Article Text

Abstract
Introduction As countries approach the UNAIDS 95-95-95 targets, there is a need for innovative and cost-saving HIV testing approaches that can increase testing coverage in hard-to-reach populations. The HIV Self-Testing Africa-Initiative distributed HIV self-test (HIVST) kits using unincentivised HIV testing counsellors across 31 public facilities in Malawi, South Africa, Zambia and Zimbabwe. HIVST was distributed either through secondary (partner’s use) distribution alone or primary (own use) and secondary distribution approaches.
Methods We evaluated the costs of adding HIVST to existing HIV testing from the providers’ perspective in the 31 public health facilities across the four countries between 2018 and 2019. We combined expenditure analysis and bottom-up costing approaches. We also carried out time-and-motion studies on the counsellors to estimate the human resource costs of introducing and demonstrating how to use HIVST for primary and secondary use.
Results A total of 41 720 kits were distributed during the analysis period, ranging from 1254 in Zimbabwe to 27 678 in Zambia. The cost per kit distributed through the primary distribution approach was $4.27 in Zambia and $9.24 in Zimbabwe. The cost per kit distributed through the secondary distribution approach ranged from $6.46 in Zambia to $13.42 in South Africa, with a wider variation in the average cost at facility-level. From the time-and-motion observations, the counsellors spent between 20% and 44% of the observed workday on HIVST. Overall, personnel and test kit costs were the main cost drivers.
Conclusion The average costs of distributing HIVST kits were comparable across the four countries in our analysis despite wide cost variability within countries. We recommend context-specific exploration of potential efficiency gains from these facility-level cost variations and demand creation activities to ensure continued affordability at scale.
- HIV
- health economics
- AIDS
- public health
- diagnostics and tools
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed under the terms of the Creative Commons Attribution IGO License (CC BY NC 3.0 IGO), which permits use, distribution,and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organization or products. The use of the WHO logo is not permitted. This notice should be preserved along with the article’s original URL.Disclaimer: The author is a staff member of the World Health Organization. The author alone is responsible for the views expressed in this publication and they do not necessarily represent the views, decisions or policies of the World Health Organization.
Statistics from Altmetric.com
Key questions
What is already known?
HIV self-testing has been proven to be acceptableand effective at reaching populations left behind byconventional testing approaches. Community-baseddoor-to-door distribution of HIV self-testing has effectively reached men and first-time testers. Thereare economies of scale to the community-based distribution of HIV self-testing with personnel costs asan important cost driver.
What are the new findings?
We evaluated the costs of integrating HIV self-testing to existing testing services in public health facilities across four Southern African countries. We found that costs of integrating HIV self-testing in the public health facilities ranged from US$4.27-US$13.42 per kit distributed. Personnel and cost of test kits were important cost drivers. Time-and-motion studies showed that non-compensated healthcare workers spent between 20-44% of the observed workday on direct and indirect HIV self-testing activities. There are existing facility-level economies of scale and efficiency gains from integrating HIV self-testing to existing testing services.
What do the new findings imply?
Our results inform resource needs for implementers seeking to integrate HIV self-testing to existing testing services. We bring awareness to the staff time commitments required by such facility-based integrated services. We additionally emphasize on the need for context when deciding how and extent of integration
Background
UNAIDS set the 95-95-95 targets with the first 95 aiming for 95% of people living with HIV (PLHIV) being aware of their status by 2030.1 These fast-track targets have contributed to unprecedented progress towards ending the AIDS epidemic, especially in Eastern and Southern Africa, the region most affected by the epidemic.2
Despite this progress, the region still faces challenges in reaching men and key populations with testing.2 Some of the hindrances to accessing testing include lack of convenient and accessible testing options especially for rural communities, high indirect user costs in accessing testing and privacy concerns associated with their test results.3–6
HIV self-testing (HIVST), which is the process whereby a person collects their specimen, performs an HIV test and interprets their own results in private, can increase the number of PLHIV who are aware of their status and initiate treatment.7 HIVST provides an opportunity for discretion and convenience when testing and is highly acceptable among young people, adult men and first-time testers.3 7 8
We explore the costs of integrating HIVST into existing HIV testing services in public primary health facilities in Malawi, South Africa, Zambia and Zimbabwe between 2018 and 2019. Service integration involves joining together different services to maximise technical efficiency through economies of scale and scope, allocative efficiency and health outcomes.9 10 Previous work on integration of HIVST into outpatient services in Malawi reported an increase in outpatient testing when compared with standard of care (SoC).11
To our knowledge, this is the first multicountry cost analysis of the integration of HIVST into public health facilities. Such information is essential to designing sustainable and cost-effective models of HIVST as countries approach the UNAIDS 95-95-95 targets. Previous studies reporting costs of distributing HIVST in the region were either on a small scale12 or focused on the community-based distribution of HIVST.5 13 14 These studies reported average full costs (cost per kit distributed) in 2019 US dollars of $9.66 and $8.91 for Malawi, $17.70 for Zambia and $14.91 for Zimbabwe5 13 and average incremental costs of $15.40 and $14.00 in early and later phases of a community-based distribution of HIVST in Lesotho, respectively.14 The only other cost analysis of HIVST integration into facility-based testing services was conducted in Malawi and reported average costs of $4.99.15
Methods
Study overview
HIVST distribution was done by unincentivised Department/Ministry of Health staff (HIV testing counsellors) supported by Population Services International (PSI) in Malawi and Zimbabwe, Society for Family Health in Zambia and the Wits Reproductive Health and HIV Institute in South Africa. Unitaid funded the supporting partners and commodities under the Self-Testing Africa (STAR) Initiative. Primary and secondary distribution approaches for HIVST were implemented. Primary distribution of HIVST involved collecting a test kit for one’s use on-site, while secondary distribution involved collecting a test kit for use by sexual partners off-site. Table 1 provides a summary of the distribution approaches by country.
Integrated distribution of HIV self-tests into routine HIV testing services by country
Integration was from the first point of encounter with the facilities’ waiting area where clients were briefed on HIVST as they waited for their consultations. Willing clients would visit the HIV testing services (HTS) room and opt for either a provider-administered finger prick test or provider-assisted oral-fluid based HIVST (which could be immediately confirmed by a facility-based provider in the event of a reactive result). In the secondary distribution channel, willing pregnant women attending antenatal care, where the HIVST kit was offered for the partner at their first visit or HIV positive clients (newly diagnosed or enrolled in the ART programme), were offered kits for use by their sexual partners. The sexual partners were encouraged through the recipient of the HIVST kit to visit the facility for a confirmatory test if they screened positive. Online supplemental figure A1-A4 in the appendix give more detailed information on the integration process in each country.
Supplemental material
South Africa’s HIVST kit distribution and cost analysis was carried out across eight facilities in Gauteng and North West Provinces. In Zambia, distribution and cost analysis took place in two facilities in Lusaka district, while in Zimbabwe, costing was carried out for distribution in two large facilities in Mashonaland East. The Zimbabwe facilities were purposively sampled based on their proximity to Harare, which is where the country’s PSI headquarters was located. Malawi’s distribution was implemented as a three-arm pragmatic cluster randomised trial in 27 facilitiess in the Southern region.16 The arms comprised SoC, HIVST-only and HIVST plus financial incentive (HIVST+FI). SoC arm offered the ANC and index clients letters inviting their partners to the facility for an HIV test. The HIVST-only and the HIVST+FI arms offered HIVST in addition to the invitation letters. In the HIVST-only arm, partners were encouraged to come to the facility only if they had screened positive. In the HIVST+FI arm, partners were encouraged to come to the facility regardless of their screening result and were given a US$10 incentive as reimbursement for their time plus transport. We analysed the costs of all three arms.
Patient and public involvement
Patients and/or the public were not involved in the design, recruitment, conduct, reporting or dissemination plans of this research.
Cost analysis
Economic costs of HIVST integration were estimated from the providers’ perspective, with data collected between 2018 and 2019 and reported in 2019 US dollars. We converted local currencies to their US$ equivalent based on each country’s average exchange rate for 2019 as sourced from the respective countries’ Reserve Bank websites.17–19 The costing process involved a combination of expenditure analysis in estimating financial costs and a bottom-up costing to identify and value any additional or donated items not included in expenditure records. We focused on HIVST costs alone because the HTS costs in this setting have been extensively studied and reported elsewhere.15 20
The expenditure analysis was used to track actual implementation expenses such as cost of buying the test kits and other supplies, salaries, transportation and storage. The bottom-up costing was used to identify and value donated items at the facility-level such as equipment and space. At the facility-level, we only included economic costs directly related to HIVST distribution such as the counsellors’ time, facility space and equipment, and excluded indirect costs such as overheads (utilities and facility security).
The costs were categorised into capital and recurrent. Capital costs included project start-up costs, training, sensitisation and equipment. Recurrent costs included operational costs such as personnel and per diems, supplies and cost of test kits, among other costs. Capital costs were annualised over the life course of the project, that is, 2 years. We used a discount rate of 3% as recommended in literature and to facilitate comparison with our earlier work in the same countries.13 14 20 21 We varied this discount rate between 0% and 15% to reflect the range in official rates across the countries.
The implementing partners introduced multiple models of distributing HIVST in addition to the facility integrated model. Shared costs between models were allocated based on the assumptions presented in appendix online supplemental table A1. The allocation factors for shared costs included the proportion of distributors trained, kits distributed, direct expenditure and vehicle mileage by model, among other variables.
we used a combination of methods to allocate the time of facility staff involved in other activities alongside HIVST distribution, . In all countries except Zambia, we undertook time-and-motion studies to estimate provider time for the HIVST process. We could not conduct time-and-motion studies in Zambia due to delays in obtaining ethics clearance within the project implementation phase. There, we retrospectively interviewed the counsellors to understand the proportion of time allocated to HIV testing and HIVST services. We asked the counsellors to estimate the percentage of time allocated to HIV testing services and of this, the percentage allocated to HIVST services. We converted these proportions to equivalent overall HIV testing and HIVST time in minutes based on the counsellors stated working hours.
In South Africa, the initial ethics approval provided for up to 3 hours of continuous observations of the counsellors; this was later revised to continuous observation of a full working day after ethics amendments. More than half of the observations included in this analysis were conducted during the 3-hour observation phase.
We obtained the counsellors’ salaries from the facilities and multiplied by the average time obtained from the time-and-motion studies and interviews to estimate the facility-level personnel cost of HIVST. Overall personnel costs are a combination of the facility-level personnel cost and personnel costs at the PSI, Society for Family Health and the Wits Reproductive Health and HIV Institute central-level offices.
Data collection tools were developed as part of a collaborative process under the STAR-Initiative consortium and standardised across the countries except for Zambia (for the time-and-motion tool only) where we could not conduct time-and-motion studies. The observations involved timing and recording on paper forms the counsellors’ activities throughout their working day. We used the same tools across all HIVST distribution models including the integrated facility-based distribution. Table 2 presents the activities and their description. The activities were broadly categorised into direct and non-direct patient services, with direct patient services capturing time spent in contact with patients. The direct patient services time was allocated directly to either HIVST or finger prick testing. The non-direct patient services time was allocated to HIVST or finger prick testing using direct HIVST or finger prick testing time as a proportion of total direct time as an allocating factor. Observations were done continuously by health economists who were trained on time-and-motion studies.
Time-and-motion activity codes
We further explored potential economies of scale by observing the incremental unit costs at facility-level as number of kits distributed increased. Economies of scale are efficiency gains from the increased scale of production achieved by spreading fixed costs over more units of output. Given the cross-sectional nature of this study, we could not observe economies of scale over time for each facility but overall relationship between unit costs and distribution scale within country.
Finally, a one-way sensitivity analysis was used to assess uncertainty around the cost estimates. We varied the discount rate from 0% to 15%, project life years from 1 to 3 years, counsellors' time on HIVST by ±50% and personnel costs by ±10%. Additionally, we varied all parameters together to assess the best-case and worst-case scenarios.
Results
HIVST kits distributed
A total of 41 720 kits were distributed across 31 facilities in the four countries: 24 553 (59%) kits were distributed through the primary distribution channel (Zambia and Zimbabwe), while 17 167 (41%) were distributed through the secondary distribution channel. In the Malawi trial, 1603 and 1903 were distributed through the HIVST-only and HIVST+FI arms, respectively (table 3).
Number of kits distributed by country
Time-and-motion studies
We conducted a total of 39 time-and-motion observations across Malawi (n=9), South Africa (n=28) and Zimbabwe (n=2); we interviewed 25 counsellors in Zambia. Across all four countries, only the counsellors working in the HTS section were involved in HIVST distribution. In South Africa, we conducted 19 observations for 3 hours each during the 3 hours of observation protocol phase and 9 observations for an average of 4 hours per observation during the longer observation protocol phase. We further observed an average of 7 hours per counsellor in Malawi, and the two observations in Zimbabwe were for approximately 5 hours each. There is a likely bias in the Malawi and Zimbabwe observations due to the small sample sizes; we have accounted for this by varying the counsellor’s time in the sensitivity analysis.
On average, a counsellor spent 32 min in South Africa to distribute a kit as presented in table 4. We could not perform a per kit analysis in Malawi and Zimbabwe due to potential small sample size bias. Overall, the counsellors spent an average of 20% and 44% of the observed time on HIVST activities in Malawi and South Africa, respectively. In the two observations in Zimbabwe, the counsellor spent an average of 68% of the observed time on HIVST. There was no clear variation across activities between the countries. Aside from HIVST, the counsellors spent a significant proportion of the observed time on finger prick testing and non-direct patient activities. The interviewed counsellors in Zambia reported spending an average of 21% of their workday on HIVST.
Average observed time per kit distributed in South Africa
Costs
The costs per kit distributed through the primary distribution channel were $4.27 in Zambia and $9.24 in Zimbabwe. The costs per kit distributed through the secondary distribution channels were $6.46 in Zambia, $8.66 in Malawi, $9.05 in Zimbabwe and $13.42 in South Africa. Table 5 provides a summary of the total costs of distributing HIVST kits across all facilities by country.
Total costs of HIV self-test kit distribution by country (2019 US$)
Personnel and test kit costs were the key cost drivers across all four countries (figure 1). Personnel costs ranged from 12% of total costs in Zambia’s primary distribution channel to 64% in South Africa. The hourly wage per counsellor was $1.10 in Malawi, $2.99 in Zambia, $3.32, $4.16 in Zimbabwe and $4.25 in South Africa. Test kit costs ranged from 17% of total costs in South Africa to 63% in Zambia’s primary distribution channel. Additionally, Malawi had relatively higher training costs accounting for 18% of total costs with the rest of the countries’ training costs ranging from 1% in South Africa to 8% in Zimbabwe. We could not completely ascertain why Malawi had higher training costs, though the most plausible explanation would be its unique implementation approach through a clinical trial. The South Africa implementation included a component of mHealth for linking clients screening positive to follow-on care.22 The unit cost for the mHealth intervention was $0.27, accounting for 2% of total costs.

Cost per kit distributed and cost drivers by country.
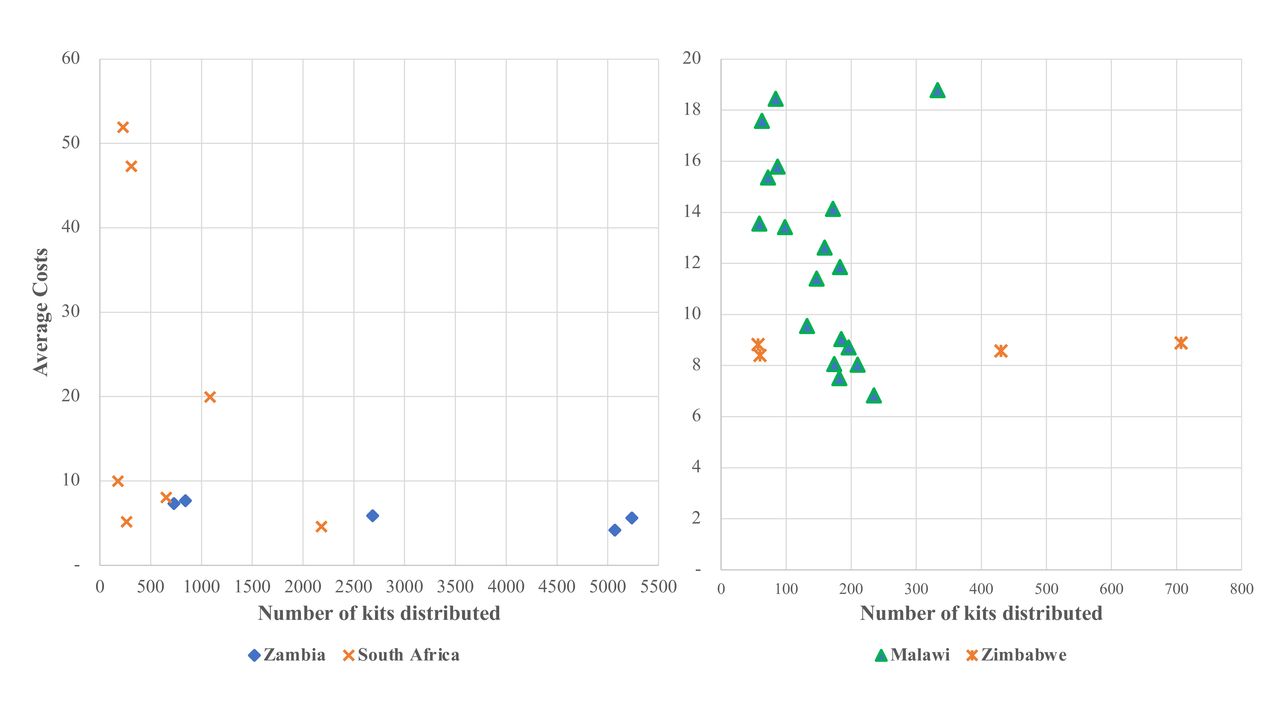
The country-level average costs conceal a wide variation in average costs by facility, especially in South Africa (figure 2). The facility-level average costs in South Africa ranged from $4.59 in a facility that distributed 2182 kits to $132 in a facility that distributed 103 kits. The facilities with the lowest average costs in South Africa were rural with low distribution volumes implying potential economies of scale to HIVST implementation. This facility-level cost analysis allowed us to explore other potential economies of scale across the 36 observations included in this analysis, as presented in figure 2. We observed potential economies of scale in Malawi and South Africa, that is, lower average costs in facilities that distributed a higher number of kits, but not Zambia and Zimbabwe.

Economies of scale by facility and country. We grouped countries by ranges of kit volumes, note that the graphs are not using the same scale. For ease of presentation, we excluded one facility in South Africa with kit volume of 103 and average cost $132 and one facility in Zambia with kit volume 13 104 and unit cost $3.78
Sensitivity analysis
Figure 3 presents the sensitivity analysis results where we varied the discount rate, project life years, counsellors’ time allocated to HIVST and personnel costs. In Malawi, the average cost was most sensitive to project life years, with the average costs rising by 21% when capital costs were assumed to have a lifespan of 1 year. In South Africa and Zimbabwe, the average cost was more sensitive to personnel costs, and in Zambia, the average cost was more sensitive to the providers’ reported time spent on HIVST. In Zambia, for instance, doubling the time spent on HIVST led to a 11% rise in average costs, compared with approximately 5% rise in South Africa and Zimbabwe. Across Malawi and South Africa, the average costs were least sensitive to changes in the discount rate.

{kind=link}
{kind=link}
{kind=link}
Sensitivity and scenario analysis by country. Note that the tornado diagrams are not drawn to the same scale. Base case in Zambia and Zimbabwe combines primary and secondary distribution unit costs.
Discussion
We observed the costs of adding HIVST to existing testing services in public facilities. In Malawi, South Africa, Zambia and Zimbabwe, HIVST was distributed through primary and secondary distribution approaches using unincentivised HIV testing counsellors. Costs per kit distributed were comparable across the countries. However, there was a wide variation in the average costs at the facility-level, driven mainly by the variability of costs in South Africa with the costs at the facility-level varying between $4.59 and $132. This study fills a gap in literature by reporting multicountry costs of integrating HIVST in public facilities, which is a viable option as countries approach the last milestone of the UNAIDS first 95.
In Zambia and Zimbabwe, the average costs of the integrated distribution observed in this study were lower than the inflation adjusted average costs of community-based distribution of HIVST reported in our earlier work.13 The average costs of community-based distribution in Zimbabwe and Zambia were 1.6 and three times higher than facility incremental costs ($14.69 vs $9.14 in Zimbabwe and $17.00 vs $5.37 in Zambia), respectively. This is expected as the community-based distribution was a vertical intervention unlike the integrated facility distribution that leveraged on existing economies of scope through shared infrastructure and human resource. It is worth noting that integration of HIV testing services may not always lead to efficiency gains in service delivery as observed elsewhere23 and in the Malawi component of this study where the average costs of the facility and community-based distribution in Malawi were comparable, that is, $8.66 versus $8.58, respectively.
Furthermore, despite the time-and-motion study raising generalisability concerns due to majority of the observations coming from South Africa, the results still offer insight into time demanded by HIVST from the counsellors. Counsellors spent at least 20% and 44% of the observed workday on direct and indirect HIVST activities in Malawi and South Africa. These results are informative to the time burden on the counsellors introduced by HIVST and have implications for the sustainability of HIVST scale-up. The degree of integration and the counsellors’ perception of HIVST are important factors in ensuring sustainability. HIVST needs to be horizontally integrated to ensure that the counsellors perceive it as a part of their routine. A viable alternative is unassisted primary distribution of HIVST, which has the potential of reducing staff time commitment especially for heavily understaffed facilities and improving linkage to follow on treatment or prevention services. For secondary distribution, pooled demonstration through for example videos streamed in the waiting areas also has potential of reducing direct patient time for the counsellors.
Additionally, the cost driver analysis demonstrated the importance of personnel and test kits in driving the integration costs. Our previous studies on facility-based HIV testing and community-based HIVST distribution also reported the costs of test kits and personnel as key cost drivers.13 20 The significance of personnel costs as a critical cost driver cannot be understated, as demonstrated by the time-and-motion studies. There is an opportunity cost to counsellors’ time—an intervention such as HIVST may be taking away time from the provision of other essential healthcare interventions especially in facilities that do not use lay counsellors for HIVST distribution. It is also important to ensure that HIVST is not introduced in facilities as a replacement for finger-prick testing but as an alternative testing option with the aim of expanding choice and supporting any potential efficiency gains.8
There are potential economies of scale to HIVST implementation. Average costs were lower in sites with high number of kits distributed due to shared fixed/overhead costs, and outlier facilities in South Africa were rural with low number of HIVST kits distributed. The average costs for such facilities need to be evaluated not relative to the high-volume facilities with low average cost but the counterfactual for such rural areas, no testing for the populations left behind.
Finally, this study has the advantage of being a multicountry costing study on integrating HIVST to existing testing services in 31 public facilities. This gives us a better understanding of the feasibility and cost implications of such an approach across countries. The time-and-motion studies enabled us to understand the time commitments required by unincentivised counsellors in an integrated approach of delivering HIVST in public health facilities. We propose room for efficiency gains at the facility-level, as demonstrated by the heterogeneity in facility-level costs24; this could be further explored using data envelopment analysis.25 We also recommend demand creation activities and continued kit price negotiations to ensure the intervention’s sustainability and continued affordability, especially at scale-up.
Limitations
There are several limitations to this study. A central limitation is that a substantial sample (58%) of the cost facilities was based on a trial. Despite excluding research costs, there may be higher protocol-induced resource use costs, and uptake, which may not be observed at scale-up.
There is also a likely upward bias in the observed time counsellors spent on HIVST due to Hawthorne effect, whereby individuals change their behaviour under observation.26 If the counsellors expected a financial incentive from HIVST integration, there was potential for them to spend more time on HIVST distribution during the observations. Nonetheless, we deem it advantageous to collect the time-and-motion data rather than basing the estimation of personnel resource costs solely on retrospective interviews, which is subject to the same bias but with the added challenge of recall bias.
An additional limitation is our inability to construct an index of integration to assess the complex nature of integration at the facility-level and to understand the sources of heterogeneity in facility-level cost due to lack of data.9 27
Finally, constructing cost functions would have been more informative in exploring potential sources of cost heterogeneity at the facility-level. We had few facilities within the countries with even more limited variables collected per facility to fully parameterise a cost function analysis. However, aside from South Africa, the rest of the countries’ average costs were more homogenous, suggesting potential uniformity in integrated service delivery.
Conclusion
We conducted a cost analysis of an intervention that integrated HIVST into existing HIV testing services in public facilities in Malawi, South Africa, Zambia and Zimbabwe. The average cost of integrating HIVST into public facilities ranged from $4.27 to $13.42 per kit distributed between countries. Personnel and cost of test kits were the critical cost drivers. We recommend taking the context into account when integrating HIVST into existing testing services. Finally, where staff time may be a constraint for conventional testing, HIVST may help alleviate this by enabling clients to have unassisted testing.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Ethics approvals for the costing work were obtained from research ethics committees of the London School of Hygiene & Tropical Medicine (Ref. # 15408, Ref. # 11 738 for Zimbabwe) and the Malawi College of Medicine (P.02/18/2352), Medical Research Council of Zimbabwe (Ref. # MRCZ/A/2038), the Human Research Ethics Committee (Medical) of the University of Witwatersrand (Ref. # M180379) and the Institutional Review Board of Boston University School of Public Health (IRB # H-37713).
Acknowledgments
We acknowledge the role played in enabling the data collection for this paper by the Ministries of Health in Malawi, Zambia and Zimbabwe and the Department of Health in South Africa, the staff and patients of the clinics involved and staff at Population Services International, Society for Family Health, Wits Reproductive Health Institute and the Malawi-Liverpool-Wellcome Trust Clinical Research Programme. Parts of this analysis were funded through the grant 'Enhancing the evidence-base of HIV Self-testing for young men' (BMGF OPP1189095) to Ezintsha, a division of Wits RHI, and HE2RO. We are grateful for the assistance of Vinolia Ntjikelane, Nonhlanhla Tshabalala, Clive Ramushu, Sandra Chidawanyika, Saviour Mphande and Progress Chiwawa with the data collection for the time-and-motion study and the cost analysis overall.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Lei Si
Twitter @cmangenah01, @Euphemia4, @ccasejohn
Contributors All authors were involved in the design and implementation of the study.
Funding The study is funded by Unitaid, grant number: PO#8477-0-600. ELC is also funded by theWellcome Trust (WT091769). Parts of this analysis were funded through the grant 'Enhancing the evidence-base of HIV Self-testing for young men' (BMGF OPP1189095) to Ezintsha, a division of Wits RHI, and HE2RO.
Disclaimer The opinions expressed are those of the authors and do not represent UNAIDS' position.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.