tease out of a person’s or group’s behaviour those features that would be true of all people and all groups, those peculiar to this person or this group, and those that are neither universal nor idiosyncratic’. This ability enables people to work more effectively with colleagues and patients from a range of cultural backgrounds.
Prior to the COVID-19 pandemic, the world was described as becoming smaller, with a greater interconnectedness due to ease and desire for travel as well as developments in technology allowing collaboration without the need for travel. Many healthcare practitioners are increasingly interested in global health and there are a growing number of learning opportunities, both experiential and academic. It is recognised that by so doing, healthcare workers from all over the world can benefit as they learn and work together. Boelen20 describes the need for healthcare professionals the world over to be ‘fit for practice’. This includes the ability to serve local communities while also being global citizens.
Overseas perspective
A 2017 evaluation of the sustainability of IGH project work outlines how fellows bring with them an ability to challenge and ‘hold up a mirror’ to the local health system. This was seen as a positive aspect of the NHS culture, along with a ‘can do’ attitude, a culture of being ‘change agents’ and an ‘evidence-based practice culture’ (unpublished, Monitoring and evaluation of system-strengthening project work, 2017). The reciprocity of the IGH programme is outlined here through the use of case studies from two sights, chosen to provide a balanced perspective, with Cambodia being one of the oldest partnerships and Myanmar one of the youngest.
Maddox Jolie-Pitt (MJP) Foundation, Cambodia written by Munichan Kung, CEO
Poverty reduction among the most vulnerable communities in Samlaut District is a part of MJP Foundation’s core mission. MJP has been supporting the Ministry of Health’s delivery of basic healthcare in the district since 2006 to reduce child mortality and sickness, improve maternal health, and tackle preventable diseases.
The IGH partnership has provided MJP with several years of technical support in the delivery of sustainable healthcare, in the areas of capacity-building, systems-strengthening and the integration of health outcomes into the wider work of MJP. With support from the IGH fellows, we have provided medical training sessions for local healthcare staff, helping them to develop their skills and expertise to deliver a high standard of clinical care. The IGH fellows supported school-based and community-wide education programmes to increase awareness of the importance of hygiene—from hand washing to waste disposal. They also worked with MJP to mount an immediate response to tackle outbreaks of diseases such as malaria, dengue and COVID-19. In 2017, the IGH fellows conducted a health services assessment and formulated a thorough long-term ‘Health Strategy’ for the Samlaut district. The document established a clear roadmap and reference for the MJP health programme.
Participation in the programme has supported leadership development in the Cambodian team. Two of the health team successfully applied for competitive government grants to undertake advanced postgraduate education overseas and have returned to take up more senior roles in the healthcare system. The partnership has proved that a difference of cultures is not an obstacle to hard work for the improvement of lives.
Myanmar General Practice, written by Myint Oo, Vice-President, General Practitioners Society (GPS)
Myanmar aims to achieve Universal Health Coverage goals by 2030. General practitioners (GP) in Myanmar receive little formal training in general practice. There is no Primary Care Trust or Clinical Commissioning Group, and health insurance is non-existent. GPS is the only professional body to provide Continuing Medical Education to these private GPs.
Ten IGH fellows have engaged with the GPS on projects ranging from the use of point of care testing, medicines management and identification of quality markers in GP clinics, to the development of a GPS website and a GP database. Fellows have made oral and poster presentations at national GPS and international conferences and have published articles in collaboration with GPS mentors. Feedback from GPS has been exceptional. One fellow, in conjunction with Royal College of General Practitioners (RCGP) representatives and GPS, met with the Union Minister for Health to champion a QI project. This project is currently being delivered virtually to over 100 local GPs from four townships. As a result of the IGH programme, the Myanmar GP improvement agenda has become one of the priorities of the Myanmar-UK Health Alliance programme.
Myanmar GPs have developed their knowledge of medicine and have furthered their careers as a consequence of the programme. Fellows helped prepare Myanmar GPs for the Membership of RCGP International examination resulting in six passing. The leadership and soft skills training created by the IGH fellows helped Myanmar GPs to strengthen their relationship with Freiburg University in Germany, resulting in a 4-year grant to launch ‘psychosomatic basic care training’ for GPs, nurses and psychiatrists being won.
UK programme evaluation
A qualitative evaluation was conducted to investigate the leadership development and long-term impact of the IGH programme on alumni. An online survey was designed with support from an experienced education researcher. It uses 10 open and 18 closed questions to explore the respondents’ thoughts and experiences. Piloted through its use in a previous programme evaluation, the survey was distributed using ‘Online Surveys’ and was sent to different groups of fellows at two different time points, July 2019 and September 2020. The ‘first survey’ refers to the survey sent to fellows who completed placements between 2008 and 2019. The ‘second survey’ refers to the survey sent to fellows who completed placements between 2015 and 2018. Fellows who did not respond initially were reminded. The first survey asked about demographics where the second did not.
The structured question responses were collated and the free-text responses were open coded and a thematic framework developed for each of the questions. For the purpose of this article, only relevant themes have been reported. The results have been described using the terms ‘a few’, relating to ideas described by less than 25% of respondents, ‘some’ relating to ideas described by 25%–50% of respondents, ‘many’ relating to ideas described by 50%–75% of respondents and ‘most’ relating to ideas described by over 75% of respondents. Some key quotes are summarised in box 1.
Quotes from returned fellows, taken from survey responses
‘The unique blend of needing to be assertive when implementing a change as well as understanding both the complexity and the necessity of tailoring a change to the circumstances.’
‘I know the theory quite a lot better and more importantly…I have experienced it now…I think quality improvement is hard work. It requires a lot of energy and the development of specific personal characteristics.’
‘It’s really hard to articulate the ways in which it has changed my life and career; the time on the fellowship allowed me to think, to be creative, to try and be a leader in a way that I had never experienced previously in the NHS. As a doctor in training you often feel as if you are on a conveyor belt with frequent hoops to jump through but little attention paid to you if you succeed in doing so - and little time to truly reflect on where you are and where you're going. I appreciated the chance to be taught, to be listened to, to have responsibility for a greater level of service other than direct clinical service provision on the shop floor. I am now interested in getting in to policy, whether that be for the CCG or for a think tank alongside my clinical work. Personally, it has given me the confidence to take a step back every now and then to think about the bigger picture and how my career choices align with my values. Working in healthcare systems through IGH in seriously income deprived countries has reaffirmed my desire to serve and support the NHS.’
‘I wanted an opportunity to contribute to development in a structured and supported way. The IGH programme offered this opportunity with well-established links to a number of organisations. The leadership development aspect was also an important consideration and allowed the opportunity to develop skills which have been valuable in my continued career progression.’
‘I learnt the importance of truly listening to understand. I discovered…the importance of not jumping to conclusions, the complexity of systems and networking.’
‘I now have much more confidence in myself and my abilities. I feel better prepared to take on leadership roles and when things can be done better on the wards I am more likely to think “how can we improve this?” rather than just complain and put up with it!’
'In my new role since returning from placement (Education Supervisor) I am using coaching and mentoring skills that I learned during placement preparation and during placement. I am also using leadership skills that I used in placement. Quality Improvement is another area I use after I practiced in placement.’
‘As CCG clinical director I use leadership, quality improvement and co-production skills all the time which I began the development of during my IGH placements.’
Results
The Respondents
The first survey had 98 (49%) responses and the second 47 (51%). The majority of fellows (70 (71%) and 35 (74%)) in both surveys were doctors, in a range of postgraduate training roles. The other respondents included nurses, occupational therapists, radiographers, dieticians, clinical psychologists, physiotherapists, podiatrists, speech and language therapists, pharmacists, project managers and midwives. The inclusivity of the programme is increased by its multidisciplinary approach.
Many respondents (in both surveys) described feeling motivated to apply to the programme to gain experience of working within a global healthcare setting. Many fellows in the first survey and some from the second were looking for personal or leadership development. Other reasons cited were to develop QI skills, as a career development step and wanting to gain life experience. Looking for personal or leadership development became more popular with time.
Demographics
There were 15 (15%) male and 83 (85%) female respondents in the first survey. There is a preponderance of women compared with NHS Employer’s data,21 where 77% of NHS employees are reported to be women. NHS employer’s data also show fewer female NHS consultants than junior doctors and fewer senior female NHS clinical staff, excluding doctors and dentists, compared with junior.21 There is a need for more women to be drawn into leadership roles, making inclusive leadership programmes such as this necessary.
Seventy-six (78%) identified as white, 17 (17%) of black and minority ethnic background, 3 (3%) mixed race and 2 (2%) preferred not to say, in the first survey. Workforce Race Equality Standard (WRES) data report fewer board members (8.4%), very senior managers (7.7%) and senior doctors are from black and minority ethnic background.5 The higher representation of IGH fellows with a black and minority ethnic background adds further evidence to its inclusivity.
Career Path
Respondents most commonly took part in the programme as part of a career break, 52 (53%) in the first survey and 14 (29%) in the second. Other times mentioned were taking part in the programme at the end of a contract or as an ‘Out of Programme Experience’. Fifty-one (52%) fellows from the first survey and 26 (55%) from the second felt that completing the fellowship had a substantial impact on their career path, with only one fellow from each survey reporting that there had been no impact. There is an increase from the first (37 (38%)) to the second survey (20 (43%)) in the percentage of respondents who felt that they were now doing a job that they would not have done prior to completing the fellowship.
Both surveys illustrate an increase in the number of fellows in a more senior clinical role, particularly when looking at medical training grades, after completion of the fellowship. This is partly explained by the natural career progression of trainee doctors. There are more consultants and GP partners after completion of the fellowship and several doctors took on additional roles such as Medical/ Clinical Directorships and Company Directorship. There is a greater variety of job roles with a number of fellows changing the focus of their career path, for example working for the Department of Health, NHS England/NHS Improvement and the Civil Service. These changes are greater in the first survey where we are looking at a longer-term follow-up, suggesting that the effect on career change is long lasting.
Leadership and quality improvement
On completion of the programme many of the respondents from the first survey described feeling better informed about QI methodology and how it can make a difference. When asked about their current job roles, some fellows felt they had better knowledge and ability to take on QI projects and some reported improved confidence in being a leader. A few described an improved understanding of global health. This was the same in both surveys. Sixty-five per cent of the respondents in both surveys felt involvement in the programme had developed their leadership behaviours substantially. A few respondents from the first survey state using improved team member engagement, communication skills, a better understanding of themselves and improved project management skills in their current job role.
A number of fellows specifically mentioned that their learning has helped with managing COVID-19 challenges. A few fellows reported an overall increase in confidence (challenging the status quo, speaking up, put themselves forward for projects) which was the most commonly mentioned area. Other areas mentioned were a better understanding of what leadership behaviours are and becoming more self-aware/reflective.
The Mentors
Eighty-seven (89%) of respondents in the first and 45 (96%) in the second felt that having a mentor supported their leadership development.
Program feedback
Ninety-eight per cent of all fellows from both surveys reflected that they would recommend the fellowship to others. The most commonly reported areas that the IGH team do well were general support and guidance, the use of mentors, programme induction and the availability of postplacement opportunities (eg, becoming an IGH mentor). Things the programme could do to improve the programme are summarised in table 1.
Programme feedback—‘what one thing could the IGH team do differently to improve the program’, most commonly mentioned themes
Discussion
Most of this group of fellows felt that involvement in the IGH programme developed their leadership behaviours substantially, and they improved their knowledge of QI methodology and improved their confidence in being a leader. There is an increase in the number of senior roles taken up on completion of the programme, and the effect on career trajectory is long-lasting. As the programme has grown, looking for leadership or personal development as a motivation for applying to the programme has become more common, reflecting the increasing focus on leadership within training curricula and revalidation.13 Previous programme evaluations have also shown a growth in leadership skills and behaviours.22 23 A more recent evaluation provides evidence of both vertical and horizontal leadership development in IGH fellows and concludes that the programme creates more mature, adaptable and culturally aware leaders (accepted for publishing, ‘a qualitative analysis of vertical leadership development among NHS healthcare workers in low to middle income country settings’, January 2020).
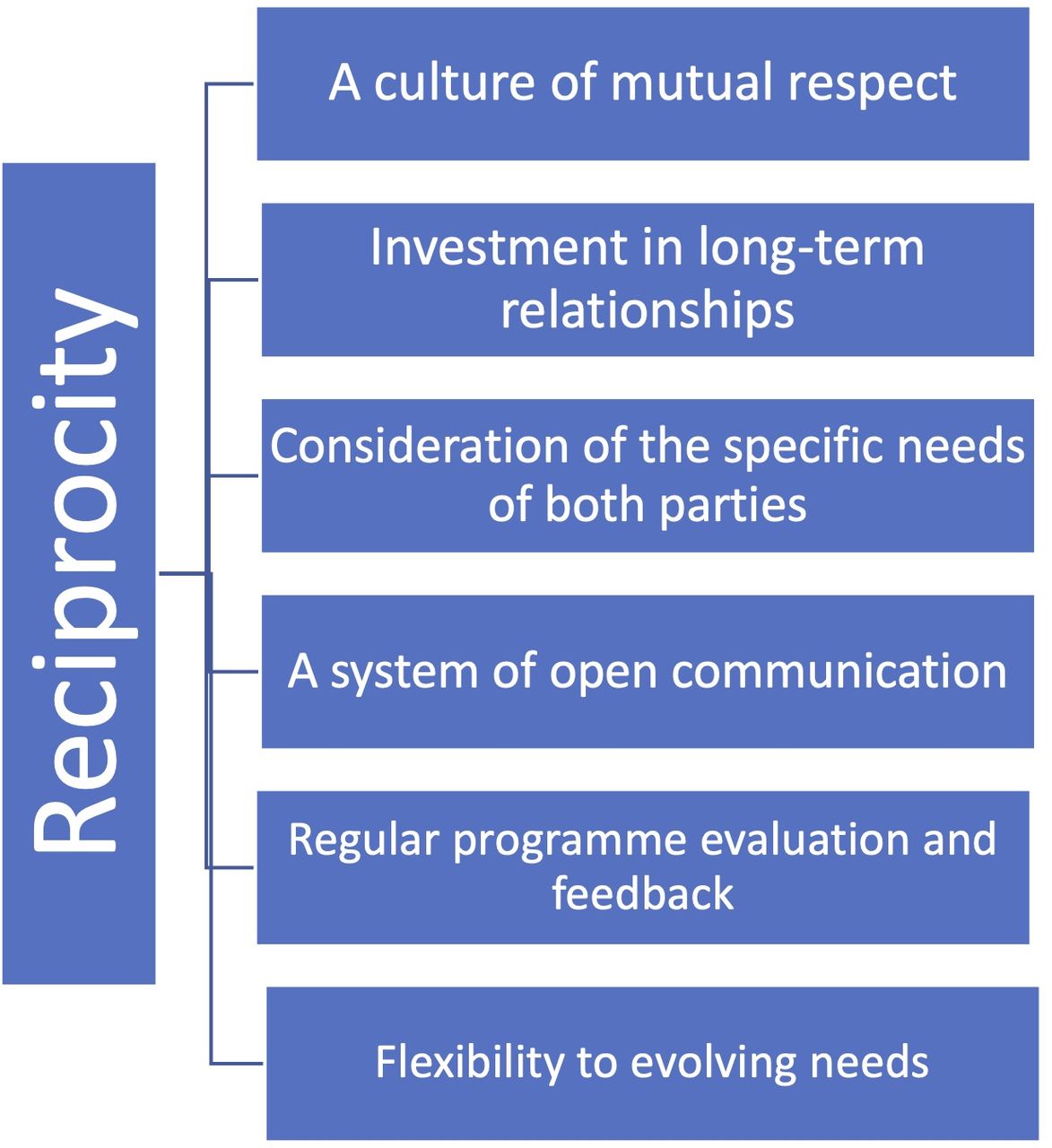
The use of a UK programme evaluation alongside the overseas perspectives aims to create a balanced understanding of the programme’s outcomes, highlighting the IGH culture of reciprocity. Reciprocity is seen here to be created by a culture of mutual respect. The needs of both parties are different, and consideration of these individual and specific needs creates mutual benefit. As described in the overseas perspectives, the low-income or middle-income country seeks development in their local healthcare system, aiming to improve the health outcomes of their citizens and develop their healthcare workers. For the UK, the need is to create leaders that are able to work within the complex and ever-changing environment of the NHS. Spending time developing individual long-term relationships through long-standing organisational partnerships creates a cohesive team that spans country borders. A system of open communication and regular programme evaluation, such as that presented here, produces flexibility to the evolving needs of both parties. Central concepts for creating reciprocity within a global health programme, drawn from the IGH experience, are outlined in figure 3.
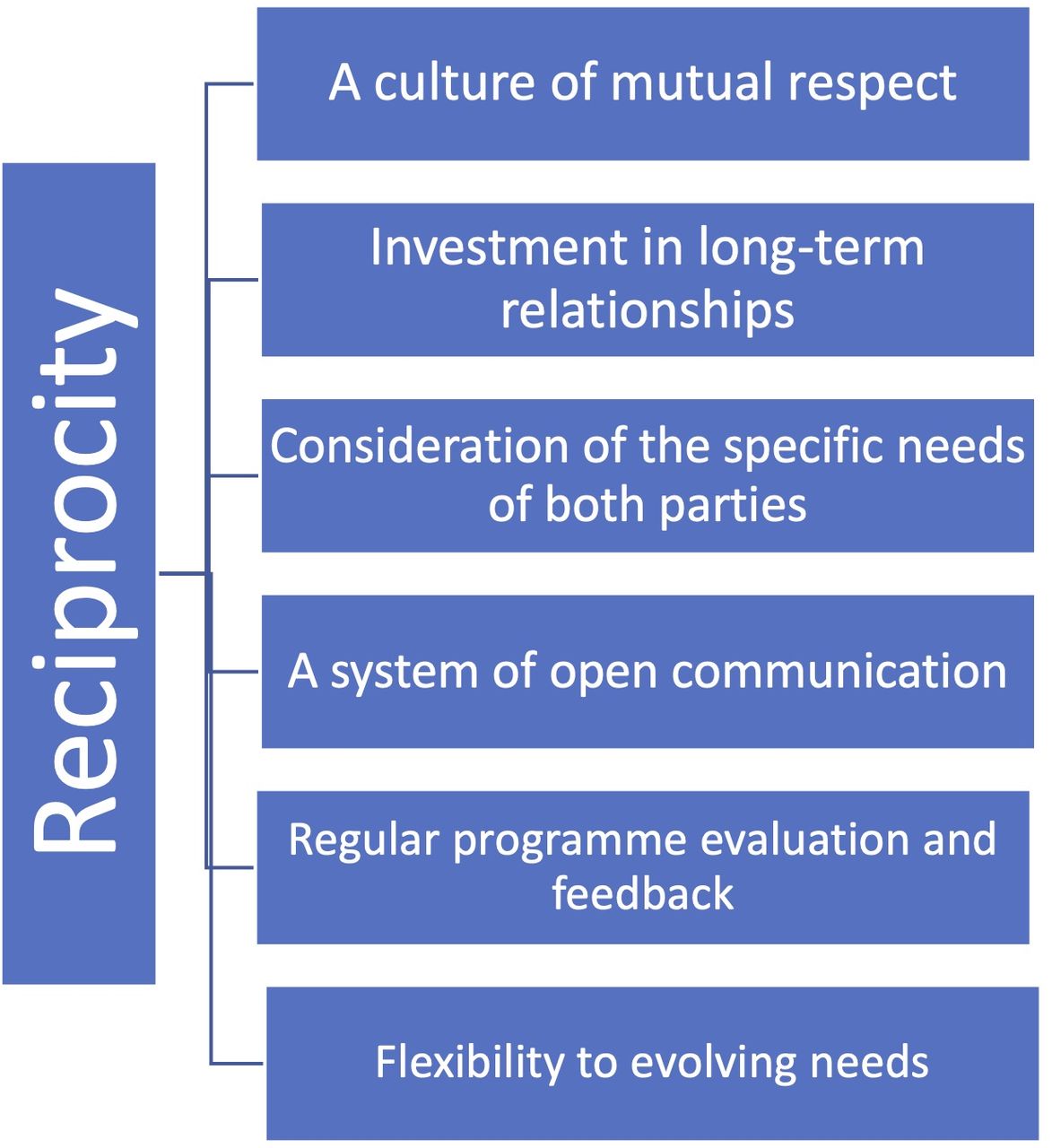
Emergent themes to running a reciprocal global health programme.
The proportion of women taking part in the IGH programme is higher than the percentage of female NHS employees.21 Women are known to be under-represented in more senior clinical NHS roles.4 The IGH programme also has a 20% representation of black and minority ethnic backgrounds; these groups are known to be under-represented in NHS leadership positions.5 The IGH programme is therefore developing both women and black and minority ethnic leadership behaviours and capacity within the NHS. The programme is also attracting a multidisciplinary group of NHS workers, although the majority are still junior doctors. Evidence is building of the inclusive nature of the programme, although more work is needed to understand exactly how and why. The proportion of other professions who take part in the programme must be increased. This particularly relates to nurses, who not only make up 50% of all professionally qualified clinical staff24 but also report their most important factor when looking for a new role as ‘opportunities for development’.25
The IGH programme has faced many challenges over the years. Some have successfully been overcome such as the maintenance of long-standing health partnerships and recruitment to mentor and PLL roles through a growing network of IGH alumni, while others remain a problem. Attracting a more multidisciplinary group of fellows to the programme remains an issue likely due to the difficulty faced in being granted leave from NHS roles, as does ensuring timely completion of fellow reports and achieving sustainability in health service improvements in the low-income or middle-income countries.
Recommendations
While the in-country case studies have shed light on the impact of the programme on the host institutions, more work is needed to assess improvements in local healthcare systems and also development of the in-country healthcare workers. A semistructured interview or survey looking at local benefits is suggested. More work is needed to understand how and why the IGH programme is attracting women and black and minority ethnic groups into leadership, if this translates to their taking up NHS leadership roles and if this ultimately leads to improved NHS outcomes.
Conclusion
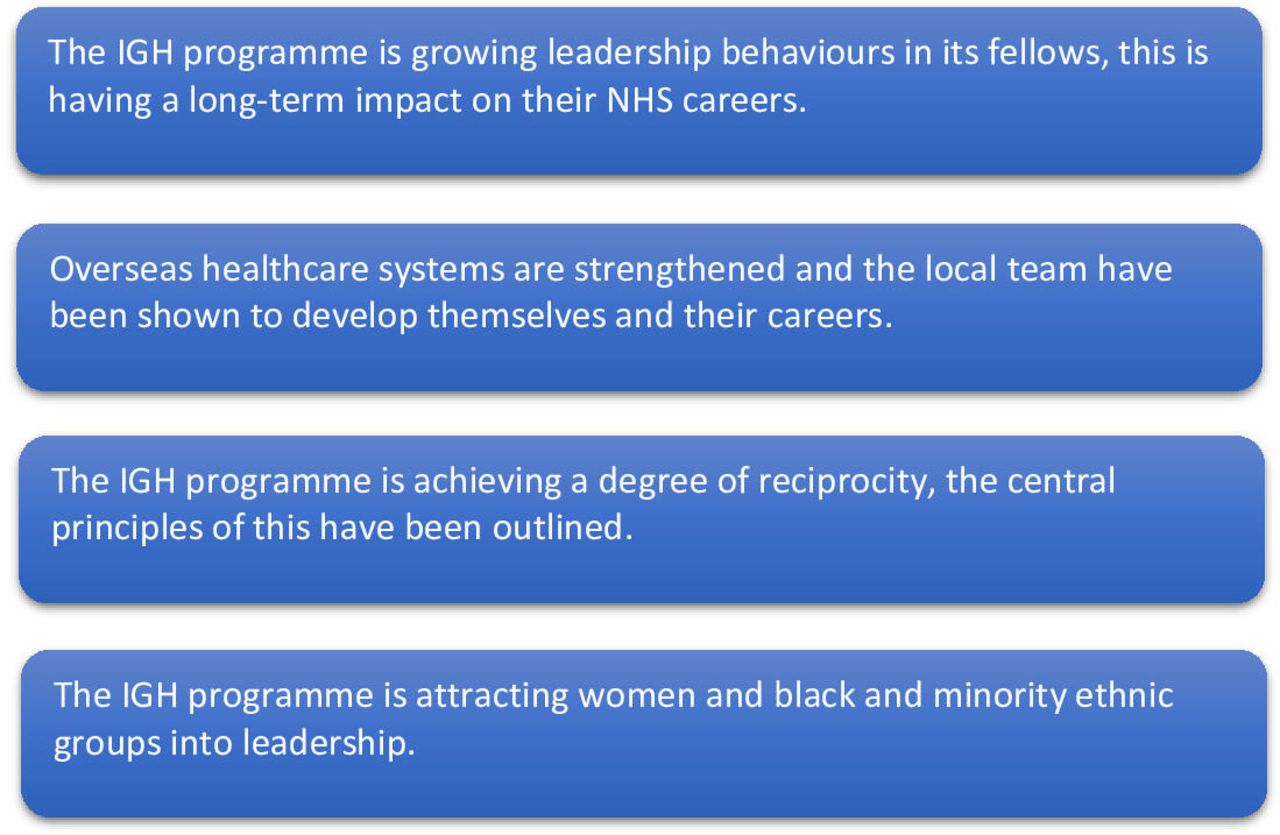
The IGH programme has been running for over 12 years, from its inception the goal has been to develop leadership skills in NHS employees, while contributing to the development of healthcare systems in low-income and middle-income countries. As time has progressed the organisation and delivery of this programme has evolved, building on the feedback and experience of previous years. The result is a truly unique leadership development programme that attracts diversity in both gender and ethnicity into leadership within the NHS. The IGH programme builds long-term health partnerships with its overseas team. Here, reflective accounts from overseas partners have been used to outline the impact of the programme on partnership sites. Not only have healthcare systems strengthened but the local team also have developed themselves and their careers(figure 4)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Summary box of key messages. IGH, Improving Global Health; NHS, National Health Service.
This article outlines how working in partnership with low-income and middle-income healthcare systems, to share knowledge and improve health is an effective strategy for working within the global health setting. The experiences of the IGH programme demonstrate that it is possible to design global health programmes that are mutually beneficial, an approach to this has been outlined here.
The two words that are central to the IGH programme are, inclusivity and reciprocity, these concepts are key to its aim of supporting sustainable change while stimulating leadership development in its fellows. It is hoped that the data and feedback outlined here will provide a valuable insight to other programmes who aim to address similar problems.
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Acknowledgments
Deborah Watts for help in conducting the programme evaluation. Dr Ian Kemp and Katy Grant for help in coordinating the work.
Footnotes
Handling editor Seye Abimbola
Twitter @Munichan2, @Myint Oo (@myintoo)
Contributors A-MS was responsible for planning, conduct and reporting. FK was responsible for planning, conduct and some reporting. MO and MK both wrote sections of the report. VR was responsible for some conduct, some reporting and also proof reading. VW was responsible for some of the conduct. HS was responsible for proof reading.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.