Article Text

Abstract
The COVID-19 pandemic has highlighted global oxygen system deficiencies and revealed gaps in how we understand and measure ‘oxygen access’. We present a case study on oxygen access from 58 health facilities in Lagos state, Nigeria. We found large differences in oxygen access between facilities (primary vs secondary, government vs private) and describe three key domains to consider when measuring oxygen access: availability, cost, use. Of 58 facilities surveyed, 8 (14%) of facilities had a functional pulse oximeter. Oximeters (N=27) were typically located in outpatient clinics (12/27, 44%), paediatric ward (6/27, 22%) or operating theatre (4/27, 15%). 34/58 (59%) facilities had a functional source of oxygen available on the day of inspection, of which 31 (91%) facilities had it available in a single ward area, typically the operating theatre or maternity ward. Oxygen services were free to patients at primary health centres, when available, but expensive in hospitals and private facilities, with the median cost for 2 days oxygen 13 000 (US$36) and 27 500 (US$77) Naira, respectively. We obtained limited data on the cost of oxygen services to facilities. Pulse oximetry use was low in secondary care facilities (32%, 21/65 patients had SpO2 documented) and negligible in private facilities (2%, 3/177) and primary health centres (<1%, 2/608). We were unable to determine the proportion of hypoxaemic patients who received oxygen therapy with available data. However, triangulation of existing data suggested that no facilities were equipped to meet minimum oxygen demands. We highlight the importance of a multifaceted approach to measuring oxygen access that assesses access at the point-of-care and ideally at the patient-level. We propose standard metrics to report oxygen access and describe how these can be integrated into routine health information systems and existing health facility assessment tools.
- health services research
- treatment
- cross-sectional survey
- COVID-19
- pneumonia
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Oxygen access is poorly understood and the most commonly used metrics (eg, presence of an oxygen source) do not correlate well with actual access to patients.
Pulse oximetry use is a critical indicator for the quality of oxygen services and may be a reasonable reflection of oxygen coverage to patients with hypoxaemia.
Oxygen, and pulse oximeter, availability must be assessed at the point-of-care in all major service delivery areas, as intrafacility oxygen distribution is highly inequitable.
Minimum functional requirements for oxygen sources must be assessed, as oxygen concentrators and cylinders may be present without being in working order.
Background
Oxygen therapy is an essential medicine required for stabilisation and treatment of severely ill patients with conditions such as COVID-19, pneumonia, and sepsis, and safe anaesthetic care.1 Reliable oxygen services are therefore crucial for every health facility that cares for unwell newborns, children or adults, and every facility providing obstetric, surgical and post-operative care.
The COVID-19 pandemic has highlighted the importance of hospital oxygen systems and exacerbated existing deficiencies.2 The pandemic has also revealed gaps in how we understand ‘oxygen access’ and the tools we use to measure it.3
In this paper, we use an illustrative case study from Nigeria to describe three domains of data required to meaningfully assess oxygen access. We aim to share lessons learnt about assessing oxygen systems in a variety of facility contexts, to provide guidance for hospital managers, health administrators, policymakers, funders and supporting non-governmental organisations.
What do we mean by ‘oxygen access’?
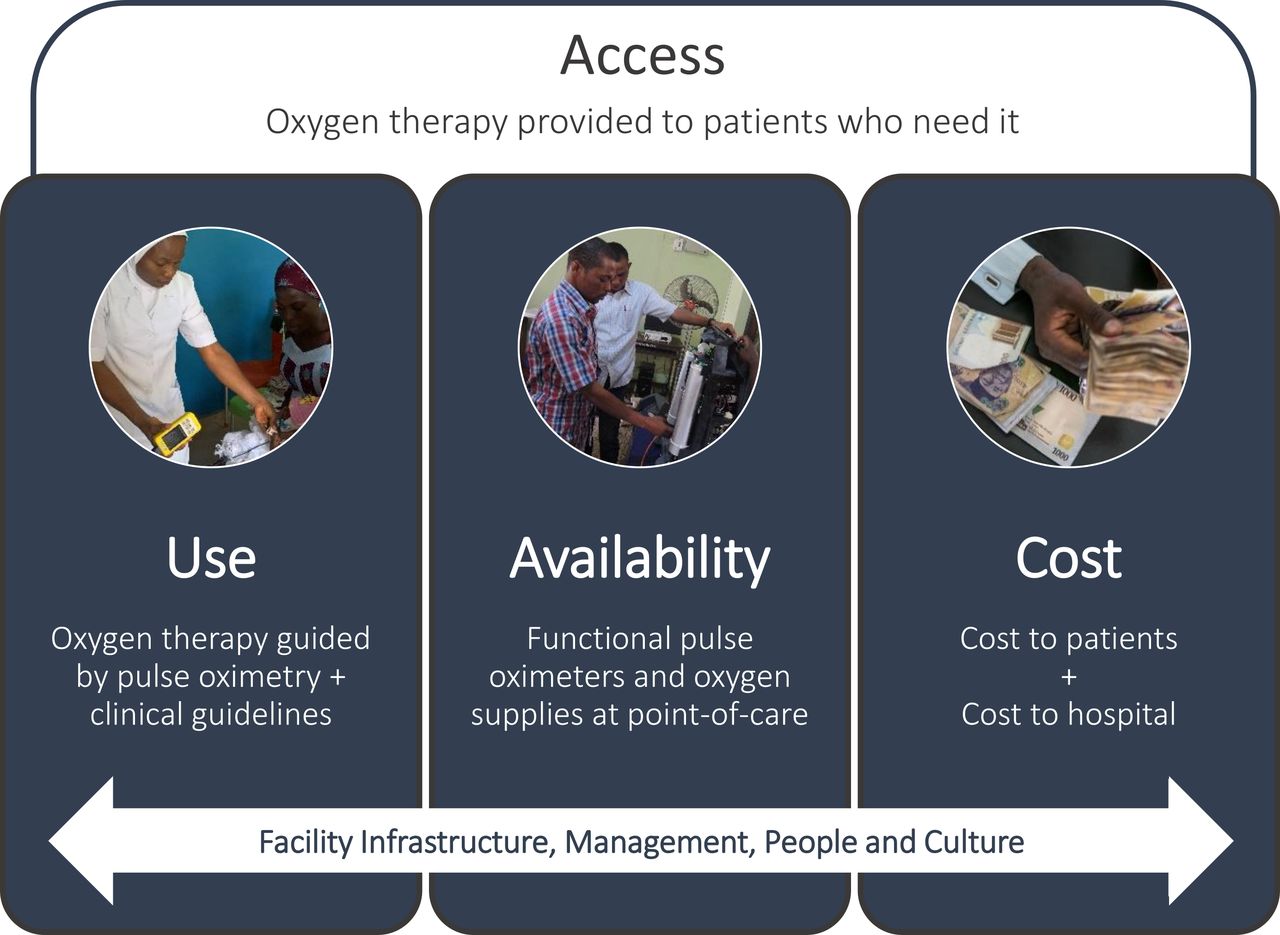
Access to medicines from a health systems perspective involves medication availability, affordability, quality and rational use.4 This means that oxygen access requires quality oxygen therapy to be available and affordable to those who need it, when they need it and used in a safe and rational way.
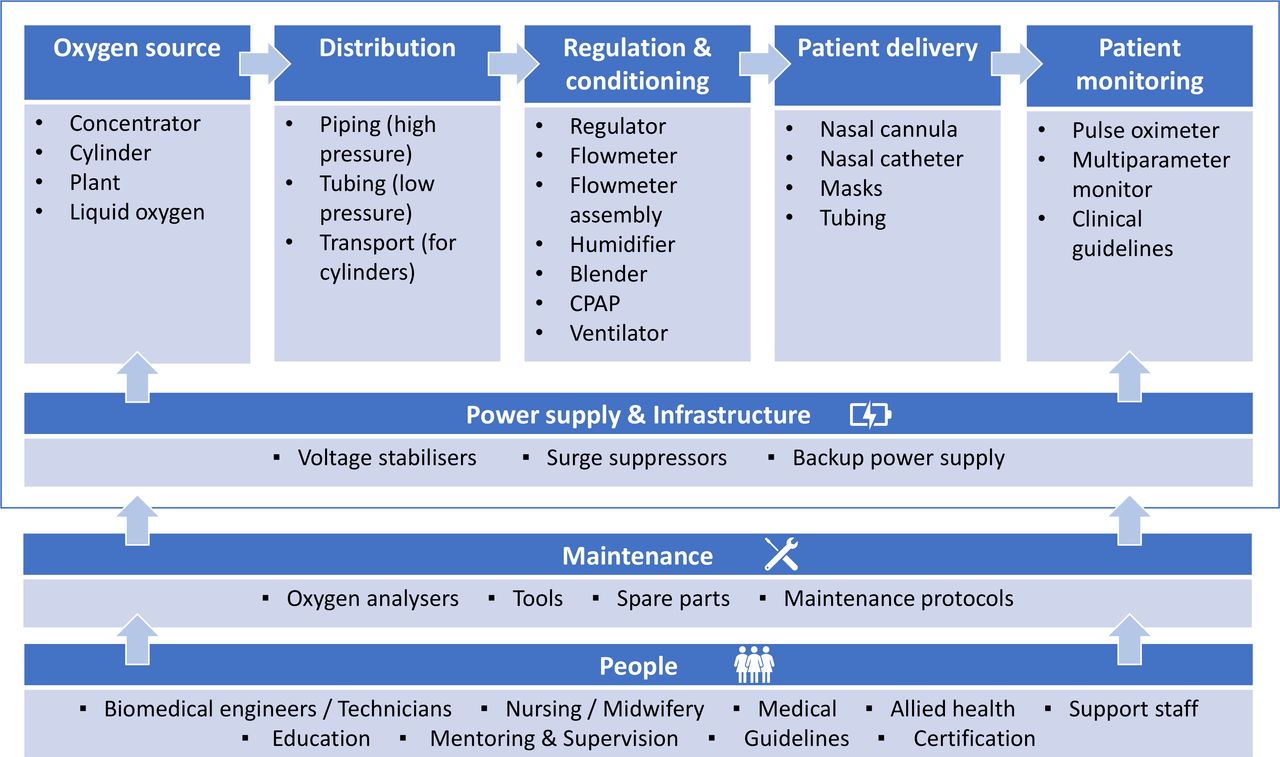
While these four core domains apply to all essential medicines, oxygen systems are somewhat unique. Medical oxygen must achieve high quality standards—including being ≥82% in purity.5 For medical oxygen to be safely administered, delivery devices must be appropriate for the particular patient and indication (eg, nasal cannula, mask with reservoir bag) and guided by the clinical situation and blood oxygen measurements (eg, SpO2, peripheral oxygen saturation from a pulse oximeter). Medical oxygen must be continually available at points-of-care throughout health facilities—from emergency departments, to wards and operating theatres. Achieving this depends on a range of medical technologies and devices (eg, oxygen concentrators, cylinders), people (eg, technicians, nurses/midwives, doctors, administrators) and broader infrastructure and logistic systems (eg, power supply, maintenance and repair tools and systems) (figure 1).

Hospital oxygen systems require key components, including people, maintenance systems, infrastructure and a range of medical devices and supplies (adapted from WHO, UNICEF5). CPAP, continuous positive airway Pressure.
Current widely used facility survey tools, including the Service Provision Assessment (SPA) and Service Availability and Readiness Assessment (SARA), focus on the binary question of ‘is oxygen equipment available?’. This approach neglects many of these other important dimensions, as well as whether the equipment is functional, what clinical areas it serves, whether healthcare workers (HCWs) can recognise who requires oxygen therapy or if patients can afford it. As such, this binary approach is a poor reflection of whether patients who need oxygen are actually getting it.6
Case study: inspiring project, Lagos, Nigeria
Nigeria is a populous lower-middle income country in West Africa with high child (2019: under-five mortality rate 117.2 per 1000 live births) and maternal mortality ratios (2017: 770 per 100 000 live births).7 Lagos is the most populous state, located in the south-west on the Gulf of Guinea. The Lagos population live in urban/peri-urban environments and have lower child mortality rates (50 per 1000 live births) and poverty levels (1.1% live in severe poverty) compared with Nigeria as a whole.8
Recent studies in Nigeria have shown major deficiencies in existing hospital oxygen systems and highlighted the importance of oxygen in improving pneumonia case management and preventing deaths.6 9–13 To better understand the current oxygen capacity and needs of health facilities in Lagos, we surveyed 58 health facilities in Ikorodu local government area (LGA), with an emphasis on paediatric care. We included all government primary health centres (PHCs, n=28), all secondary healthcare facilities (SHFs, n=3) and a random sample of private primary care facilities (n=27/148) (figure 2). There are no tertiary care facilities in Ikorodu LGA.

Flow diagram showing selection of 58 health facilities in Lagos, Nigeria. Initial identification of facilities conducted in November 2019. We randomly assigned numbers to private facilities then screened and selected until reaching the prespecified target number for enrolment. LGA, local government area.
Trained data collectors conducted facility visits between January and August 2020, collecting data from observation, equipment testing and staff surveys using a standardised form, input directly onto tablet computers using CommCare (Dimagi, Cambridge, Massachusetts, USA). We used Handi+ and UltraMax02 oxygen analysers (Maxtec, Salt Lake City, Utah, USA) to test oxygen purity and ProSim SPOT Light (Fluke Corporation, Everett, Washington, USA) to test pulse oximeter function. We cleaned and analysed data using Stata V.15 (StataCorp) and report data descriptively under three broad domains: availability, use, cost (figure 3).
{kind=link}
{kind=link}
{kind=link}
Three domains of data on the quality of ‘oxygen access’.
Patient and public involvement
This study was conducted to inform the ‘Integrated Sustainable childhood Pneumonia and Infectious disease Reduction in Nigeria’ (INSPIRING) programme, implemented by Save the Children to improve child health in Jigawa and Lagos states. INSPIRING involved civil society representatives in co-design activities, including a co-design workshop in April 2019 involving representatives from civil society, local and national government and professional organisations, together with Save the Children, GSK and evaluation partners. Selection of the facilities was conducted in partnership with the Ikorodu local government. Community perspectives were sought during the situational analysis but did not contribute substantively to this study.
Availability: pulse oximetry
Pulse oximeters enable HCWs to accurately and non-invasively measure blood oxygen levels and guide oxygen treatment decisions.14 Given that clinical signs of hypoxaemia (low blood oxygen level) lack both sensitivity and specificity, pulse oximeters are now a global standard of care for hypoxaemia management and regarded as a ‘priority medical device’ by WHO.15 16
Is a pulse oximeter present?
We located pulse oximeters in all three SHFs—exclusively located in the paediatric wards; none of the government PHCs and 56% (15/27) of the private primary care facilities. In the private facilities, oximeters were typically located in outpatient clinics (12/27, 44%), paediatric ward (6/27, 22%) or operating theatre (4/27, 15%) (table 1). The two government hospitals were the only facilities that had paediatric oximetry probes available.
Oxygen access summary data for secondary and primary health facilities in Ikorodu LGA, Lagos, Nigeria
Is the pulse oximeter functional?
We tested 27 oximeters in 22 ward areas, including 4 desktop, 5 handheld and 18 fingertip oximeters (table 1, detail in online supplemental appendix). Models varied widely, half (14/27, 52%) had visible CE markings, indicating conformity with European regulatory standards. Twenty-two of 27 (81%) oximeters turned on, and 19/27 (70%) provided an SpO2 reading. Testing with the Fluke device revealed that 13/19 (68%) were within ±2% of the correct SpO2 for a simulated healthy person (one read falsely low, five gave no reading). However, only 9/19 (47%) were within ±3% for a simulated sick person (two read falsely high, eight gave no reading). Overall, one-third (9/27) of oximeters were demonstrably functional, including 3/4 (75%) desktop, 1/5 (20%) handheld and 5/18 fingertip (28%) devices—all at private primary care facilities.
Supplemental material
Availability: oxygen supplies
Is an oxygen source present?
We found all SHFs (3/3) and private facilities (27/27), and half of PHCs (12/28, 43%), had an oxygen source in the facility (table 1). Similar numbers of facilities used oxygen cylinders and oxygen concentrators (34 vs 32), and many facilities had both (24/58, 41%; table 1). No facilities had a bulk liquid oxygen tank or oxygen plant.
Most oxygen cylinders (49/82, 60%) and concentrators (27/42, 64%) were in the operating theatre, intensive care unit or delivery room (online supplemental appendix). Seven facilities had cylinders in store for distribution to wards on demand.
Is the oxygen source functional?
We visually inspected and tested 42 oxygen concentrators in 36 ward areas; 11 could not be fully tested due to power failure (n=10) or active clinical use (n=1). Models varied greatly and one-third (26/42, 62%) had visible CE markings. We found 5/42 (12%) were functional at the time of inspection (table 1, online supplemental appendix). All used main power as the primary power source, but only 4/42 (10%) used a voltage stabiliser to protect the device from power fluctuations.
We visually inspected 82 oxygen cylinders in 43 ward areas, finding 53/82 (65%) cylinders had a regulator apparatus available (or manifold connection for piped supply) making them ready for use (table 1, online supplemental appendix). We did not obtain reliable data on leaks, oxygen purity or pressure.
Overall, 34/58 (59%) facilities had a functional source of oxygen available on the day of inspection, of which 31 (91%) had it available in a single ward area (11 exclusively in the operating theatre, 10 delivery suite, 5 emergency, 2 clinic room, 1 ward, 2 store) (table 1, online supplemental appendix). We did not evaluate the presence of appropriate oxygen delivery devices.
What is the technical capacity for oxygen provision?
Five facilities (9%), including all three SHFs, had onsite biomedical engineers or technicians; but only two of these facilities had staff who had been trained on oxygen equipment (table 1). Three facilities (5%) had routine maintenance schedules for medical equipment and reported performing oxygen concentrator and/or cylinder maintenance in the past 6 months. One facility reported procurement of concentrator and cylinder spare parts in the past year. We did not evaluate technician skills or knowledge.
Cost of oxygen
What is the cost of oxygen services to patients?
We obtained patient oxygen cost data from 39/58 (67%) facilities, which variously billed for oxygen using hourly or daily rates, or per admission, cylinder or episode of use. When available, oxygen was typically free to patients at PHCs, but expensive in SHFs and private facilities. The median cost for 2 days oxygen was 13 000 Naira (US$36) and 27 500 Naira (US$77), respectively, accounting for two-thirds of the cost of a 3-day admission for a child with severe pneumonia (table 2). This is consistent with previous findings of high out-of-pocket costs for oxygen services in Nigeria6 and reflective of Nigeria’s relatively high out-of-pocket health expenditure (2018: 77% of total health expenditure).17
Estimated cost of a 3-day admission or stabilisation care at government PHC, for a child under 5 years of age with severe pneumonia
What is the cost of providing oxygen services to facilities?
We found no facilities that included oxygen-related items in their budgets, and few could provide information on pulse oximeter, oxygen concentrator or cylinder costs. Limited data from seven facilities suggested median oximeter purchase cost was 93 500 Naira (US$260), range 7000–180 000 (US$19–500); concentrator purchase cost was 160 000 Naira (US$446), range 80 000–350 000 (US$223–975); and cylinder refill cost was 640 Naira per cubic metre (~US$2), range 250–1470 (US$1–4) (online supplemental appendix).
Clinical use of oxygen
In addition to having pulse oximeters and oxygen supplies available, rational use of oxygen also requires trained and motivated HCWs who regularly perform pulse oximetry and provide oxygen therapy according to clinical guidelines.10 18
What is the capacity of healthcare workers to provide oxygen therapy?
We conducted knowledge and skills tests for 169 HCWs in 56 of the 58 facilities (online supplemental appendix). Participants included doctors, nurses, midwives, health assistants,and community health extension workers with varying levels of experience (median 12 years).
One-quarter (40/169, 24%) of HCWs reported training on oxygen, and one-third of these had been trained in the past 5 years (online supplemental appendix). Most HCWs (97/169, 57%) reported experience using oxygen therapy, though only 13 (8%) had administered oxygen in the prior 2 weeks. Experience with oxygen therapy was low in government primary care facilities (2/96, 2%, had used in previous 2 weeks), despite regularly seeing children who required resuscitation (10/96, 10%, had resuscitated a child in the previous 2 weeks).
Knowledge test results showed generally low appreciation of the fundamentals of oxygen therapy, with many respondents lacking the confidence to answer questions—particularly in government primary care facilities (online supplemental appendix). For example, 22% (37/169) of HCWs could identify the core functions of pulse oximetry (ie, heart rate and SpO2) and 28% (48/169) recognised that a child with an SpO2 of 87% warranted oxygen therapy.
Is pulse oximetry a routine practice?
Audit of routine case notes for children presenting with acute illness to outpatients in a subsample of 12 participating clinics (April–September 2020) showed that pulse oximetry use was low in secondary care facilities (32%, 21/65 patients had SpO2 documented) and negligible in private facilities (2%, 3/177) and PHCs (<1%, 2/608).
Among all participating facilities, 17/27 (63%) of the oximeters had not been used in the previous day and only five (19%) had been used ≥10 times (online supplemental appendix). Thus, despite 31% of facilities having an oximeter, routine use was rare.
Is oxygen therapy provided to all patients who need it?
The capacity to deliver oxygen services does not tell us whether the patients who need oxygen are actually getting it. The clearest metric to measure actual oxygen access to patients is the proportion of patients with hypoxaemia (typically defined as SpO2 <90%) who are provided with oxygen therapy. We were unable to obtain this data via clinical audit as pulse oximetry coverage was too low and hypoxaemia cannot be accurately determined using clinical signs alone.9 Alternative approaches to measuring oxygen access to patients are using cross-sectional hypoxaemia and oxygen therapy surveys,19 crude counts of patients who receive oxygen or relying on HCW recall about oxygen supply stock-outs.20 These approaches are problematic and provide a poor indication of whether oxygen is actually reaching those who need it.10
Triangulating the data from the 58 health facilities shows clear gaps between need and access with the vast majority of facilities and ward areas lacking a functional oxygen supply and/or pulse oximetry capacity (online supplemental appendix). At best, 10 facilities had oxygen supply adequate to provide minimum services to at least one ward area but only the two government hospital paediatric wards had both oxygen supplies and routine pulse oximetry. Without routine pulse oximetry, the other facilities are likely to miss up to 50% of patients with hypoxaemia even with adequate oxygen supplies.9
Implications
The COVID-19 pandemic has illuminated the need to better measure access to oxygen therapy and stimulated activity to respond.3 21 As part of a comprehensive response to the pandemic,22 the WHO has released guidance on oxygen-related biomedical equipment, including how to conduct facility surveys23 and technical specifications.5 24 25
Many other governmental and non-governmental organisations are also working to document oxygen access capacity and needs in health facilities globally—including large-scale facility surveys26 27—and provide practical tools to improve access (eg, UNICEF online repository at https://bit.ly/OxygenResources).21 However, if these efforts count oxygen equipment without assessing actual oxygen availability and patient access, they will overestimate the capacity of current oxygen systems and condemn patients to substandard care—particularly those in smaller and more remote facilities.
We tested strategies to obtain more meaningful data on oxygen access, identifying lessons learnt that can help HCWs, hospital managers, health administrators, policymakers and funders who wish to better understand and respond to the oxygen access crisis (box 1). We included a wide variety of healthcare facilities in Lagos state, Nigeria, and while our specific findings reflect this urban Nigerian environment, the broader lessons about measuring oxygen access are highly generalisable. We focused on oxygen access metrics that would be most widely applicable and broadly feasible but recognise that some readers will also want additional detail on specific populations (eg, neonates), services (eg, continuous positive airway pressure (CPAP)) or supply systems (eg, cylinder distribution).
Summary of lessons learnt on assessing oxygen access
Lessons learnt: oxygen use
Measuring the proportion of hypoxaemic patients receiving oxygen therapy is the single most important indicator for evaluating patient access—but is only interpretable with reliable pulse oximetry data to define the denominator.
Pulse oximetry coverage (ie, the proportion of patients who receive pulse oximetry and have SpO2 documented) is a critical indicator of the quality of oxygen services. Given that pulse oximetry is essential to identifying who requires oxygen and routine pulse oximetry is rare without oxygen supplies, pulse oximetry coverage may be a reasonable proxy for patient oxygen access.
The presence of a pulse oximeter correlates poorly with actual use. If clinical data on oximetry use is unavailable, reported device use may be an acceptable proxy.
Lessons learnt: pulse oximetry availability
Pulse oximeter presence must be assessed in all major service delivery areas—including availability of appropriate oximeter devices and probes for patient populations being served (eg, neonatal and paediatric care).
Simple functional testing of oximeters can be done by applying to your own finger. More detailed testing requires specialised equipment calibrated to particular oximeters and may be most useful to technicians managing large numbers of oximeters.
Some low-cost oximeters, particularly fingertip devices, are not suitable for children or unwell populations with low perfusion and/or dark or thick skin.
Assessments of healthcare worker knowledge and skills are useful in the context of planning and conducting training—but are a poor reflection of actual oxygen practices. Oxygen practices are largely determined by individual motivators (intrinsic and extrinsic), attitudes and behaviour of peers and seniors, and the culture of the work environment.18
Lessons learnt: oxygen availability
Oxygen availability must be assessed at the point-of-care and include all major service delivery areas. Hospital-wide summary data on the availability of oxygen equipment can be very misleading, as intrafacility oxygen distribution is highly inequitable (eg, skewed towards anaesthetic care).
Minimum functional requirements for oxygen sources must be assessed, as many oxygen concentrators and cylinders may be present without being in working order. For oxygen concentrators, this should include assessment of oxygen purity using an oxygen analyser. For oxygen cylinders, this should include assessment of whether it is currently full or empty and whether it is fitted with a regulator and pressure gauge at point of use.
These basic assessments can be carried out by trained non-experts, but more detailed equipment data requires greater technical expertise.
Efforts to improve hospital oxygen systems must involve hospital technicians and seek to understand existing capacities and restraints without blame. Hospital technicians have valuable skills, experience and understanding of hospital equipment systems, but are too frequently neglected by clinical and administrative decision-makers.
Lessons learnt: oxygen cost
Oxygen costs can be prohibitive to patients and exacerbate existing inequities. Understanding cost structures and variation between facilities could help construct more efficient, equitable oxygen systems.
Many facilities do not keep clear records of their current oxygen expenditure, making it difficult to demonstrate financially advantageous alternatives. Further, reliable cost data may be difficult to obtain without high levels of trust. Assistance to health managers in understanding and forecasting whole-of-system costs for oxygen could improve oxygen system efficiency and sustainability.
To aid readers in adapting our approach to local context and needs, we describe three domains of oxygen access that should be considered when seeking to understand and respond to oxygen needs (figure 3, table 3, box 1).
Summary of most useful indicators of oxygen access
At the centre is patients—evaluating whether patients who need oxygen actually receive it. Evaluating patient oxygen access requires clinical data on pulse oximetry and oxygen use. Recent studies from Nigeria and Malawi have shown that without routine pulse oximetry to guide oxygen therapy, only around 20% of hypoxaemic patients receive oxygen—even if adequate oxygen supplies are available.10 19 Given that pulse oximetry is essential to identifying who requires oxygen and routine pulse oximetry is rare without oxygen supplies,6 18 pulse oximetry coverage (ie, the proportion of patients who receive pulse oximetry and have SpO2 documented) may be a reasonable proxy for patient oxygen access.
High level metrics on pulse oximetry and oxygen use can be sourced via clinical audit but are ideally integrated into health information systems and are essential for health service planning (table 3). More detailed data, including who receives oxygen-related care, where, with what and for how long, would be desirable for hospital-level quality improvement activities and improving oxygen system efficiencies.
While measures of oxygen availability are important, existing surveys that contain this metric often fail to assess functionality of equipment or address intrahospital distribution, missing huge deficiencies in oxygen availability at the point of care.6 13 Basic assessments of equipment functionality and distribution are not difficult and could be integrated into existing surveys such as the SPA and SARA (table 3). More detailed data on equipment types, locations and access to spare parts is useful for hospital-level decision-making and efficiency—particularly in facilities providing a wider range of respiratory support services (eg, CPAP, mechanical ventilation) across multiple service areas.
Measures of oxygen cost are important for planning purposes but were challenging to obtain in practice. We propose metrics that address oxygen costs to patients, crucial in contexts where out-of-pocket health expenditure is high, and oxygen costs to facilities/governments obtained from financial records and surveys (table 3). However, we recognise the difficulties in obtaining sensitive financial information and the limitations of relying on administrator or technician recall in the absence of reliable financial records.
Finally, our case study highlights opportunities for priority improvements in existing oxygen systems. First, pulse oximeters are low-cost devices that were grossly lacking and could substantially improve rational use of existing oxygen supplies. Second, while many devices were non-functional, support for technicians could likely rehabilitate some of these and prevent future growth of equipment graveyards (eg, Open O2 in Malawi, www.openo2.org). Third, many devices did not have CE or similar quality control markings, highlighting the ongoing challenge of inappropriate equipment donation and procurement of consumer devices for medical purposes. Fourth, the differences between government and private facilities highlight that oxygen access is fundamentally an issue of equity and efforts must include smaller, poorer and more rural facilities that care for the most at-risk populations.
Conclusion
Data on oxygen access is lacking and makes efforts to improve oxygen systems for COVID-19 and beyond clumsy and inefficient. We propose three data domains to assess oxygen systems: use, availability and cost. Measuring these three domains of oxygen access will support local, regional and global efforts to provide life-saving oxygen to those in need.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
This study has received ethical approval from the Research Ethics Committee at: University of Ibadan (REF UI/EC/19/0551), Lagos State (REF LS/PHCB/MS/1128/VOL.V1/005), and University College London (REF 3433/005).
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @grahamhamish, @omotayoolojede, @drIsahIsah, @thewrittenro, @tinylungsglobal
Collaborators INSPIRING Project Consortium: Carina King; Tim Colbourn; Rochelle Ann Burgess; Agnese Iuliano; Hamish R Graham; Eric D McCollum; Tahlil Ahmed; Samy Ahmar; Christine Cassar; Paula Valentine; Adamu Isah; Adams Osebi; Ibrahim Haruna; Abdullahi Magama; Ibrahim Seriki; Temitayo Folorunso Olowookere; Matt MacCalla; Adegoke G Falade; Ayobami Adebayo Bakare; Obioma Uchendu; Julius Salako; Funmilayo Shittu; Damola Bakare; Omotayo E Olojede.
Contributors CK, HRG, EM, AI, AAB, AGF and TC conceived the study and TC, CK and AGF are grant holders. CK, TC, HRG, EM, AGF, RB and AAB initiated the study design and OEO and OO led to data collection and implementation. Data analysis was conducted by HRG. The manuscript was drafted by HRG, with input from OEO, AAB and CK. All authors contributed to revisions and approved the final manuscript.
Funding This work was funded through the GlaxoSmithKline (GSK)-Save the Children Partnership (grant reference: 82603743). Employees of both GSK and Save the Children UK contributed to the design and oversight of the study as part of a co-design process.
Disclaimer Any views or opinions presented are solely those of the author/publisher and do not necessarily represent those of Save the Children UK or GSK, unless otherwise specifically stated. Sponsor: University College London (UCL).
Competing interests HRG, EM and CK are advisors to the Lifebox Foundation on pulse oximetry. AAB, AGF and HRG are board members for Oxygen for Life Initiative (OLI), a private non-profit that has provided services to the INSPIRING project. SA, TA, CC and PV are employed by Save the Children UK who are part of the partnership funding the research. TFO and MM are employees of and stockholders in GSK, a multinational for-profit pharmaceutical company that produces pharmaceutical products for childhood pneumonia, including a SARS-CoV-2 vaccine, and no direct financial interests in oxygen or pulse oximeter products.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.