Article Text

Abstract
Introduction Community-based strategies can extend coverage of HIV testing and diagnose HIV at earlier stages of infection but can be costly to implement. We evaluated the costs and effects of community-led delivery of HIV self-testing (HIVST) in Mangochi District, Malawi.
Methods This economic evaluation was based within a pragmatic cluster-randomised trial of 30 group village heads and their catchment areas comparing the community-led HIVST intervention in addition to the standard of care (SOC) versus the SOC alone. The intervention involved mobilising community health groups to lead 7-day HIVST campaigns including distribution of HIVST kits. The SOC included facility-based HIV testing services. Primary costings estimated economic costs of the intervention and SOC from the provider perspective, with costs annualised and measured in 2018 US$. A postintervention survey captured individual-level data on HIV testing events, which were combined with unit costs from primary costings, and outcomes. The incremental cost per person tested HIV-positive and associated uncertainty were estimated.
Results Overall, the community-led HIVST intervention costed $138 624 or $5.70 per HIVST kit distributed, with test kits and personnel the main contributing costs. The SOC costed $263 400 or $4.57 per person tested. Individual-level provider costs were higher in the community-led HIVST arm than the SOC arm (adjusted mean difference $3.77, 95% CI $2.44 to $5.10; p<0.001), while the intervention effect on HIV positivity varied based on adjustment for previous diagnosis. The incremental cost per person tested HIV positive was $324 but increased to $1312 and $985 when adjusting for previously diagnosed self-testers or self-testers on treatment, respectively. Community-led HIVST demonstrated low probability of being cost-effective against plausible willingness-to-pay values, with HIV positivity a key determinant.
Conclusion Community-led HIVST can provide HIV testing at a low additional unit cost. However, adding community-led HIVST to the SOC was not likely to be cost-effective, especially in contexts with low prevalence of undiagnosed HIV.
Trial registration number NCT03541382.
- other diagnostic or tool
- health economics
- HIV
- cluster randomized trial
Data availability statement
Deidentified participant data and data dictionary are available on request to the corresponding author. Data are available with investigator support following publication.
This is an open access article distributed under the terms of the Creative Commons Attribution IGO License (CC BY NC 3.0 IGO), which permits use, distribution,and reproduction in any medium, provided the original work is properly cited. In any reproduction of this article there should not be any suggestion that WHO or this article endorse any specific organization or products. The use of the WHO logo is not permitted. This notice should be preserved along with the article’s original URL.Disclaimer: The author is a staff member of the World Health Organization. The author alone is responsible for the views expressed in this publication and they do not necessarily represent the views, decisions or policies of the World Health Organization.
Statistics from Altmetric.com
Key questions
What is already known?
Community HIV strategies can extend coverage of HIV testing and diagnose HIV at earlier stages of infection. However, community-based strategies can be costly to implement, with community-led HIV self-testing (HIVST) a promising approach for providing HIV testing services.
What are the new findings?
Community-led HIVST delivered HIV testing at a low additional unit cost.
The incremental cost per person tested HIV positive was sensitive to variation in prevalence of HIV positivity. Therefore, the addition of community-led HIVST to the standard of care was not likely to be cost-effective in contexts with low prevalence of undiagnosed HIV.
What do the new findings imply?
Community-led HIVST may be more cost-effective if targeted to settings and populations with more substantial prevalence of undiagnosed HIV.
Introduction
Expanding access to HIV testing services (HTS) is important for early diagnosis to reduce HIV-related morbidity and mortality and prevent HIV transmission.1 In 2018, approximately 1.7 million people were newly infected with HIV, with 800 000 new cases in southern and eastern Africa.2 Almost one-fifth of HIV-positive individuals were unaware of their HIV status.2 Demand and supply-side barriers to conventional facility-based HTS have resulted in poorer knowledge of HIV status among certain population subgroups and hindered achievement of HIV elimination goals.3 4
Aimed at addressing barriers to access, community-based strategies can extend coverage of HIV testing and diagnose HIV at earlier stages of infection but can be costly to implement.4 5 Meeting and maintaining high awareness of HIV status is dependent on identifying sustainable approaches for providing HTS beyond health facilities, especially with declining global funding for community health programmes.6 Moreover, as countries successfully scale-up HIV testing and treatment services, costs per new HIV diagnoses are increasing.7 To remain cost-effective, community-based HIV testing strategies must further minimise costs and maximise the proportion diagnosed, treated or linked to prevention.7
Community-led approaches involve engaging underserved communities in disease prevention and management.8 Through context-driven design and implementation, community participation in health programmes has been shown to improve health outcomes at low costs.9–12 HIV self-testing (HIVST), which is recommended as an additional strategy to reach underserved populations,13 could be introduced within a community-led framework to enable direct provision of HTS by communities and improve the coverage, efficiency and sustainability of community programmes.8
In this study, we evaluated the costs and effects of community-led delivery of HIVST within a pragmatic cluster-randomised trial comparing community-led HIVST in addition to the standard of care (SOC) versus the SOC alone.
Methods
Trial design, setting and participants
We conducted an economic evaluation of community-led delivery of HIVST using individual-level data on costs and effects generated from a cluster-randomised trial in Mangochi District, Malawi. Clusters, defined as group village heads and their catchment areas, were identified from communities served by five government primary health centres in one of the most HIV-prevalent districts in Malawi.14 Thirty clusters were randomised 1:1 to community-led HIVST in addition to the SOC or the SOC alone, which includes facility-based HTS. The aim of the trial was to determine whether the community-led HIVST intervention increased the proportion of the population who tested for HIV, especially among subgroups with high undiagnosed HIV, including adolescents, older adults and men. The trial protocol and analysis are reported separately.15 16
The trial was conducted through the Unitaid/Population Services International (PSI) HIV Self-Testing Africa Initiative (STAR) (http://hivstar.lshtm.ac.uk/). The study team included PSI Malawi, the Malawi-Liverpool-Wellcome Trust Clinical Research Programme and the Ministry of Health.
Procedures
The community-led HIVST intervention involved mobilising established community health groups to lead the design and implementation of HIVST campaigns. Established groups included community health action groups, who deliver basic health services with government community health workers (CHWs) at group village head level, and community volunteers, including village health committees, who oversee service provision at village level.
The intervention was delivered in groups of two-to-three clusters every 14 days and consisted of three main components: participatory workshops, trainings and HIVST campaigns. Community health action groups and CHWs were invited to a 2-day participatory workshop facilitated by the study team. To inform the design of an HIVST campaign in their respective areas, participants identified drivers of HIV, available HIV services and barriers to access, and underserved subgroups. Participants then determined how the campaign would be implemented, including plans for distribution of HIVST kits, support for linkage to routine HIV services and demand creation for HIVST. Afterwards, community volunteers attended 2-day trainings on how to support HIVST use, interpretation and linkage to routine HIV services. Volunteers were also trained on communicating HIV prevention messages, managing social harms, handling and storing kits, and collecting data.
Community volunteers then delivered 7-day HIVST campaigns under the supervision of community health action groups and CHWs. Implementation was based on strategies outlined by each cluster during participatory workshops. Inputs provided by the study team included the OraQuick HIV Self-Test (Orasure Technologies, Thailand), communications and instructional materials, data collection tools and a nationally standardised gratuity of MWK 7000 (US$10) per volunteer. Cluster residents aged 15 years and older were eligible to take an HIVST kit for themselves and an additional kit for secondary distribution.
The SOC, which was available in both study arms, included HTS provided by the Ministry of Health. HTS is primarily available at facility level through provider-initiated testing in outpatient services or client-initiated testing, or at community level through periodic outreach by health facilities. Lay healthcare workers performed HIV testing using finger-prick rapid diagnostic tests based on serial testing algorithms using Determine HIV-1/2 and Unigold HIV-1/2.
Cost measurement
Economic costs of the community-led HIVST intervention and the SOC were estimated from the provider perspective using global costing guidelines.17 Costing methods are more fully described in online supplemental text 1. Intervention costs were collected for the 5-month intervention period. Financial data were extracted from expenditure records, with each expenditure item allocated to a cost category and activity. Financial costs, which contributed to the majority of costs due to vertical implementation, were then supplemented with economic costs. Microcosting involved direct observations and interviews with the study team and community volunteers in three sites, with one site selected per subdistrict. Start-up costs included the costs of training and sensitisation and costs incurred during the start-up period in the month prior to the intervention. Implementation costs included costs of capital and recurrent inputs, including building and storage, equipment, vehicles, personnel, supplies and HIVST kits (unit price of US$2.50). Shared costs between HIVST distribution models and sites were allocated using the volume of HIVST kits distributed, reported time use by staff, mileage from the central office to sites, and weighted average of allocation factors. The value of resources donated by communities were captured but excluded from the analysis due to incomplete data collection.
Supplemental material
Costs for the SOC were retrospectively collected for a 12-month period. Using an ingredients-based approach, resources required to deliver HTS were identified by cost category and valued based on their quantity and unit price through observations and interviews with facility personnel in the five health facilities. Unit prices were US$0.98 for Determine and US$1.97 for Unigold. Overhead costs at the health facility level were allocated using the number of patients accessing outpatient services and HTS and reported time use by staff.
Start-up and capital costs were annualised using a 3% discount rate.17 An annualisation timeframe of 2 years was assumed for start-up costs, while the useful life for capital costs was dependent on input type. Wastage assumptions also varied by input type. Local costs were converted to 2018 US dollars using the median exchange rate over the analysis period.18 Overall and site-level unit costs for the community-led HIVST intervention and the SOC were estimated, with programme and facility registers respectively providing the number of HIVST kits distributed and the number of persons tested for the costing periods. The number of persons self-tested was obtained by adjusting the number of kits distributed with the proportion of kit usage reported from the postintervention survey for the outcome measurement.
Activity and site-specific unit costs were then combined with frequency of HIV testing and self-testing events in the last 12 months reported in the postintervention survey, with individual-level provider costs estimated for each survey participant.
Outcome measurement
For the economic evaluation, we measured the effect of the community-led HIVST intervention on the proportion tested HIV positive, defined as individuals who self-reported a positive HIV test in the last 12 months through the postintervention survey. To measure new diagnoses, we alternatively defined the proportion tested HIV positive as: (1) testing positive through the SOC or newly self-testing positive and (ii) testing positive through the SOC or self-testing positive and not on antiretroviral therapy (ART). HIV testing in the last 12 months was also included as an outcome of interest. Outcomes were captured over a 12-month period, since community-led HIVST was designed to be delivered as an annual intervention to a high HIV-prevalence population who might benefit from recurrent testing. Of note, data on previous diagnosis were only collected for individuals who self-tested and not for individuals who tested through standard HTS.19 We also did not account for confirmatory testing following HIVST .
Outcomes were measured through a postintervention survey administered 8–12 weeks after the start of the intervention in the community-led HIVST arm or corresponding dates in the SOC arm. Cluster residents were sampled to form the evaluation population. In each cluster, villages with at least 500 residents and located near the group head village were randomly selected for the survey. Households were then recruited in a clockwise spiral starting from a common location across selected villages, aiming to include at least 250 participants per cluster based on sample size calculations for the trial.15 Residents aged 15 years and older were eligible to participate in the survey, with written informed consent or assent obtained. Participants provided information on sociodemographic background and prior experience with HIV testing and treatment.
Statistical analysis
Incremental costs and effects were estimated using individual-level data from the postintervention survey. Analysis used intention-to-treat and cluster-level methods appropriate for cluster-randomised trials with a small number of clusters.20 To estimate the mean difference (MD) in costs, we used linear regression to adjust for sex, age group and imbalance between arms at the individual level. Covariate-adjusted residuals were then summed for each cluster and compared by arm using a t-test. Similarly, risk differences (RDs) for the proportion tested for HIV and tested HIV-positive were estimated using a cluster-level analysis, with logistic regression used at the individual level to obtain covariate-adjusted summary values.
The incremental cost per person tested and tested HIV positive were calculated as the ratio of adjusted incremental costs and adjusted incremental effects. Uncertainty was estimated using two-stage non-parametric bootstrap, whereby clusters were sampled in the first stage and individuals within clusters were sampled in the second stage, both with replacement.21 22 A shrinkage correction was applied.21 22 Incremental costs and incremental effects were calculated across 1000 bootstrap replicates and plotted on cost-effectiveness planes.23 CIs were estimated using bias-corrected percentiles.23 Cost-effectiveness acceptability curves were also generated from bootstrap replicates to illustrate probabilities for a range of willingness-to-pay values. Subgroup analyses were conducted to understand differences in individual-level costs and effects by sex. Statistical analysis used Stata V.14.0.
We compared the incremental cost per person tested HIV positive to a willingness-to-pay threshold of $315 across alternative outcome definitions. The threshold is based on a simulation study in Southern Africa, which showed that additional testing beyond the SOC was considered cost-effective if the cost per new diagnosis was below a threshold of 2018 US$315 and therefore strongly associated with the cost per disability-adjusted life year (DALY) averted below a threshold of 2018 US$500.7 The threshold represents opportunity costs of reallocating resources within an HIV programme from other HIV interventions to HIV testing and relevant to national programmes dependent on overseas funding.7 We aimed to improve comparability of our outcome to the threshold by adjusting for previous diagnosis among self-testers.
Sensitivity and scenario analysis
One-way deterministic sensitivity and scenario analysis assessed the impact of varying parameters on the mean cost per HIVST kit distributed and the incremental cost per person tested HIV positive. In sensitivity analysis, we varied cost assumptions, including the discount rate (none, 16%) and exchange rate (minimum, maximum).18 In scenario analysis, we varied inputs that were considered to be important cost determinants, including the price of HIVST kits from $0.98 (price of HIV RDTs) to $3.40 (unsubsidised price of HIVST kits).24 Furthermore, we modelled real-world scenarios for routine implementation under the Ministry of Health by varying personnel costs (±10%), start-up costs (±10%), lifespan of start-up costs (1 year, 5 years) and number of kits distributed (±10%). Parameters were selected based on scenarios evaluated in earlier STAR studies in anticipation of scale-up.24 We also estimated best and worst case scenarios for routine implementation by adjusting parameters that produced the lowest and highest values. Lastly, in addition to assessing alternative outcome definitions for HIV positivity, we assessed the impact of uncertainty using 95% CIs for the effect estimate.
Results
The community-led HIVST intervention was delivered in 15 clusters between 5 October 2018 to 17 January 2019. HIVST campaigns were implemented in each cluster, with 157 community health action group members and 190 community volunteers distributing 24 316 HIVST kits. The postintervention survey included 90.2% (3960/4388) and 89.2% (3920/4394) of listed residents in the community-led HIVST and SOC arms, respectively (online supplementary figure 1). Across arms, response rates were lower among men (83.5%, 3072/3677) compared with women (94.2%, 4808/5105). Participant characteristics are summarised in online supplemental table 1, with differences between arms observed for literacy, religion, ethnicity and self-reported health status.
Costs
The total provider cost of the community-led HIVST intervention was $138 624, which includes costs for the 5-month start-up and implementation period (table 1). The proportion of start-up and capital costs were respectively 10.3% ($14 308) and 9.4% ($13 023). Recurrent costs accounted for 80.3% ($111 293) of the total cost, with the main contributing inputs including test kits (46.0%) followed by personnel (25.3%) and vehicle operation and maintenance (4.2%). The mean cost per HIVST kit distributed was $5.70. Mean costs varied by cluster from $4.45 to $8.49, with lower costs achieved in clusters with higher volumes of kits distributed (online supplemental figure 2). The mean cost per person self-tested was $5.73, which was estimated based on self-reported kit usage among survey participants who collected kits (99.6%, 3128/3142).
Total and average unit costs of the community-led HIV self-testing (HIVST) intervention and standard of care (SOC)
From January to December 2018, the total provider cost of the SOC was $263 400 (table 1). Of total costs, capital costs were 3.0% ($7887), while recurrent costs were 97.0% ($255 513). In contrast with the community-led HIVST intervention, personnel (48.1%) contributed the largest proportion to costs followed by test kits (24.6%) and supplies (23.5%). The mean cost per person tested was $4.57, ranging from $2.90 to $6.41 by health facility.
Based on the frequency of HIV testing and self-testing events reported in the postintervention survey, participants in the community-led HIVST arm had a mean number of 1.66 tests in the last 12 months (online supplemental figure 3), providing a mean provider cost per person of $9.06 (table 2). In the SOC arm, the mean number of annual tests was 1.17, with a mean provider cost per person of $5.52. The adjusted MD was $3.77 (95% CI $2.44 to $5.10; p<0.001). Among men, the mean cost per person was $8.04 and $4.68 in the community-led HIVST and SOC arms, respectively. Mean costs were higher for women than men in both the community-led HIVST ($9.74) and SOC ($6.04) arms, reflecting higher frequency of testing among women. The MD in costs were similar among men (adjusted MD 3.57, 95% CI 2.33 to 4.81; p<0.001) and women (adjusted MD 3.91, 95% CI 2.49 to 5.32; p<0.001; p value for interaction; p=0.25).
Incremental costs and effects of community-led HIV self-testing (HIVST)
HIV testing
HIV testing in the last 12 months was higher in the community-led HIVST arm (84.9%, 3363/3960) compared with the SOC arm (65.7%, 2574/3920), with adjusted RD of 19.5% (95% CI 15.0% to 24.0%; online supplementary table 2). The intervention effect was greater among men (adjusted RD 23.1%, 95% CI 17.8% to 28.4%; p<0.001) than women (adjusted RD 17.2%, 95% CI 12.7% to 21.8%; p<0.001; p value for interaction=0.002). The incremental cost per person tested was $19.35 and lower for men ($15.44) than women ($22.67).
HIV positivity
HIV positivity was also higher in the community-led HIVST arm (2.6%, 104/3960) than the SOC arm (1.7%, 67/3920; adjusted RD 1.2%, 95% CI 0.3% to 2.0%; p=0.008), with more pronounced differences among women (adjusted RD 1.6%, 95% CI 0.5% to 2.6%; p=0.005) than men (adjusted RD 0.5%, 95% CI −0.5% to 1.5%; p=0.29; p value for interaction=0.06; table 2).
However, differences between arms were not observed when the outcome definition excluded previously diagnosed self-testers (adjusted RD 0.3%, 95% CI −0.4% to 1.0%; p=0.42) or self-testers on treatment (adjusted RD 0.4%, 95% CI −0.3% to 1.1%; p=0.27).
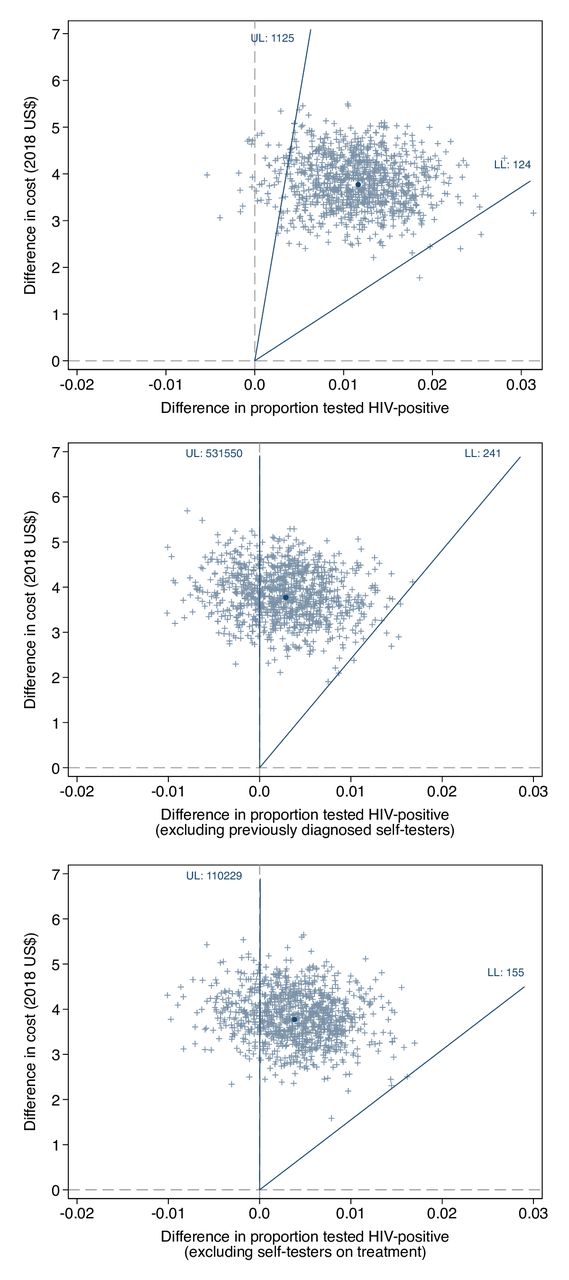
The incremental cost per person tested HIV positive was $324, and higher for men ($716) compared with women ($246) due to lower HIV positivity (online supplemental figure 4). The incremental cost per person tested positive was $1312 and $985 when previously diagnosed self-testers or self-testers on treatment were excluded. Bias-corrected confidence intervals are presented with cost-effectiveness planes in figure 1. The joint distribution of the difference in costs and difference in the proportion tested positive fell in the upper left and right quadrants of the cost-effectiveness plane, meaning incurred costs could potentially result in zero or negative benefits.
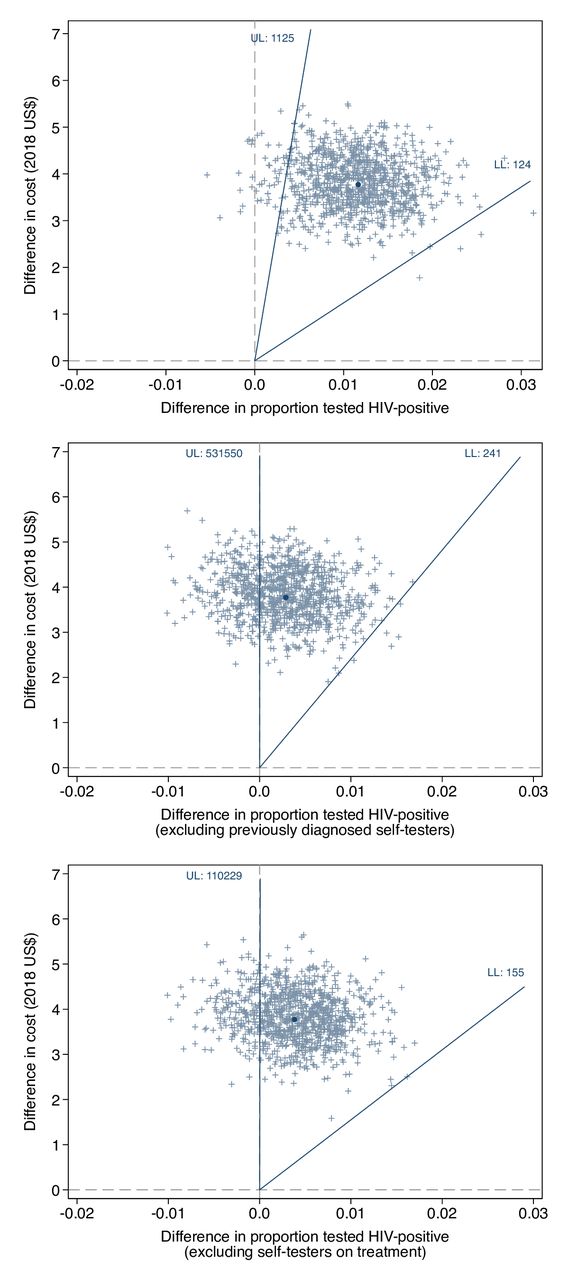
Cost-effectiveness plane for community-led HIV self-testing. Cost-effectiveness plane of adding community-led HIVST to the standard of care. The incremental cost per person tested HIV positive for alternative outcome definitions are illustrated. Each point represents the adjusted mean difference in cost (incremental cost) and adjusted risk difference in the proportion tested HIV positive (incremental effect) for one bootstrap replicate. The dark blue circle indicates the incremental cost per person tested positive and the dark blue line indicates the bootstrap confidence intervals using the bias-corrected percentile method. LL, lower limit; UL upper limit.
Cost-effectiveness acceptability curves are illustrated in figure 2. With respect to a threshold of $315 per positive test, cost-effectiveness probabilities varied depending on the outcome definition: 45.0% for testing HIV positive, 30.2% when excluding previously diagnosed self-testers and 21.2% when excluding self-testers on treatment.

Cost-effectiveness acceptability curves for community-led HIVST by scenario. Cost-effectiveness acceptability curves of adding community-led HIVST to the standard of care. Cost-effectiveness probabilities for the incremental cost per person tested HIV positive are plotted for alternative outcome definitions across a range of willingness-to-pay values. HIVST, HIV self-testing.
Sensitivity and scenario analysis
One-way sensitivity and scenario analysis for the mean cost per HIVST kit distributed and the incremental cost per person tested HIV-positive are presented in figure 3. Varying the price of the HIVST kit from $0.98 to $3.40 led to the largest changes in average costs, from $4.09 to $6.70. Best and worst case scenarios for routine practice, which varied personnel costs, start-up costs, lifespan of start-up costs and the volume of kits, yielded average costs ranging from $3.57 to $7.56. Results remained robust to variations in sensitivity analysis.

{kind=link}
{kind=link}
{kind=link}
Tornado diagram of one-way deterministic sensitivity and scenario analysis. Tornado diagram illustrating changes in the mean cost per HIVST kit distributed and incremental cost per person tested HIV positive based on variations to inputs. Light blue bars represent changes at minimum input values, while dark blue bars represent changes at maximum input values. LL, lower limit; UL upper limit.
Uncertainty associated with HIV positivity led to the largest changes in the incremental cost per person tested positive, ranging from $184 to $1141 based on 95% CIs for the effect estimate. In best and worst case scenarios modelling routine implementation and uncertainty in the effect estimate, the incremental cost per person tested positive varied from $105 to $1614.
Discussion
We conducted an economic evaluation within a cluster-randomised trial of community-led delivery of 7-day HIVST campaigns in Malawi. The community-led HIVST intervention showed low average cost of $5.70 per HIVST kit distributed, with test kits and personnel the main contributing costs. Individual-level provider costs were higher in the community-led HIVST arm than the SOC arm, demonstrating low substitution due to HIVST uptake among recently tested individuals. The intervention effect on HIV positivity varied based on adjustment for previous diagnosis. The incremental cost per person tested HIV positive was $324 but increased to $1312 and $985 when adjusting for previously diagnosed self-testers or self-testers on treatment, respectively. The addition of community-led HIVST to the SOC demonstrated low probability of being cost-effective, with HIV positivity a key determinant. Despite providing HIV testing at a low additional unit cost, community-led HIVST was not likely to be a cost-effective strategy, especially in contexts with low prevalence of undiagnosed HIV.
Universal HIV testing and treatment can be used to support reductions in HIV incidence in the general population,1 but financial sustainability remains a limiting factor. Our cost analysis showed a mean cost of $5.70 per kit distributed through the community-led HIVST intervention and $4.57 per person tested through the SOC. The largest contributors to intervention costs were test kits, personnel, and vehicle operation and maintenance. SOC costs were driven by personnel followed by test kits and supplies. Differences in resource use reflect the higher price of HIVST kits but lower cost of personnel from campaign-style implementation by community volunteers. The cost of supplies was also higher in the SOC due to recurrent use of medical supplies alongside provision of HIV RDTs. The average cost for HIVST implementation reported in this study is lower than costs previously reported for door-to-door distribution of kits in Malawi, both in rural (2017 US$8.15) and urban (2014 US$8.78) settings.24 25 Lower costs are likely influenced by the high volume of kits delivered within a short period of time in addition to pragmatic implementation through established community health groups, who are routinely activated to support basic health service provision.
Our findings highlight potential areas for cost reductions under scenarios modelling routine implementation by the Ministry of Health. Personnel salaries and per diems contributed substantially to costs and could be further reduced under routine practice. Packaging HIVST with other health interventions could also reduce the ratio of fixed costs, including personnel, to variable costs through economies of scope. Recurrent implementation could produce efficiency gains as community health groups become more familiar with HIVST and start-up costs are spread over a longer period of time. Minimising retesting among recently tested individuals or reducing the price of HIVST kits could additionally lower costs, with HIVST kits accounting for the majority of costs. Furthermore, community-led HIVST is likely to realise greater economies of scale as unit costs decrease with increasing volume of kits distributed.
A community-led approach has often been promoted as a mechanism to include context-specific knowledge and resources in health programmes.8 Implementation through community-driven systems could lower costs and expand the pool of available resources for service provision.8 Earlier studies have shown that community-led approaches can be less costly than vertically delivered strategies.26 However, there is a risk of shifting economic costs down to resource-constrained communities. In a multicountry study, community-led multidisease campaigns were less costly than the SOC, but higher median opportunity costs were reported by community volunteers.26 In our analysis, costs incurred by communities were not captured due to incomplete data collection, though community contributions observed by the study were relatively nominal and included donated building space, equipment and transportation. Opportunity costs were also captured through gratuity received by community volunteers.
Accounting for retesting among previously diagnosed self-testers or self-testers on treatment yielded an incremental cost per person tested HIV positive of $1312 and $985, respectively. Community volunteers were trained to advise against self-testing on ART to avoid false negative results. However, volunteers did not discourage self-testing among recently tested individuals or individuals known to be HIV positive but not on treatment. High prevalence of retesting among known HIV-positive individuals has previously been reported for both facility-based and community-based services, with retesting motivated by loss to treatment follow-up.27 In Malawi, desire to monitor sero-reversion was reported by female sex workers, while opportunity for HIV status disclosure was described among couples.28 29 Furthermore, we reported an increase in the proportion of testing at an additional mean cost of $19.35 per person tested, reflecting low substitution due to HIVST uptake among recently tested individuals. Reasons that have been reported for retesting among HIV-negative individuals included to monitor HIV status, respond to HIV risk exposure or facilitate partner testing.28 30 Pressure to self-test could also lead to unnecessary retesting but was reported to be limited in the main trial.16 Targeting of subgroups currently underserved by facility-based HTS could improve efficiency, with variable costs associated with HIVST kits higher than fixed costs. Equally, targeted distribution could heighten stigma around HIV testing and reduce uptake among priority subgroups. Under such conditions, wider implementation might be required to identify undiagnosed people living with HIV despite losses in efficiency.
Adding community-led HIVST to the SOC had 21%–45% probability of being cost-effective at a threshold of $315 per positive test. We used HIV positivity as an outcome but did not distinguish between newly and previously identified people living with HIV. We aimed to improve comparability with the threshold, which is based on the cost per new diagnosis, by adjusting for previously diagnosed self-testers or self-testers on treatment. However, we did not collect data on previous diagnosis among individuals who tested through standard HTS and may have underestimated known HIV-positive status in the SOC arm.19 We also did not account for confirmatory testing following HIVST and may have overestimated HIV diagnosis in the community-led HIVST arm. Furthermore, we used a willingness-to-pay threshold recommended for decision making within HIV testing programmes, with thresholds as low as $150 per new diagnosis suggested when considering resource allocation across healthcare services.7
Cost-effectiveness of community-based HIV testing is dependent on minimising implementation costs and maximising uptake among populations with high prevalence of undiagnosed HIV.31 32 Using a community-led approach, we aimed to lessen costs through pragmatic and short-term implementation and better outcomes through community participation and implementation in a high-prevalence district. Mobilising community health groups beyond an annual period may improve probability of cost-effectiveness, given the low impact on HIV positivity reported in this study. Districts with more substantial prevalence of undiagnosed HIV should also be targeted, though diminishing returns to HIV testing will continue to influence cost-effectiveness as countries near global HIV targets. Additional health benefits could also potentially be gained by delivering HIVST within a broader package of multidisease interventions at community level.
The main strength of our study is the use of a cluster-randomised trial as an instrument for economic evaluation, with our analysis based on individual-level data for costs and effects. Individual-level costs were estimated using the frequency of HIV testing and self-testing events, providing insights into retesting behaviours and potential opportunities for efficiency gains. In our analysis, we also accounted for the clustered design, correlation between costs and effects, and covariate adjustment. Furthermore, we present findings from a pragmatic intervention implemented through established community health groups. The intervention was aimed at replicating real-world implementation, underpinning the generalisability of our costs to similar settings in sub-Saharan Africa with community health groups. However, our findings on cost-effectiveness were highly sensitive to variations in HIV positivity.
The study, however, has limitations. First, costs of the community-led HIVST intervention were collected from the perspective of a non-governmental organisation rather than the health system. However, we aimed to replicate scenarios for routine implementation by varying start-up and personnel costs and the volume of kits distributed. We also did not account for costs incurred by communities and patients, though this was expected to be very low.25 Second, individual-level costs and effects are based on self-report and subject to recall or social desirability bias, with potential for over-reporting in the community-led HIVST arm following exposure to the intervention. Third, trial-based economic evaluations have limitations, with the time horizon for evaluating costs and effects limited to the trial period. Fourth, our outcome was restricted to HIV positivity. We aimed to adjust our outcome for known HIV-positive individuals to improve comparability with the willingness-to-pay threshold based on the cost per new diagnosis. However, we were unable to account for previous diagnosis under standard HTS or confirmatory testing following HIVST. We also did not evaluate treatment or prevention outcomes or generic health endpoints. Finally, we did not consider non-health benefits associated with community-led programmes.33
Conclusion
Community-led delivery of 7-day HIVST campaigns provided HIV testing at a low additional unit cost. However, adding community-led HIVST to the SOC was not likely to be cost-effective, especially in contexts with low prevalence of undiagnosed HIV. To maximise the value of community-led HIVST, we recommend targeted delivery to settings and populations with more substantial prevalence of undiagnosed HIV.
Data availability statement
Deidentified participant data and data dictionary are available on request to the corresponding author. Data are available with investigator support following publication.
Ethics statements
Patient consent for publication
Ethics approval
Ethical approvals were obtained from the University of Malawi College of Medicine (P.01/18/2332), London School of Hygiene & Tropical Medicine (14761) and WHO (STAR-comm led CRT-Malawi).
Acknowledgments
We would like to thank the study participants; community partners and the Mangochi District Health Office for their involvement in the implementation of the study; the Department of HIV and AIDS at the Ministry of Health for their involvement in the study design; the Malawi-Liverpool-Wellcome Trust Clinical Research Programme and Population Services International Malawi team for their contributions to the study design and implementation; and the technical advisory group for their scientific input and guidance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Lei Si
Contributors PPI and FTP conceptualised the study. PI, KF, ELC and FT-P contributed to the study design. PPI, LAS, SM, MKK and RC supervised implementation of the study, including the intervention and data collection. PI conducted the statistical and cost analysis, with scientific input from KF, HM, ELC and FT-P. PPI, KF, RN, CCJ, KH, ELC and FT-P critically interpreted the results. PPI wrote the first draft of the manuscript. All authors reviewed and approved the final manuscript.
Funding The study is funded by Unitaid, grant number: PO#8477-0-600. ELC is also funded by the Wellcome Trust (WT091769).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.