Article Text

Abstract
‘Vertical’ responses focused primarily on preventing and containing COVID-19 have been implemented in countries around the world with negative consequences for other health services, people’s access to and use of them, and associated health outcomes, especially in low-income and middle-income countries (LMICs). ‘Lockdowns’ and restrictive measures, especially, have complicated service provision and access, and disrupted key supply chains. Such interventions, alongside more traditional public health measures, interact with baseline health, health system, and social and economic vulnerabilities in LMICs to compound negative impacts. This analysis, based on a rapid evidence assessment by the Social Science in Humanitarian Action Platform in mid-2020, highlights the drivers and evidence of these impacts, emphasises the additional vulnerabilities experienced by marginalised social groups, and provides insight for governments, agencies, organisations and communities to implement more proportionate, appropriate, comprehensive and socially just responses that address COVID-19 in the context of and alongside other disease burdens. In the short term, there is an urgent need to monitor and mitigate impacts of pandemic responses on health service provision, access and use, including through embedding COVID-19 response within integrated health systems approaches. These efforts should also feed into longer-term strategies to strengthen health systems, expand universal healthcare coverage and attend to the social determinants of health—commitments, both existing and new—which governments, donors and international agencies must make and be held accountable to. Crucially, affected communities must be empowered to play a central role in identifying health priorities, allocating resources, and designing and delivering services.
- health systems
- health policy
- public Health
- COVID-19
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Summary box
Pandemic responses, especially ‘lockdowns’ and associated measures (eg movement restrictions), make it difficult for people to provide and access health services, particularly in low-income and middle-income countries. Such disruptions have led to negative impacts on other areas of health, including non-communicable and infectious disease, sexual and reproductive, and newborn and children’s health, and gender-based violence.
The range of pandemic-related supply and demand-side drivers of health impacts interact with baseline vulnerabilities (eg, lack of safe and adequate housing, water and healthcare) to further exacerbate these impacts.
Social groups including women and children, the elderly, people living with disabilities, migrant workers, ethnic and religious minorities, refugees and displaced people, and people in conflict-affected settings are particularly vulnerable to broader health impacts.
Integrated health system approaches which address COVID-19 alongside other disease burdens, as well as inclusive priority setting, resource allocation, programme design, monitoring and implementation, are essential for improving response and equity.
Introduction
The COVID-19 pandemic has undermined capacity and efforts to address other health needs that are just as pressing as the virus itself, particularly in low-income and middle-income countries (LMICs). Ongoing pressure on governments to act on COVID-19 now to save ‘immediately identifiable lives’ rather than ‘statistical lives at risk’ has had and will continue to have both short-term and long-term negative consequences for health.1
This analysis, based on a longer paper produced by the Social Science in Humanitarian Action Platform,2 highlights the impacts of vertical responses to COVID-19 on health systems, services, and people’s access to and use of them in LMICs, where historic and ongoing underinvestments heighten vulnerability to a multiplicity of health threats. By ‘vertical’ responses, we refer to COVID-19 interventions focused primarily on preventing and containing the virus, without adequately ensuring other health services remain safely operational, accessible and used by people who need them. This paper provides insight for use by actors in government, agencies, organisations and local communities to design and implement more proportionate, appropriate, comprehensive and socially just responses that address COVID-19 without compromising other aspects of health, particularly in LMICs. It presents a more holistic picture of the broader health and health system impacts of the pandemic, and specifically, those resulting from responses to contain to it.
To identify broader impacts and their drivers under narrow time constraints, we conducted a rapid evidence assessment of both academic and grey literature in August 2020.3 Following a search in the academic database Web of Science, which yielded few relevant articles, we also relied on Google and Google Scholar searches, as well as extensive snowballing methods. Due to the rapidly changing situation surrounding the COVID-19 pandemic, we also identified emerging information through reliable news outlets and reporting from development, public health and humanitarian organisations and databases. This iterative strategy enabled us to include the most recent developments and to capture data not represented in formal research from a range of settings and across a range of health and health system issues to address our broad questions, and thus to provide a snapshot of some of the key ways in which pandemic responses have and are likely to continue having broader impacts on health and health systems. See online supplementary appendix for a more detailed description of our methods and limitations.
Supplemental material
Ultimately, we argue there is a need to re-evaluate priorities and approaches in global health, moving past immediate action, both in the context of COVID-19 and other crises. ‘Whole of health’ approaches which account for the health trade-offs of COVID-19 response in the short term1 as well as address the health needs of diverse populations in the medium term to long term are crucial for just and effective health outcomes.
Vertical responses to COVID-19 and drivers of broader health and health system impacts
Health security and the legacy of vertical response
While the scale of response to COVID-19 is unprecedented, ‘disease exceptionalism’ and vertical strategies/responses are not new.4 5 For decades, through the frame of ‘health security’, the global health community has focused on targeted preparation for, identification of and response to infectious disease outbreaks when and where they emerge—usually in LMICs—not least, as suggested by a common critique, to stop them before they can threaten wealthier populations in the global north.6 This orientation may have come at the expense of more holistic and equity-based approaches to health. Alongside structural adjustment policies—which critics have also suggested have undermined many LMICs by, for instance, forcing them to cut spending on health and social programmes—the health securitisation regime may have contributed to chronically weak health systems which do not meet the needs of populations and, ironically, may actually result in increased risk of outbreaks of infectious disease in these settings.7 8 Furthermore, in the context of emergencies, a long-standing issue has been that ‘humanitarian response’ models often do not allow for investments that benefit people in the longer term.9 For instance, funding may be pledged and budgets made available to cover the trucking in of water to healthcare facilities during a health crisis, but not for investments in new clean water infrastructure.
Responding to COVID-19 in LMICs
The scale of the COVID-19 pandemic and its impacts on wealthy countries and individuals have prompted claims that the virus ‘does not discriminate’. Indeed, the fact that it has significantly impacted global power centres and elites may very well have generated the enthusiasm to mobilise so robustly across the world. Such vigour is rarely on offer with regard to the persistent and still massive burdens of disease and health risks faced by LMICs, even when we are not in the midst of a global crisis.10 Powerful COVID-19-focused discourses and political pressures at the global and national levels have pushed these burdens further out of sight and mind, and emergency logics focused on understanding, preventing and containing COVID-19 have prevailed.
Early, targeted action against COVID-19 in LMICs was also spurred by real and legitimate fear of high morbidity and mortality caused by the virus, and the potential overwhelming of already weak health systems. Several months down the line, many of these countries, particularly on the African continent, have not experienced the catastrophic scenarios initially predicted.11 One model for Africa suggested it could expect 190 000 deaths to COVID-19 over the period of 1 year12—a small fraction of the over 2.7 million mostly preventable under-5 child deaths that occurred on the continent in 2018 alone.13 While such a contrast may make broader health and health system impacts of COVID-19 responses seem even more unjustified in these settings, the significant non-COVID-19 disease burdens in LMICs which have experienced more substantial direct impacts indicate a need to recognise, mitigate and address broader impacts in these settings as well.
‘Supply-side’ drivers of broader health impacts
Early moves by LMIC governments to prevent COVID-19 from spreading in their countries focused on emergency measures aimed at limiting in-person contact, similar to those initially enacted in high-imcome countries. Strategies across settings ranged from near complete ‘lockdowns’ to more partial interventions in daily life.14 The specific mix of these ‘non-pharmaceutical interventions’ (NPIs), their stringency and duration has ranged widely as governments have responded to COVID-19 transmission dynamics within particular political, social and economic contexts. Such NPIs have included
Halting ‘non-essential’ work activity.
Movement restrictions and strict border controls or closures.
Suspension of public gatherings.
Stopping or scaling down public and private transportation systems.
Curfews and stay-at-home measures.
Closure of schools and other public institutions.
Suspension of non-essential health services.
Modifications to health service delivery, including closure of brick-and-mortar facilities.
Whatever mix and intensity, many of these measures have been disruptive to the availability, accessibility and use of health services in LMICs, and the public health rationales for deploying them in these settings have been widely questioned.15 Restrictive measures also interact with already profound weaknesses in LMIC health systems to produce even worse health outcomes. Limited material resources, staff and space have been diverted to address COVID-19, further straining capacity to address the wide range of health needs of different LMIC populations. Table 1 presents examples of how these interventions and systemic limitations have had broader health system impacts, which in turn have consequences for other areas of health.
Supply-side drivers of broader health system impacts related to vertical response
Beyond lockdowns
As suggested in table 1, not all drivers of broader health system and health impacts derive from restrictive measures. Limited health system resources play a major role, as does their prioritisation. Equally important are the connections between negative health impacts and vertical approaches to other elements of response. It is widely acknowledged that an effective overall epidemic response requires a range of public health measures such as surveillance, contact tracing, testing, risk communication and community engagement. All of these are key pillars of epidemic response16—and yet, they may have blind spots for other areas of health if vertical approaches to them are taken. While it is important that medical testing for COVID-19 is available and functioning amidst an outbreak, this should not be done at the expense of testing for other diseases, such as tuberculosis (TB), HIV or malaria which do not go away in the face of COVID-19, and still cause considerable morbidity and mortality in many LMICs.17 Risk communication and community engagement focused solely on COVID-19 risks leaving people without crucial information on how to protect themselves from other still-present health risks (although COVID-19 preventive measures may also protect people from a range of other infectious conditions), and importantly, how they can seek care for other health conditions in rapidly shifting health system landscapes.
Demand-side drivers of broader health system and health impacts
While it is hard to disentangle exactly what keeps people from accessing health services in any given context without detailed research, significant drops in use in some settings have been clear. In Kinshasa (Democratic Republic of Congo), for instance, researchers observed a nearly 40% drop in use of diabetes services from March to June of 2020.18 Although the impeding supply-side factors described earlier may contribute to low use, demand-side dynamics, including fear—and not only of the virus—social circumstances, loss of income and difficulty adhering to treatment also play a role. Table 2 includes additional explanation of these factors.
Demand-side drivers of broader health system and health impacts
Interacting with and exacerbating baseline vulnerabilities
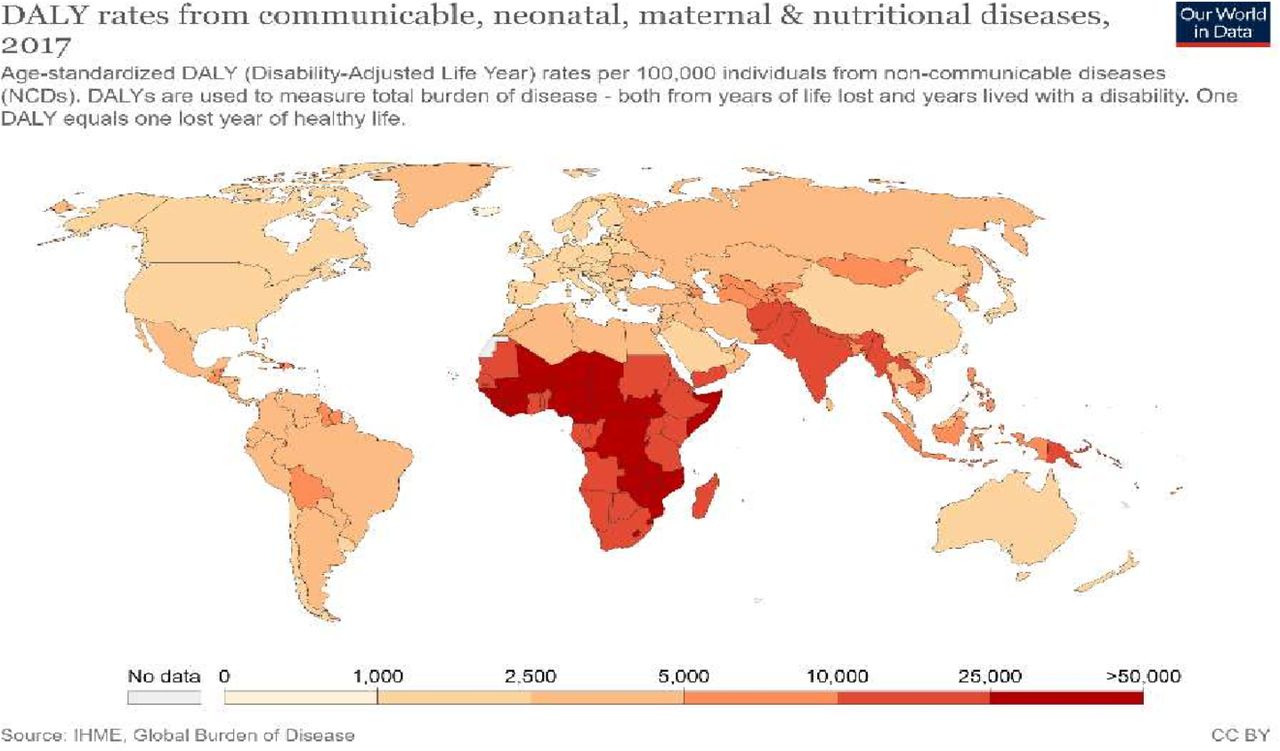
While many of the initial restrictive measures have been lifted or relaxed in many contexts (although lockdowns have been and will likely continue to be reimposed depending on dynamics of COVID-19 transmission), their effects continue to ripple across time and space, particularly as they interact with baseline vulnerabilities which have also been exacerbated by the pandemic. Indeed, even before the pandemic, LMIC populations faced disproportionately high risks of communicable, neonatal, maternal and nutritional diseases which lead to early death (see figure 1), as well as rising rates of non-communicable diseases (NCDs).
{kind=link}
DALY rates from a range of disease and health issues. Source: Our world in data (2017), DALY rates from a range of diseases and health issues (https://ourworldindata.org/grapher/burden-of-disease-rates-from-communicable-neonatal-maternal-nutritional-diseases). DALY (disability adjusted life years).
These health risks have long been interlinked with poverty and economic precarity: large swathes of people in LMICs rely on informal livelihoods and already lacking social protection, have now also lost income earning opportunities due to the pandemic. The World Bank has estimated an additional 71 million people may be pushed into extreme poverty,19 severely compromising their ability to access health resources including safe and adequate housing, water, food and healthcare.
Vulnerable social groups
Just as countries are not equally vulnerable to broader health system and health impacts, people within countries, communities and households face different levels of risk. Marginalised social groups are likely to be impacted much more acutely by both supply-side and demand-side drivers described previously, as well as face sets of challenges that are unique to their own circumstances and context. Table 3 highlights additional challenges faced by particularly vulnerable groups. Categories may also often overlap, compounding vulnerability for people who live at their intersections.
Social groups especially vulnerable to broader health impacts
Documenting broader health system and health impacts
Limited evidence and limited prioritisation
Research priorities and data collection have focused on COVID-19, with far less attention given to other health issues and impacts. Indeed, it is difficult to collect or monitor data in any fast-moving emergency, particularly in LMICs where robust data collection mechanisms are weak to non-existent. Broad modelled estimates, based on assumptions, past experiences and emergent understandings predominate, alongside qualitative descriptions in the media and from responding agencies and organisations. Although attention to broader health system and health impacts has been growing,1 it remains urgent to expand research, understanding and response in these areas.
One indicator of broader health impacts is the number of deaths in excess of expected mortality not attributed to COVID-19. However, quality data of this nature are limited in LMIC settings,20 and in many cases, only proxies are available for its estimation. In Jakarta, for instance, burial data suggest nine times as many excess deaths from non-COVID-19 causes occurred from March to May 2020 as COVID-19 deaths.21 It is likely that some (or indeed, many) were caused by COVID-19 and have simply been missed as such due to limited testing and surveillance capacities. Nevertheless, substantial additional mortality is clearly occurring,22 likely reflecting limited access or use of crucial healthcare.23 Both qualitative and quantitative investigations need to be deployed to better understand the extent, character and causes of impacts and to provide ‘actionable’ data.24
Evidence of impacts
As earlier discussed, broader health system and health impacts are being driven by a range of dynamics. Some health services, such as child immunisations, antimalaria campaigns, HIV and TB screening and treatment, screening and treatment for NCDs and sexual and reproductive health services, have been particularly affected.
Table 4 offers an overview of impacts, including both modelled estimates and more selective evidence, in several health areas.
Broader health system and health impacts in a range of health areas
Mitigating negative health impacts: health system and community approaches
COVID-19 must be put in perspective vis-à-vis other disease burdens and health services, including medium-term and long-term views. Prioritisation of health system resources should be set via meaningful participation of affected communities, health system users and patients, with special consideration for the participation of vulnerable groups. This requires funding and support for dedicated spaces and staff to bring the public (including community members, civil society organisations and grassroots movements) and policy makers together for inclusive dialogue.25 Past experiences from the HIV and West African Ebola epidemics demonstrated how community involvement was crucial to improving response.25 Coordination between international, national and local actors also proved critical to raising awareness and prompt action. Tools including evidence-to-decision frameworks and systematic trade-off appraisal can also be leveraged to support better informed short-term decision-making.26 27
COVID-19 has shed light on health system capacity and the importance of preparing for and addressing comorbidity. Emerging concerns about other infectious conditions (measles, TB and HIV/AIDS) and NCDs in their relation to COVID-19 create opportunities to incorporate these priorities into a more integrated, health system approach. A positive experience drawn from the fight against HIV/AIDS is the importance of tracking the disease and its treatment and holding governments accountable for containing the spread and ensuring universal treatment coverage.28 The global community and LMICs should be accountable to the commitments to primary healthcare made at Alma Ata and to Universal Health Coverage commitments, and donor countries should provide necessary funding and support. This global support for health system strengthening in LMICs is also crucial to avoid a medium-term scenario in which COVID-19 is addressed in wealthier countries, but remains endemic in poorer ones, as has occurred with diseases such as cholera.29
In the wake of COVID-19, NCD response, locally relevant contagious disease and health services (eg, nutrition and maternal and child health), and their integration into universal and affordable primary healthcare should be a priority.30 The COVID-19 response and services should be integrated, whenever possible, within existing health and social programmes.31 These programmes could share information systems, infrastructures, diagnostic and treatment capacities and outreach to break siloes.32 Health systems should establish cross-sectoral links (eg to social protection and education) to incorporate the social determinants of health.30 Digital solutions—where feasible—can help build linkages across and beyond health systems.
Decentralised, community-based, and people-led approaches are more likely to reach people suffering from broader health impacts and be accepted by communities.33 Examples of community-based approaches have been implemented to address COVID-19-associated service disruption in some settings. In India, for instance, volunteer health workers shared tablets and phones, and went door-to-door (while maintaining physical distance) to find cases, deliver antiretroviral therapy, ensure treatment uptake, deliver food, and give advice on HIV and COVID-19 transmission.34 In sub-Saharan Africa, community health workers have similarly delivered bed nets, medications and supported people to sustain needed treatment.35 The lack of personal protective equipment (PPE), however, has been an important challenge. Investing in financial resources and capacity building for community workers is crucial to prevent future outbreaks.30
Health provision for COVID-19 and its broader health system and health impacts must build on existing response networks: civil society organisations (unions, professional associations, religious groups and women’s groups) and social movements (within and beyond health). These organisations and movements should be provided with resources and support to lead elements of response and healthcare delivery. In turn, health policy makers should consider, wherever relevant, the plurality of health providers and therefore engage with private clinicians, pharmacists, drug sellers, traditional and faith healers, herbalists and others who may be patients’ first point of healthcare. These providers should be awarded necessary resources and skills for infection prevention (including PPE), in order to support triaging, surveillance, diagnosis and treatment for a range of health issues.
Real-time surveillance of perceptions, delivery, access to and use of health services can enable policy makers and responders to take immediate, context-relevant action.36 Expanded collection and use of granular social science research should be put into place to identify what health services are disrupted and why, to understand localised impacts, and to guide local and national response action. A framework for integrated data analysis, such as the integrated, multisectoral outbreak analytics (IMOA) model can provide a comprehensive understanding of cause and effect of broader impacts at multiple levels. IMOA brings together data on behaviour, perceptions, health service use, epidemiological trends of other health outcomes, movement mapping and market prices against a timeline of applied NPIs.37
These systems would also support accountability of local-level health providers and policy makers through public monitoring of health indicators and services, and integration of patient and community feedback to improve health services. Over time and integrated alongside a diversity of natural and social science data considered through multisectoral deliberative processes,36 this surveillance can also feed into joined-up medium-term and longer-term approaches and commitments up to the task of addressing the triple threat of COVID-19, other serious health priorities and impending economic crises into the future.
Conclusion
In just a few months, COVID-19 fundamentally changed the ways in which our social, economic and political systems operate. Not least among these are our health systems. While some changes have been necessary (to prevent in-person health service visits from becoming sites of COVID-19 infection and to allocate scarce resources), they have not necessarily been well conceived or executed, in part due to a lack of resources. Furthermore, the fallout from the interactions between vertical response measures, pre-existing vulnerabilities and wider impacts of the pandemic have led to myriad new challenges and barriers for health systems and for people who need care. The lack of attention to the broader health system and health impacts of vertical response measures, particularly under lockdowns—but also other elements of public health responses which, while less directly disruptive than lockdowns, may still have blind spots—has resulted in and will continue to cause significant harm to health and well-being. LMICs are particularly vulnerable as their substantial disease burdens and historically weak health systems present significant challenges. In addition to documenting some of the pathways and evidence of these impacts, this paper calls for more holistic approaches to health in the context of COVID-19, but also beyond it, and urges action to mitigate tragedy in both the short- and long-term.
Acknowledgments
The authors thank the two anonymous reviewers for their thoughtful comments and suggestions, which resulted in an improved version of this paper. Additionally, the authors thank a number of individuals who initially contributed to the framing or provided comments and input on the original review for the Social Science in Humanitarian Action Platform upon which this paper is based, including Y-Ling Chi (Centre for Global Development), Gillian McKay (London School of Hygiene and Tropical Medicine (LSHTM)), Neha Singh (LSHTM), Olivia Tulloch (Anthrologica), Melissa Leach (Institute of Development Studies (IDS)), Annie Wilkinson (IDS) and Hayley MacGregor (IDS).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @thrynick, @simone_tweets
Contributors TAH, SRL and SEC all contributed to the research and drafting of the manuscript, as well as revisions following peer review.
Funding This work was supported by the Wellcome Trust Grant Number 219169/Z/19/Z and the UK Foreign, Commonwealth and Development Office. The opinions expressed are those of the authors and do not necessarily reflect the views or policies of IDS, Anthrologica, LSHTM, Wellcome Trust or the UK government. For the purpose of Open Access, the author has applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.