Article Text

Abstract
Background In 2019, there are more than 290 million people who have ever migrated from rural to urban areas in China. These rural-to-urban internal migrants account for more than one-fifth of China’s population and is the largest internal migrant group globally. We present the first systematic review that examines whether internal migrants are more likely to exhibit non-communicable diseases (NCDs) risk factors and have worse NCD management outcomes than non-migrant counterparts in China.
Methods A systematic review was conducted via medical, public health, and economic databases including Scopus, MEDLINE, JSTOR, WHO Library Database and World Bank e-Library from 2000 to 2020. Study quality was assessed using the National Institute of Health Quality Assessment tool. We conducted a narrative review and synthesised differences for all studies included, stratified by different types of outcomes. We also conducted random-effects meta-analysis where we had a minimum of two studies with 95% CIs reported. The study protocol has been registered with PROSPERO: CRD42019139407.
Results For most NCD risk factors and care cascade management, comparisons between internal migrants and other populations were either statistically insignificant or inconclusive. While most studies found migrants have a higher prevalence of tobacco use than urban residents, these differences were not statistically significant in the meta-analysis. Although three out four studies suggested that migrants may have worse access to NCD treatment and both studies suggested migrants have lower blood pressure control rates than non-migrants, these findings were not statistically significant.
Conclusion Findings from this systematic review demonstrate that there is currently insufficient evidence on migrant and non-migrant differences in NCD risk factors and management in China. Further research is expected to investigate access to healthcare among internal and its effect on both their NCD outcomes and long-term healthcare costs in China.
- systematic review
- epidemiology
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Over the last few decades, China has undergone a rapid epidemiological transition, with the shifting the burden of disease shifting from infectious disease to non-communicable diseases (NCDs).
There is an ongoing debate on whether migrants are more likely to exhibit NCD risk factors and have worse NCD care cascade management than their rural and urban counterparts.
What are the new findings?
There is insufficient evidence on the differences in NCD risk factors and the management of NCDs between migrant and non-migrant populations in China.
From very limited evidence, migrants may have worse NCD diagnoses, treatment and control than their counterparts. This might be due to inadequate access to healthcare and delay in seeking treatment.
What do the new findings imply?
Policies should consider removing barriers for migrants to access healthcare in their new city of residence, reforming social health insurance reform to consolidate rural and urban insurance schemes, and allowing greater portability for all people, including migrants.
Further research is required to understand the health-seeking behaviours of migrants, including implications of such behaviours and management of NCDs for health outcomes and long-term healthcare costs among internal migrants in China.
Introduction
Non-communicable diseases (NCDs) are the leading causes of death globally and contribute considerably to existing health inequalities in low-income and middle-income countries (LMICs).1 In China, both the ageing population and increasing exposure to major NCD risk factors have led to a substantial increase in the prevalence of NCDs.2 This rising prevalence, coupled with poor quality of care outcomes for chronic diseases, pose a major challenge to attaining both the Sustainable Development Goal target 3.4 of reducing mortality from NCDs by 25% before 2025 and the Healthy China 2030 goal of reducing premature mortality from NCDs by one-third by 2030.3 4
In the past three decades, China experienced the largest internal migration—an increase in urban population from 17.9% in 1978 to 51.3% in 2011.5 In 2019, the total number of rural-to-urban internal migrants in China had reached 290.8 million, which accounts for more than one-fifth of China’s population.6 Rural-to-urban migrants tend to be younger, live in suboptimal conditions and work long hours with unstable employment.7 The experience of migration exposes individuals to substantial life transitions, including alterations in the physical environment, lifestyle, occupational and socioeconomic status.8 9
Rural and urban living differences influence residents’ health status in China through environmental, social and cultural factors. Several hypotheses have been proposed to explain potential differences in health profiles and health-seeking behaviour between migrants and non-migrants. While urban residents generally have better health status and greater access to healthcare services than rural residents (ie, the ‘urban health advantage’ hypothesis,10 11 large-scale urbanisation has led to the possibility of an ‘urban penalty’ where poorer groups, including migrants, are exposed to higher health risks, unhealthy living conditions, and poorer access to healthcare in urban areas.12 13 In contrast, the ‘healthy migrant hypothesis’ suggests that despite facing some disadvantages, migrants are ‘selected’ working-age individuals who tend to be healthier than the general population in the host destination during the initial years.14–16 In addition, the ‘Salmon bias hypothesis’ presumes that migrants who are unhealthy tend to return to their place of origin while healthier migrants remain in the host destination.14 16 Previous studies which examined these hypotheses primarily focused on general health status, with little comparable data in the context of NCDs. Additionally, it is unclear how these hypotheses may inter-relate across the life course in LMICs where the majority of the global internal migrants reside17 18
Over the past few decades, China has made substantial progress in achieving universal health coverage.19 However, some evidence suggests that internal migrants may be excluded from urban services, including access to public health and other city welfare and social security systems.20 21 This is due to the stringent ‘Hukou’ system, a household registration system that divides residents into ‘urban’ or ‘rural’ groupings based on administrative regions.22 23 Under this system, migrants may lack access to common privileges such as public health services, medical insurance, education, housing and employment, irrespective of how long they have lived or worked in the city.23 24 Migrants do not qualify for the urban employee basic medical insurance (UEBMI) scheme or the urban resident basic medical insurance scheme and have to pay out-of-pocket for medical services in cities, which can only be reimbursed when they return to their place of origin.25 26 Inadequate health insurance coverage may restrict access to local health services and contribute to worse NCD outcomes.27
Despite the large internal migrant population in China, there is an ongoing debate on the rural-urban-migrant difference in NCD profiles (including risk factors) and management.28 29 The aim of this study was to conduct a systematic review to assess whether internal migrants are more likely to exhibit NCDs risk factors and have worse NCD management outcomes compared with non-migrant counterparts.
Methods
We followed the methods described in the peer-reviewed systematic review protocol that is registered with PROSPERO (Registration CRD42019139407).
Search strategy
We conducted a systematic review in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. We performed a comprehensive search of five electronic medical and economics databases, that is, Scopus, MEDLINE, JSTOR, WHO Library Database and World Bank e-Library. The database searches were restricted to peer-reviewed studies written in English only and published from January 2000 to March 2020. Searches were tailored to the functionality of each database but were generally an intersection of three sets of keywords—(1) Migrant; (2) NCD risk factors and disease management; (3) China, using the following terms: (migrant OR migration) AND ((risk factor) OR tobacco OR alcohol OR diet OR activity OR overweight OR obesity OR (blood pressure) OR hypertension* OR (blood sugar) OR diabetes OR (blood lipids) OR (disease management) OR diagnosis OR treatment OR control)) AND (China). Additional records were identified through manually searched references of the included papers. Detailed search terms and search records are listed in online supplemental appendices 1 and 2, respectively. Two reviewers (CXQ and KA) independently screened articles by title and subsequently by abstract to select articles for further review. All disagreements were resolved by consensus or by reference to the third reviewer (JL).
Supplemental material
Inclusion and exclusion criteria
Studies were screened according to the inclusion and exclusion criteria listed in table 1. All studies focusing on adults living in mainland China were included. We excluded studies that only focused on overseas migration or studies solely focusing on children or adolescents. We adopted a broader approach in terms of defining ‘internal migrant’, which can be defined via one of the following approaches: (1) by residence status; (2) by Hukou registration status and (3) by health insurance type. We included studies that examined differences in NCD risk factors or outcomes between migrant and non-migrant populations, including rural residents, urban residents and the general population. We excluded studies that investigated NCD risk factors and outcomes only for the migrant population and did not compare the outcomes of migrants to any other population group. We did include quantitative studies that were based on all types of study design but did not include qualitative studies, systematic reviews and commentaries.
Inclusion and exclusion criteria for study selection based on PICOS
Quality assessment
We used the National Institute of Health Quality Assessment (NIH QA) Tool for Observational Cohort and Cross-Sectional Studies to assess the methodological quality of the included studies.30 Twenty included studies were independently rated by two reviewers using the NIH QA tool, and in the case of differing opinions, discussions were conducted to reach a consensus. Risk of bias was assessed with a modified version of the Effective Public Health Practice Project quality assessment tool.31 Overall, the quality of studies is good and have moderate risk of bias. Sixteen studies received a ‘Good’ quality rating, and four studies received a ‘Fair’ quality rating. A detailed outcome table of methodological quality assessment by the NIH QA tool can be found in online supplemental appendix 4.1. Only 3 out of 20 studies32–34 met criteria 3—‘Was the participation rate of eligible persons at least 50%?’ and only two out of twenty studies29 35 met criteria 5—‘Was a sample size justification, power description or variance and effect estimates provided?’ All other criteria were well received except for one study36 which did not meet criteria 14—‘Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s) and outcome(s)?’. Nine studies had high risk of bias, while 11 studies generally had moderate risks of bias. No study had low risk of bias since all of the included studies adopted cross-sectional study design (online supplemental appendix 4.2).
Data extraction and synthesis
The data extracted from selected publications consisted of the study design, data source, study setting, sampling strategy, participants, statistical analysis methods, the definition of migration, comparator or reference group, and key findings on the NCD risk factors and outcomes. Although most included studies performed multivariate regression analysis, some studies only applied univariate regression analysis and presented unadjusted findings. For those studies that performed multivariate regression analysis, they reported results variously as ORs, HRs and rate ratios. There was significant heterogeneity of the included studies in terms of study population, geographical location. Statistical results were also reported using different reference groups. Some studies use rural or urban residents as the comparison group, and not all included studies chose internal migrants as the comparison group. We conducted a narrative review and synthesis differences for all studies included, stratified by different types of outcomes. The detailed information of the studies, including study design, adjusted OR (AOR) or RR, 95% CIs was extracted and presented in online supplemental appendices 5 and 6 for studies that conducted multivariable regression analysis. We also conducted random-effects meta-analysis where we had a minimum of two studies, using the same outcomes measure, with the same comparison group (ie, rural or urban, or the overall population), and where 95% CIs were reported, or where t-statistics or SEs were presented that allowed calculation of CIs.
Patient and public involvement
Patient and public involvement statement is not applicable in this paper since the patients or the public were not involved in either the design, conduct, reporting or dissemination plans of our research.
Results
Study characteristics
We identified 29 724 citations from bibliographic databases and an additional 92 from other sources. After the removal of duplicates, 25 344 unique studies were screened by title and abstract, and 105 full texts were sourced. Of these studies, 85 studies were further excluded. Twenty studies met the final inclusion criteria. Figure 1 provides details of the process of study identification.

PRISMA flow chart of identifying eligible studies. NCD, non-communicable disease; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Table 2 presents the study characteristics. Among the 20 included studies, 13 were conducted at the national level while the rest were conducted at the city (one study), municipal (four studies), district (one study) or township (one study) level. Fifteen studies compared migrants with rural residents, twelve studies compared migrants with urban groups, and two studies compared migrants with the general population or non-migrants. For the outcome variables, we examined in this paper, two studies only reported descriptive statistics while fifteen studies used multivariate regression to conduct statistical analysis. The detailed methodology of included studies, including the study designs, settings, data sources, sampling methods, participants, definitions of migrant, comparator groups and statistical methods is reported in online supplemental appendix 3.
Summary characteristics of included studies (N=20)
The behavioural risk factors were categorised into four groups: tobacco use (13 studies), alcohol use (13 studies), unhealthy diet (2 studies) and physical inactivity (6 studies). The metabolic risk factors were examined and categorised into four groups: overweight (six studies), obesity (seven studies), central obesity (two studies); raised blood pressure (six studies); raised blood sugar (three studies) and raised blood lipids (two studies). NCD outcomes were also studied and categorised into three groups: diagnosis (no studies), treatment (four studies) and control (two studies).
The detailed methodology of included studies, including the study designs, settings, data sources, sampling methods, participants, definitions of migrant, comparator groups and statistical methods is reported in online supplemental appendix 3.
Findings on NCD risk factors
The detailed results of the studies examined NCD risk factors by multivariable regression models, including mean prevalence or AOR/RR, and 95% CIs were extracted and presented in online supplemental appendix 5 along with study settings, data sources, sampling methods and participants.
Tobacco use
Thirteen studies37–39 reported the difference in smoking behaviour, exposure to secondhand smoke (SHS), and quitting behaviour between migrants and non-migrants. While most studies reported a higher prevalence of tobacco use among migrant populations compared with rural and urban counterparts, studies that adjusted for covariates yielded inconclusive findings.
Using the WHO Study on Global AGEing and Adult Health survey, Oyebode et al32 found migrants and urban dwellers had similar tobacco use in China among those aged 18 years and above (p<0.05).32 In addition, Hou et al, using China Health and Retirement Longitudinal Study, showed no statistically significant differences in self-reported behaviour of ever-smoking status between rural-to-urban migrants and rural non-migrants (AOR 7.1, 95 CI 2.46 to 20.46, p>0.05).37 40
In the unadjusted results, most studies reported that the prevalence of ‘ever smoking’ was higher in migrants compared with urban residents.37 40–43 However, there were no statistically significant differences for smoking outcomes in the meta-analysis (AOR 1.04, 95% CI 0.239 to 4.518; for the ever-smoking outcome) comparing migrant with urban residents (figure 2).

Forest plot of prevalence of NCD risk factors or outcomes (migrants vs urban residents (urban as reference group)). NCD, non-communicable disease.
Only one study examined exposure to SHS among women of reproductive age. Gong et al examined 23 594 women age 15–49 using Chinese Labor Dynamic Survey in 2014, found that the crude prevalence of exposure to SHS among reproductive women with migration experience was higher than those without migration experience (43.9% vs 35.2%).44 Only one study examined quitting smoke. Hou et al37 found that migrants are significantly more likely to quit smoking compared with the rural residents (AOR=3.832, p<0.01).37
Alcohol consumption
Thirteen studies29 32 35 36 38–47 investigated the migrant and non-migrant difference in alcohol consumption yield inconclusive findings. Most studies reported that the prevalence of current drinking was higher among migrants than urban residents35 41–43 and the prevalence of current drinking was higher in migrants than in rural residents.40–43 45 For instance, Qi and Niu42, a high-quality study of respondents aged 18–64 based Internal Migration and Health in China survey, indicated that migrants were currently more likely to drink alcohol compared with rural and urban residents (28.1% vs 23.9% vs 19.2%).42 However, using a national survey of 4026 respondents in nine provinces, Chen et al38 reported that migrant men were less likely to drink alcohol compared with both rural male men (p<0.01) and urban men(p<0.01).38 The study also found that migrant women were more likely to drink alcohol compared with rural women (p<0.01), while migrant women were less likely to drink alcohol compared with urban women (p<0.05).38
Unhealthy diet
Two studies32 36 that examined differences in dietary habits, including the intake of fruits and vegetables, meats, soybean and dairy products between migrants and non-migrants, yielded mixed findings. Oyebode et al32 found no statistically significant difference between migrants and rural residents in their consumption of more than 5 portions of fruit and vegetables per day.32 In contrast, Yu et al,36 a moderate-quality study only investing township level, found that migrants had a significantly lower intake of fruits, vegetables, meats and eggs compared with urban residents.36
Physical inactivity
Six studies32 35 42 43 45 47 examined differences in physical activity between migrants and non-migrants with mixed results. Four out of six studies found that migrants were less likely to undertake physical activity compared with non-migrants.32 35 43 45 Oyebode et al32 found that the prevalence of occupational physical activity was significantly lower (RR=0.59, 95% CI 0.35 to 0.87), but leisure-time physical activity was much higher (RR=5.10, 95% CI 3.02 to 7.86) among migrants compared with rural populations.32 Qi nd Niu42 showed that migrants had a higher prevalence of physical inactivity compared with rural non-migrants (20.2% vs 13.4%), but migrants had a lower prevalence of physical inactivity compared with urban citizens (20.2% vs 23.0%).42
Overweight
Six studies29 32 35 45 46 48 examined the prevalence of being overweight (ie, body mass index (BMI) larger than 25 but smaller than 30), with mixed results. Three out of six studies reported that overweightness was more prevalent in migrants than in non-migrants.29 45 46 For instance, Shan et al46, a local study focusing on the health of migrant population among Yi ethnic group in Sichuan Province of China, revealed that Yi migrants had a higher prevalence of overweightness compared with Yi rural residents (29.29% vs 4.74%).46 Shan et al also reported that migrants had a significantly higher likelihood (OR=5.52, 95% CI 3.62 to 8.42) of being overweight or obese compared with rural residents.46 Bi et al29, a high-quality study of 48 704 participants nationally using 2012 China NCD and Risk Factor Surveillance in Migrant Workers study, examined the gender difference in metabolic risk factors.29 This study revealed that the age-standardised prevalence of being overweight was significantly more prevalent among migrant men compared with men in the general population (33.5% vs 29.2%, p<0.001).29 However, it was also found that prevalence of being overweight was significantly less prevalent among female migrants compared with women in the general population (24.8% vs 25.8%, p<0.001).29
Obesity
Seven studies examined the prevalence of obesity (ie, BMI no less than 30 kg/m2).29 32 35 42 45 46 48 In comparison to urban residents, both studies found that migrants were less likely to be obese.35 42 However, in comparison to rural residents, the results are inconclusive.32 36 42 44 45 For instance, Qi and Niu42 found that migrants had a lower prevalence of obesity compared with the rural group and urban group, (2.4% vs 6.4% vs 6.2%).42 In comparison to general population, Bi et al29 revealed that obesity was more prevalent among migrants compared with non-migrants with statistical significance (male: 33.5% vs 29.2%, female: 24.8% vs 25.8%).29
Raised waist circumference
Two studies assessed the prevalence of raised waist circumference with mixed results.29 32 Oyebode et al, a high-quality study, revealed that migrants have a slightly lower risk of raised waist circumference than rural residents (RR 0.94, 95% CI 0.64 to 1.30).32 By contrast, Bi et al29, revealed that raised waist circumference was statistically significantly more prevalent among migrant to general population in regard to male (29.0% vs 23.7%).29 In regard to female, Bi et al29, also found that the prevalence of central obesity was slightly higher in migrant compared with general population, however, the result is not statistically significant (40.0% vs 38.9%).
Raised blood pressure
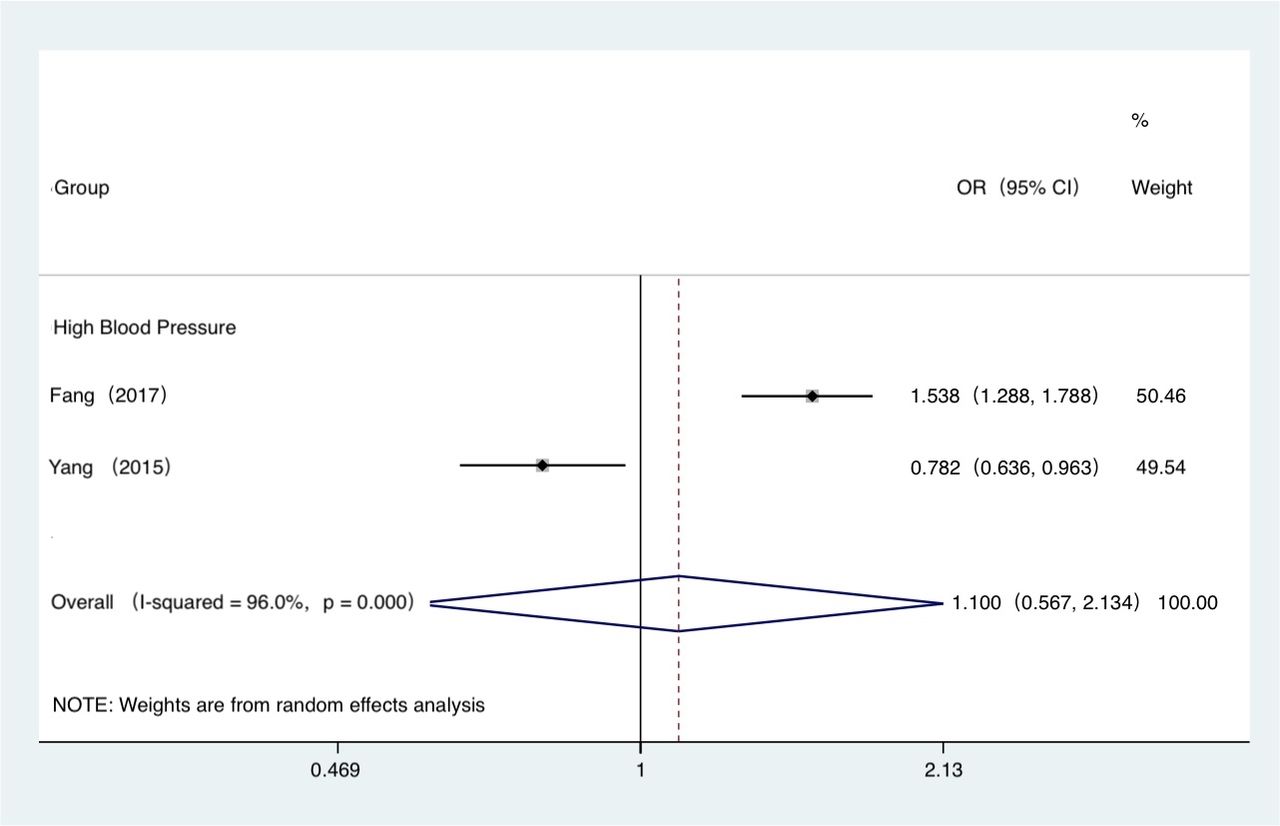
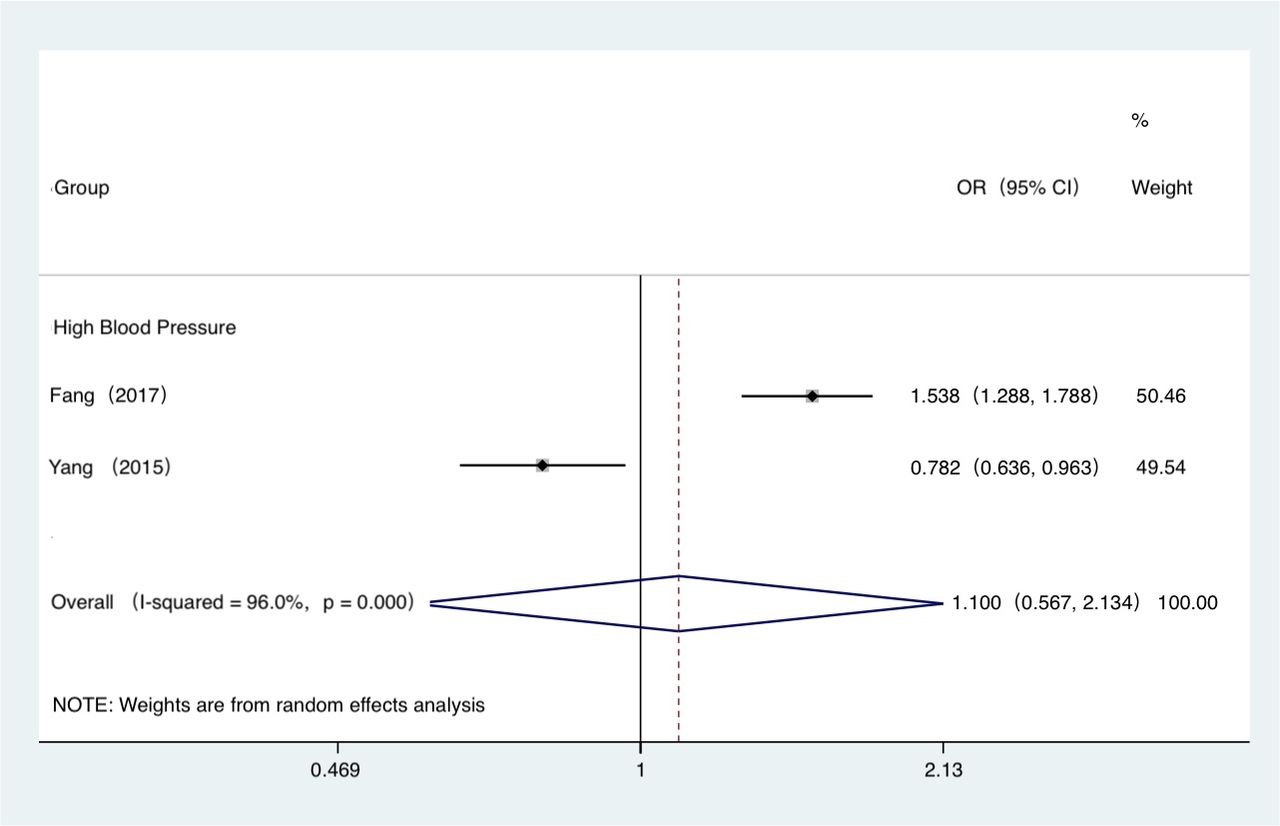
Six studies29 32 42 47–49 reported the prevalence of raised blood pressure as measured by direct physical measurement with mixed findings. Four out of six studies indicated a lower prevalence of elevated blood pressure among migrants compared with non-migrants.29 32 42 49 For instance, Bi et al29, a high-quality study, showed that the prevalence of hypertension was lower among migrants compared with the general population for both males (26.6% vs 29.9%) and females (17.3% vs 24.4%) with statistically significance.35 Qi and Niu42 found similar prevalence of hypertension among migrant, rural and urban residents (p>0.05).42 By contrast, two studies that assessed hypertension in the Yi population revealed that the prevalence of hypertension was higher in Yi migrants compared with Yi farmers.47 48 The pooled OR of high blood pressure derived by meta-analysis was 0.848 (95% CI 0.658 to 1.094; I∧2=0.00%; figure 2) for migrants compared with urban residents, and the pooled OR of high blood pressure was 1.100 (95% CI 0.567 to 2.134; I∧2=96%; figure 3) for migrants compared with rural residents.
{kind=link}
{kind=link}
{kind=link}
Forest plot of prevalence of NCD risk factors (migrants vs rural residents (rural as reference group)). NCD, non-communicable disease.
Raised blood sugar
Three studies reported the prevalence of raised blood sugar, measured by direct physical measurement, with mixed findings.29 32 47 Wang et al47 only focusing on southwestern China and compared Yi ethnic groups, found that the prevalence of diabetes in migrants was higher than that in rural non-migrants.47 Similarly, Oyebode et al32 reported that migrants had an 86% higher likelihood (RR 1.86, 95% CI 1.05 to 3.25) of being diagnosed with diabetes compared with rural residents.32 In contrast, Bi et al29, a high-quality study, showed that the prevalence rate of diabetes in migrants was lower than that of the general population with statistical significance (p<0.001).29
Raised blood lipids
Two studies reported the prevalence of raised blood lipids, measured by direct physical measurement, with mixed findings.29 47 Bi et al29 showed a much lower prevalence rate of dyslipidaemia in migrants compared with the general population with statistical significance (p<0.001).47 By contrast, Wang et al47 indicated that Yi migrants had a higher prevalence of dyslipidaemia than the Yi farmers.47
Findings on NCD management
The detailed results of the studies examined NCD outcomes by multivariable regression models, including mean prevalence or AOR/RR, and 95% CIs were extracted and presented in online supplemental appendix 6 along with study settings, data sources, sampling methods and participants.
NCD diagnosis
There is no evidence on undiagnosed NCDs.
NCD treatment
Four studies evaluated access to non-traditional treatment for hypertension, diabetes and cardiovascular conditions with mixed findings.33 34 49 50 Three out of four studies found that migrants were less likely to receive treatment for NCDs compared with rural or urban residents.33 34 49 For instance, Chen et al, a high-quality study based on 19 provinces in China, found that migrants are less likely to receive treatment for chronic conditions, compared with their urban counterparts (AOR 0.51, 95% CI 0.11 to 2.43 for rural-to-urban migrants compared with urban residents). However, these estimates did not reach statistical significance due to small sample size.33 In contrast, Xu et al,50 a study based on 993 patients with diabetes aged 45 years old and above, found that diabetes treatment did not significantly differ between migrants and urban residents (OR 1.07, 95% CI 0.67 to 1.69; p=0.779).50 There were no statistically significant differences in NCD treatment outcomes (AOR=0.89; 95% CI 0.61 to 1.29) comparing migrants with urban residents in the meta-analysis (figure 2).
NCD control
Two studies evaluated the prevalence of controlled blood pressure, defined as systolic BP less than 140 mm Hg and diastolic BP less than 90.34 49 Both studies revealed that there was no difference in the prevalence of controlled blood pressure between migrants and non-migrants.34 49 For instance, Fang et al49, a high-quality study, revealed that hypertensive migrants had a slightly lower probability of controlled blood pressure compared with hypertensive non-migrants (OR 0.91, 95% CI 0.53 to 1.57). Nevertheless, this finding was not statistically significant.49
Discussion
Principal findings
Our findings suggest the rural-urban-migrant differences in NCD risk factors and management in China remain uncertain. While most studies found migrants have a higher prevalence of tobacco use compared with urban residents, these differences were not statistically significant in the meta-analysis. Although some studies suggested that migrants may have worse access to NCD treatment and lower rates of blood pressure control, these findings were not statistically significant. None of the previous studies have examined life-course differences in NCD risk profiles by rural-urban-migrant population. There is little and very weak evidence that differences in NCD diagnosis, treatment and control between migrants and non-migrants in China.
The worse NCD treatment and control among migrants compared with their urban counterparts may be due to the differences in the health insurance schemes available to urban residents and migrants. Insufficient health insurance coverage among migrants poses barriers to seeking health services.51 Additionally, reimbursement constraints for those migrant employees under current medical insurance scheme may result in them seeking healthcare primarily for acute NCD conditions. The lower access to and utilisation of healthcare services may thus lead to a lower treatment and control rate among migrants compared with urban residents.
Strength and limitation
To our knowledge, this systematic review is the first study in China that has systematically analysed behavioural risk factors, metabolic risk factors and NCD outcomes among three comparison groups (migrants, rural and urban residents) simultaneously to assess migration-related differences in NCD-related risk factors and outcomes. In addition, this systematic review provides a comprehensive examination of the available literature. Ultimately, this work highlights the need for a greater effort in improving NCD-related health outcomes and disease management for all migrants. It also strengthens the evidence base and establishes common approaches to measure and assess NCD health outcomes among these populations.
However, the overall quality of the studies was generally low with methodological flaws, weak statistical tests, inadequate adjustment for confounding and limited generalisability in terms of the overall population in China. Cross-sectional designs used to estimate the difference in NCD risk factors and health outcomes between migrants and their counterparts have limitations as they do not provide information on changes in outcomes of interest over time. Additionally, most studies investigated very few common NCDs, such as hypertension and diabetes. Studies focusing on migrant and non-migrant disparities regarding several severe chronic diseases are lacking and there were no studies identified on cardiovascular disease and chronic obstructive pulmonary disease.
Policy implications
Large-scale internal migration in China in the past three decades has introduced several crucial challenges to the healthcare system in the country.52 53 Previous studies of migrant health in China were mainly focused on infectious diseases, maternal health and occupational disease and injuries.35 Findings from this study demonstrate there is currently insufficient evidence on the differences in NCD risk factors and management of NCDs between migrant and non-migrant populations in China. Policy-makers should use caution when implementing population-based targeting NCD strategies. Continuous monitoring of the migrant population’s NCD status and other health outcomes is warranted, given some evidence has suggested migrants may be exposed to different risk factors and have worse health outcomes compared with their rural and urban counterparts.
Our findings suggest that migrants may have worse treatment and control of their NCDs compared with their counterparts, but there were very few studies to confirm this definitively and these findings were not statistically significant in the meta-analysis. A feasible explanation of this difference is that internal migrants in China are less likely to seek timely treatment for their NCD. This may be due to insufficient health insurance coverage among internal migrants in China as migrants are often excluded from the welfare and social security systems of cities and have inadequate health insurance coverage, requiring patients to pay more for healthcare.54 It is necessary to reach out to the migrant population and provide equal access to health services in urban areas. Access to health services is closely associated with the Chinese hukou system. It is imperative that the restrictive rural-urban division of the hukou status is reformed, especially about citizens’ basic rights of equal access to education, healthcare and social services.55
Optimising the health insurance system can play an important role in improving access to healthcare services and provide financial risk protection. Health policies should consider removing barriers to migrants accessing healthcare in their new city of residence, changing social health insurance reform to consolidate rural and urban insurance schemes and allowing greater portability for all people, including migrants. At the end of 2015, China had officially announced the merger of the UEBMI and the new rural cooperative medical care, and one of the most critical elements was the further extension of funding pools and narrowing of disparities in health services and medications covered between the migrants and urban–local residents.56 Future research is needed to examine the effect of these interventions on reducing inequalities in access to healthcare and health outcomes between migrants and non-migrants in China.
Conclusion
Overall, NCD prevention for internal migrant populations is likely to remain the top priority of public health policy in China. Further research is expected to understand health-seeking behaviours of migrant populations, including implications of such behaviours and management of NCDs for health outcomes and long-term healthcare costs among internal migrants in China.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @RifatAtun
Contributors CXQ conducted the whole systematic review, from search to data synthesis. She also drafted and revised the paper. JL initiated the collaborative project. He also conducted the risk of bias assessment and revised the paper. YZ was responsible for the data synthesis and revised the paper, especially the discussion part. KA reviewed all the articles assessed for eligibility and conducted the quality assessment. NT revised the introduction part. AD, RA, VMQ and PM also help revised the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.