Article Text

Abstract
Background Community health worker (CHW) programmes are a valuable component of primary care in resource-poor settings. The evidence supporting their effectiveness generally shows improvements in disease-specific outcomes relative to the absence of a CHW programme. In this study, we evaluated expanding an existing HIV and tuberculosis (TB) disease-specific CHW programme into a polyvalent, household-based model that subsequently included non-communicable diseases (NCDs), malnutrition and TB screening, as well as family planning and antenatal care (ANC).
Methods We conducted a stepped-wedge cluster randomised controlled trial in Neno District, Malawi. Six clusters of approximately 20 000 residents were formed from the catchment areas of 11 healthcare facilities. The intervention roll-out was staggered every 3 months over 18 months, with CHWs receiving a 5-day foundational training for their new tasks and assigned 20–40 households for monthly (or more frequent) visits.
Findings The intervention resulted in a decrease of approximately 20% in the rate of patients defaulting from chronic NCD care each month (−0.8 percentage points (pp) (95% credible interval: −2.5 to 0.5)) while maintaining the already low default rates for HIV patients (0.0 pp, 95% CI: −0.6 to 0.5). First trimester ANC attendance increased by approximately 30% (6.5pp (−0.3, 15.8)) and paediatric malnutrition case finding declined by 10% (−0.6 per 1000 (95% CI −2.5 to 0.8)). There were no changes in TB programme outcomes, potentially due to data challenges.
Interpretation CHW programmes can be successfully expanded to more comprehensively address health needs in a population, although programmes should be carefully tailored to CHW and health system capacity.
- HIV
- child health
- health services research
- maternal health
- diabetes
Data availability statement
Data are available on reasonable request. Data collected for this study will be made available to others as aggregate and de-identified data. The study protocol is published in a peer-reviewed journal, and supplemental materials include the CHW procedures and the data forms and data flow used in the project. Data and programmatic documents will both be shared via email request to the first author, and additional analysis proposals must be discussed and approved by the first and last authors to ensure dataset is well understood.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
There is extensive literature documenting and evaluating community health worker (CHW) programmes.
However, most CHW literature in low-income and middle-income countries examines single health issues, most commonly maternal and child health, HIV and malaria.
Overall, there is little high-quality evidence comparing CHW programmes that focus on single programmatic areas with those that cover a broad range of areas, and whether expanding programmes improves coverage for a broader range of health conditions with better clinical and health system outcomes in areas of existing coverage.
What are the new findings?
This study presents a stepped-wedge cluster randomised controlled trial of a polyvalent CHW programme covering HIV, tuberculosis (TB), non-communicable diseases and maternal and child health versus an HIV and TB-specific programme in Malawi.
Improvements were observed in antenatal care attendance and rates of default from chronic care with no evidence of a change in the default rate from HIV care, which was already covered by the previous programme with very strong results.
Evidence of improvement in paediatric malnutrition and TB case finding were not detected.
Key questions
What do the new findings imply?
Community health worker (CHW) programmes can be successfully expanded to improve health coverage by addressing multiple health areas, particularly where their role involves community linkage to care, ensuring or encouraging attendance at clinics and appointments, and identifying defaulting patients.
For more complex tasks, such as identifying cases of malnutrition or collecting sputum samples, improvements may be harder to achieve, which may be explained by the strength of and integration with the primary healthcare system.
Results from CHW programmes are also likely to be highly context specific; this programme prioritised strong leadership structure, financial remuneration and high-quality training and supervision.
Introduction
Community health worker (CHW) programmes have been recognised as integral parts of national and local health systems, linking community members with primary care.1 Hence, several low-income and middle-income countries have implemented CHW programmes in the last two decades with the aim of improving access to care,2–4 especially for vulnerable populations.5 6 In recognition of their cost-effectiveness, there has been a push by institutions to finance the institutionalisation of CHWs in order to improve access to high-quality care.4
CHWs are community members outside of the formal nursing or medical profession who are trained to perform tasks ranging from health education, screening for diseases/case finding, referral and accompaniment to care, and sometimes delivery of basic health services.3 7 In sub-Saharan Africa, CHWs are most often engaged in areas of maternal and child health, malnutrition, family planning and infectious diseases such as HIV and tuberculosis (TB).2 3 A recent review found that—between 2005 and 2014—half of the published research studies on CHW programmes were from Africa, with 35% focusing on maternal child health and 16% on HIV. Studies in non-communicable diseases (NCDs) and mental health were less common, each contributing approximately 4% of the research during this period.3
At present, rigorous evaluations tend to focus primarily on one area of a CHW programme, such as maternal health,8 child health,9 HIV10 11 or TB.3 12 In the context of HIV, CHWs have played important roles in adherence counselling,13 defaulter tracking and linking patients to social support.3 In maternal and child health, introduction of CHWs alone or in combination with facility-based improvements has increased uptake of services,14 first trimester antenatal care (ANC) visits15 and a reduction in under-5 mortality.9 Working with CHWs in NCD programmes remains limited and primarily focused on health promotion and prevention, such as screening for cardiovascular disease and cervical cancer, though there is growing interest in incorporating NCDs into CHW programmes.16–20 In Ghana, for example, despite NCDs not being part of the formal programme, CHWs reported working on NCDs in nine out of 10 regions.21 To date, there are very few examples of evaluations of polyvalent CHW programmes that incorporate multiple conditions in their care provision model.3
CHWs in Malawi
In Malawi, the Community Health Strategy (2017–2022) focuses on increasing primary care delivery through health surveillance assistants (HSAs), a small cadre of government-supported CHWs based at community clinics, each serving approximately 250 households in areas of malaria treatment, immunisations, environmental health, and maternal and newborn health.22 However, an evaluation of the role of HSAs in community-based maternal and neonatal care showed that only 30% of pregnant women received a home visit during pregnancy and only 11% received a postpartum visit within 3 days of delivery.23 Furthermore, there was evidence of inequity, with women of higher socioeconomic status being more likely to receive home visits while pregnant.24
In Neno District, Malawi, since 2007 an additional cadre of CHWs work alongside the HSAs on HIV and TB. They possess a comparatively lower level of skills relative to HSAs but have a higher ratio of CHWs to the population.11 25 Partly as a result of the initial CHW programme, Neno district has had the highest rates of HIV retention and survival in Malawi.25 The new polyvalent ‘Household Model’ (HHM) CHW programme is unique to Neno district. Under the HHM, a CHW is assigned to households rather than patients, and focuses on a set of priority conditions including HIV, TB, paediatric malnutrition, maternal and child health, and NCDs. The programme was launched in 2017 and rolled out in a random order to 11 health facility catchment areas clustered into six groups following the principles of a stepped-wedge cluster randomised controlled trial (cRCT) design.26 The study protocol has been previously published,27 with the results of the study reported in this manuscript.
Methods
Setting
Neno is an impoverished, rural district of approximately 165 000 people in Malawi.28 There are no tarmac roads, and only 3.4% have electricity.29 The district is served by 14 health facilities including 12 primary care centres and two hospitals, all operated by and overseen by the Ministry of Health (MOH). From 2007, Partners In Health, an international non-governmental organisation, was invited by the MOH to support service delivery in Neno.
Study design and participants
The intervention was implemented using a stepped-wedge cRCT design between September 2016 and November 2018. Six clusters were formed incorporating one or more of the 11 health facilities and their catchment areas, which were: (1) geographically contiguous and (2) approximately equal in population. The remaining three health facilities in Neno district were not included; two had previously served as pilot facilities of an earlier model focused on maternal health and the third opened just before study roll-out and thus directly adopted the HHM. The main outcomes of the study (described below) all related to diagnosis and utilisation of health services, so within each cluster, all residents or relevant active patients (depending on the outcome) of the catchment areas formed the cohort. The intervention was implemented in a new cluster every 3 months.
Randomisation and masking
The intervention roll-out occurred in accordance with the stepped-wedge study design, with the order determined by a random number generator. Starting in March 2017, a new cluster received the intervention every 3 months until all clusters had received the intervention. Given the nature of the intervention, it was not possible to mask the participants, implementers or research team to a cluster’s intervention status.
Procedures
Implementation of the HHM included expanding coverage to all households in the district, incorporating new disease areas, redesigning training curricula, retraining of existing CHWs, recruitment and training of additional CHWs, enhancing CHW supervision with an introduction of two supervisory cadres and updating data collection tools and monitoring methods. The key differences between the HHM and the previous CHW model are identified in table 1, based on categories defined by the CHW Assessment and Improvement Matrix.27 30 31
Key elements of the household model
Description of roles and responsibilities of community health worker (CHW) staff under the household model
Site supervisors (n=11)
Based at health facilities and primary link with clinical staff and health surveillance assistants (HSAs). Responsible for supervising senior CHWs and for data collection and review for their respective catchment areas. Also responsible for eliciting missed visits and other concerns from HSAs and communicating information to CHWs.
Senior CHWs (n=142).
Based in the community. Responsible for household visits and for supervising approximately five CHWs each. They also aggregate data from CHW paper-based registers and report to their site supervisor.
CHWs (n=935).
Based in the community. Responsible for monthly household visits (20–40 households) and for recording data in paper-based registers.
Houses were geographically grouped, and each CHW was assigned to visit 20–40 households each month. Home visits included education and screening for multiple conditions including sexually transmitted infections, TB (via sputum collection), HIV and paediatric malnutrition (via mid-upper arm circumference, MUAC), enrolment of pregnant women into ANC, and referral or accompaniment of symptomatic household members to clinic, as needed. This involved identifying community members not already diagnosed or enrolled in care and linking them to the clinic. Accompaniment here means walking with a client to the facility to help navigate the medical screening and care processes.15 Patients enrolled in integrated chronic care clinics for HIV and NCDs were visited more frequently, with CHWs conducting treatment and adherence counselling, identification of medication side effects, psychosocial support, screening for other conditions (eg, TB), and missed visits tracking (see online supplemental material 1 on CHW Accompaniments, Referrals and Home Visits).
Supplemental material
HSAs, the government cadre of CHWs, remained largely facility based, with a ratio of one to approximately 500 households in intervention areas, well above the recommended ratio of 1 HSA to 1000 people. Site Supervisors, also based at facilities, partnered directly with HSAs on programmatic priorities, troubleshooting and data review (box 1). The priority conditions for CHWs were consistent with those emphasised in the Health Sector Strategic Plan and gaps identified in Neno district.27
Each quarter, an initial household mapping exercise was carried out in the new intervention area to determine the number of additional CHWs needed. To maintain the ratio of 20–40 households per CHW, an additional 252 CHWs were recruited for a total of 935 CHWs in the trial. The new CHWs were recruited in collaboration with the MOH and community leadership using selection criteria which required candidates to be able to read, write and live in the village they were serving.32
A new cadre of senior CHWs was introduced in order to provide supervision, mentorship and support to CHWs at the village level. The senior CHWs, selected out of existing high-performing CHWs, liaised directly with an existing site supervisor who was positioned at each of the 11 health facilities and was responsible for communication and collaboration with clinical staff (Box 1).
All CHWs underwent a 5-day foundational training that introduced the programme and skills needed to conduct their activities. CHWs were assessed at the end of this training to ensure they were deployment ready and to identify CHWs who may need additional mentorship. Senior CHWs underwent the foundational training as well as an additional 2-day training on mentorship and supervision procedures, which included quarterly spot-checks of all CHWs to assess performance and identify areas for support.
The HHM programme held routine structured meetings to review data and discuss areas for improvement. These meetings happened at each level of data aggregation. First, monthly meetings were held at the village level between the senior CHWs and their CHWs for data aggregation (from household level to village level). Second, senior CHWs met with facility-based CHW site supervisors for additional data review and aggregation (from village level to health facility catchment area level). Third, monthly meetings were held to share and review data directly with HSAs and other clinical staff. Site supervisors and HSAs used a structured checklist to identify any nutrition or TB clients that missed a visit or might need additional support, which was communicated to the CHW following those households. This allowed a much higher number of home visits to these clients than the HSA programme alone was capacitated for. Finally, management meetings to review staffing, data and performance were held at the district level. The process monitoring data captured by CHWs in paper registers and aggregated monthly were used for internal monitoring and quality improvement (see online supplemental material 2 on HHM form overview). Data used for the stepped-wedge cRCT evaluation are described below.
Supplemental material
Data sources
Data used for evaluating this intervention were sourced from three data systems:
District Health Information Software II (DHIS2) system maintained by the Malawi MoH, where data from paper registers are collated and aggregated from every health facility on a monthly basis. Monthly data were downloaded from the DHIS2 platform and missing or possibly erroneous data points were checked by MoH against facility paper records.
Electronic medical record (EMR) system in OpenMRS platform maintained by Partners In Health (PIH), where identifiers are assigned to individual patients with HIV and/or NCD. Treatment records are updated at every clinical visit. Patient-level data were extracted from the EMR and aggregated by cluster and facility.
Local instance of DHIS2 maintained by PIH specifically for monitoring the HHM process monitoring indicators. Aggregated data by catchment area were entered monthly into the local instance of DHIS2.
Outcomes
Six primary outcomes and 14 secondary outcomes were defined to capture each of the areas of care the HHM programme was targeting; these are reported along with the source of the data in box 2.
Definitions of outcomes and data sources
Primary outcomes (monthly)
HIV default.
Percentage of clients taking antiretrovirals who default from care. Default is defined as 8 weeks past a missed scheduled visit.
Electronic medical record (EMR)
Non-communicable disease (NCD) default.
Percentage of clients enrolled in the NCD clinic who default from care. Default definition same as above.
EMR
Paediatric malnutrition case finding.
Children aged 6–59 months newly enrolled in care for moderate or severe paediatric malnutrition (per 1000).
District Health Information Software II (DHIS2)
Tuberculosis (TB) case finding.
New laboratory confirmed TB cases via a positive sputum sample (per 100 000).
DHIS2
Family planning uptake.
Percentage of women of childbearing age newly starting family planning.
DHIS2
First trimester antenatal care (ANC) enrolment.
Percentage of women enrolled in ANC in the first trimester.
DHIS2
Secondary outcomes
HIV in care and surviving.
Percentage of clients taking antiretrovirals who were retained in care and surviving.
EMR
NCD in care and surviving.
Percentage of NCD clients who were retained in care and surviving.
EMR
NCD hypertension default.
Percentage of clients enrolled in the NCD clinic with hypertension who default from care.
EMR
NCD diabetes default.
Percentage of clients enrolled in the NCD clinic with diabetes who default from care.
EMR
NCD asthma default.
Percentage of clients enrolled in the NCD clinic with asthma who default from care.
EMR
NCD epilepsy default.
Percentage of clients enrolled in the NCD clinic with epilepsy who default from care.
EMR
NCD mental health default.
Percentage of clients enrolled in the NCD clinic with mental health conditions who default from care.
EMR
Moderate paediatric malnutrition case finding.
Number of children aged 6–59 months newly enrolled in treatment for moderate malnutrition (per 1000).
DHIS2
Severe paediatric malnutrition case finding.
Number of children aged 6–59 months newly enrolled in treatment for severe malnutrition (per 1000).
DHIS2
Paediatric malnutrition inpatient admission.
Number of children aged 6–59 months admitted in the nutritional rehabilitation unit (per 1000).
DHIS2
Paediatric malnutrition cure.
Percentage of children aged 6–59 months discharged as cured in treatment programmes for moderate or severe malnutrition.
DHIS2
TB cure.
Percentage of TB cases successfully completing treatment.
DHIS2
Family planning uptake (long term).
Women of childbearing age receiving long-term family planning methods (per 1000).
DHIS2
ANC 4+ visits.
Percentage of women enrolled in ANC with four or more visits.
DHIS2.
Statistical analysis
The unit of observation was cluster-month, and all analyses were based on aggregates at this level as generally more granular data were not available. All six clusters were observed for 27 months each: In the first 6 months, no cluster received the intervention, in the following 15 months a new cluster received the intervention every 3 months until all clusters had received the intervention, and then in the final 6 months all clusters had the intervention, for a total of 27 months (figure 1). The amount of time each cluster spent in preintervention and postintervention states therefore varied from 6 to 18 months. One exception was made for malnutrition outcomes where, instead of 6 months of preintervention data, we used 12 months of preintervention data in order to better capture seasonal effects. We took a Bayesian approach to trial design and analysis since it: (1) permits the incorporation of prior information into the analyses; (2) has a ‘natural’ probabilistic interpretation in terms of effect sizes; (3) can be simply incorporated into decision models and subsequent economic evaluation and (4) has no reliance on statistical significance, which would be complicated by the multiple testing and small number of clusters.33

Timeline by cluster.
We conducted a Bayesian assurance analysis, which is analogous to a frequentist power calculation.34 We determined the probability of there being at least a 95% posterior probability of the treatment having an effect different from (greater or less than) zero based on an aggregated prior distribution for treatment effects from an expert elicitation exercise conducted in Blantyre, Malawi in 2016. The analysis is reported in the trial protocol.27 For all outcomes there was a >95% probability that there would be at least 95% probability of the treatment effect being greater than zero, except for retention in care for HIV patients where the relevant probability was 75% due to only a small effect expected.
We present summary statistics as preintervention and postintervention means and SD along with the difference and its SE. The data are also plotted against time relative to intervention roll-out and a loess smoothed average added to visually compare preintervention and postintervention trends. Plots were produced for each primary outcome against both calendar time and time relative to the intervention. A model-based analysis was conducted following the standard linear mixed model approach for stepped-wedge cRCTs.35 The model included a cluster random effect, unstructured monthly fixed effects and a dichotomous treatment indicator. No covariates were included in the model. We conducted analyses with both an informative prior, from an expert elicitation, and a weakly informative prior N(0,52) for the treatment effect coefficient. All other parameters had weakly informative prior distributions: N(0,52) for covariates and half t-distribution with four df for hierarchical SD terms.36
For each primary outcome we estimated models with linear, logit, probit and beta distribution link functions and selected the best fitting one based on graphical posterior predictive model checks and leave-out-out cross validation.37 Coefficient estimates and average marginal effects (ie, absolute risk differences) were estimated. We also report the intraclass correlation coefficient estimated from each model. Secondary outcome models were specified according to the selected related primary outcome for comparison. All models were estimated in Stan V.2.19 in R V.3.4.4.
Results
The intervention was delivered according to the trial plan and a total of 162 cluster months of data were available for analysis. Table 2 shows process monitoring data and activities of the CHWs in the programme. Table 3 reports the outcome averages for the preintervention and postintervention periods and figure 2 shows trends in the outcomes over time. By the completion of roll-out, approximately 29 000 households were receiving monthly CHW visits (98% of all households) and an average of 1800 patients were being referred or accompanied to care each month. Households per CHW ranged from 31 to 41 with an average of 38 households per CHW as of the last month of observation.
Household (HH) ratios, HH visits and supervision
Summary statistics for monthly outcomes in preintervention and postintervention periods
{kind=link}
{kind=link}
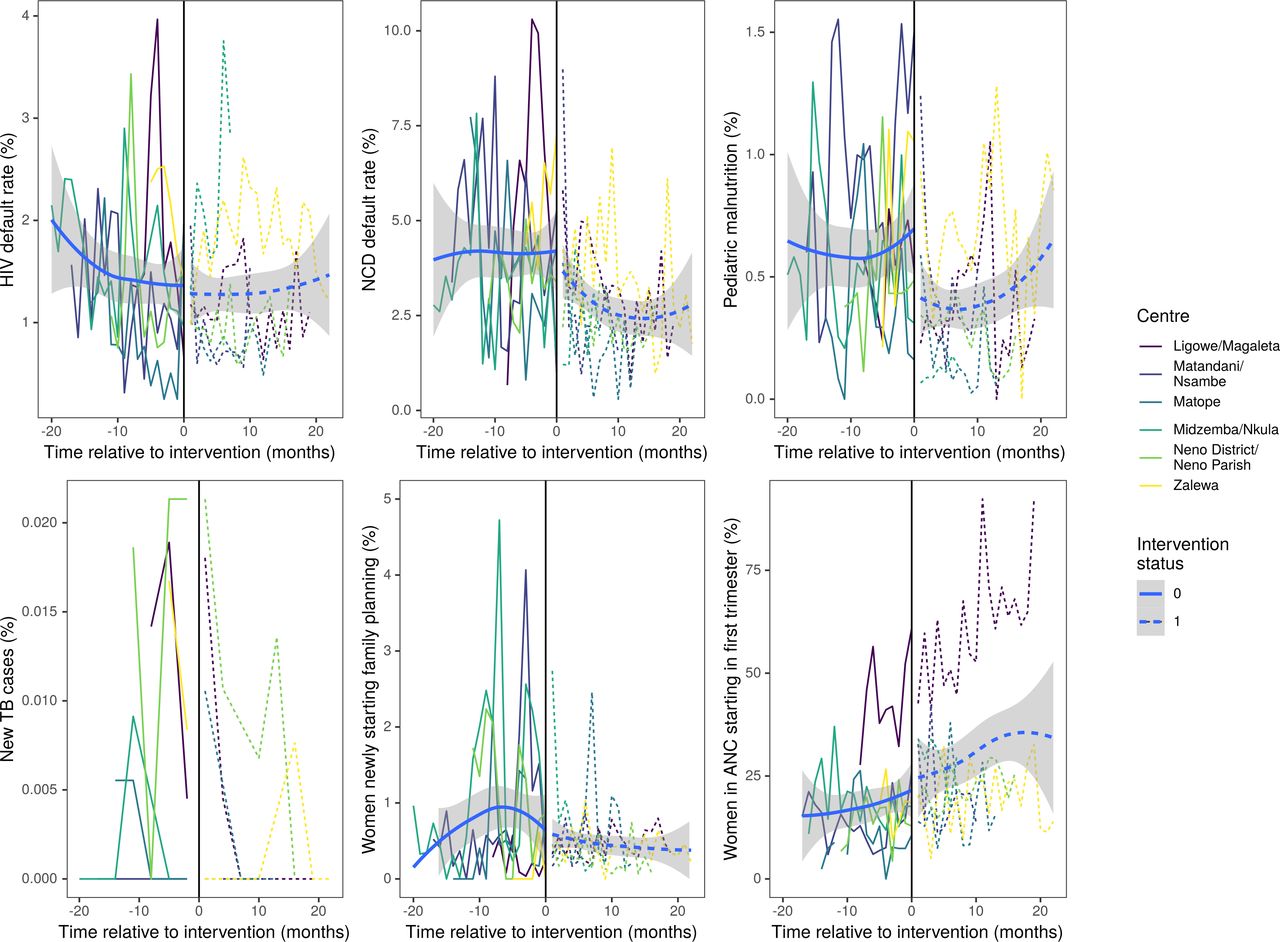
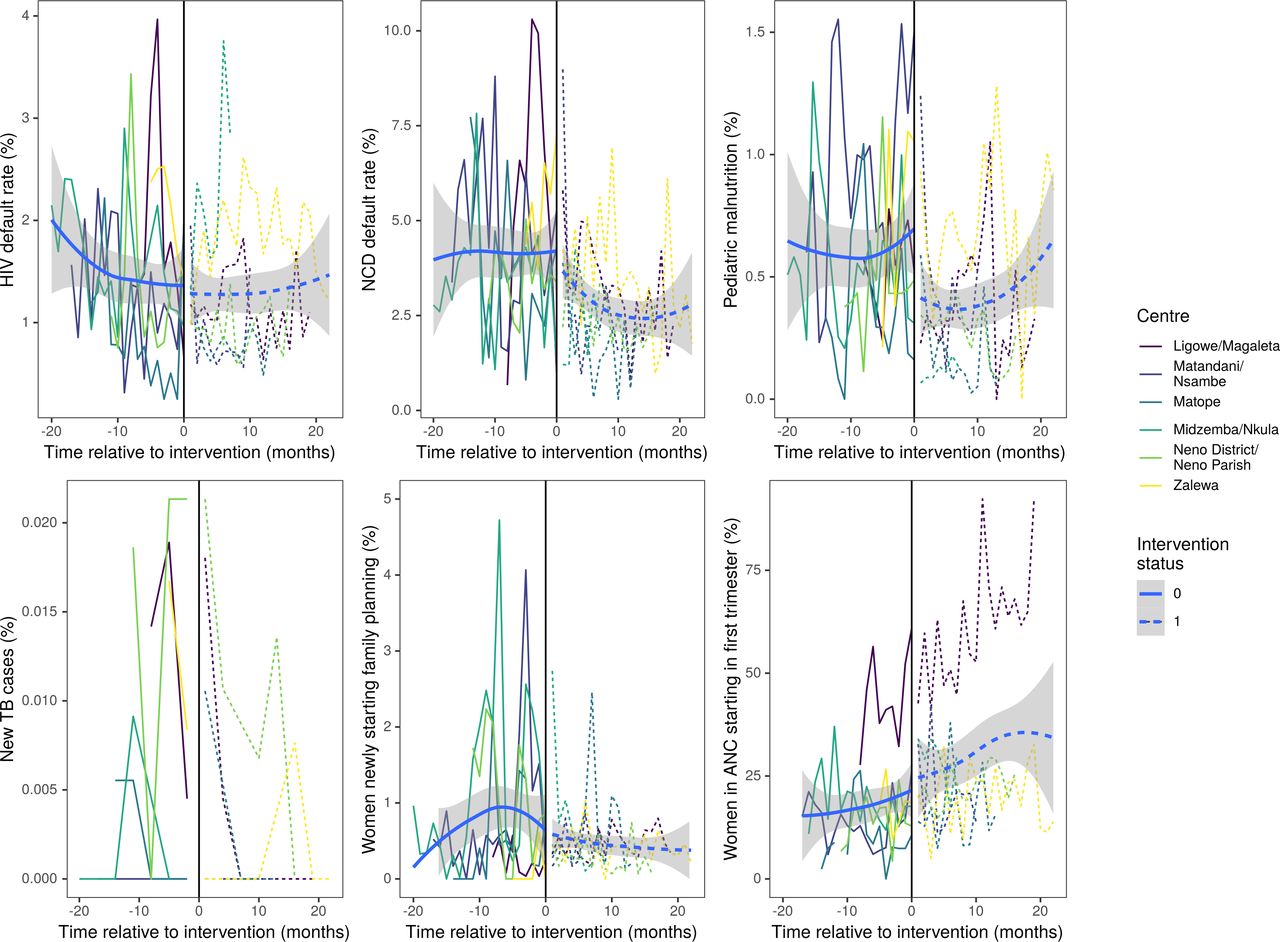
Primary outcomes by month for each cluster relative to intervention implementation with smoothed preintervention (solid) and postintervention (dashed) trend lines. ANC, antenatal care; TB, tuberculosis.
The NCD monthly default rate declined from 4.2% in the preintervention period to 2.8% in the postintervention period. Secondary outcomes also exhibited favourable trends. For example, the proportion of patients in NCD care and surviving increased from an average of 95.7% to 97.1% and default rates fell across all NCD conditions with the greatest reductions observed for mental health (from 4.6% to 2.3%) and diabetic (from 4.3% to 2.3%) patients. Little change was observed in the low monthly rate of default from HIV care of 1.3%. The percentage of women enrolled in ANC in the first trimester and those receiving at least four ANC visits over the duration of their pregnancy increased by 11.6 and 8.2 percentage points, respectively. The detection rate of new cases of paediatric malnutrition declined by 2.1 cases per 1000 children per month.
Table 4 reports the results from the model-based analyses for the primary outcomes with both informative and weakly informative prior distributions. Treatment effects were qualitatively similar to the crude differences reported in table 3, although were generally smaller in magnitude. For example, the intervention was estimated to reduce the monthly NCD default rate by −0.82 percentage points (95% credible interval (CrI): −2.54 to 0.51), equivalent to a OR of 0.78 (CrI 0.66 to 0.92). This compares to a crude risk difference of −1.4 percentage points. The treatment effect was smaller in magnitude under weakly informative prior distributions. Reductions in paediatric malnutrition and family planning, and an increase in ANC use were similar to the crude differences.
Estimated model coefficients and absolute risk differences for primary outcomes
Reliable monthly data for TB outcomes could not be obtained so a model-based analysis was not conducted. Post-intervention around 3% of sputum samples submitted by CHWs were positive for TB and CHWs were the source of 69% of all cases of chronic cough that were tested in a facility. The TB case finding rate declined from an average of 5.7 new cases per 100 000 per month to 3.3 (table 2), and the percentage of patients successfully completing treatment increased from 39.5% to 48.0%.
Table 5 reports the estimated treatment effects for the secondary outcomes. The treatment effects were smaller in magnitude than the crude differences and accompanied by relatively wide CrIs that all included zero. The sign (reduction or increase) of effects was consistent across outcomes within the same clinical category, that is, the posterior mean effect was a reduction in all NCD default rates (of between approximately 5% and 35% of baseline rates), a reduction for all paediatric malnutrition outcomes (of 10%–50% of baseline values), and an increase in all ANC outcomes (of approximately 15%–30% of baseline rates).
Estimated treatment effects of the intervention on secondary outcomes
Discussion
In this study, we present results from a polyvalent CHW model which expanded an existing programme to meet a more diverse set of health needs in a very poor rural setting served by several public health facilities. Assigning CHWs to every household, called the HHM, is increasingly common.30 Our results provide evidence that such a model can expand health coverage by reducing default rates from chronic care and improving uptake of ANC. Importantly, existing HIV programme success was not harmed by the expansion of the CHW role; we did not anticipate or observe changes in HIV retention in care, given long-term survival and retention rates above 90% in Neno district prior to the study.11
A principal aim of the intervention was to improve retention of patients enrolled in NCD care, approximately 5% of whom technically defaulted each month, meaning they had not been seen for eight or more weeks after a missed routine appointment. The NCD clinic cohort at the conclusion of the study was around 12 000 patients, a growth of more than 8000 patients over the course of the intervention, and the intervention reduced the monthly default rate by approximately 0.8 percentage points. This translates into approximately 1200 additional patients being retained in care each year because of the intervention, assuming that none of the defaulters would have otherwise returned to care. This demonstrates how employing polyvalent CHWs to track patients in their homes longitudinally is an effective contributor to retaining patients in care, a critical finding given the significant burden of NCDs in Malawi. Similarly, previous work, including our early work in Neno district, suggests that CHWs can play a key role in increasing ANC visits during the first trimester of pregnancy and maintaining ANC attendance over the course of the pregnancy, a key part of Malawi’s strategic plan.38 39 Our results suggest this effect can be achieved as part of a polyvalent multicondition programme, not only as a result of a vertical programme focused on maternal health.
These results further suggest that improved health outcomes are realised even more when CHW interventions are coupled with a well-designed and well-managed patient-centred clinical programme at the facility level. Neno district has one of the best chronic care programmes in Malawi, as evidenced by excellent HIV and NCD patient outcomes in the Integrated Chronic Care Clinic, a well-coordinated and documented treatment and care programme for clients living with chronic conditions.40 41 Neno did not, however, have outlying malnutrition or TB programmes at the time of the study. Correspondingly, the effect of the HHM on the TB and malnutrition outcomes was not observed. This suggests some level of risk in implementing polyvalent CHW programmes, in that their effects may not be detectable at a facility that does not have correspondingly strong clinical programming or reliable data systems.
This point is underscored by the malnutrition and TB findings. It was hypothesised during intervention design that screening children in the home would identify cases of malnutrition that were missed by community screening, possibly diagnosing children earlier in the course of disease. However, our results do not support the hypothesis that we would see an increase in cases. Process monitoring data collected during the HHM implementation showed that CHWs were reliably visiting households, and monthly meetings, CHW register review and supervisory spot checks did not reveal gaps in performing screening children under 5 for malnutrition each month. It is therefore unlikely that a lack in performing MUAC explains the nutrition results. Several reasons could help explain this. First, the prevalence of undernutrition had been declining in Malawi, following a severe hunger crisis in preceding years, up to and including 2018, so it is logical that case identification in Neno would also decrease.42 43 Second, a supply side problem is possible, as facilities tend not to enrol children when food supplements are stocked out, thus undercounting true diagnoses in the population, and we did not track stock outs as part of this research. Third, there could have been some over-reporting of under 5 malnutrition cases prior to the intervention. This pattern had been observed during times of inconsistent supply; facilities would report extra cases in order to avoid future stockouts. Lastly, though this alone would not explain a decline in malnutrition detection, there could be quality issues with interpretation of MUAC measurement by CHWs as this is more of a technical exercise than they had previously been requested to do.
No evidence was found that the intervention increased the identification of TB cases in Neno district. TB data were limited to quarterly reports rather than monthly, with some quarters having missing data, so we were limited in our power to show a difference. However, results do suggest that having CHWs consistently screen household members for TB and collect sputum is feasible. This is similar to experience in Ethiopia, where 2.4% of those submitting sputum were smear positive.44 CHWs were submitting the majority of the samples examined in Neno district, and 1 in 34 was positive, similar to the findings in Ethiopia.44
This rigorous evaluation of a polyvalent CHW programme in rural Malawi contributes several valuable lessons in the design and implementation of CHW programmes. First, our results suggest that a robust connection to quality primary care is crucial. CHWs perform complementary tasks, as opposed to operating in parallel or as a replacement for primary care. The most significant impacts from the HHM programme correspond to strong primary care programmes in Neno for chronic disease and maternal health.11 41 We found that interventions requiring both CHWs and complex health facility interventions are the most challenging and complex to implement, but present the highest potential as solutions are found. With respect to TB services, the intervention also worked to ensure health facilities had the capacity to examine the increased number of sputum samples referred from CHW TB screening. As a result, the number of patients tested for TB during this period increased. Similar attention needs to be paid to the supply side for paediatric malnutrition and family planning. This discussion around primary care is particularly important considering that many disease-based CHW programmes are subject to vertical funding mechanisms. Our work highlights the need to focus on long-term investment in integrated CHW programmes, thus addressing the continuum of the primary care system best positioned to produce impact at population level.
Second, other components of primary care can have a large impact on findings. Our team acknowledges the role of leadership—facilities with strong leadership, consistent data review meetings and good communication among staff tended to more smoothly take up the intervention and interact with it in positive ways. Additionally, integration of data systems is a complex but necessary challenge. Data systems for CHWs are extremely complex to implement and must be connected to facility data systems. We confronted many hurdles in our attempt to use public data systems, but despite the challenges, we would still recommend this approach in order to strengthen public systems rather than create parallel ones. Indeed, routine evaluation of programmes like this should be incorporated into roll-outs where possible. However, the available data and data quality does limit the ability to isolate impact from components of complex systems requiring CHW action such as referral, laboratory action (such as diagnostic confirmation), and clinical action (such as enrolment).
Finally, our experience with the HHM suggests that the matching of programme aims with CHW skills and competencies is important and warrants more research. For example, factors such as the educational background and training of CHWs may be key, as well as compensation, workload and CHW to household ratios. For example, we did not find evidence of any difference in the uptake of family planning, which could be due to the complexity of the intervention and counselling required or the fact that CHWs may be related/acquainted with their clients, along with external factors such as broader societal issues or religious affiliation of some clinics, or challenges on the facility supply side. Evidence supporting this was found in a different research study, revealing that very few households are asked about family planning by their CHWs (unpublished data). Qualitative follow-up suggested that CHWs reported difficulty discussing sensitive topics such as sexually transmitted infections with their friends and neighbours (unpublished data). Further investigation is ongoing to explain this effect; nevertheless, CHW intervention alone for this complex issue may not suffice without additional complementary culturally appropriate methods.
There are several limitations to this analysis. As indicated the quality of the routinely collected data used for this evaluation (namely DHIS2) is limited in some instances. These data, manually aggregated by overworked clinical staff, are entered in large volumes into the electronic platform by the district data team, which makes them prone to errors.45 Data points were cross-checked against paper records and triangulated with any other comparable data sources or reporting systems. Nevertheless, data for TB and malnutrition were considered of poor quality. Because our data sources were from CHWs and clinical care, we were also not able to track population surveillance data during the study in order to detect changes in population prevalence of specific conditions, such as malnutrition. Second, intervention fidelity was preserved to the extent possible over time, but changes such as health facility staff and leadership turnover, improvements in staff knowledge and changes within the health system external to the CHW programme inevitably occurred. These changes could have impacted our primary (and downstream) indicators that we could not measure explicitly. Indeed, differences in crude and model-based effect estimates suggest a confounding secular trend in the same direction as the intervention effects. Next steps to address some of these limitations include robust initiatives around data quality, particularly for the public sector and ongoing improvement of the new supervision cadre. Ongoing research includes time motion studies to investigate how CHWs allocate their time as well as qualitative research to help explain some of these quantitative findings.
The findings of the study are in agreement with the National Community Health Strategy (2017–2022), which highlights that the provision of quality, integrated community health services that are affordable, culturally acceptable, scientifically appropriate and accessible to every household requires a revised community health system that is designed to be community led. The learnings of connecting the CHWs to the primary care system may be of particular import in this regard, and this work could provide a platform for future standardisation of elements such as training, data systems, linkages to primary care and incentives. The polyvalent, HHM programme provides a model of how the communities can be systematically organised to participate in health, contributing to the strategy’s vision and mission. For example, part of the strategy is to drive down maternal mortality ratio from 439 to 350 per 100 000 live births by promoting ANC facility visits which the HHM programme was able to achieve.
Polyvalent CHW programmes may be able to replicate the success of single focus programmes evidenced in multiple countries while reducing the overall programme cost as workflows are combined. Ultimately, a polyvalent approach such as the household-based model can expand coverage and address a wide range of health needs in a population while maintaining existing gains within disease programmes. In this study, evidence suggests that CHWs can simultaneously improve attendance and reduce default rates across a range of conditions including chronic NCDs, maternal care and HIV care. However, we did not find evidence that CHWs were able to improve nutrition or TB case finding, requiring more complex tasks, although outcomes did not worsen. This may suggest more intensive training is required, that staff with greater experience and qualification are required for these tasks, and/or that the primary care systems need additional strengthening in tandem with community interventions. Further research of polyvalent programmes is required to support their optimal configuration.
Data availability statement
Data are available on reasonable request. Data collected for this study will be made available to others as aggregate and de-identified data. The study protocol is published in a peer-reviewed journal, and supplemental materials include the CHW procedures and the data forms and data flow used in the project. Data and programmatic documents will both be shared via email request to the first author, and additional analysis proposals must be discussed and approved by the first and last authors to ensure dataset is well understood.
Ethics statements
Patient consent for publication
Ethics approval
The trial received ethical approvals from the Malawian National Health Science Research Committee (#16/11/1694) in Lilongwe, Malawi; Partners Healthcare Human Research Committee (#2017P000548/PHS) in Boston, Massachusetts, USA; and the Biomedical and Scientific Research Ethics Sub-Committee (REGO-2017-2060) at the University of Warwick, Coventry, UK.
Acknowledgments
We would like to thank the Ministry of Health in Neno District, Malawi for their support of this programme and the patients in Neno District who work with us to improve health systems in Neno District. Implementation of the CHW Household Model in Neno involved the hard work of many people, and the authors are endlessly grateful to the work and dedication of Dr Ravi Gupta, Liberty Neba, Clement Trapence, Dr Alexandra Priebe, Sitalire Kapira, Bright Mailosi, Robert Kawonga, Victor Kanyema, Edwin Kambanga, Hilda Mbalati, Russel Msiska, George Mhone, Precalia Chipondeponde, Tafwirapo Chihana, Charles Malindi, Jeanel Drake, Lila Kerr, Katherine Ruffing, Paul Gondwe, Fainala Phiri, Grant Gonani, Patrick Phiri, Brazilia Mose, Sangster Gome, Ganizani Mkwate, Nelson Mwale. The team is also grateful to the extensive work from CHW Site Supervisors Anga Sawasawa, James Lipenga, John Kaiya, Christopher Kachingwe, Amos Ganisha, Elizabeth Chikapa, Alfred Thoza, Robert Jackson, Luckson Chaluchalu, Dyson Seven, Luke Cham’mudzi, Ignatius Katema, Chancy M’manjamwada,Pilirani Maluwa, who were in continuous movement launching and maintain the household model. And lastly but not least, the authors are also indebted to a numerous number of HSAs, facility in-charges, program coordinators, various health care workers and community structures that played different roles during implementation of the program. Special thanks to Wagner Foundation who helped make the publication of this paper possible. RL is supported by the NIHR ARC West Midlands.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Stephanie M Topp
Twitter @emwroe, @siwatson
Contributors EBW, ELD, BN, CK, RM, AVK, HM, BC and LN conceptualised the household model, tailored it to the setting, designed the training and data collection system, and led its implementation and data collection. SIW, RL, CB, ELD, EBW, RM, AM and LD developed the methodology to evaluate the model, with SIW developing the quantitative analysis plan. Throughout the study, EBW, BN, ELD, AVK, CK, MA, HM, BC, BP, LN and EPLN provided ongoing oversight, data review and quality control. EBW, SIW and AVK drafted the first version of the manuscript. BN, ELD, AVK, CK, MA, LD, HM, BC, BP, AM, RM, CB, LN, EPLN, DP and RL provided substantive comments and revisions to the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement statement The Ministry of Health in Neno District and its advisory committee, which includes community members, were involved in the design of the Community Health Worker program in Neno. For this trial, when the program was redesigned to incorporate more conditions, the committee was consulted and updated every 6 months during the program, which is routine for all health programming in Neno District by Partners In Health. In addition, community members and community health workers are consulted and involved in the design of the CHW intervention and the monitoring of its progress.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.