Article Text

Abstract
Objective To review the effectiveness of travel measures implemented during the early stages of the COVID-19 pandemic to inform changes on how evidence is incorporated in the International Health Regulations (2005) (IHR).
Design We used an abbreviated Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols to identify studies that investigated the effectiveness of travel-related measures preprinted or published by 1 June 2020.
Results We identified 29 studies, of which 26 were modelled. Thirteen studies investigated international measures, while 17 investigated domestic measures (one investigated both). There was a high level of agreement that the adoption of travel measures led to important changes in the dynamics of the early phases of the COVID-19 pandemic: the Wuhan measures reduced the number of cases exported internationally by 70%–80% and led to important reductions in transmission within Mainland China. Additional travel measures, including flight restrictions to and from China, may have led to additional reductions in the number of exported cases. Few studies investigated the effectiveness of measures implemented in other contexts. Early implementation was identified as a determinant of effectiveness. Most studies of international travel measures did not account for domestic travel measures thus likely leading to biased estimates.
Conclusion Travel measures played an important role in shaping the early transmission dynamics of the COVID-19 pandemic. There is an urgent need to address important evidence gaps and also a need to review how evidence is incorporated in the IHR in the early phases of a novel infectious disease outbreak.
- COVID-19
- control strategies
- public health
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Previous reviews of the evidence from outbreaks of influenza and other infectious diseases have generally found that there is limited evidence of the effectiveness of travel measures in containing outbreaks.
However, it is unclear if the lessons from other infectious disease outbreaks are relevant in the context of COVID-19.
Based on evidence at the time, WHO did not recommend any travel restrictions when it declared COVID-19 a Public Health Emergency of International Concern (PHEIC).
What are the new findings?
This study rapidly reviews the evidence on the effectiveness of travel measures implemented in the early phase of the pandemic on epidemiological outcomes.
The study investigated both international and domestic travel measures, including a wide range of travel measures.
The study finds that the domestic travel measures implemented in Wuhan were effective at reducing the importation of cases internationally and within China and that additional travel restrictions were also likely important. The study also finds that travel measures are more effective when implemented earlier in the outbreak.
The findings generated implications for how evidence is integrated into the International Health Regulations and highlights important research gaps that remain.
What do the new findings imply?
Findings highlight the need to evaluate the potential effectiveness of travel measures using a risk and context-based assessment of each specific outbreak and the types of measures used.
The findings of this study also suggest the need to strengthen the PHEIC process in such a way to increase the likelihood that travel measures, when warranted, can be implemented rapidly enough to maximise their effectiveness.
Introduction
On 31 January 2020, the WHO declared the outbreak of SARS-CoV-2 a Public Health Emergency of International Concern (PHEIC). Based on information available at the time, and beyond recommending that China should enforce exit screening at its borders, the International Health Regulations 2005 (IHR) Emergency Committee explicitly did not recommend the adoption of ‘any travel or trade restriction’.1 While the IHR do not preclude State Parties from adopting health measures aimed at travellers, they do state that State Parties should follow WHO guidance and that they should avoid the adoption of measures that may lead to ‘unnecessary interference with international traffic’ and that such measures should not be ‘more restrictive of international traffic and not more invasive or intrusive to persons than reasonably available alternatives that would achieve the appropriate level of health protection’ (Article 43). Moreover, measures adopted should be based on ‘scientific principles’ and evidence.
As early as 31 December 2019, the same day that the Chinese Centre for Disease Control first notified WHO of a cluster of atypical pneumonia cases in Wuhan, some jurisdictions (including Taiwan, Russia and Macau) began to impose travel-related measures on travellers from Wuhan, mainly airport screening.2 Within weeks, additional countries also restricted flights to and/or suspended entry from Wuhan, including Mongolia, Australia and North Korea. On 23 January, a cordon sanitaire was drawn around Wuhan, effectively suspending all international and domestic travel in and out of the city.3 A day later, the measures were extended to all of Hubei province. By March 2020, despite WHO’s initial recommendations, virtually all IHR (2005) State Parties had implemented some form of cross-border travel-related measure during the initial phase of the COVID-19 pandemic.4 This is, by far, the largest number of countries adopting such measures during a PHEIC: only about a quarter of countries had imposed such measures during the 2009 H1N1 pandemic and the 2014 Ebola outbreak in West Africa.5–7 It is estimated that there was a 65% drop in international travel in the first half of 2020 as a result of the COVID-19 pandemic.8
The nearly universal adoption of travel-related measures, especially in light of the potentially large economic and social consequences, raises questions as to whether such measures can be, and have been, effective at reducing international transmission of the virus during the pandemic. Studies from previous infectious disease outbreaks have suggested that certain travel-related measures have only limited, or at best modest, effectiveness in containing outbreaks of influenza. For example, a systematic review of the effectiveness of international travel measures (screening, travel restrictions and border closures) to control pandemic influenza identified 15 studies and found that measures implemented early could delay local transmission by a few days or weeks, slow international spread and delay the epidemic peak in isolated locations by reducing the number of seeding events.9 The review did not identify any evidence that screening methods were effective but it did find that border closures had been effective in preventing virus introduction to small island states during the 1918 influenza pandemic. However, the authors also concluded that the overall evidence base on which they drew their conclusions was small and of low quality.
A related but larger review of a broader range of measures, including travel advice, screening, internal travel restrictions and border closures, for both epidemic and pandemic influenza, also found that travel restrictions could delay the arrival and spread of epidemics and that select isolated locations may benefit more from border closures. However, once again, the overall effect sizes were relatively small, and the quality of evidence was also found to be very low.10 Another review of both international and domestic travel restrictions concluded that such measures could delay, but not contain, dissemination of both pandemic and seasonal influenza after it emerged.11 Based on the 23 studies identified, the review concluded that internal and international border restrictions could delay the spread of an outbreak by 1 week and 2 months, respectively, and that such restrictions could delay the spread and peak of epidemics from between a few days to up to 4 months. However, the timing of the introduction of such measures was key; the extent of the delay of spread was greatly reduced when restrictions were imposed more than 6 weeks after the onset of an epidemic.
Beyond influenza, evidence from other infectious disease outbreaks is more limited. A modelling study of travel restrictions implemented during the West African Ebola outbreak estimated that such measures may have delayed further international transmission by a few weeks for some countries.12 Given the low proportion of all international travellers originating in Ebola-affected countries at that time, another study suggested that exit screening measures in affected countries were likely to be more effective at reducing onward international transmission than travel restrictions,13 a finding that was supported by a similar study.14 The travel advisories issued by WHO during the 2003 SARS outbreak, which led to substantial declines in international travel to Hong Kong and Mainland China, were estimated to have delayed the export of cases by only a few days.15 Importantly, other studies have suggested that travel measures during outbreaks can be counter-productive by preventing countries from launching effective epidemic responses,16 undermining the detection of cases and causing widespread economic effects on the travel industry itself.17
However, since the onset of this pandemic, it has become clear that the clinical features of COVID-19 make it more challenging than previous infectious diseases to detect and contain,18 raising questions about whether evidence of effectiveness from previous studies is relevant for COVID-19.19 The goal of this paper is to review evidence of the effectiveness of travel-related measures implemented during the early stages of the COVID-19 pandemic, a time of many unknowns regarding the clinical and epidemiological features of the COVID-19. Since the emergence of COVID-19, dozens of studies have now been published or made available that evaluate the effectiveness of travel-related measures in the context of the pandemic. The only other effort we know of to review the evidence of travel measures is a very recently released Cochrane review of the literature on the effectiveness of international travel-related measures to contain COVID-19, severe acute respiratory syndrome (SARS) and Middle East Respiratory Syndrome (MERS).20 This review certainly adds to our understanding of the evidence base of travel measures; however, it did not investigate the effect of domestic travel measures, including those imposed in Wuhan, potentially overlooking a valuable piece of evidence on the effectiveness of travel measures. That review identified 36 studies, of which 25 were specific to COVID-19 and concluded that cross-border travel measures may limit the spread of disease across national borders, specifically in terms of reducing the number of imported cases and delaying or reducing epidemic development, although it found that the certainty of the reviewed evidence was low to very low. Given the widespread adoption of travel restrictions, and the likely enormous economic and social consequences resulting from them, a fuller understanding of the effectiveness of all of the measures adopted during the early phase of the pandemic is warranted. While the question of whether the adoption of these measures is compliant with the IHR has received attention in the literature,21 22 it is beyond the scope of this paper.
Methods
To conduct this review, we adopted an abbreviated version of the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) Protocol using the 17-point checklist.23 The rationale for the study was the widespread adoption of travel measures despite consensus view at the time that such measures were largely ineffective and to strengthen the application of the IHR during this and future pandemics. The objectives were to rapidly review evidence of the effectiveness of the full range of travel measures adopted during the early stage of the COVID-19 pandemic, from both published and unpublished studies. We further elaborate on other methods of the study below.
Search strategy
Our search strategy was designed to be as inclusive as possible of all studies (as of 1 June 2020) that provide new evidence of the effectiveness of any travel-related measure adopted during the early phase of the COVID-19 pandemic. According to the IHR, travel-related measures include travel advice, entry and exit screening of travellers, medical examination or vaccination requirements for travellers, isolation or quarantine of suspected or affected persons, the refusal of entry of travellers and restrictions on travellers from affected areas.1 While only those measures that are applied by State Parties at the level of an international border are covered by the IHR, many of these measures have also been applied to domestic travellers (eg, at the level of interprovincial or interstate borders). Private companies, such as airlines and cruise ships, have also implemented travel measures which, while also not subject to the IHR, further restricted travel during this pandemic. We did not restrict the search to specific outcomes (eg, epidemiological or otherwise), or any specific methodological approach, or any specific geography. We only identified one study that looked at non-epidemiological outcomes,24 so while we include it in our description of the search and screening strategies, we exclude it from our main analysis below.
Given the rapidly evolving nature of the outbreak, as well as the rapidly expanding published literature on COVID-19, our search strategy targeted both preprint and published articles, with the strategies to identify each differing slightly. Keywords were identified based on both inductive iterative testing of potential keywords, as well as deductively through papers identified through other channels. Search terms were then refined to minimise overlap and to maximise the number of studies that could be identified. While we did not impose a language restriction, we did not specifically search in non-English sources.
For preprint papers, we searched the BioRxiv and MedRxiv servers, which offer limited search functionality, using the following keywords in the title field: travel*, flight*, airline*, border*, airport*, passenger or air traffic. We restricted the sample to papers that also included at least one COVID-19 keyword, either related to the virus itself (eg, coronavirus, corona virus, coronavirinae, coronaviridae, betacoronavirus, COVID-19, COVID-19 19, COVID-19, nCoV, CoV 2, CoV2, sarscov2, 2019nCoV, novel CoV, OR Wuhan virus), the location of the early outbreak (eg, Wuhan, Hubei or Hunan) or less specific but widely used terms (severe acute respiratory OR pneumonia AND outbreak). We used the same travel-related keywords to search the WHO’s COVID-19 global research database but did not impose a COVID-19 search term as theoretically all articles in this database were on this topic.25
For published papers, we searched PubMed with the following search strategy: studies must include at least one COVID-19 keyword mentioned above or one of the location-specific terms mentioned above combined with either (“severe acute respiratory” OR pneumonia AND outbreak) or one of the following MESH terms (Coronavirus, Coronavirus Infections, or Betacoronavirus) or the supplementary concept (COVID-19 or severe acute respiratory syndrome coronavirus 2). All studies must also include at least one travel-related measure term in the title or abstract (eg, screening, travel advice, travel advisory, cordon sanitaire, ban, restrict*, prohib* or clos*) as well as one travel-related term in the title or abstract (travel*, cruis*, ship*, terrest*, airplane, flight, plane, migrant, passenger, return, outflow, outbound, inbound, inflow, traffic, arrival, train, trains, bus, buses, transit, port*, airport*, tourist*, international importation, international exportation, case importation, imported cases, exported cases or border).
Screening strategy
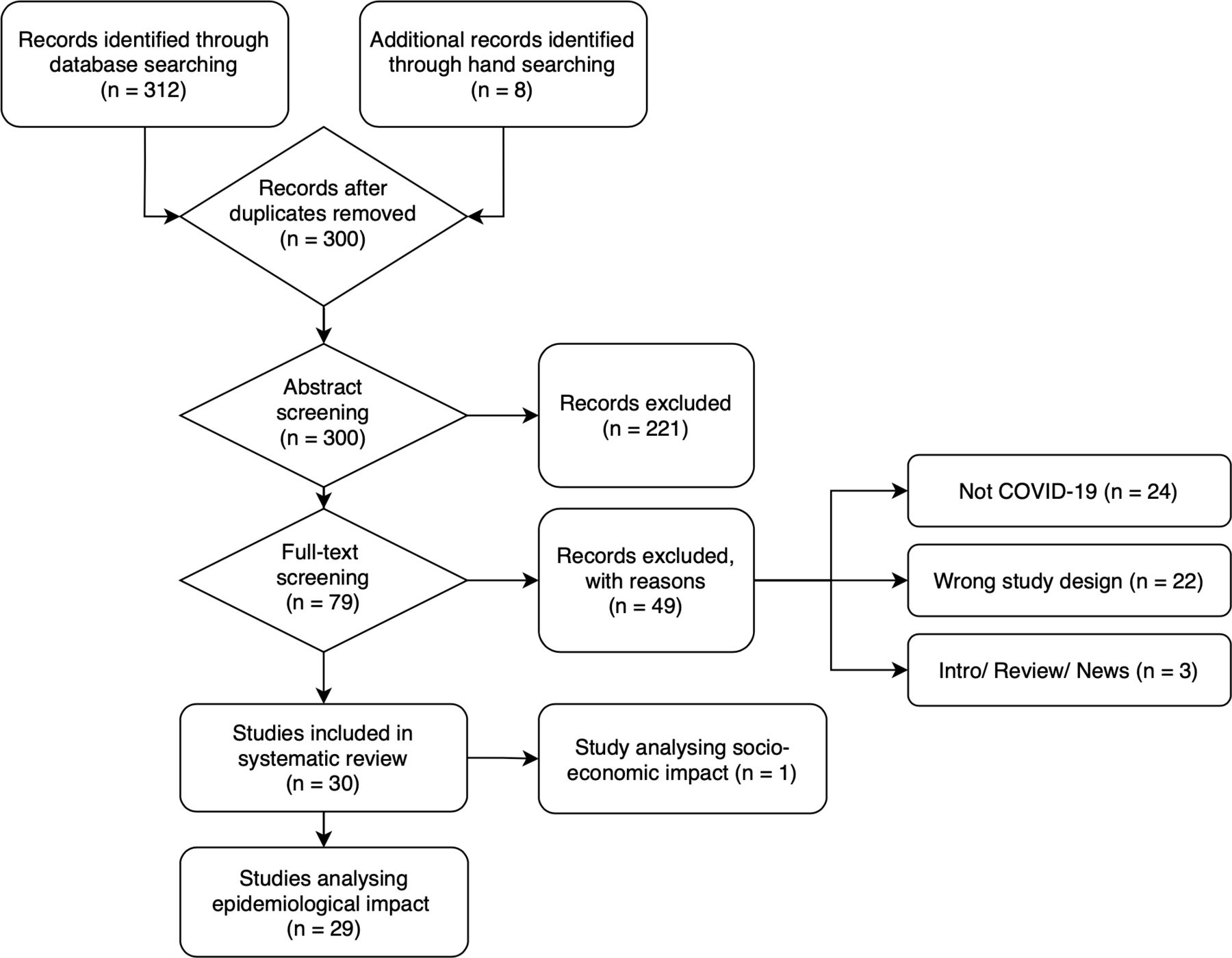
As of 1 June 2020, we identified a total of 312 articles, and during the review process, we identified another eight articles through other sources (see figure 1). From all identified studies (n=320), we removed duplicates, which left 300 articles to be screened. We uploaded the abstracts into Covidence (https://www.covidence.org/), software developed for systematic reviews, to perform a title and abstract screen. Our inclusion criteria were that studies must investigate the COVID-19 pandemic and at least one travel-related measure (applied either at an international or domestic border), must be empirical (ie, modelled or observational) and must evaluate a specific outcome (epidemiological or other). Measures could have been undertaken by either a public (ie, a government) or a private actor (eg, an airline). We excluded articles that were news reports, review articles, commentaries or editorials, or conjecture (ie, did not provide new data or evidence) about the effectiveness of travel measures. Each article was screened by two independent reviewers (T-LH and ZL). Where there was disagreement among the reviewers, a third reviewer (KG) resolved any disagreement.

{kind=link}
PRISMA diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
After screening, we were left with 79 articles. The full texts of each were obtained and again uploaded into Covidence. Two reviewers again screened each article to determine if the article still met the inclusion criteria. Any disagreements among the two reviewers were again reviewed by a third reviewer (KG) who was not otherwise involved in the screening process. After the full-text screening, we were left with 30 studies that met all of our selection criteria. Of these, one study investigated socioeconomic outcomes, which we exclude from this analysis given the lack of overlap in outcomes.
Updating strategy
We continued to search the relevant databases for any newly published papers or to identify papers that had originally been identified as preprints but were subsequently published until 1 June 2020. We retained the subsequently published versions of such papers.
Data extraction
For the remaining 29 studies, we extracted the title, authors, article source, publication date, whether it was a preprint or published (or had previously been a preprint) article, country context in which the study was conducted (or global), country(ies) implementing the measure, the country(ies) affected by the travel measure, specific measure(s) adopted, the timing of the measures, the duration of the measures, whether the study was modelled or based on observational data, the type of model used, epidemiological assumptions made in the models, the specific outcomes observed, the overall findings, the way in which cases/deaths were recorded, whether there was any description of diagnostic methods used to identify cases/deaths, whether the study made assumptions about asymptomatic cases, whether the study also accounted for secondary transmission, the extent to which the model accounted for other measures imposed around the same time, the data sources used in the study and the stated limitations of each study. For modelled studies, we also collected the name of the model used if an existing model was used, whether the model used was a dynamic or static model, whether the model used was a stochastic or deterministic model and whether it was an individual versus population-based model. A full list of the papers, with additional details on each, is presented in online supplemental appendix table 2.
Supplemental material
Analysis of travel measures
We characterised the investigated travel-related measures into four groups: suspended transportation, border restrictions, entry or exit screening and entry quarantine, which are summarised in table 1. Papers may have investigated more than one measure and thus may contribute more than once to the table. In our analysis, we grouped studies according to whether the measure affected international (table 2) or domestic travellers (table 3). One study fit both criteria and thus is listed twice in the analysis. We used a narrative approach to synthesise the evidence of effectiveness. Two studies,26 27 despite study design and stated objectives to investigate the impact of travel-related measures, did not present their findings in such a way that allowed us to extract the evidence generated in the study. These are summarised in online supplemental appendix table 2 but not in tables 2 and 3.
Summary statistics
Effect of international travel measures
Effect of implementation of interprovincial travel measures
Analysis of outcome measures
Outcomes included the number of observed cases, date of the epidemic peak, risk of transmission, case growth rate, doubling time, time of arrival in a new country, the reproductive number (R0 or Rt) and projected cumulative cases. Details are listed in tables 2 and 3, which summarise papers that investigate international and domestic travel measures, respectively. One article that evaluated the effectiveness of both types of measures28 appears in both tables.
Assessment of bias
Individual articles were assessed for bias using a proprietary scoring system consisting of three tiers: low, moderate and high risk of bias. Low scores were given when the author had adequately addressed the domain, moderate when it had been either partially or incompletely addressed or high when it was not or only poorly addressed. Articles were assessed with regards to their ability to form a clear and precise definition of the research question, travel restriction measures included in the analysis, comprehensiveness of outcome, suitable mathematical modelling, model assumptions described, confounding factors, model validation and uncertainty assessment.29 A detailed summary of our bias assessment is presented in online supplemental appendix table 1.
Supplemental material
Results
Of the 29 identified studies in this rapid review, 24 had been published by 1 September 2020, while the rest were preprint studies (see table 1). Almost all of the studies (26) were modelled studies with few observational studies (3). Given the timing of the studies, almost all of the studies focused on the initial exportation of cases from Wuhan either domestically within China or internationally. Among the travel-related measures adopted, the most commonly investigated were suspended transportation (24), border restrictions (21) and screening (5). Only four studies investigated entry quarantine.
Effectiveness of travel-related measures on the international spread of COVID-19
In table 2, we present the summary of evidence generated from the papers that investigated the impact of international travel measures. All but one30 were modelled studies. Four studies directly investigated the impact of the Wuhan travel ban on the initial export of cases internationally.28 31–33 Comparing the observed number of exported cases to scenario-based modelled estimates without the ban, studies consistently found that these measures were highly effective at reducing exportation of cases. Among the studies that investigated the impact of the Wuhan travel measures, there was a consensus that the measures led to a 70%–77% reduction in the number of cases exported internationally through early to mid-February: Anzai et al31 estimated a 70% reduction in exported cases globally in the week following the introduction of the ban, Chinazzi et al28 estimated that the ban led to a 77% reduction in imported cases while Wells et al32 estimated that it reduced the number exported cases by 70.5% through mid-February. Kucharski, however, estimated that transmission rates outside of China were reduced by about half in the 2 weeks following the introduction of the ban.33
Beyond the direct effect of the Wuhan travel ban, Chinazzi et al28 estimated that the application of additional travel-related restrictions, in this case, the reduction in flights between Mainland China and receiving countries, led to substantial additional reductions in imported cases globally, though the extent of reduction varied by country and the extent of the flight reductions. Namely, reductions in international traffic of 40%–90% between China and other countries could have led to large additional decreases in imported cases and important delays in the arrival of a substantial number of cases in other countries through the beginning of March. Adiga et al34 investigated the impact of government or airline-imposed travel-related measures against China and estimated that these led to a delay in the importation of the virus by about 4–5 days on average and up to 10 days in select countries. This study, however, did not directly control for the impact of the Wuhan lockdown, which happened around the same time as many of the measures investigated.
In terms of specific country case studies, Adekunle et al35 found that Australia’s ban on air travel to and from China may have prevented 82% of imported cases through 2 February. Anzai et al31 which focused on the impact of the ban on the outbreak in Japan, estimated that the absolute risk of a major outbreak was only modestly delayed due to the Wuhan travel ban and that the median time delay in a major outbreak was only 1–2 days. Similarly, Costantino et al36 estimated that it may have led to a 79% reduction in imported cases through 2 March. Linka et al37 estimated that the travel restrictions implemented both at the external and internal borders of the European Union significantly decreased the speed of virus spread across member states, especially in Central European countries. These last two studies, both of which focused on an earlier period in the pandemic, failed to account for the impact of the Wuhan lockdown in addition to the restrictions evaluated.
Studies that investigated the effectiveness of screening found that only very highly effective screening could reduce (or decrease) the risk of importation or exportation. Clifford et al38 found that when the number of cases was low in the exporting country, screening may delay the onset of the epidemic in the importing country by up to a week, while Mandal et al39 found that if screening could detect 90% of asymptomatic individuals, it could delay the average time of the epidemic by up to 20 days in select countries. Assuming that self-identification of cases was effective, another study suggested that such measures could identify a large proportion of infected travellers. However, this assumes that screening is effective but does not study this directly.32
A single observational study identified in this review investigated the impact of border restrictions, in combination with mandatory quarantine and screening, for incoming travellers to Hong Kong. Cowling et al30 concluded that the application of quarantine measures of incoming travellers into the region was an important element of their successful public health response, but the study does not specifically estimate its impact independent of other measures including travel-related measures.
Effectiveness of travel-related measures on the domestic spread of COVID-19 within China
In table 3, we present the findings from the studies that investigated the impact of the Wuhan travel restrictions, on the domestic export of cases to other parts of China. By comparing actual observed cases to counterfactual scenarios where such measures had not been imposed, Chinazzi et al28 predicted that the travel ban led to a 10% reduction of exported cases within the first 7 days, Fang et al40 estimated a 39.3% reduction over 1 month Shi, Fang41 similarly identified a 39% reduction in cases over 1 month, while Tian et al42 estimated a 73% reduction through mid-February. Tang et al43 found that the Wuhan travel ban led to a 91.1% reduction in imported cases in Beijing for over 7 days. Similarly, Kraemer et al44 also found that these travel measures dramatically reduced the transmission of the outbreak across the country, with areas that had greater prelockdown connectivity with Wuhan experiencing a greater decline. Aleta et al45 estimated that the measures were effective in reducing the exportation of cases but only in the short term. Yuan also found the lockdown to be effective at reducing the number of cases outside of Wuhan but notes that the timing also coincided with a nationwide stay-at-home campaign imposed by the central Chinese government.46
Studies also investigated the impact of the travel ban on the domestic timing of the outbreak. Tian et al42 estimated the ban delayed outbreaks within China by 2.91 days, while Chinazzi et al28 estimated a delay of 3–5 days. Studies also investigated the impact of the travel ban on the effective reproductive rate, the doubling time and other measures. Hou et al47 found that the ban quickly reduced the reproductive rate of the virus outside of Wuhan,; similarly, Li et al48 found that the reproductive number dropped by more than half within 2 weeks of the introduction of the ban. Using observational data, Lau et al49 found that the doubling time of the virus increased from 2 days to 4 days after the travel ban was imposed. Another study found substantial declines in transmission routes between Chinese provinces within weeks of the introduction of the Hubei travel bans.50
The timing of travel-related measures, again, appears to be important in predicting effectiveness. Both Lai et al and Liu et al, the former a modelled study and the latter an observational study, estimated that the Wuhan travel ban would have been substantially more effective if implemented 1–3 weeks earlier.51 52 This is supported by Wu et al,53 who found that the travel ban had a relatively minor effect on the overall speed of transmission of the outbreak in areas of China outside of Wuhan, largely because a large number of cases had already been exported before the travel ban, limiting its effectiveness.
Finally, a few studies evaluated domestic travel bans in combination with other travel-related measures. For example, one modelled study estimated that if major cities within China had imposed additional measures, they could have further reduced their epidemic risk.54
Quality of available evidence
Our review of the risk of bias in the included studies (online supplemental appendix table 1) suggests that, apart from a few exceptions, while most of the studies had clear research questions, descriptions of the travel-related measure(s) evaluated, and discussions of the outcomes, few of the studies made efforts to adequately control for the presence of other public health or other travel-related measures implemented at the same time, or for other contextual factors that could influence the impact of travel-related measures. One important challenge common to all of the studies was the quality of data on detected cases early on in the pandemic and only a small number of the studies allowed for their estimates to vary based on potential ranges of the number of true cases that were actually detected early in the outbreak (eg, Chinazzi et al28 estimated 24.4% of all cases were undetected, Fang et al40 estimated 42%–80% were undetected, Kucharski et al33 predicted that there were at least 10 times as many cases as were confirmed in Wuhan in early February). The studies also varied markedly in their efforts to validate their models or provide uncertainty analysis around their estimates. Also, with a few exceptions, most studies did not discuss the potential measurement error associated with case data collected during the early phases of the pandemic, which likely did not capture most asymptomatic cases. The overall quality of the studies to evaluate effectiveness was thus relatively low.
Discussion
Despite WHO’s lack of recommendations of the adoption of travel measures and given the evidence of the limited effectiveness of such measures in other contexts at the onset of the COVID-19 pandemic, there was an unprecedented adoption of such measures during the early phase of the pandemic, both domestically and internationally, which contributed to dramatic declines in international travel. This paper reviewed the emergent evidence on the effectiveness of travel measures adopted during the early phase of the COVID-19 pandemic and identified several key findings.
First, there was a high level of agreement among the studies reviewed that the adoption of travel measures played an important role in shaping the early transmission dynamics of the COVID-19 pandemic. At the international level, studies consistently estimated that the Wuhan travel measures led to a 70%–80% reduction in cases exported in the first few weeks, and likely had a smaller effect within Mainland China, where estimates of effectiveness ranged from 10% to 70%. Also, the Wuhan travel ban likely led to delays of up to a few weeks in the importation of cases to other countries. Additional travel measures, namely a reduction in the number of flights to countries, had additional effects at reducing the number of imported cases. However, almost all the studies in this review focused on either domestic or international travel bans imposed on Wuhan and, to a lesser extent the rest of China, during the early period of the pandemic. As such, this review does not identify substantial new evidence of the effectiveness of travel-related measures aimed at controlling spread to and from other parts of the world or beyond the initial exportation of cases out of China.
Second, most of the studies also concurred that the effect of the Wuhan specific measures was short lived partially because, over time, other provinces became the source of most of the internationally exported cases from China. This suggests narrowly targeted travel-related measures against specific countries alone may not be sufficient since knowledge about where a new virus is circulating may be limited at the outset and that countries should also begin to implement domestic public health containment measures alongside international travel measures. This view is further supported by evidence identified in this review that suggests once four or more infections are introduced into a new location, there is an over 50% chance that a major outbreak will occur (absent other interventions).33
Third, the evidence reviewed suggests timing was a key factor influencing the effectiveness of travel-related measures. Several studies supported the view that within China, had the same policies been implemented a few weeks earlier, it is likely there would have been substantially less seeding of the virus across the country and internationally. Indeed, as noted previously, some jurisdictions (such as Taiwan, Russia and Macau) acted faster than Wuhan in implementing travel measures. While the Wuhan measures may have been too slow to be optimally effective, they were still implemented a full week before the PHEIC declaration was made by the WHO.
Fourth, many of the studies focused on the effectiveness of international travel measures failed to account for the implementation of the domestic Wuhan travel ban. Although this was a domestic policy, and thus outside the remit of the IHR, this review suggests restricting travel to and from Wuhan dramatically changed the outflow of cases from the region at a crucial period. Studies that did not account for the Wuhan travel ban in their estimates, or reviews that excluded domestic travel measures, likely overestimated the effectiveness of international travel measures. The notable exception was Chinazzi et al,28 which still concludes that the additional measures provided an important benefit above and beyond the effect of the Wuhan measures, through at least early March.
Fifth, during the early phase of the pandemic, there were likely large numbers of undetected cases globally, and although some studies allowed for their estimates to vary based on assumed proportions of undetected cases, the validity of the estimated effects in all of these studies is likely affected by data quality issues. Also, given that symptomatic individuals may be more likely to curb their travel than asymptomatic travellers, especially internationally and after the introduction of travel-related measures aimed at detecting symptomatic cases, modelled effectiveness studies may be biased if they do not account for this difference. Also, it is possible that some of the travel-related measures adopted (eg, screening) could have led to increased detection of cases,48 which could further complicate the evaluation of the effectiveness of travel measures, as the measurement of the outcome was also influenced by the intervention and few studies acknowledged this limitation.
Finally, while this study identified a relatively large number of studies, we assess the quality of these studies overall to be low. Almost all of the studies identified in this review were modelled studies, and therefore, the results depend on important parameter assumptions that varied considerably. Given the rapidly evolving and dynamic nature of the pandemic, it is unclear how close to reality these assumptions were. Comparability across the studies is also undermined by a lack of standardised terminology. Furthermore, few studies attempted to isolate the potential effect of international travel-related measures from a range of domestic measures implemented concurrently, or from the other social, political or economic characteristics of the implementing or target locations or populations.
This systematic review also has several important limitations. First, while we aimed to be systematic in our search strategy as well as inclusion criteria, the rapidly expanding literature on COVID-19 pandemic almost certainly means that we likely overlooked some relevant studies. Second, although we aimed to focus on the early phase of the outbreak, it is unclear when the appropriate time was to end our review. Newer studies that have been published since we completed our literature search may present a different picture on the effectiveness of travel measures, and thus, the evidence from this study must be evaluated in this context. Third, assessments of bias in studies are challenging and are inherently subjective.
Although the WHO did not initially recommend the adoption of such measures, it had softened its stance on the adoption of such measures over time. By May, the IHR Emergency Committee had recommended that WHO updated its recommendations to include measures that were better at ‘balancing the benefits of such measures with their unintended consequences’.55 By October, the committee had further suggested that WHO should work with partners to develop new guidance on the use of such measures, including guidance on the use of testing and quarantine, an ongoing process.56 Also, initiatives have commenced in recent months to review and strengthen the IHR. The universal use of travel-related measures by State Parties during the COVID-19 pandemic will likely be a major focus of discussion on the limitations of the current treaty.
Based on this review, we draw the following conclusions to inform those discussing ways to better integrate evidence into the IHR process and to inform better responses to future outbreaks. First, the findings of this review suggest that it is very difficult to know in the early phases of a novel infectious disease outbreak how effective travel measures are likely to be. As such, assessments of the potential effectiveness of such measures cannot be inferred from previous infectious disease outbreaks, especially when the clinical and epidemiological features of the virus are unknown. It also highlights the need to move from blanket assessments of the effectiveness of travel-related measures (‘travel measures don’t work’) to acknowledge that pathogen-specific assessments of effectiveness based on possible scenarios of transmission risk may be needed (‘for which types of threats might such measures be effective?’). Due to the limited transparency of the PHEIC declaration process, it is unknown what risk assessments were conducted by the Emergency Committee, or how. Given that both the level and range of measures adopted by countries during COVID-19 were very different from previous PHEICs, future assessments should consider a full range of potential scenarios.
Second, it is also clear that the effectiveness of travel measures cannot be estimated using a single fixed parameter. The effectiveness of measures will vary based on the setting, which other measures are also implemented (domestically and internationally), the extent to which they are implemented and the speed at which they are implemented. All of these factors, weighed against potential harms, also need to be taken into consideration in discussions about the potential effectiveness of international travel measures. Decision makers thus should further consider context-specific assessments of the effectiveness of such measures (‘when and where might such measure be effective?’).
Third, this study finds that measures implemented early were likely more effective than those implemented late. In this pandemic, the PHEIC declaration was not made until after many countries had begun to adopt travel measures, and when it was, the WHO recommended against the adoption of such measures. Also, the IHR require State Parties to provide evidence for any additional health measures that they implement. In the context of an outbreak of a novel infectious disease agent, it is unclear what constitutes evidence in the early phases of the outbreak. The importance of evidence, especially when it is unlikely that such evidence will exist, needs to be balanced against the potential of risk and the need to implement containment measures early.
This review also highlighted areas where more research is urgently needed to understand the appropriate role of travel measures during PHEICs. First, a greater understanding of the effectiveness of travel measures adopted globally during the COVID-19, including both at early stages but more importantly at stages beyond the early phases of the pandemic, is urgently needed. For example, many of the countries that were able to successfully control their pandemic in 2020 implemented strong border control measures, and many attributed their success directly to these measures.56 Second, there is a need to better understand the broad range of measures affecting travel beyond those covered in the reviewed studies, including the role of testing, which was not widely available during the early phase of the pandemic. Third, lack of data on true case numbers remains an underlying challenge across all of the study reviewed and thus needs to be taken more seriously in future studies. Fourth, models need to better account for how travel measures work in tandem with other measures implemented concurrently, including domestic travel measures and other public health measures. Fifth, studies need to better account for the possibility that some locations see greater benefit from travel measures than others based on geographic and socioeconomic factors. Finally, one of the rationales against the use of travel measures is their economic and social impacts, yet we were only able to identify one study that investigated their impact on non-epidemiological outcomes.
At the onset of the COVID-19 pandemic, there was a widely held belief that travel measures were unlikely to play much of a role in curbing the international spread of the virus. However, the widespread adoption, and persistent use of such measures, globally, as well as the evidence identified in this review, challenge this belief in favour of a more nuanced view. While this review emphasises that the quality of evidence remains low and highlights many methodological shortcomings in the reviewed studies, findings also identified new evidence of the impact of such measures during the early phase of the pandemic. These findings suggest travel measures did play an important role in shaping the early dynamics of the pandemic, even if they were unable to contain the virus globally on their own. Alongside many other transformations catalysed by COVID-19, the pandemic has also challenged our views of what constitutes evidence of the effectiveness of international travel measures.57
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @KarenGrepin, @bobby_ho_hk, @summermarion, @julianneepiper, @catworsnop, @profplum8
Contributors KG developed the study methodology, drafted the manuscript, and oversaw data analysis. ZL and T-LH conducted the systematic review search, article screening, data extraction and data analysis. KL, CZW, SM and JP contributed to the design of the study and provided input into the manuscript.
Funding The authors are funded by the New Frontiers in Research Fund (Grant NFRFR-2019-00009) through an operating grant awarded under the Canadian Institutes of Health Research Rapid Research Funding Opportunity.
Competing interests KL was a member of two donor-funded reviews of WHO in 1995 and 1997. She has previously received funding from WHO to conduct research on global health governance and global tobacco control and review evidence on the impacts of globalisation and infectious diseases. CZW was a member of a WHO guideline development group and technical consultation in 2019.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.