Article Text

Abstract
Introduction The post-2005 rise in clinical trials and clinical research conducted in India was accompanied by frequent reports of unethical practices, leading to a series of regulatory changes. We conducted a systematic scoping review to obtain an overview of empirical research pertaining to the ethics of clinical trials/research in India.
Methods Our search strategy combined terms related to ethics/bioethics, informed consent, clinical trials/research and India, across nine databases, up to November 2019. Peer-reviewed research exploring ethical aspects of clinical trials/research in India with any stakeholder groups was included. We developed an evidence map, undertook a narrative synthesis and identified research gaps. A consultation exercise with stakeholders in India helped contextualise the review and identify additional research priorities.
Results Titles/Abstracts of 9699 articles were screened, full text of 282 obtained and 80 were included. Research on the ethics of clinical trials/research covered a wide range of topics, often conducted with little to no funding. Studies predominantly examined what lay (patients/public) and professional participants (eg, healthcare staff/students/faculty) know about topics such as research ethics or understand from the information given to obtain their consent for research participation. Easily accessible groups, namely ethics committee members and healthcare students were frequently researched. Research gaps included developing a better understanding of the recruitment-informed consent process, including the doctor-patient interaction, in multiple contexts and exploring issues of equity and justice in clinical trials/research.
Conclusion The review demonstrates that while a wide range of topics have been studied in India, the focus is largely on assessing knowledge levels across different population groups. This is a useful starting point, but fundamental questions remain unanswered about informed consent processes and broader issues of inequity that pervade the clinical trials/research landscape. A priority-setting exercise and appropriate funding mechanisms to support researchers in India would help improve the clinical trials/research ecosystem.
- systematic review
Data availability statement
All analysed data relevant to this study are included in the manuscript or uploaded as supplementary information. The dataset on which this work is based consists of articles already available within the published literature.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
The increase in the number of clinical trials and clinical research conducted in India after 2005 was accompanied by many reports of ethical misconduct, with bioethics reports and health activism prompting a series of regulatory changes by the government.
While there was a corresponding increase in empirical research on various ethical aspects of clinical trials/research in India, little was known about the scope of this research or what areas of research required further attention to improve the clinical trials/research ecosystem.
What are the new findings?
Research on ethical aspects of clinical trials/research in India was often carried out with limited to no funding, covered a wide range of topics but with a focus on knowledge assessments of lay and professional groups on topics such as research ethics, and leaned on easily accessible groups such as ethics committee members and healthcare students for study populations.
A range of research gaps were identified, facilitated by a consultation exercise with key stakeholders from India, and included developing a better understanding of the different components of the recruitment and informed consent process, such as the doctor-patient interaction, developing models of informed consent specific to the Indian context and exploring issues such as equity and justice within the context of clinical trials/research.
What do the new findings imply?
There is a need to move from knowledge assessments towards addressing other fundamental questions about recruitment, informed consent, equity and justice.
The large number of research gaps identified warrants a locally led priority-setting exercise as well as appropriate funding mechanisms to support researchers in India to undertake clinical trials/research methodology and ethics-related research.
Introduction
International clinical trials recruit participants from low-income and middle-income countries (LMICs) for economic, pragmatic and scientific reasons.1 Post-2005, when the World Trade Organisation-Trade Related Intellectual Property Rights agreement became fully binding for India, the number of clinical trials approved by the Indian government’s regulatory authority, Central Drugs Standard Control Organisation, began to increase,2 peaking in 2010 followed by a sharp decline to 20133 (online supplemental file 1). An identical pattern of growth and contraction was observed in India’s clinical trial sector’s growth rate, in research using clinicaltrials.gov data.4
Supplemental material
The downward trend is attributed to the chain of events that began with unacceptable ethical practices, such as failure to obtain participants’ informed consent for trial participation,5 being reported nationally and internationally.6–11 In 2013, the Supreme Court of India intervened and briefly halted approvals for new clinical trials12 in response to concerns for participant autonomy and safety, and public interest litigations from non-governmental organisations.13 14 New regulations were introduced in 2013 as amendments to Schedule Y of the Drugs and Cosmetics Rules 1945,15 mandating measures such as registration of ethics committees16 and audio-visual (AV) recordings of the informed consent discussion,17 18 the latter being a requirement that is unique to India (see Gogtay et al18 for an overview of regulatory changes/requirements in India from 2005 to 2016). Also specific to India is that the term ‘clinical trial’ is limited to the study of ‘new drugs’ only, with Biomedical and Health Research (BMHR) referring to all other basic, applied, operational and clinical research19 (in contrast to broader definitions of ‘clinical trial’, which include medical, surgical and behavioural interventional research).20 21 The most recent regulatory changes outlined in the New Drugs and Clinical Trial (NDCT) Rules of 201919 22 bring non-drug-related research (ie, BMHR) within the regulatory ambit for the first time19 23 (previously, regulatory mechanisms in India were principally focused on ‘new drug’ research). The NDCT Rules19 also separate the ethics and governance processes for clinical trials and bioavailability/bioequivalence studies from those for BMHR studies. For instance, two different types of ethics committees, each with separate authorities responsible for their registration and monitoring, will approve the two groups of studies. It is also now mandatory for BMHR ethics committees and academic clinical trials to adhere to the Indian Council for Medical Research’s National Ethical Guidelines for Biomedical and Health Research Involving Human Participants.24 25
Given this backdrop, there is a large body of theoretical bioethics literature and commentary by researchers, advocacy groups and bioethicists, covering topics such as lessons learnt from conducting clinical trials,26–28 ‘standard care’ in clinical trials,29 30 structure of the clinical trial industry,31 informed consent placed within the wider socioeconomic context,32 role of ethics committees33 and ensuring appropriate compensation mechanisms.34 There has also been a corresponding increase in empirical research on the ethics of clinical trials specifically and clinical research more broadly (henceforth clinical trials/research) in India, which has not been comprehensively reviewed. We therefore sought to summarise this body of research evidence through a systematic scoping review and narrative synthesis to help identify research gaps.
Methods
We undertook a systematic scoping review following the established six-step framework by Arksey and O’Malley,35 drawing from recommendations to enhance the methodology36–38 and adhering to the Preferred Reporting Items for Systematic Reviews and Meta-analysis extension for scoping reviews39 (online supplemental file 2).
Supplemental material
An initial systematic review of clinical trial informed consent interventions in India (PROSPERO registration: CRD42017068966) was amended to a systematic ‘scoping’ review (not within PROSPERO’s remit, hence withdrawn) of research on the ethics of clinical trials/research in India, as the latter method is particularly useful when the aim is to map the evidence base in a broad but complex unreviewed area.35 37 38
Identifying the research question
We sought to obtain an overview of the empirical evidence in relation to the ethics of conducting clinical trials/research in India. More specifically, we aimed:
to map the empirical research undertaken on any ethical aspect of conducting clinical trials/research in India;
to synthesise the key themes from this evidence base, with a focus on informed consent;
to identify gaps to inform future research priorities.
Identifying relevant studies
Inclusion criteria
The research questions were assessed in relation to the setting, population, phenomenon of interest and the study design of articles (online supplemental file 3). We included articles that reported (a) on original research in a peer-reviewed journal, (b) on India as a country for data collection (if study involved many countries, included if India-specific findings could be differentiated), (c) on ethical issues in relation to clinical trials/research and (d) with any key stakeholder groups—lay (public; clinical trials/research participants; patients/guardians), professional (healthcare/research faculty, students or practitioners; ethics committee members; regulatory/governmental agencies) or documents (informed consent forms; ethics applications).
Supplemental material
Exclusion criteria
We excluded commentaries, ‘lessons learnt’ articles, abstracts, letters, audits (eg, Clinical Trials Registry-India audits,40 41 except when linked to an ethical issue), and studies from countries other than India (eg, studies exploring views of researchers from high-income countries undertaking research in LMICs).42 43 We excluded studies on the following topics:
Willingness to participate (WTP) in clinical trials/research and recruitment-focussed studies, except when they considered ethical issues (there are other systematic reviews on WTP44–46; WTP components of included studies were not considered in this review).
Informed consent/ethical issues in relation to procedures/treatment outside of clinical trials/research (eg, in routine surgery).47 48
Pharmacovigilance (PV) studies (there are systematic reviews on PV49; PV components of included studies were not considered in this review).
Other: studies on medical/healthcare/clinical ethics (ie, not in relation to clinical trials/research or research ethics) and research skills/capacity with professional groups (eg, healthcare students).50 51
No restrictions were applied based on language, age (children/adult), study design or quality of research.
Search strategy
We searched the following nine electronic bibliographic databases with no start date and up to 5 September 2017 and this was updated using the technique by Bramer and Bain52 to 12 November 2019: MEDLINE, Cochrane Library, Web of Science, Scopus, Embase, PsycINFO, Cumulative Index of Nursing and Allied Health Literature, International Bibliography of Social Sciences and Online Resource for Recruitment research in Clinical TriAls.53 Search terms relating to three domains were combined: (a) ethics, bioethics, informed consent; (b) clinical trials/research and (c) India. A comprehensive search strategy first developed on MEDLINE (SP) drew from systematic reviews on related topics,54 55 was refined by an information specialist (ARi) and adapted to the other databases (online supplemental file 4—MEDLINE search strategy). Searches included other South Asian countries to gather contextual information, but the review focused on India. We used a combination of Medical Subject Headings, text word searches and search strings using proximity indicators. We searched the reference lists of eligible research articles and ineligible key opinion/commentary pieces, and contacted authors of published conference abstracts to trace studies.
Supplemental material
Study selection
All articles identified from the databases and other sources were downloaded to EndNote-X956 and duplicates removed. Following the original search in September 2017, one reviewer (SP) screened the titles and abstracts of all articles with a 20% random sample screened independently by a second reviewer (PD). There was a high level of agreement across the two reviewers (disagreement in 3 of 1292 articles), with discrepancies discussed and resolved. Full text of all relevant articles were obtained and screened independently by at least two authors (SP with NM, JW, LR). Discordance was again resolved through group discussion among all four reviewers. Where it was unclear if an article or a particular topic should be included (eg, biobanking, data sharing), a decision was made by meeting with two content experts (ethicists JI and RH) and reviewing the articles together. For the search and screening update in November 2019, SP carried out all steps.
Charting the data: data extraction and quality assessment
A data extraction form was developed (SP) and independently applied by two reviewers (SP and ARe) on a sample of articles (n=10). The form was refined after discussion and captured the following information (SP, ARe, JPR, SS): authors, year of publication and data collection, location, study aim, topic area, population, study design/methods, participants and findings. Subsequently, further information was captured on (SP): (a) whether studies were conducted within the context of a real or hypothetical study/scenario and (b) whether they explored broad (eg, clinical trials/research, research ethics) or specific topics (eg, data sharing, compensation).
Two review authors (SP with LR, JW, PD, JPR, SS) independently assessed the quality57 of the majority of studies using the following tools: Critical Appraisal Skills Programme (CASP) checklist58 for qualitative studies; Appraisal tool for Cross-Sectional Studies (AXIS; adapted to have 14 items instead of 20)59 for quantitative studies and AXIS, CASP and a section of the Mixed Methods Appraisal Tool60 for mixed methods studies. Quality assessments were discussed to resolve discrepancies and used to summarise relevant methodological issues in the narrative synthesis.
Collating, synthesising and reporting the results
We first quantified the data in relation to the study characteristics. Next, we created an evidence map to visualise the volume of studies by topic, population group and methods. Finally, we synthesised the quantitative and qualitative findings reported in included studies, using EndNote-X956 for data management and MaxQDA-1261 for coding articles, and used narrative and thematic description to write detailed descriptive accounts. The synthesis broadly followed the categorisations in the evidence map, but looked across all included articles to provide a comprehensive account of research on a given topic.
Consultation
The consultation phase, considered optional in scoping reviews,35 took place after the synthesis, with the aim of informing the review and ensuring local priorities and context were accounted for. We approached colleagues in India who were researchers, ethicists and representatives from advocacy groups, through prior networks or because they had authored seminal empirical and/or conceptual papers (online supplemental file 5—consultation members). Consultation was carried out via virtual conferencing, email and telephone. Findings and research gaps identified through the review were discussed. Key recommendations made by stakeholders were grouped by topic and incorporated in the manuscript, tables or supplements.
Supplemental material
Patient and public involvement
No patients or members of the public were involved in this review.
Results
Description of included studies
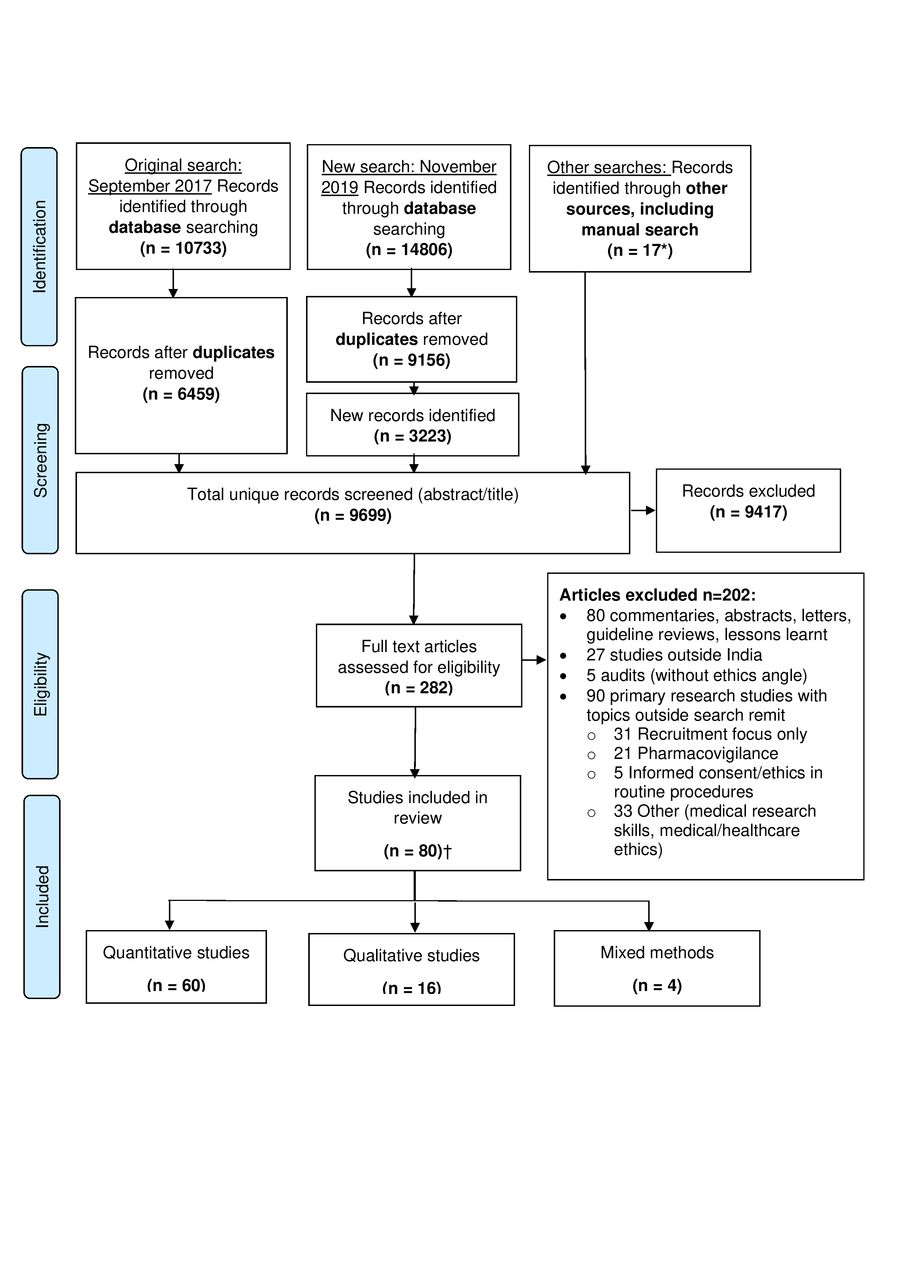
A total of 9699 unique records were identified (original, updated and manual searches), of which 282 full-text articles were assessed against the inclusion/exclusion criteria and 80 included62–141 (figure 1). Key study characteristics are summarised in table 1 (individual study details are in online supplemental file 6).
Supplemental material

{kind=link}
Preferred Reporting Items for Systematic Reviews and Meta-analysis flow diagram.160 *One study was identified through the consultation exercise. †This includes articles that reported on different aspects of the results derived from the same dataset73 92 93 107 108 or on different datasets obtained through the same grant.113 114 120 126 127 160
Key characteristics of included studies
Most studies were conducted in urban settings (47/80), in the western (24/80) and southern (21/80) parts of India. Studies were mainly quantitative (60/80), questionnaire surveys (36/60), conducted with professional groups (34/80) and appeared in journals published in India (49/80), primarily the Indian Journal of Medical Ethics142 and Perspectives in Clinical Research143 (n=15 and 16, respectively).
There were no research studies published on the ethical issues around conducting clinical trials/research until 2008, with a large proportion published a few years before and after the landmark regulatory changes of 2013 (53/80 were published 2011–2016; online supplemental file 1). Many studies did not mention the year of data collection (27/80) and of those that did, only a few were carried out in/after 2013 (17/53).
Corresponding authors of most studies were based within academic institutions (69/80; 15 outside India and 54 within India), primarily within Departments of Pharmacology of various Indian institutions (24/54). Seth Gordhandas Sunderdas Medical College and King Edward Memorial Hospital, Mumbai had the most number of corresponding authors (12/54), followed by Christian Medical College, Vellore (5/54). Two-thirds of studies (53/80) did not provide information on their funding source (26/53) or stated they did not receive any funding (27/53); of the remaining, 21 were funded/supported by international grants, 4 by intramural grants and 2 by pharmaceutical companies. There was no statement on conflicts of interest in 28 studies.
Evidence map: research on ethical aspects of conducting clinical trials/research in India
We developed an evidence map that charts the total articles included (n=80) by the main focus of the topics and population covered in the studies, alongside the methods used (table 2).
Evidence map of the number of primary and secondary research articles by topic and population group (studies explored multiple areas and have been categorised by main topic area studied)
Primary research (n=58): more than half (32/58) were studies exploring knowledge (with or without attitude and practice components) of participants on topics such as information provided to obtain informed consent (primarily with lay participants), clinical trials/research, research ethics and ethics committees (primarily with professional participants), and were mainly quantitative (27/32). Studies that assessed comprehension of the informed consent form or verbal information provision (n=10) were carried out in real (8/10) and hypothetical (2/10) randomised controlled trials (RCTs), clinical trials and cohort studies.
Another large group of primary research studies (26/58) focused on perceptions, experiences and practices/processes on topics such as the extent of patient participation in informed consent discussions, AV recording of consent processes, ethics committees, research governance (eg, data sharing) and the larger clinical trials landscape in India (such as outsourcing, contract research organisations and civil society organisations). Studies employed a wider range of methods (11 quantitative, 13 qualitative studies, 2 mixed methods) and some (9/26) were conducted in the context of a real and/or hypothetical study.
Secondary research (n=22): these studies were all quantitative and were centred around documentary reviews of the quality of application forms submitted to ethics committees, compliance of informed consent documents to guidelines/regulations, and Indian journal articles’ reporting practices on informed consent and ethical approval.
Narrative synthesis: key findings and research gaps
The findings from included studies were synthesised based on population groups (lay/professional) and key topic areas, with summaries of methodological issues where relevant. Sections A1–A6 and B1 indicated below correspond to those in table 3, which highlights the key findings from the synthesis alongside identified gaps (see online supplemental file 7 for full report of synthesis).
Supplemental material
Summary of synthesised findings and gaps
Primary research was synthesised in six key areas (A1–A6). The first four (A1–A4) covered studies that involved comprehension of the informed consent form and knowledge of clinical trials/research, research ethics and ethics committees (where attitudes and/or practices were reported, these were synthesised). Research on informed consent processes (A5) and broader cross-cutting themes that provided a more holistic understanding of the clinical trials industry (A6) were also synthesised. Secondary research (B1) was synthesised based on the type of documents scrutinised (eg, ethics application forms, informed consent documents, journal articles) and the area under investigation (eg, completeness, errors, quality; reporting practices). The number of articles tagged to a given topic includes studies where that topic was the main focus as well as those where the topic was briefly explored. Salient findings from the synthesis are presented below narratively.
Primary research
The synthesis (table 3) established that, despite the focus on knowledge-based studies evident in the evidence map (table 2), it was difficult to build a coherent picture of lay and professional participants’ understanding of the topics explored (written/verbal information provision, clinical trials/research, research ethics, ethics committees), primarily due to the methodological (eg, validity of survey instruments) and reporting limitations in studies (A1–A4). Methodological research aimed at developing locally validated tools to assess knowledge will help improve the quality of future studies and facilitate meta-analysis.
Ethics committees (A4) were among the most studied topics (18 studies) and also the source of data in a large volume of studies (16 studies, 8 each with committee members and documents submitted to/produced by committees). Studies highlighted a number of challenges faced by ethics committees73 92 101 102 108 121 130 (eg, conflicts of interest, onerous workload, impact of frequent regulatory changes without support for implementation), which would benefit from the development of interventions to support the optimal functioning of ethics committees. Healthcare students were the next most researched group (10 studies).
Research on interventions to optimise comprehension of written/verbal information provision for informed consent (A1) were particularly lacking (except one RCT that compared group and individual counselling and found no difference in comprehension).116 While there is some evidence of the difficulties of communicating research terminology (around terms such as research, trial, randomisation) particularly in local languages,70 112 127 research is required on interventions to overcome these barriers (A2). There was overwhelming support for education and training on clinical trials/research and research ethics in the curriculum for key stakeholder groups, including healthcare students75 81 98 131 137 but we do not know what, if any, aspects of these topics are currently covered in healthcare students’ curriculums so that deficiencies can be identified and addressed (A3).
There is some evidence in relation to the ‘reported’ practice of informed consent77 126 135 138 (eg, not conducting informed consent in local languages or indication of coercion among student research participants), but limited70 83 111 140 information on the ‘actual’ practice of gaining informed consent, what research participants consider important to know or models of informed consent that are tailored to the local context (A3, A5). Where ‘actual’ practice was examined, it was illuminating—for instance, in healthy volunteer studies, informed consent appeared to be a formality and discussions were centred around payment for participation than risks to volunteers’ health.140 Future research on informed consent processes should include an in-depth exploration of the recruitment interaction with potential research participants that delves beyond the questions participants ask, towards the identification and dissemination of good practice, across multiple contexts (eg, consent/assent in trials with children; student-led trials in academic institutions). A good starting point would be to explore if it is feasible, within the current regulatory framework and following strict confidentiality requirements, to use the AV recordings of the consent process more proactively for these purposes, rather than be reviewed only when there are reports of ethical misconduct.76 Similarly, the development of core information sets that help define the essential information that participants would like to receive is warranted (A3, A5).
The small group of studies (A6; seven studies) that focused beyond the surface issues around clinical trials provided rich insights into the origins, growth and workings of the clinical trials industry, while placing the industry within the wider regulatory environment and existing health inequities. Four key cross-cutting themes were examined among these primarily qualitative studies (informed by other qualitative/quantitative studies that touched on similar areas):
Compensation (for study participation, treatment or study-related injuries) was well researched and studies highlighted the need for a nuanced consideration of compensation arrangements127 (to account for views such as free treatment being perceived as inferior/dangerous by those from lower socioeconomic groups). It also appeared that compensation determination is fraught with challenges76 103 125 140 (such as lack of uniformity in the process and incentives approved by ethics committees being overridden). Studying current practice in relation to actual compensations that have been awarded may help chart out areas of inconsistencies that can be addressed. Also, there appear to be challenges with implementing and complying with the compensation rules, which could be investigated in future studies (no studies were conducted after NDCT Rules 2019).
Data sharing was explored in a small volume of studies84 127 128 that nonetheless provide valuable insights. For instance, lay participants appeared cautious about consent for data sharing after receiving detailed information (despite readily agreeing initially)127 and some professional participants supported sharing clinically relevant and actionable results with individuals who contributed to biobanking research, but acknowledged the challenges to this process.128
Power imbalances within the clinical trials/research environment were frequently discussed by professional participants, especially members of ethics committees and civil society organisations. Imbalances of concern included the paternalistic doctor-patient relationship contributing to therapeutic misconception127 (where participants perceive unproven trial treatments to be beneficial), the lack of correlation between India’s disease burden and diseases studied,90 92 the equation between paid healthy volunteers (exploited due to their lower socioeconomic status) and contract research organisations (with whom the volunteers have bargaining power),140 capacity building that does not foster local innovation114 115 and the hierarchy between medical and non-medical experts in ethics committees.92 108 133 Some of these concerns would benefit from empirical investigation—for instance, studying the doctor-patient interaction in trial recruitment can help delineate the components of communication that contribute to therapeutic misconception. Similarly, research, particularly qualitative, that further explores issues of equity and justice in relation to clinical trial recruitment processes is warranted. Research on patient and public involvement in clinical trials is conspicuous by its absence and should be prioritised to redress some of the power inequities.
A small group of studies provided nuanced insights into organisations that appear to be at opposite ends of the ethical debates on clinical trials in India—contract research organisations (CROs) and civil society organisations (CSOs).114 115 Although critical of ethical malpractice in general, CRO staff were less inclined to acknowledge instances of the same in their own CROs.115 CSO representatatives were supportive of clinical trials, felt the need to move away from pitting Indian and/or public sector clinical trials against foreign and/or private sector clinical trials as good versus bad and emphasised the need to focus on wider ethical issues that delve beyond simplistic procedure-based agendas.
Secondary research
The synthesis of documentary research (B1) corroborated findings from the synthesis of primary research and reported: inadequacies in informed consent documentation, increased workload for ethics committees particularly after the 2013 regulatory changes, mismatch between clinical trials and India’s disease burden, lack of uniformity in compensation mechanisms and suboptimal clinical trial reporting practices in Indian journals.64 66 71 74 119 124 125 139 141 The use of Western readability tests for written information provided in India62 86 needs addressing with the development of readability tests in Indian languages. Similarly, while studies on journal reporting practices have focused on the reporting of ethical approval and informed consent, future studies could investigate reporting practices in relation to questionnaire surveys (given their frequent use and methodological/reporting limitations as indicated earlier).
Consultation exercise
Nine of the 10 individuals approached agreed to participate in the consultation exercise (virtual conferencing group: n=7, one meeting, 1 hour 30 min; telephone: n=1; email: n=1). The consultation group’s recommendations and actions taken were grouped into five key areas as summarised in table 4 (detailed in online supplemental file 5).
Recommendations from the consultation group and actions taken
Discussion
We carried out a scoping review and narrative synthesis of the empirical literature on ethical issues in relation to clinical trials/research in India. We developed an evidence map of 80 studies and synthesised the findings narratively, revealing a wide range of topics investigated and the gaps that exist, with key insights from the consultation group. We found that some topics and populations were more favoured than others—the literature was heavily focused on ‘knowledge’ assessments of participants from lay/professional groups on various topics; ethics committees were examined from multiple angles while also being the source of data in many studies and healthcare students were often research participants. On the other hand, studies that investigated the recruitment-informed consent process, models of informed consent tailored to the Indian context and issues such as equity and justice in the context of clinical trials/research were far fewer in number or absent.
To our knowledge, this is the first systematic scoping review that focuses on empirical research on the ethical aspects of clinical trials/research in one country. Systematic reviews on related aspects (eg, willingness to participate) have tended to combine LMICs together44 or included people living in India with those of Indian origin living in other countries.45
Our findings indicated that the volume of literature on a given topic was not associated with whether or not it allowed the development of a cohesive synthesis on the topic. We found it challenging to develop a lucid picture of some frequently researched areas such as knowledge on clinical trials/research and research ethics. Given the diversity and scale of the population in India, this could be a reflection of reality, but the numerous methodological limitations and reporting variations, particularly among questionnaire surveys, made it difficult to identify commonalities that may exist. By contrast, although only a small number of studies focused on the wider ethical issues, they provided valuable insights into the workings of the clinical trials/research industry. This may also be because the former group of studies, primarily questionnaire surveys, were likely aiming for breadth but were often compromised methodologically, while the explorations of wider ethical issues were more amenable to qualitative research and successfully provided the depth that was warranted in intense and nuanced debates.
Research gaps were identified on topics that need to be researched (when limited or missing from current literature) as well as topics that need to be ‘better’ researched (when present in literature but requiring methodological/reporting improvements). Given that questionnaire surveys (particularly those exploring knowledge) were the predominant method used, methodological research on developing and validating culturally relevant survey tools and minimum journal reporting standards for surveys would be crucial, drawing from existing guidelines.144–146 Small-scale, single-centre surveys may be useful to inform local practice, but consistent use of validated measures and standardised reporting practices are needed to contribute to national policy and practice. Calls to ensure inclusion of research ethics and clinical trials education in the curriculum of healthcare students would be bolstered if research can establish and evaluate the content of aspects that are already covered.
The direct impact of the 2013 regulatory changes on the research landscape are unclear in this review. A few studies investigated professionals’ perceptions of regulatory changes,76 89 acceptability and impact of new measures such as the AV recording of consent72 78 79 and the impact of changes on ethics committees66 106 (latter is examined in-depth in an excluded literature review147). It would have been useful to further examine the review findings through the prism of the landmark 2013 regulatory changes, but with a third of the studies not reporting the year of data collection, this was not feasible. It is also important to interpret the findings in light of the continually evolving regulatory landscape in India, with the most recent changes introduced in March 2019 (NDCT Rules).19 For instance, some studies raised concerns in relation to the conflicts of interest that compromise the independence of ethics committee members and the hierarchy between medical and non-medical (lay) members of ethics committees, stemming partly from issues such as lack of adequate training for lay members.92 108 133 With the NDCT Rules now requiring 50% of members to not be affiliated to the institution in which the committee is based and necessitating mandatory training for ethics committee members,148 future studies can investigate if this has redressed some of the concerns around the independence of ethics committees and the power imbalances within. Similarly, Indian regulations on compensation for trial-related injuries are acknowledged as comprehensive and having unique features (eg, the compensation for injuries not related to research),149 but it would be crucial to study the challenges in the implementation of these national laws on compensation.
The views expressed by some participants (and authors) of studies in this review that there was an excessive focus on the proceduralism of informed consent is conceivably true in practice and appears well documented,67 90 101 121 yet the informed consent process was grossly under-researched. Given the breaches of good practice reported in the past and the routine AV recording of the informed consent interaction, it is notable that only one study83 was conducted using this resource. It is unclear if the challenges in undertaking, storing and retrieving AV recordings150 151 has a role in their underutilisation for research purposes or if this is due to regulatory restrictions. Opening the black box of the informed consent process in future qualitative research can help optimise comprehension of participants, communication of complex trial-related terminology in local languages and identify aspects of the doctor-patient interaction that contribute towards therapeutic misconception.
Given the lack of established benchmarks for what constitutes optimal information provision for potential clinical trial participants in India or in the West,152 researchers could also establish core information sets (information of core importance to convey to patients, drawing from empirical evidence and consensus building approaches.153 Patient and public involvement would need to be a central component in such efforts. Interventions to identify informed consent models that are suited to the Indian context (community-family based and/or Western-individual autonomy based) and to specific situations (eg, industry-led and investigator-led trials) are warranted.
It would also be useful to critically consider the topics, populations and methods that we, as researchers, choose to investigate and employ in future studies—for instance, (a) whether the ease of access to healthcare students and ethics committee members and/or its documentation justifies them being frequently researched, especially when they are so unrepresentative of participants in trials or (b) whether assessing comprehension of informed consent information is meaningful without assessing the quality of written and/or verbal information provision that preceeded it. Future research could also address the lack of readability tests in Indian languages, develop interventions to improve ethics committee functioning by overcoming some of the identified barriers and curtail the excessive focus on ‘knowledge’ to redirect efforts on the larger ethical issues to tackle the inequities and imbalances in the clinical trial industry.90 92 105 112 114 115 121 127 128 However, if knowledge assessments were to be undertaken, it would be prudent to consider what constitutes optimal understanding among research participants152 and whether the outcome of any knowledge assessments can be used to improve the informed consent process or the comprehension of participants locally. The suitability of interventions employed in high-income countries to improve participant understanding in informed consent for research154 155 needs to be carefully assessed for India. Qualitative research methods, underused in the range of topics covered in this review, are best suited to investigate the larger issues that require depth of understanding rather than breadth.
The consultation exercise with key stakeholders in India was instrumental in contextualising this scoping review and identifying missed research priorities. A key structural constraint identified in the consultation exercise and evident in the dataset was that most studies were conducted with no to limited external funding. Calling for high-quality studies that span a range of topics to fill the identified gaps would be misguided without appropriate funding mechanisms. Initiatives such as the Medical Research Council’s trials methodology hubs across the UK have been instrumental in improving clinical trial design, conduct and reporting (eg, see final report of trials methodology research carried out over 4 years, 2014–2018, in one of the hubs156), with subsequent provisions for initiating trials methodology projects in LMICs.157 It is time for international/national funding agencies to consider establishing similar methodology hubs led by researchers in India, with a focus on the ethical conduct of clinical trials. It would be important, however, to ensure that in our pursuit of empirical evidence, we do not downplay the vital role played by other forms of evidence and catalysts for change, given that not all ethical issues are amenable to being researched.
Limitations
Despite our best efforts, we may have missed some relevant journal articles and studies included in books. However, if missed articles reflected the patterns of published research included in this review, it is likely that they would not substantially alter our synthesis and conclusions. A decision to only include peer-reviewed research also meant we did not seek out grey/unpublished literature158 159 (although condensed publications from them, if any, are included103). Some of the topics we excluded may have helped contexualise our findings. For instance, we included studies on research ethics but excluded those on medical/clinical ethics—an associated topic of interest that requires a separate review.
While the review has helped underline the gaps in the existing literature, it is not exhaustive and cannot claim to have identified all gaps. It also cannot prioritise the identified gaps in a meaningful way and is limited in identifying key topics that are completely absent or of importance to key stakeholders. Designing and conducting the review with the input of researchers in India from conception stages may have resulted in a different focus and outcome. Our intention was that the critical input of key stakeholders at the consultation phase helped focus the review and overcome some of the shortcomings. A locally led priority-setting exercise, informed by this review, to determine pressing concerns that warrant empirical investigation would be an ideal next step.
Conclusion
This systematic scoping review is the first attempt at summarising peer-reviewed empirical research on topics related to the ethics of clinical trials/research in India. The review demonstrates that while a wide range of topics have been studied in India, the focus is largely on assessing knowledge levels across different population groups. This is a useful starting point, but fundamental questions remain unanswered about the recruitment and informed consent process, such as the doctor-patient interaction, and the larger issues of equity and justice that dominate the clinical trials/research landscape.
The evidence map and narrative synthesis are meant to be a starting point for discussions on future research directions, to be used in ways that benefit the research community and patient population and contribute towards the ongoing efforts within India to improve the clinical trials/research ecosystem. A priority-setting exercise that could be informed by this review, led by researchers in India, would be an ideal next step, alongside funding mechanisms that support researchers based in India to undertake research in priority areas in clinical trials/research methodology and ethics.
Data availability statement
All analysed data relevant to this study are included in the manuscript or uploaded as supplementary information. The dataset on which this work is based consists of articles already available within the published literature.
Acknowledgments
We are immensely grateful to the following individuals for taking part in the consultation exercise and providing critical input on all aspects of the review, identifying additional research priorities and contextualising the findings: Amar Jesani, Anant Bhan, Gagandeep Kang, Manjulika Vaz, Nithya Gogtay, Rashmi Rodrigues, Sarojini Nadimpally, Urmila Thatte, Vijay Gopichandran (the first two members provided further input at the journal peer-review stage). Errors and omissions, if any, are ours. We would also like to thank the two anonymous reviewers for their critical input that helped improve this manuscript.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @s_paramasivan1
Contributors The study was conceptualised and designed by SP, with contributions from PD, JMB and JLD at the protocol stage. SP and ARi developed and applied the search strategy. SP and PD carried out the initial title/abstract screening. SP, JW, LR and NM equally contributed to the full-text screening. JI and RH provided content expertise and reviewed studies where a decision could not be made on inclusion; PD provided methodological expertise. SP, PD, JW, LR, JPR and SS carried out the quality assessments. SP, ARe, JPR and SS extracted the data. SP wrote the first draft of the manuscript and reviewed it based on initial feedback from JLD and PD, followed by all other authors. SP conducted the consultation exercise and incorporated suggestions, with further input from JD. All authors contributed intellectual content, edited the manuscript and approved the final manuscript for submission.
Funding This study was funded in part by the MRC ConDuCT-II (Medical Research Council, Collaboration and innovation for Difficult and Complex randomised controlled Trials In Invasive procedures) Hub for Trials Methodology Research (MR/K025643/1) and support from the Royal College of Surgeons of England Bristol Surgical Trials Centre. JMB, JI and RH are part funded by the National Institute for Health Research (NIHR) Bristol Biomedical Research Centre at University Hospitals Bristol and Weston NHS Foundation Trust and the University of Bristol. JLD and JMB are NIHR Senior Investigators. PD and ARi were supported by the NIHR Applied Research Collaboration West (NIHR ARC West) at University Hospitals Bristol NHS Foundation Trust.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.