Article Text

Abstract
Introduction Conventional care packages around screening for sexually transmitted infections (STIs) entail multiple clinic visits and precipitate losses to follow-up. To prevent these losses, multiplexed technologies for STIs (immunochromatographic tests/devices/assays and molecular assays that can screen multiple pathogens or multiple strains of one STI) can yield same-day results in a single visit. Research evidence of patient-centred (preference, satisfaction) and clinical health outcomes (feasibility, case positivity, uptake, impact) has not been synthesised. We conducted a systematic review to fill this gap.
Methods For the period 2009–2020, two independent reviewers searched PubMed and Embase, retrieved 4440 citations and abstracted data from 42 relevant studies.
Results Of 42 studies, 10 (23.8%) evaluated multiplexed immunochromatographic and 32 (76.2%) molecular assays. Outcomes were reported as follows: preference (n=3), satisfaction (n=2), uptake (n=1), feasibility (n=2), case positivity (n=42) and impact (n=11). Screened populations included various at-risk groups. A majority (86.1%–92.4%) of participants preferred (60.2%–97.2%) multiplexed technologies (over conventional testing). Compared with conventional lab-based testing, test uptake improved by 99.4% (hepatitis C), 99.6% (Trichomonas vaginalis), 78.6% (hepatitis B) and 42.0% (HIV). Varying case positivities were documented depending on populations screened: HIV (1.8%–29.3%), hepatitis B (1.1%–23.9%), hepatitis C (0.5%–42.2%), Chlamydia trachomatis (2.8%–30.2%), Neisseria gonorrhoeae (0.0%–30.3%) and T. vaginalis (0.0%–32.7%). Regarding impact, 70.0%–100.0% of screened participants were linked to care, with result turnaround times ranging from 14 min (immunochromatographic assays) to 300 min (molecular assays).
Conclusions Compared with conventional lab-based testing, rapid multiplexed technologies were preferred by testees and led to quicker turnaround times for many STIs yielding same-day results thereby allowing to initiate rapid linkages to care. They were further shown to be highly feasible and impactful for detection and treatment facilitation. Based on these promising results, multiplexed technologies offer potential to screen at-risk populations to reduce onward STI transmission worldwide.
- diagnostics and tools
- systematic review
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
A majority of sexually transmitted infections (STIs) are asymptomatic and if left undetected and untreated, they can lead to long-term health complications.
Multiplexed technologies include both immunochromatographic tests and molecular assays.
What are the new findings?
Multiplexed technologies were preferred by participants, operationally feasible, impacted detection and treatment of various STIs with same-day results and rapid linkages to care.
What do the new findings imply?
Immunochromatographic and molecular assays are able to address gaps in the care cascade for screening and treating STIs.
Our consolidation of research evidence on outcomes that are patient-centred and that can support implementation will aid a variety of stakeholders including healthcare professionals and policymakers.
Introduction
Diagnosing, treating and managing sexually transmitted infections (STIs) represent key pillars to reduce STI transmission and significant morbidity, and thus represent crucial targets across the spectrum of STI management. Approximately 1 million curable STIs are acquired globally each day leading to on average 376 million STIs being acquired annually worldwide, primarily in resource-limited settings.1 While a vast majority of these infections are asymptomatic, when left untreated, they can cause lifelong and often serious complications. Evidence from epidemiological studies has shown that commonly occurring STIs such as chlamydia, gonorrhoea and syphilis increase transmission of HIV. Moreover, behaviours associated with acquiring HIV infection increase the risk of acquiring additional STIs and of worsening severity among those with existing infections.2
STIs are conventionally diagnosed and confirmed using laboratory-based tests, considered the reference (gold standard) on account of their high diagnostic accuracy.3 4 However, they include culture, often entail multiple patient visits due to the longer turnaround time to test results (at minimum two visits: to collect samples and to communicate test results to individuals), and sample transportation; collectively, these multiple requirements associated with lab-based testing precipitate inaction and consequent losses to follow-up.4 5 Furthermore, they often require substantial laboratory infrastructure used by trained laboratory personnel making them difficult to carry out in remote settings. This puts rural communities with high rates of STI transmission at risk.6–8 With a rise in the global prevalence of STIs, a shift towards efficient technologies such as multiplexed technologies is needed to enable healthcare providers to screen several STIs both rapidly and accurately and return the result to the patient often in one visit.
Multiplexed rapid screening technologies are of two types primarily: (a) antibody-based immunochromatographic tests/assays/handheld devices and (b) molecular tests/assays. Multiplexed technologies also meet the needs and preferences of testees, primarily by reducing the number of clinic visits, with incumbent time and cost savings. As a result, multiplexed rapid testing, if integrated into routine testing, can optimise treatment linkages thereby minimising losses to follow-up and patient anxiety associated with conventional STI testing.9
While a number of published STI-related reviews have described technologies and their use both in clinical and field settings worldwide,10–12 a systematic review of evidence to support implementation (ie, impact, uptake, feasibility) and to collect end users’ preferences beyond diagnostic accuracy has not been synthesised. With a view to plug the knowledge gap, we conducted a systematic review. Diagnostic accuracy outcomes (sensitivity, specificity) have been separately synthesised and are being peer reviewed.13
Methods
Search strategy and study selection
We followed Preferred Reporting Items for Systematic Reviews and Meta-Analyses (http://www.prisma-statement.org/). We registered the protocol with The International Prospective Register of Systematic Reviews (registration number: CRD4202179218).14
For the period 1 January 2009–20 April 2020, two independent reviewers (FN and AK) searched two electronic databases, PubMed and Embase, to retrieve relevant primary articles and conference abstracts. In addition, we searched bibliographies of included studies. We included abstracts only if full-text articles were unavailable.
Our objective was to consolidate evidence on clinical outcomes pertaining to multiplexed technologies, including immunochromatographic point-of-care devices and molecular assays used to screen populations for various bacterial, viral and parasitic STIs. FN and AK independently reviewed all citations to achieve a final subset of studies for inclusion (figure 1). Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of our research.
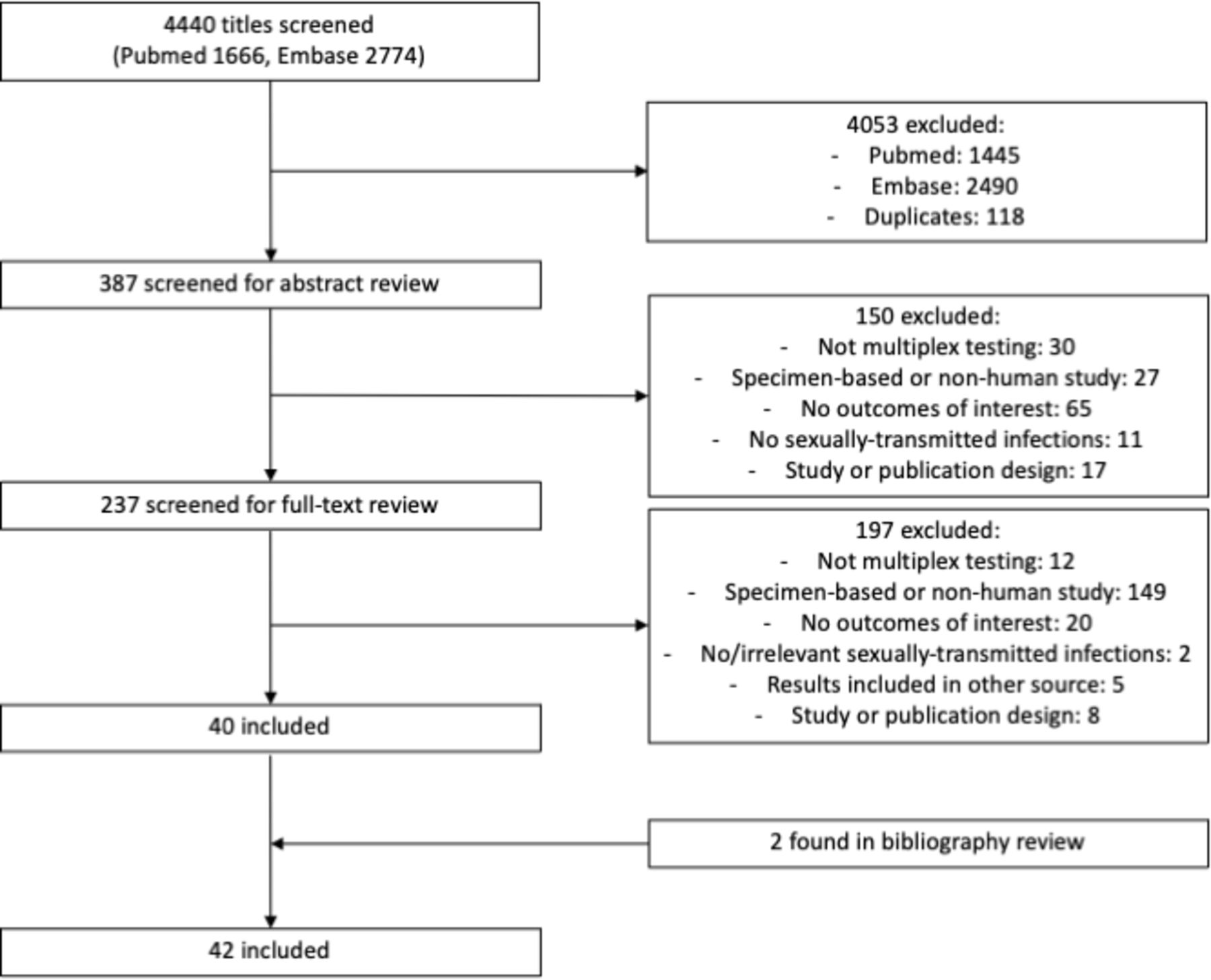
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart.
Search string
Our search string included multiplex*, duplex*, triplex*, quadruplex*, simultaneous*, point-of-care, rapid, platform, molecular, sexually transmitted infection*, sexually transmitted disease*, human immunodeficiency virus, acquired immunodeficiency syndrome, chlamydia, gonorrh*, hepatitis, syphilis, Treponema pallidum, human papillomavirus, herpes simplex and trichomonas.
Eligibility criteria
Studies that were included for review consisted of full-text primary articles or abstracts that assessed rapid multiplexed technologies where multiplexed was defined as testing for more than one STI or more than one strain of the same STI. Reviews, reports, editorials, commentaries and studies that used precollected specimens (not for the purposes of STI testing) or studies not based on human subjects were excluded (figure 1).
Outcomes
Four outcomes were analysed: impact, feasibility and preference, and the number of positive cases for each STI.
The impact of multiplexed technologies included their ability to detect new infections, turnaround times to test results and linkages to care. A change in uptake was also used to assess impact; this was defined as the increase in STI testing once multiplexed rapid testing was made available and quantified by calculating the absolute difference between the percentage of test usage from baseline, that is, conventional lab-based testing, to follow-up, that is, multiplexed rapid testing.
Testee preference was assessed in one of several ways, depending on the manner reported in each article: (1) participants’ preference to undergo multiplexed testing using a rapid test (immunochromatographic or molecular assay) over conventional testing; (2) participants’ satisfaction or acceptance of multiplexed technologies; and (3) participants’ willingness to recommend multiplexed testing to others. Preference outcomes were quantified by dividing the number of participants who indicated preference of rapid multiplexed testing by the total number of participants who were surveyed. Feasibility was quantified by metrics such as completion rate of the multiplex rapid testing strategy.
Finally, we aimed to identify the case positivity of the specific STIs based on the positive test results generated by multiplexed technologies. The number of positive STI cases was ascertained by determining the number of laboratory-confirmed positive cases divided by the total number of participants tested for the specific STI. When available, the positive (PPV) or negative (NPV) predictive value of each index test used to ascertain STI positivity was recorded or calculated.
Data abstraction
The data abstraction was performed independently by two reviewers (FN and AK). Abstraction items were tabulated in a data abstraction form and included general study characteristics, participant information, types of index and reference tests, diagnostic accuracy and the above-stated four outcomes.
Quality assurance
The quality of included studies was assessed using a revised tool for the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) by the two reviewers (FN and AK).15
Results
As shown in figure 1, we reviewed a total of 4440 citation titles. After deduplication and our initial review of titles, we reviewed 387 abstracts. Of 387, 150 citations were excluded such that a total of 237 citations were eligible for full-text review. Of 237 citations, 197 did not meet our eligibility criteria, leading to 40 eligible publications. Two additional sources were identified from bibliography review and added to the final set, therefore a total of 42 publications were included in the final set. The reasons of exclusion as well as the counts for each are detailed in figure 1. Online supplemental table 1 provides a description (including author/year of publication; study design, setting and population; STIs and the type of diagnostic test used) of the 42 studies included.
Supplemental material
Description of included studies
Of the 42 studies included, 10 (23.8%) studies reported the use of multiplexed immunochromatographic tests, while 32 (76.2%) studies reported using multiplexed molecular assays (online supplemental table 1).
Our review includes data from high-income, middle-income and low-income countries and includes key populations at a higher risk of acquiring STIs (such as men who have sex with men (MSM), sex workers, injection drug users (IDUs) as well general STI clinic attendees).
All 42 (100.0%) studies reported on case positivity.3 5 16 17 About 11 studies reported on impact outcomes; 3 (7.1%) studies reported on preference17–19 ; 2 (4.8%) on patient satisfaction19 20; 2 (4.8%) on acceptance of multiplexed testing17 18 and 1 (2.9%) on recommending multiplexed testing19 (table 1).
Impact outcomes (detection of new infections/uptake/turnaround time/linkage to care) associated with the use of rapid multiplexed STI diagnostic devices
Impact
The impact of multiplexed technologies was defined in one of several ways including their ability to detect new infections, increase uptake and to improve turnaround times to test results and linkages to care. Impact was reported by 11 (25.6%) where 3 (6.8%) studies reported on the increased detection of new/previously undiagnosed infections as a result of multiplexed testing, 1 (2.3%) study reported the increase in multiplexed testing from baseline,21 6 (13.9%) studies reported the turnaround time to test results,22–27 and 3 (6.9%) reported on linkages to/retention in care18 21 28 (table 1).
One study reported the detection of a single new infection of syphilis and HIV using an immunochromatographic test, respectively.19 In another study, 30 new infections of hepatitis B virus (HBV) and 11 new infections of Trichomonas vaginalis (TV) were detected with immunochromatographic assays.21 Finally, one study determined that 3.2% more infections of TV were detected by a molecular assay than culture and 71.4% more infections were detected compared with wet mount29 (table 1).
Increased uptake of multiplexed testing from baseline was reported for four STIs: HIV (58.0% at baseline to 100.0% at follow-up, an overall 42.0% increase), HBV (21.0% at baseline and 100.0% at follow-up, an overall 78.6% increase), hepatitis C virus (HCV) (0.6% at baseline and 100.0% at follow-up, an overall 99.4% increase) and TV (0.4% at baseline and 100.0% at follow-up, an overall 99.6% increase).21 The turnaround time for immunochromatographic devices ranged from 15 min to 20 min, whereas for molecular assays it ranged from 14 min to 300 min.22–27 Most participants who underwent multiplexed testing were linked to care (70.0%–100.0%)18 21 28 (table 1).
Preference and feasibility
Testee preference for multiplexed testing varied from a low of 60.2% to a high of 97.2% among study participants.18 19 21 Overall, participants reported high satisfaction with being tested by multiplexed technologies (92.0%–99.5%)19 21 and high acceptance of multiplexed technologies (100.0%).18 21 With regard to recommendation, up to 99.1% of study participants would recommend multiplexed technologies to others.19
Finally, with respect to feasibility, two (4.7%) studies reported on completion rates19 21 (table 2). In terms of feasibility, among participants, completion rate of multiplexed testing procedures ranged between 86.1% and 92.4%19 21 (table 2).
Preference and feasibility outcomes associated with the use of rapid multiplexed STI diagnostic devices
Positivity (case), PPV and NPV
Varying prevalence rates of STIs were documented in studies, conducted in diverse populations; we computed PPVs and NPVs across studies and technologies (both molecular and immunochromatographic assays) in online supplemental tables 2 and 3.
The high PPVs and NPVs of both immunochromatographic tests and molecular assays support the usage of multiplexed technologies in the detection of numerous STIs whether disease prevalence is low or high in a variety of populations and settings worldwide.
For molecular assays, the ranges of PPVs and NPVs for assessing STIs were calculated or abstracted. These included: Chlamydia trachomatis (91.2%–100.0% and 98.5%–100.0%, respectively), Neisseria gonorrhoeae (NG) (50.0%–100.0% and 98.4%–100.0%, respectively), TV (37.5%–100.0% and 98.9%–100.0%, respectively), Treponema pallidum (syphilis) (100.0% and 93.3%–100.0%, respectively), herpes simplex virus (HSV)-1 (75.0%–100.0% and 12.5%−100.0%, respectively), and HSV-2 (40.0%–100.0% and 36.1%−100.0%, respectively).
Similarly, for immunochromatographic tests, the ranges of PPVs and NPVs for assessing the most commonly reported STIs were: T. pallidum (93.3%–100.0% and 86.0%–100.0%, respectively), HCV (97.1%–100.0% and 95.7%–98.2%, respectively), and HIV (94.1%–100.0% and 99.5%–100.0%, respectively).
Twenty pathogens were identified by these tests. These included: adenovirus, C. trachomatis, Gardnerella vaginalis, Haemophilus ducreyi, H. influenzae, HBV, HCV, HIV, HSV-1 and HSV-2, human papillomavirus (HPV), Mycoplasma genitalium, M. hominis, NG, N. meningitidis, Streptococcus pneumoniae, T. pallidum (syphilis), TV, Ureaplasma parvum, U. urealyticum and other Ureaplasma spp.
Across studies, the most commonly reported STIs were: C. trachomatis in 22 (51.1%) studies, NG in 21 (48.8%), TV in 11 (25.6%), HIV in 6 (13.9%), T. pallidum in 6 (13.9%), HSV-1/2 in 8 (18.6%), HBV in 3 (6.9%), and HCV in 4 (9.3%) studies, respectively.
For the more commonly reported STIs, case positivity estimates varied within populations studied: C. trachomatis (2.8%–30.2%), NG (0.3%–30.3%), TV (0.1%–32.7%), T. pallidum (syphilis) (0.9%–27.0%), HSV-1/2 (0.8%–90.2%), HCV (0.5%–42.2%), HIV (1.8%–29.9%), HBV (1.1%–23.9%), and HPV (12.3%–98.2%).
Quality assessment of included studies
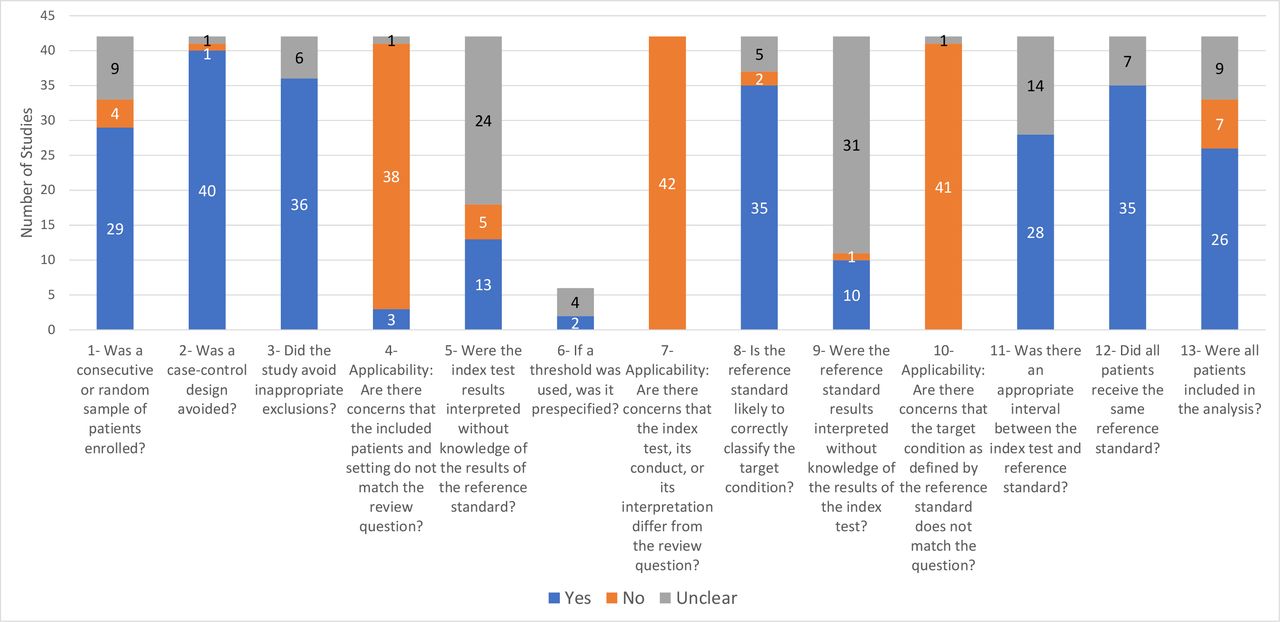
The QUADAS-2 checklist was used to evaluate quality of the included studies. In general, the majority of studies (83.7%) used appropriate reference tests to ascertain patient disease status, and most studies (60.5%) included all patients in their respective analyses. Figure 2 provides a breakdown of the included studies according to the quality checklist.
{kind=link}
{kind=link}
Quality assessment of included studies.
Discussion
Multiplexed technologies fill many gaps in the spectrum of STI diagnostic care.24 30 These technologies offer the ability to screen for many pathogens including those that do not present any clinical manifestations and those that are not commonly identified in standard STI diagnostic practices yet are able to give rise to coinfections. The test results also help catalyse the process of diagnosis and the process of seeking subsequent linkages to care. In fact, modelling studies have shown that immunochromatographic tests with adequate sensitivity can reduce prevalence of disease in communities where it is otherwise high.22 Particularly now, during the COVID-19 pandemic, rapid testing is more relevant than ever and would offer several benefits, such as to destigmatise testing, whether related to STI or COVID-19 testing, and to expedite turnaround time for both types of pathogens. Certain multiplexed test devices are now available that can test for both COVID-19 and STIs, such as Cepheid’s GeneXpert.31 32 The ability to conduct simultaneous testing of various pathogens presents as an additional advantage in diagnostic evaluations.33
The evidence presented herein suggests that over the past decade, multiplexed technologies are increasingly being developed and used to address the burden of the most common viral, bacterial and parasitic STIs in both high-income and low-income countries. While we found high feasibility of execution of multiplexed rapid testing (86.1%–92.4%),4 19 21 the uptake of these technologies for less commonly screened STI was very high: HBV (79.0%), HCV (99.4%) and TV (99.6%). The high PPVs and NPVs of both immunochromatographic and molecular assays support the usage of multiplexed technologies in the detection of numerous STIs whether disease prevalence is low or high in a variety of populations and settings worldwide. Unsurprisingly, with respect to case positivity and new cases detected with these multiplexed technologies, we found that the highest rates were reported for asymptomatic C. trachomatis, NG, T. pallidum and TV.16 34–36 Our findings suggest that asymptomatic STIs may be left undetected and untreated thereby emphasising the need for routine STI screening for at-risk populations, including MSM, IDUs, sex workers and transgender populations residing in endemic settings. Given their high feasibility and rapid turnaround time, multiplexed technologies have the potential to accelerate the screening and treatment process of these key populations and other asymptomatic individuals.37 These results further support implementation of multiplexed rapid tests in clinical care, particularly as 41 out of the 42 studies included in our final set were observational in nature and therefore alluded to real-world implementation of these test devices.
We also found evidence in favour of rapid turnaround time, and that multiplexed rapid testing was preferred by participants over conventional lab-based testing (60.2%–97.2%). Published findings corroborate these results; Rompalo et al and Widdice et al reported that patients are in favour of rapid and user-friendly diagnostic tests.12 38 With respect to HIV, multiplexed technologies addressed various barriers to testing including having to wait for test results.39 Long wait times can induce feelings of prolonged anxiety and fear among test seekers thereby discouraging individuals from seeking testing.
As the turnaround times ranged between 15 and 20 min for immunochromatographic devices and between 14 min and 5 hours for molecular assay-based testing, rapid tests have the potential to eliminate the time barrier in getting tested for STIs by yielding same-day results. While a 5-hour turnaround time for a molecular assay may be considered a lengthy period to receive test results, it nonetheless obviates the need for additional patient visits, therefore facilitating the testing and linkage to care process for individuals with limited healthcare access, such as those residing in rural areas.
Additional published findings further support the feasibility and usefulness of rapid testing into clinical care. For instance, in a qualitative research study, Fuller et al concluded that patients and clinicians across six sexual health clinics in the UK expressed their acceptance in regard to point-of-care testing, particularly if information is provided prior to testing regarding the changes they may expect in services rendered.40 Furthermore, Harding-Esch et al demonstrated the high feasibility associated with a ‘sample first’ clinical pathway where patients provided samples on arrival at a London sexual health clinic, subsequently to be tested in the point of care. Their findings illustrated that over 90% of patients reported high satisfaction with the evaluated strategy, and that all results were available prior to patients leaving the clinic which led to high linkage to treatment rates.41
Despite the benefits associated with rapid multiplex testing, we must however acknowledge that certain devices are not fully optimisable at the point of care. While the design of handheld immunochromatographic tests fully support point-of-care usage, the majority of molecular tests are conducive for laboratory testing. The sole molecular assay recommended for use near testees is the Cepheid GeneXpert.22 42–45
Strengths and limitations
We were unable to conduct a meta-analysis due to the heterogeneity of settings, populations and pathogens screened and outcomes that could not be pooled due to the lack of data in clinically relevant subgroups defined by pathogens, populations and technologies. This limitation needs to be addressed in future research. Moreover, the wide range of pathogens evaluated across studies present as a limitation and as a strength. A number of studies assessed STIs that are not generally included in STI testing guidelines such as various Mycoplasma and Ureaplasma spp. As a result, these infections were omitted from analysis as they demonstrate limited clinical utility. Also, while our review focused on the preference, case positivity, uptake, feasibility and impact of multiplexed rapid testing, the examination of these devices to detect antimicrobial resistance may be warranted, in particular with respect to gonorrhoea testing.
Study limitations, as identified by the study authors, included variability in disease prevalence in the settings and populations screened that led to limited case finding.19 26 46–48 Convenience sampling potentially introduced biases (namely, volunteer, selection and/or confounding),19 21 49 and missing data generated potential for information bias.50 Technological challenges were reported in regard to the multiplexed devices. For instance, the simultaneous molecular amplification performed by STDFinder used by Muvunyi et al reduced the device’s capability to amplify and detect singleton targets.51 Molecular assays reported PCR drift.52 Moreover, skilled healthcare staff were required to perform testing with molecular assays and venous blood was required for confirmatory tests.19 27 29 46
Implications
Several important implications of timely screening ensue as a result of ascertaining disease status early: the mitigation of transmission of disease and disease-specific complications, such as chronic pelvic pain, ectopic pregnancies, stillbirths, infertility, hepatic failure or cirrhosis.19 53 These time savings allow people who test positive to immediately be linked to counselling and care, as evidenced by the 70.0%–100.0% of tested patients in three identified studies being linked to care after multiplexed rapid testing.18 21 28 An additional benefit of using these tests is the non-invasive nature of specimen collection, such as blood samples. While our findings support the numerous clinical benefits associated with rapid multiplexed devices in STI management, the importance of conventional lab-based testing should not be overlooked to confirm preliminary positive test results as these still constitute the gold standard of testing to diagnose STIs.
Our systematic review findings add value to the current body of literature as it consolidates data relevant for healthcare professionals, policymakers, decision makers, and government officials, academics and researchers to make decisions on an offer of multiplexed testing to meet the needs of integrated testing agenda of public health organisations.
Conclusion
With the issues related to routine STI testing, particularly the high rates of loss to follow-up and the lengthy turnaround time to test results, multiplexed rapid testing (both immunochromatographic and molecular assays) offer the potential to fill many early and timely screening gaps in the spectrum of care.
We conclude that both multiplexed technologies were found to be feasible and preferred by participants, impacted detection and treatment of many STIs, with provision of same-day test results and rapid linkages to care. Given the increasing incidence of STIs worldwide, multiplexed technologies can safely be the future of integrated screening initiatives for STI diagnosis and treatment worldwide. Based on these findings, we recommend the incorporation of multiplex rapid tests into clinical care, whether they may be in the form of immunochromatographic or molecular assays. Testees’ high satisfaction of multiplexed rapid testing as well as the added benefit and impact support their usage in the spectrum of STI diagnostic care, particularly to complement conventional lab-based testing which may at times present as a suboptimal testing approach to reach vulnerable at-risk populations.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Acknowledgments
The reviewers (FN and AK) acknowledge the support of Ms Genevieve Gore, librarian at McGill University, for her help in conducting the literature search.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @nikkiannike
FN and AK contributed equally.
Contributors FN, AK and NP designed, drafted and reviewed the initial manuscript, while the remaining authors (SN, J-PR, CPY, JK) provided critique on subsequent drafts. The search strategy was developed and executed by FN, AK and NP. The quality assessment was performed by FN and AK. All authors approved and contributed to the final written manuscript.
Funding The authors acknowledge the support of the following agencies: the Canadian Institutes of Health Research grant PJT 153149 (NP), the Fonds de recherche du Québec-Santé Research-Scholar Senior Award (NP), the MUHC Foundation (NP) and the India-Canada Centre for Innovative Multidisciplinary Partnerships to Accelerate Community Transformation and Sustainability (IC-IMPACTS) (NP and SN).
Disclaimer The agencies had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.