Article Text

Abstract
Background The large burden of injuries falls disproportionately on low/middle-income countries (LMICs). Health system interventions improve outcomes in high-income countries. Assessing LMIC trauma systems supports their improvement. Evaluating systems using a Three Delays framework, considering barriers to seeking (Delay 1), reaching (Delay 2) and receiving care (Delay 3), has aided maternal health gains. Rapid assessments allow timely appraisal within resource and logistically constrained settings. We systematically reviewed existing literature on the assessment of LMIC trauma systems, applying the Three Delays framework and rapid assessment principles.
Methods We conducted a systematic review and narrative synthesis of articles assessing LMIC trauma systems. We searched seven databases and grey literature for studies and reports published until October 2018. Inclusion criteria were an injury care focus and assessment of at least one defined system aspect. We mapped each study to the Three Delays framework and judged its suitability for rapid assessment.
Results Of 14 677 articles identified, 111 studies and 8 documents were included. Sub-Saharan Africa was the most commonly included region (44.1%). Delay 3, either alone or in combination, was most commonly assessed (79.3%) followed by Delay 2 (46.8%) and Delay 1 (10.8%). Facility assessment was the most common method of assessment (36.0%). Only 2.7% of studies assessed all Three Delays. We judged 62.6% of study methodologies potentially suitable for rapid assessment.
Conclusions Whole health system injury research is needed as facility capacity assessments dominate. Future studies should consider novel or combined methods to study Delays 1 and 2, alongside care processes and outcomes.
- injury
- traumatology
- health systems evaluation
- health services research
- health systems
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Injuries represent a major global health burden with 90% of deaths occurring in low/middle-income countries (LMICs).
Trauma health system strengthening has improved injury outcomes in high-income settings and could avoid one-third of all trauma deaths if similar case fatality rates could be achieved in all LMICs.
The Three Delays model, widely adopted in maternal and child health research, has been advocated for assessing and strengthening emergency care systems, including following injury.
What are the new findings?
Our review found that conceptual Delay 3 (receiving quality care) was most commonly assessed (79.3%) followed by Delay 2 (reaching care, 46.8%) and Delay 1 (seeking care, 10.8%).
Facility assessment data (primarily or secondarily analysed) was the most common methodological approach overall (36.0%) and for Delay 3 specifically (44.3%), with resource availability the most common study outcome reported overall (45.9%).
For Delay 2 and Delay 1, medical case note review (25.0%) and household surveys (58.3%) were the most common methods used, respectively.
Key questions
What do the new findings imply?
Injury care health system research in LMICs has focused on Delay 3 and the healthcare facility with relatively little attention given to Delay 1, despite this being known to be an important contributor to patient care delay in other emergency conditions in LMIC settings.
To ensure equitable access to injury care, future injury health system studies in LMICs should consider combining well-established facility capacity assessment methods with others that can generate insight into Delays 1 and 2.
Introduction
Injuries are a serious global health problem. Trauma causes more deaths globally than HIV, tuberculosis and malaria combined.1 Low/middle-income countries (LMICs) bear the brunt and account for 90% of these deaths.1 Non-fatal injuries also represent an enormous burden with 1 billion people sustaining an injury requiring care annually.2 Road traffic collisions (RTCs) were projected to become the third leading disease burden by 2030.3 Injury-related morbidity and mortality varies globally, partly attributable to differences in health system response.2 4–7
Prevention is an important target for reducing the burden of injuries, however health system-delivered care has a major role in reducing avoidable trauma deaths.4 8 It is known that survival rates from equivalent injuries in LMICs are lower than those seen in high-income countries (HICs).4 If this gap in outcomes could be closed, one-third of trauma deaths annually could be avoided.4 Focus on the system of care following injury has led to major improvements in HICs, particularly for the most severely injured.9–11 This supports a health system focus on improving injury outcomes in LMICs. Additionally, care provided after trauma is an exemplar tracer condition useful as a marker of health system strength.12 13 Promoting essential trauma care can benefit other time-critical conditions through wider health system development and is advocated by the WHO.14 However, there remains little data on access to quality healthcare services for the injured in LMICs. This should be a priority for research.13
Health systems are complex and adaptive, with characteristics of non-linear and unpredictable responses to interventions.15 They are social institutions, influenced by human relationships and behaviours driving their performance.16 Assessing health systems is important to inform impactful health system improvement.17 There are multiple frameworks describing health systems, with origins in differing paradigms of understanding and sociopolitical backgrounds.18 Although a universal framework may not exist, health system researchers should use a framework that fits the purpose of their study.18
The Three Delays model frames barriers driving delays to care contributing to adverse outcomes, and was originally described for maternal mortality in LMICs.19 It specifically considers factors delaying care seeking (Delay 1), reaching a place of care (Delay 2) and receiving appropriate, quality care (Delay 3).19 While widely adopted across reproductive, maternal, newborn and child health settings,20–24 the Three Delays have recently been proposed and tested to evaluate emergency healthcare in LMICs, including trauma.5 6 25 26 Trauma and obstetric emergencies are common in LMICs and have similar health system requirements.27 28 Relatively few aetiologies cause maternal death and effective treatments are available.25 29 Although many mechanisms can cause injury, patient management protocols standardise initial treatment priorities, regardless of aetiology.30 31 Both are acute-onset, time-critical conditions,5 with overlapping health system response requirements including timely facility transfer,32 33 anaesthesia34 and haemorrhage control. However, they differ in funder priority,35 36 community and cultural understanding,37 38 and the demographic characteristics of affected individuals.39
In the relatively under-resourced and under-researched field of trauma systems in LMICs, identifying ways to assess trauma care systems efficiently, such as through rapid assessment, could encourage locally driven research to identify needs and monitor interventions. Rapid assessments have been described for various health-related conditions and systems for communicable and non-communicable diseases, risk-taking behaviour, humanitarian crises and patient safety.40–46 They are advocated when data are needed quickly and resource or logistical constraints mean some research techniques are impractical.41 Such assessments adopt principles of pragmatism, use of multiple data sources, speed and cost-effectiveness.42 Methodological pluralism is common44 47 and time scales for completion short—in some cases not more than 1 month,47 in others, 341 or 640 months are more typical.
To inform the development of trauma care health system assessment, we undertook a review of the existing literature on assessing LMIC trauma care health systems. The primary aim was to characterise the literature within the Three Delays framework. Secondarily we aimed to assess the potential suitability of methods identified for use within rapid health system assessments.
Methods
Search strategy and selection criteria
This review report follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.48 The study was registered with PROSPERO (CRD42018112990) and the protocol previously published.49
Search methods
The following databases were searched by a senior medical librarian from inception until 9 October 2018: Africa Wide Information (Ebsco), Cochrane (Wiley), Embase (Ovid), Global Health (Ovid), Global Index Medicus (WHO), MEDLINE (Ovid) and Web of Science (Clarivate Analytics) (online supplemental material 1). We used variations from text in titles, abstracts, keywords and subject headings to obtain articles combining the following concepts: (1) trauma and injury, (2) assessments, evaluations, benchmarking or tools, and (3) health system programmes. All languages were included. Animal studies were excluded when possible. We collated and deduplicated articles in EndNote V.X9.50 We searched the grey literature in four stages51: grey literature databases, a customised Google search, targeted websites and consultation with experts.51 We used the search terms “trauma” OR “injury” AND “assessment” OR “evaluation” AND “health system” in Core, New York Academy of Medicine Grey Literature Report, OpenGrey and WorldCat Dissertations and Theses (OCLC). We used the search terms “trauma”, “injury”, “assessment”, “evaluation” and “health system” in combinations for advanced Google searches with and without limiting the domains to .org, .edu, .int and .gov. We screened the top 50 sites per search. We also searched the organisational websites listed in online supplemental material 2 with the same terms. We reviewed reference lists of identified articles and included additional relevant literature.
Supplemental material
Eligibility criteria
We included primary quantitative, qualitative and mixed-method studies, as well as secondary literature reviews, published and unpublished, from LMICs. LMICs included low, lower middle and upper middle-income countries according to the World Bank classification at time of review.52 We excluded studies only set in HICs but included studies with both HICs and LMICs. We included grey literature reports and publications from relevant national and international health organisations. Case reports, letters and conference proceedings were excluded. Studies must have focused on trauma or injury (used interchangeably) care and assessed one or more health system aspects of care specified in table 1.
Inclusion and exclusion criteria
Identification of studies
Two reviewers (NO’D, MD) used the Rayyan QCRI online open-source web application53 to screen articles by title and then abstract. Rayyan key term screening removed any identified animal studies. We discussed disagreements until reaching consensus with third reviewer (JW) arbitration where necessary. Two reviewers (all by JW, half each by MD and NO’D) reviewed the full texts. We used Google Translate for non-English articles.54–56 One reviewer (JW) conducted each grey literature database, Google and focused website search.
Risk of bias
This review focuses on understanding the breadth of diverse research approaches used to assess trauma care health systems and we did not analyse the results of individual studies. The quality of study conduct and trustworthiness of findings was not our aim, and no risk of bias assessment was therefore performed.57
Data extraction
We developed and piloted a standardised extraction spreadsheet. We extracted the following study characteristics:
Author.
Publication year.
The number, names, income status (low, lower middle, upper middle and high) and World Bank region52 for included countries.
Urban or rural setting.
Which of the Three Delays were assessed.
Methodological approach with description.
Trauma population (all trauma, road traffic only, fractures only, burns only, eye injuries only, trauma as a subset of wider emergency pathology).
Conceptual framework, tool or guidelines used where applicable.
Indicators of care quality or quality improvement (QI).
Subjects under study (about what or whom the study reports as facility according to type (primary, secondary or tertiary), patients, healthcare workers (prehospital or facility-based), community members and other stakeholders, or referral mechanisms or patterns).
Outcome type (description of barriers and challenges, availability of resource, defined measure of care process, mortality, operative care, patient disposal or destination, length of stay or other outcome specified in free text).
What health system intervention is reported, if any.
Study cost.
Time taken for data collection.
If multiple data sources were used.
Original study author comments on pragmatism of approach.
Original study author reported strengths and limitations.
Where more than one response was appropriate, all were captured. Two authors extracted this independently (all by JW, half each by MD and NO’D) from the database search articles. Differences were discussed until agreement was reached.
Analysis of results
Given the review aims, of characterising the literature within the Three Delays framework and assessing the potential suitability of methods identified for use within rapid health system assessments, a narrative synthesis of findings was performed.58 59
Synthesis of variables extracted
With regard to the primary review aim, we mapped studies reporting health-seeking behaviour to Delay 1 and studies reporting aspects of reaching care following injury to Delay 2. We mapped studies reporting aspects of receiving formal healthcare, whether in a prehospital, primary, secondary or tertiary facility to Delay 3. Studies could be mapped to more than one delay. We understood and categorised care quality within the Donabedian framework of Structure, Process and Outcome.60 Structure includes the organisational, human and physical resources required to deliver quality care, process denotes what is actually done and outcome signifies the effect of care on health status.60
With regard to the secondary review aim, for principles of rapid assessment (pragmatism, use of multiple data sources, speed and cost-effectiveness), we recorded any data on monetary cost of studies and the time taken for study data collection in days. For retrospective studies, the available data were the time window for the dataset. We classified any study using more than one data source, whether or not they were described as mixed methods, as using multiple data sources. Pragmatic approaches to research need to be real-world problem orientated, producing stakeholder relevant results and be based on practical research philosophy.61 62 Pragmatic metrics are feasible to collect, not onerous, user friendly, easy to interpret and broadly applicable,63 providing adequate rather than perfect information.42 Based on this understanding, we recorded study features that its authors reported as being either pragmatic or non-pragmatic. We judged potential suitability or not for inclusion of study method within a rapid assessment based on rapid assessment principles following discussion between two reviewers (out of JW, NO’D, MD). Study author reported strengths and limitations were further synthesised into categorical themes by one author (JW).
Patient and public involvement
Neither patients nor the public were involved in the design, conduct, reporting or dissemination plans of this literature review.
Results
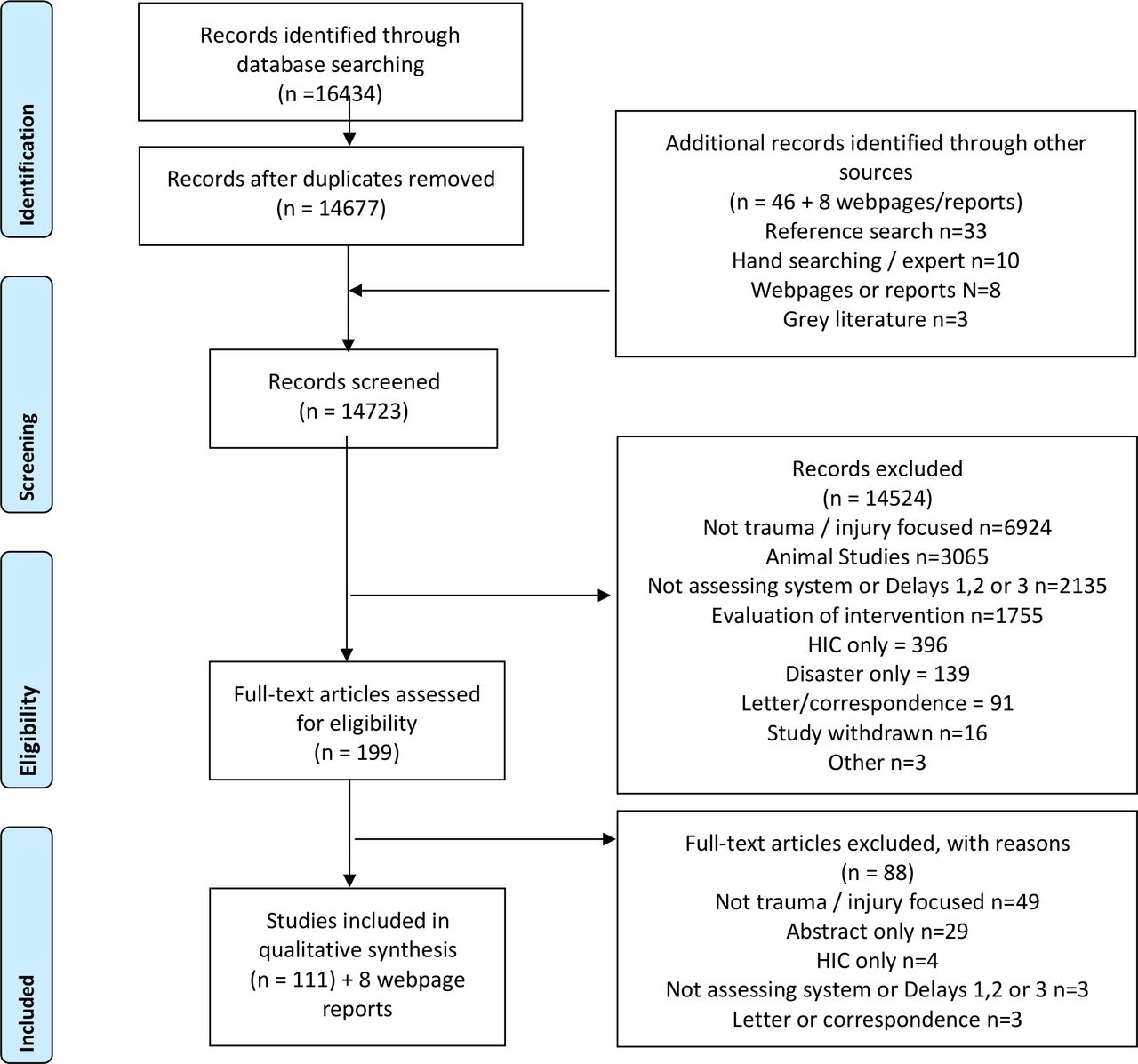
After duplicate removal, we identified 14 677 articles from the database search and 46 from other sources (figure 1). We included 111 studies and 8 relevant non-study documents or websites in the final analysis. Lower middle-income countries were most commonly included (56 of 111, 50.5%) (table 2). Studies originated across the World Bank regions although predominantly (49 of 111, 44.1%) from sub-Saharan Africa (online supplemental table 1 and figure 2) with Ghana being the most studied country (16 of 111, 14.4%). Combined urban and rural were the most common study settings (53 of 111, 47.7%).

PRISMA flow chart.48 HIC, high-income country; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study findings overview

(A) Map of studies according to World Bank regions. (B) Map of studies according to countries.
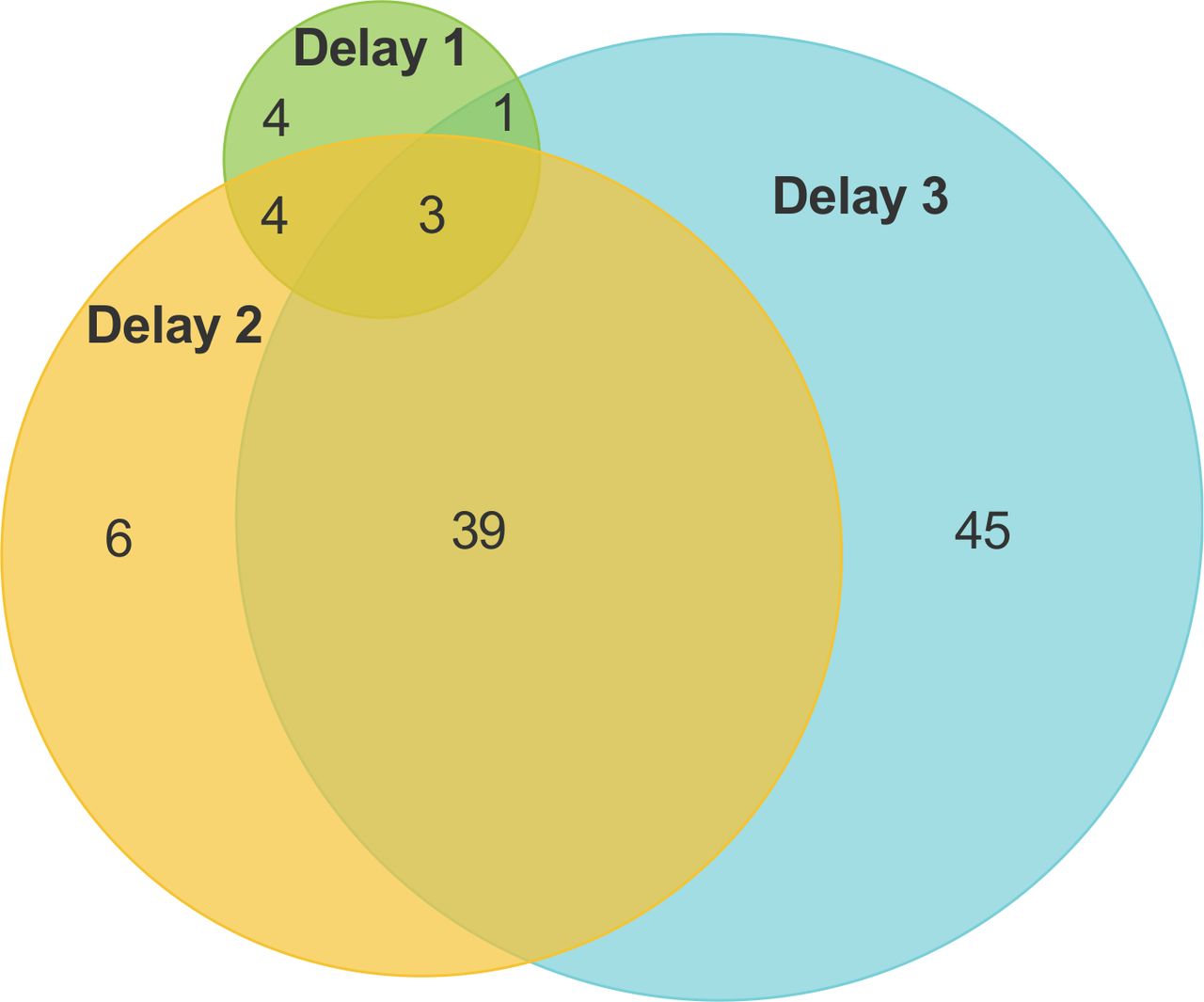
Delay 3, either alone or in combination, was the delay most commonly assessed (88 of 111, 79.3%) followed by Delay 2 (52 of 111, 46.8%) and Delay 1 (12 of 111, 10.8%) (figure 3). Most studies were mapped either solely to Delay 3 (45 of 111, 40.5%) or to both Delays 2 and 3 (39 of 111, 35.1%). Only three (2.7%) studies were mapped to all Three Delays. Studies not mapped to any of the Three Delays included four (3.6%) reporting how to assess injury care64–67 and five (4.5%) reporting evidence of QI activity rather than the quality of delivered care.68–72 Delays according to geographical region are reported in online supplemental table 1.
{kind=link}
{kind=link}
{kind=link}
Number of studies per conceptual delay.
A heterogeneous range of study methods were identified including quantitative, qualitative and mixed methodological approaches. Across all studies, the most common methodological approach was using facility assessment data, either primarily collected or secondarily analysed (40 of 111, 36.0%) (online supplemental table 2). The study methodologies most commonly mapped to each of the Delays (either alone or in combination) were household surveys for Delay 1, (7 of 12, 58.3%), medical case note review-based methods for Delay 2 (13 of 52, 25.0%), and methods using facility assessment data primarily collected or secondarily analysed (39 of 88, 44.3%) for Delay 3. Studies not assessing Three Delays most commonly included healthcare worker (HCW) surveys reporting QI activity (5 of 9, 55.6%).
The most commonly studied population encompassed all injuries and trauma, 87 (78.4%), with 13 (11.7%) studying RTCs only, and 6 (5.4%) studying fractures and orthopaedics only. Most studies incorporated a framework within the assessment (68 of 111, 61.3%), the most commonly used was the WHO Essential Trauma Care guidelines and accompanying checklist (WHO ETC) (28 of 111, 25.2%). The predominant subject of studies was facilities (84 of 111, 75.7%) followed by patients in (51 of 111, 45.9%) studies. Care quality was studied in 95 studies (85.6%), mostly through assessing structures of care (64 of 111, 57.7%), rather than care process (39 of 111, 35.1%), or care outcomes (26 of 111, 23.4%). The most common study outcome reported was availability of resources (51 of 111, 45.9%) studies.
We judged most (69 of 111, 62.2%) study methodologies potentially suitable for including within a rapid health system assessment (online supplemental table 3). The most common approaches were patient, staff or stakeholder interviews, meetings, group discussion or surveys,37 68–84 occasionally combined with care observation17 or case note review supplementation.85 Similarly common were facility assessments through survey or interview.86–111 A further 42 (37.8%) studies were thought to be unsuitable, including 20 retrospective studies relying on case note data,112–118 established registry data119–124 or a combination of both,125–131 and 8 household surveys in local languages.132–139 Both registries and household surveys were considered time-consuming and resource-intensive to conduct or maintain, with data accuracy commonly problematic with the former.
Cost was not specifically reported in any of the studies. However, some described the approach as low-cost without specifying an amount.80 140 141 Such approaches included teleconference-based case reviews, preventable death panel reviews, a mixed-method WHO ETC facility assessment and key informant interviews generating a process flow chart.
Studies reported a data collection time frame in 74 (66.7%) cases. The range of time for study data collection varied from 4 days to 12 years. Twenty-four studies using cross-sectional data collection reported data collection periods of not more than 3 months; 18 of these were mapped to Delay 3, whereas only 4 were mapped to Delay 1.
Use of multiple data sources was evident in 34 (30.6%) studies (online supplemental table 4). Facility assessments were the most common data source to be combined with others including: household surveys139; Emergency Medical Services (EMS) data83 139; Geographic Information System (GIS) analysis142 143; travel time analysis144; peer case analysis via teleconference141; Ministry of Health data108 143 145; logbook data105 106 108; administrative data143; staff interviews80 86; clinician knowledge assessment94 and desk review.107
Study authors reported various positive and negative pragmatic aspects of their studies (online supplemental table 5). Positive pragmatic aspects were categorised as leveraging available data or infrastructure to conduct their study, strategies for effective engagement of study stakeholders, and maximising methodological convenience and feasibility. Non-pragmatic aspects of studies reported were categorised as difficult practical challenges of facility-based research methods and practical challenges for study conduct across facilities or communities.
Original study authors reported various strengths to the identified studies (online supplemental table 6). These included combining data sources, in particular adding in-depth qualitative methods for deepening understanding.79 86 133 Widespread use of tools used in WHO ETC and WHO Tool for Situational Analysis to Assess Emergency and Essential Surgical Care-based assessments was seen as strengths, demonstrating their applicability and comparability across locations and countries.89 98 100 140 146 147 The inclusion of a variety of sectors, professions and patients in studies was seen by study authors as positive.67 76 78 84 88 148 149
Original study authors reported various limitations. These included lacking patient outcomes17 66 72 80 83 99 102 144 148 150 and not capturing or adjusting for injury severity.125 133–135 146 147 151 Study authors highlighted that resource availability, commonly studied, does not necessarily equate to the quality of care process or outcome.88 89 152 Authors reported that facility-orientated studies neglected community and prehospital environments,80 85 94 101 103 104 108 114 120 124 128 148 153–158 and follow-up.80 129 147 159 They highlighted that facilities had incomplete or inaccurate data,114 116 119 122 126 129 140 154 155 159–164 lacking reliable records or data systems.86 94 106 147 164 Study authors similarly highlighted that HCW views or experiences are subjective83 88 98 109 112 114 140 148 149 155 162 as are assessment tool ratings including the WHO ETC.87–89 93 95 96 100–102 105 106 143 152
Non-study literature included WHO publications or webpages (online supplemental table 7). These predominantly mapped to Delay 3 with only one to Delay 1. The WHO ETC guidelines and checklist underpinned many assessments in this review.165 166 The WHO guidelines for conducting community surveys on injury and violence167 provide methodological instruction and survey questions, but without focus on care quality, and were the basis for two surveys in this review.135 139 The WHO guidelines for trauma QI programmes propose mortality and morbidity conferences, preventable death panel review and tracking of audit filters for driving QI.168 Studies identified in this review used these guidelines to both study what QI activity undertaken as well as studies applying recommended QI practices such as preventable death panels.70 72 114 140 162 The other non-study literature identified had not been applied for health system assessment by studies in this review.14 169–171
The individual included study characteristics are reported in online supplemental tables 8 and 9.
Discussion
We found 111 studies that assess health system’s ability to provide trauma care in LMICs. Very few studies considered the whole system as understood within the Three Delays framework and there was a bias towards a sole focus on Delay 3, receiving appropriate care. Multiple heterogeneous methodologies have been used to assess trauma systems and most are potentially suitable for inclusion in a rapid health system assessment.
Given the importance of injuries as a growing global disease burden,1–3 future LMIC injury research needs to consider the whole post-injury health system. Injury care research has not been embraced by the global health and health system research communities in the same way as other conditions such as communicable disease and reproductive, maternal, neonatal and child health.1 This neglect of injury care is also reflected by only one sustainable development goal being related to trauma, focused on RTCs and primarily related to prevention.172 Although prevention is necessary, injuries will inevitably occur and warrant parallel investment in post-injury care.
We found only three studies were mapped to all Three Delays and none explicitly applied the Three Delays conceptual framework. This is problematic as 40% of mortality after trauma in LMICs may be avoidable due to factors within each of the Three Delays.6 We found very few studies focused on healthcare seeking following injury. Narrow facility-based research should be expanded to include the whole ‘surgical ecosystem’, working with a multidisciplinary team that includes health system researchers, informal providers and the community.34
Many of the studies were concentrated within a few countries. Ghana in particular, despite a burden of injury typical of sub-Saharan Africa (50.5 per 100 000),173 was relatively heavily represented. This could be explained by well-established academic collaborations publishing multiple studies in specific locations. Such author groups may have shaped the geographical findings of this review more than the injury burden. Meanwhile, few studies had investigated many countries’ trauma systems—representing an important gap for future research.
The lack of Delay 1 injury studies contrasts with the maternal health community, from which the Three Delays framework originates. Many barriers to women seeking obstetric care have been identified from sociodemographic and economic factors, community and cultural perceptions of childbirth, gender-based factors, health literacy and previous experiences in healthcare,19 38 174 which may also be relevant following injury.7 26 In maternal healthcare, recognition of barriers at Delay 1 has led to effort being directed towards avoiding harmful traditional beliefs and practices,175 such information is needed if similar efforts are to be successfully deployed after injuries. Compounding the relative paucity of studies exploring the first delay in this review is that almost all were from seven sub-Saharan African countries. This contrasts with a review of 159 studies of health-seeking behaviour in maternal and child mortality using a range of observational and qualitative methods across a broad collection of LMICs.176 Patient-based and provider-based studies which we found in this review can provide insight into why patients delay seeking care,6 74 85 but alone will not capture those who never access formal care services. Similarly identified community-based qualitative studies may be well suited to explore the breadth of possible barriers to seeking care.73 However, quantitative assessment, such as through household surveys, also reported in this review, may be needed to understand the scale and impact of identified barriers.138 Mixed-method studies with an exploratory sequential design177 (qualitative exploration to inform the development of quantitative assessment) may be suitable. Other methods such as using verbal autopsy data have been proposed,6 178 although they miss non-fatal injuries. Given the lack of research identified in this review, further study is urgently warranted to understand the importance of the first delay following injury across LMICs.
Fewer than half of the studies mapped to Delay 2. Some studies in this review used GIS analysis, focusing on geospatial accessibility, considering distance, road quality and trauma locations.179 A limitation of this method is that proximity to facilities is not equivalent to actual care access.180 Other important barriers to reaching care exist7 26 180 which could all impact on the median time from injury to facility admission, a proposed high-quality health system indicator.13 While patient-focused studies such as seen in this review help to understand the actual patient journey,74 we did not find attempts to validate GIS techniques with information from actual injured patients, as has been done for other conditions.181 182 Community-based qualitative studies, which were infrequently found in this review, may similarly be needed to understand the role of bystanders in facilitating reaching care as well as other community level barriers.73 EMS-derived data from registries, records, service inspection and staff were also identified, informing Delay 2/3-mapped studies.83 119 126 149 However, formal EMS care is not available in many LMICs and most of Africa.183 Where present, studies including EMS should include its communication and coordination including any primary facility bypass practices, known to be problematic and poorly studied.7 26 184 LMIC EMS priorities are known to differ: some function exclusively or primarily for obstetric patients,175 185–188 some focus on trauma,189 190 while some cover trauma, obstetric and medical conditions in similar proportions.32 33 Knowing and reporting this context should be part of incorporating EMS data meaningfully in future studies.
Within Delay 3, facility-based studies and assessments of resource availability predominated in this review, often using the WHO ETC. Surveys for structures of care are common across LMIC health systems research. Such data are problematic, becoming out-of-date quickly and correlating poorly to measures of delivered care quality.13 191 That said, these facility assessments can be useful, as our review has shown; they can be widely adopted, quick to complete and comparable across settings. However, when conducted alone, they are unsuitable to study Delays 1 and 2, or the process, and outcome of delivered care. Such assessments can, for example, describe the presence or absence of care protocols. But whether care delivery matches best practice, or whether staff are sufficiently trained to follow them,26 would require alternative methods, used by some studies found in this review, such as direct observation17 159 or case analysis.141 Non-technical aspects of care quality such as respectful and compassionate care, relating to HCW attitudes and motivation, require the patient perspective.192 This would similarly be required to assess patient cooperation,26 rarely studied in this review.193 Studies reporting care outcomes mostly required time-consuming database development and maintenance or case note extraction, although repurposing administrative data represents a potentially efficient alternative if available.147 To comprehensively assess Delay 3,6 7 26 combining methods and perspectives is required.
As a secondary aim, we also assessed the suitability of methodological approaches for use as a rapid assessment able to appraise systems quickly with limited resources to guide policy and practice. We will now discuss how the rapid assessment principles of pragmatism, use of multiple data sources, speed and cost-effectiveness42 were evidenced in the identified literature.
We identified several positively pragmatic characteristics of studies in our review including leveraging available data or infrastructure (such as open source maps, existing administrative or routine facility data),141 142 145 147 151 maximising methodological convenience and feasibility (such as pragmatic sampling strategies, and using established tools or criteria),74 88 89 95 96 164 194 and effectively engaging stakeholders (such as leveraging existing networks, involving key policymakers and use of electronic communication).17 67 70 78 84 109 110 150 Elsewhere in global surgical research, successful pragmatic collaborative approaches have engaged stakeholders, established networks of researchers and minimised the burden of data collection.195–197 Although currently facility-centred, they offer a potential means for future wider health system collaborative study. A negatively pragmatic characteristic, particularly for studies using medical case note review, related to practical challenges of obtaining complete data116 117 159 in a time and resource-efficient manner.114 122 Extracting high-quality data from immature data systems can be logistically difficult and health data incompleteness and inaccuracy is a problem in many LMICs.198 Although pragmatic use of routine health information is growing, it remains a small part of the overall LMIC health system evaluation literature.199 We found only some evidence of significant harnessing of technology for trauma system evaluation. While health technology availability is inversely related to health need,200 improving access to information technology is a widely recognised strategy to augment global health research capacity.201 Mobile smart phone applications for health delivery are growing, however their use in research remains in its infancy.202 Due to time, logistical and human and physical resource implications for household surveys found in this review, they were considered potentially unsuitable for rapid assessment. However, technological innovations could represent an exciting opportunity for growth in such health system research, particularly to help address some of the practical challenges in studies outside of facilities and within communities.17 111 135
Most studies in this review did not use multiple data sources, however we found innovative examples of combining data sources to deepen understanding, such as combining household surveys with focus group discussions for qualitative and quantitative insights133 and GIS analysis with facility assessment data to interpret facility resource capacity in light of population proximity.142 However, LMIC trauma system research could benefit additionally from incorporating methodological approaches from other global health fields that were not evidenced in this review. One example of a method, not found in this review, but that could be adopted to address the relative lack of care process quality assessment, are clinical vignettes, which can be used for assessing standardised clinician care quality.203–205 They are more feasible but comparable with standardised patient and case note review for patient–provider interaction assessment and are relatively inexpensive.206–208 To address the gap we identified in studying the whole health system across the Three Delays, other methodologies advocated for applying systems thinking to health research could be used.209 210 These could include process maps, graphical representation of an end-to-end description of activities, stakeholders and requirements of a process.210 211 They have been applied to LMIC health systems evaluation including emergency and surgical care.212 213 Causal loop diagrams can similarly help visualise dynamic complexity of health systems210 211 and have been used to evaluate vaccination coverage in India214 and Fijian public health food policies.215 Some of the study methodologies we found in our review could also be adapted. An example is preventable death analysis through peer review. It has advantages reported by the identified study authors of triangulating multiple perspectives, being theoretically simple, low cost140 and broadly applicable to any context.140 If data completeness140 155 162 and local expert engagement were secured,140 162 it could be better aligned toward rapid assessment.
While data collection time was often reported by studies in this review, this would not include the time for planning, ethical approval, material sourcing and analysis which are uncommonly reported. These factors should be considered when planning time frames for rapid assessments. Well-designed surveys, electronic data capture and preplanned analysis could potentially allow quicker collection.216–219 Qualitative studies across each Delay were judged potentially suitable for rapid assessment in this review.37 73–75 77 81 85 Although the data are often quick to collect, they may require lengthy transcription and analysis.220 Nevertheless, rapid assessments frequently and typically include qualitative elements45 46 and software can help.220 Trade-offs between principles could also allow some methods judged to have high resource requirements, like community-based household surveys, to be potentially accomplished quickly, within 1138 or 2 months139 if given sufficient investment.
We found no quantitative data on the monetary cost of studying trauma care systems in this review. This is unhelpful for future researchers wishing to make judgements on comparative cost-effectiveness of future methods for health system assessment or indeed subsequent interventions. Guidance for costing research in LMICs is available221 and researchers can draw on other data sources to consider cost implications for each method. However, varying costs of living, salary and consumables should be considered between settings. A facility-capacity assessment study, focused on surgery, assessed 44 district hospitals in Rwanda for US$5000.222 However, this may not be typical of health facility assessments reportedly starting at US$100 000 per national survey and often many times more.13 223
This study has several limitations. Although we extensively searched a large volume of literature, we could have missed some assessment methodologies, including any published subsequent to our search date. While our grey literature search was comprehensive, it was by a single reviewer only. However, due to the breadth of studies identified and included, we remain confident that the results adequately address the study aims. The assignment of studies into conceptual delays and suitability for rapid assessment is subjective. We have tabulated the findings to allow others to reclassify but consider this unlikely to affect overall review insights. Literature set exclusively in HICs was excluded to allow this review to be feasible. Learning from assessment methods seen in HICs only may have been missed. Some HIC frameworks such as the American College of Surgeons and Arizona guidelines have been advocated for use in LMICs.194 224 However, other authors using HIC-orientated methods questioned their applicability.225 The review also did not include time-critical or emergency care studies not specific to trauma, although we acknowledge that injuries can be studied together with wider emergency care.25 As this review excluded studies not specifically focusing on injuries, other approaches may have been missed, particularly in areas that were not well covered such as Delay 1.226 Methods in this review overlapped conceptual delays, particularly across the Delay 2 and 3 categories. Finally, we have not clearly characterised the relative amount of focus on each delay for each study, although in many cases the facility-based focus predominated. Nevertheless, researchers wishing to incorporate multiple conceptual delays into an assessment can adapt methods to capture the required data focus.
Conclusion
This study has identified literature assessing trauma care systems in LMICs, mapped them to the Three Delays framework and considered their suitability to rapidly assess a health system. Few studies considered the whole health system as understood by the Three Delays framework with assessments of facility capacity dominating the literature. More methodological approaches and data are needed to better understand the importance of delays in particular to seeking care. Most studies used methods that could potentially be applied within a rapid assessment. However, future studies should consider combining methods to generate insight into Delays 1 and 2, as well as evaluation of the quality of care processes and outcomes.
Supplemental material
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AJML and JID are joint senior authors.
Handling editor Soumyadeep Bhaumik
Twitter @maxdenning1, @drjackoids
Contributors JW, JID and AJML conceived of the project. JW, JID, AJML, DP and EG developed the study design. EG conducted the database search. JW, MD and NO'D conducted screening and data extraction. JW conducted the analysis and synthesis and wrote the first draft. All authors contributed to manuscript revisions and approve the final version.
Funding MD is supported by a graduate fellowship award from Knight-Hennessy Scholars at Stanford University. JW is a serving member of the UK Defence Medical Services.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.