Article Text

Statistics from Altmetric.com
Summary box
Current production and distribution of COVID-19 vaccines as a global public good has failed on equity.
The task of solving global vaccine inequity presents us an opportunity to build better global governance and decision-making mechanism over vaccine production and distribution to assure sustainability and equity between and within countries.
Solving vaccine inequity requires sharing the control and ownership over generating and distributing vaccines, beyond reallocating vaccine doses or building new manufacturing facilities in low- and middle-income countries.
Losing sight of the unequal power relations undergirding vaccine inequity would leave us at the risk of having the global vaccine production and distribution shaped by a handful of powerful nations, multinational corporations, and private philanthropies.
People’s WHO represents our best framework within which governments with limited resources and power can collectively negotiate for the interests of their populations as the global majority.
Solving COVID-19 vaccine inequity requires sharing decision-making power over production and distribution of vaccines as a global public good
As of 9 April 2021, of more than 700 million COVID-19 vaccine doses administered globally, only 0.2% have gone to low-income countries, with over 87% gone to high income countries (HICs) or upper middle-income countries.1 COVAX was established to pool demands and funds among countries to collectively negotiate an affordable price for the vaccine with vaccine manufacturers.2 The aspiration was to ensure equitable distribution of vaccines regardless of countries’ income level. This aspiration failed. COVAX’s collective purchasing power was outcompeted by governments who had greater means to pay and purchased directly from vaccine manufacturers outside COVAX. Consequently, global COVID-19 vaccine supply was left to competition among countries based on their ability to pay rather than public health needs in what can be termed ‘survival of the wealthiest’.
In recognition of the vaccine inequity, civil society actors, governments of wealthy nations (eg, G7, G20) and multilateral agencies have called for redistributing excess doses from HICs to low-income middle-income countries (LMICs), more funding for COVAX, and strengthening local vaccine production capacity in LMICs.3–7 For example, WHO called for ’strengthening local production of medicines and other health technologies’ at a recent World Health Assembly,3 and released a call for proposals to support the capacity of LMICs to produce COVID-19 vaccines by establishing hubs to ‘transfer a comprehensive technology package and provide appropriate training to interested manufacturers in LMICs.’8
Gavi, the Vaccine Alliance, raised US$2.4 billion from governments, the private sector, private philanthropies and multilateral agencies for COVAX to secure additional doses for LMICs.9 The International Monetary Fund, WHO, the World Trade Organization, the World Bank released a US$50 billion investment plan which includes vaccinating at least 40% of the population in all countries by the end of 2021, additional grants to COVAX, donating surplus vaccine doses and investing in additional vaccine production capacity.10
These responses aim at improving access to COVID-19 vaccines through donated doses or increased vaccine production where they are scarce. They are necessary steps towards solving vaccine inequity. What is obscured in this distribution-focused lens is the decision-making power over vaccine production in LMICs.
To illustrate this, consider a strong desire recently expressed by the WHO Member States for strengthening local production of vaccines and other essential medicines and health technologies with a ‘more comprehensive, all-of-government approach’, aligned with national strategies and action plans.3 This desire will necessarily have to be negotiated with other global actors, including wealthy nations, transnational corporations and private philanthropies.
The question of whose views will ultimately set the agenda and shape the implementation of the local vaccine production and distribution at the regional and global level is a question of power. That question hinges on not just sharing vaccine doses and technology but also sharing ownership and control over the means to produce vaccines (eg, knowledge, resources). Global actors negotiate and deliberate on programmes and policies within profoundly unequal relations of power. Unequal relations of power in decision-making over vaccine production should be made visible. Charitable intent and donated doses cannot make up for power asymmetry. They may legitimise and further cement unequal power relations.11 Concentration of decision-making power over vaccine production (i.e. control and ownership) within the hands of a few wealthy nations, corporations and private philanthropies will likely ensure that vaccine inequity recurs.
Solving vaccine inequity requires increasing collective control and ownership of vaccine production and distribution to ensure equitable access based on coordinated but independent agenda setting by countries at the national and regional levels. It requires a governance structure to allow countries with limited resources and power to represent their own interests rather than having to rely on a handful of powerful actors to advocate for them.
Current efforts open an immense opportunity not only to solve the pandemic vaccine inequity in the near-term, but to relook at global governance over production and distribution of vaccines as a global public good towards long-term health equity globally.
We need the leadership of ‘people’s WHO’ to solve vaccine inequity towards a long-term global health equity
In the current economic order where resources and decision-making power are concentrated within HICs, multinational corporations and private philanthropies, it is inherently difficult for the global majority with less resources and power to advocate for their interests and ensure that their perspectives shape global programmes and policies. WHO via its representation of 193 Member States and a rotating, elected 343-member executive board is the world’s best platform within which governments with lesser means and power can collectively negotiate for the interests of the global majority.
A collective desire of the global majority was best expressed in the vision of Health for All articulated in the Alma Ata Declaration from 1978.12 This vision called for a community-driven, government-led ‘health for all’ approach. It was distinct from the market-delivered health services championed by the USA and the highly centralised, state-controlled provision of primary healthcare (PHC) championed by the Soviet Union during the Cold War (1946–1989).12 13
Health for All represented a movement of the global majority, known as Third World, which called for a ‘new system of international economic relations based on equity, sovereign equality and interdependence of the interests of developed and developing countries’.14 In the face of the astounding social inequalities and health inequity laid bare during the COVID-19 pandemic, this vision is more relevant than ever to solving vaccine inequity towards long-term health equity.
To achieve that vision, we urgently need to remake and empower ‘people’s WHO’ as Birn and Nervi aptly termed15 that can effectively represent and advocate for the interests and perspectives of the global majority.
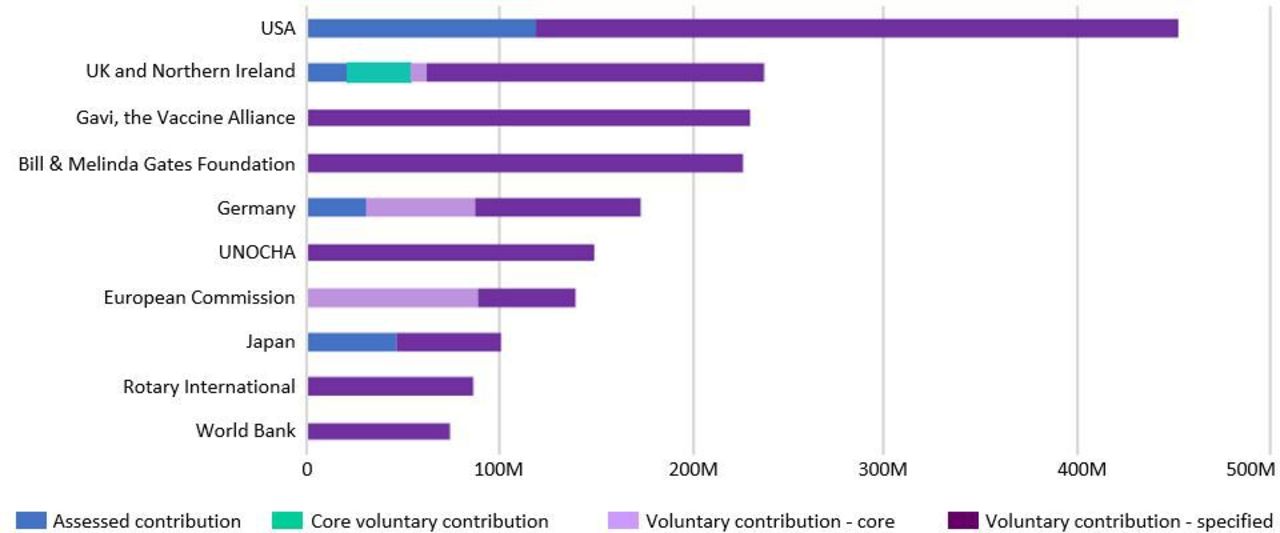
For decades, WHO has been seized and sidestepped by a handful of powerful Member States, multilateral organisations and private philanthropies, notably the Bill & Melinda Gates Foundation.15 16 It is critical to restore WHO’s independent agenda setting in order for it to function as people’s WHO. According to the WHO 2019 Audited Financial Statement, of the total contributions of US$2937 million, most contributions are highly specified and earmarked funding and 64% comes from the top 10 contributors (figure 1).17 Highly specified, earmarked funding hamstrings WHO’s ability to set policies and agenda independently to represent its member states. Instead, it can reduce WHO to the role of merely providing legitimacy to the interests of a handful of powerful actors.15 16

{kind=link}
Top 10 contributors for 2019, combining assessed and voluntary contributions (US$ million). Assessed contributions, a percentage of a country’s gross domestic product agreed by the United Nations General Assembly;Core voluntary contributions, fully unconditional funds;Voluntary contribution—core, voluntary contributions earmarked for purposes within the WHO programme budget and designated at a medium level of flexibility; UNOCHA, United Nations Office for the coordination of Humanitarian Affairs. Adapted from WHO Audited Financial Statements, 2019[17]
A call to action
The world indeed needs a ‘stronger WHO at the centre of the global health architecture’ as emphasized by independent international panels.18 But that WHO needs to be people’s WHO, not a broker for the global elite. An urgent first step towards empowering people’s WHO is to reform the financing of WHO in quality and quantity.18 Non-government funders and donor governments can play a critical role by increasing voluntary contributions from a broader base of the WHO Member States, and shifting the specified, earmarked funding towards unearmarked funding. Indeed, for the top 10 contributors, this is an opportunity to critically reflect on the intended and unintended consequences of their position of power, and join the collective effort towards global health equity as ‘allies and enablers’19 in the spirit of solidarity rather than as leaders with an assumed sense of superiority.
For WHO, it would be imperative to ensure that increased resources strengthen democratic governance within WHO with an increased ‘bottom-up’ orientation. Strengthened democratic governance would ensure that decision-making power is not concentrated in the secretariat in Geneva or among the political elites of Member States, and would reflect the views of Member States and their communities. WHO’s emphasis on country ownership and active engagement with community organisations will continue to be important. Additionally, it would be valuable to have mechanisms within WHO to hold Member States accountable to active engagement with their communities including the most marginalised ones.
Strengthened WHO regional offices would be extremely valuable in providing regional-level collaboration and coordination with other stakeholders (eg, national and regional public health institutions) to generate epidemiological data to guide policies around vaccine development, production and immunisation, and to provide training and certification for integrated disease surveillance: an integral public health function to guide vaccine development and immunisation.
Community organisations will continue to be vital in holding their local governments accountable for the provision of vaccines equitably as part of PHC and demanding that communities’ perspectives and interests shape health programmes and policies rather than the local elites whose interests may be better aligned with the interests of the global elites than those of the local marginalised communities.
Vaccine inequity is rooted in inequalities in ownership and control of resources. Focusing on the distribution side of resources carries the risk of obscuring power relations inscribed in vaccine inequity and of leaving power imbalances unperturbed. Vaccine inequity is unlikely to be solved within profoundly unequal relations of power.
Let us continue our efforts to share vaccine doses, resources and knowledge to close the COVID-19 immunisation gap. At the same time, let us not lose sight of who is calling the shots over production and use of ‘shared’ resources, and who is left at the mercy of others’ making decisions for them.
Data availability statement
There are no data in this work.
Ethics statements
Acknowledgments
I am grateful for incisive feedback on the manuscript from Dr. Elizabeth Ochola at the University of Waterloo, Canada, Dr. Resham Khatri at the University of Queensland, Australia, Dr. Rozita Razavi at the University of Toronto, and Uros Novakovic at Office Ou, Toronto, Canada.
Footnotes
Twitter @HaniKim_hk
Collaborators Elizabeth Ochola; Resham Khatri; Rozita Razavi; Uros Novakovic.
Contributors HK conceptualised and wrote the manuscript.
Funding The author has not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer Views expressed in this article are the author’s alone, and do not represent views, interests or funded work by the Bill & Melinda Gates Foundation.
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.