Article Text

Abstract
We finally have a vaccine for the COVID-19 crisis. However, due to the limited numbers of the vaccine, states will have to consider how to prioritise groups who receive the vaccine. In this paper, we argue that the practical implementation of human rights law requires broader consideration of intersectional needs in society and the disproportionate impact that COVID-19 is having on population groups with pre-existing social and medical vulnerabilities. The existing frameworks/mechanisms and proposals for COVID-19 vaccine allocation have shortcomings from a human rights perspective that could be remedied by adopting an intersectional allocative approach. This necessitates that states allocate the first COVID-19 vaccines according to (1) infection risk and severity of pre-existing diseases; (2) social vulnerabilities; and (3) potential financial and social effects of ill health. In line with WHO’s guidelines on universal health coverage, a COVID-19 vaccine allocation strategy that it is more consistent with international human rights law should ensure that vaccines are free at the point of service, give priority to the worst off and be allocated in a transparent, participatory and accountable prioritisation process.
- vaccines
- epidemiology
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
States will continue to be confronted with the ethical issue of how to allocate limited supplies of COVID-19 vaccines that are proven safe and effective as more of them become available.
International human rights law requires that ‘vulnerability’, if used as a criterion for priority access to COVID-19 vaccines, must include social vulnerability (eg, socioeconomic status) in addition to medical vulnerability (eg, comorbidities), and attend to intersectionalities.
National vaccine allocation schemes must address disparities in health risk and adverse health outcomes across systematically disadvantaged groups when determining COVID-19 vaccine priority groups.
Introduction
With over 170 COVID-19 vaccine candidates in clinical trials, and several already authorised for emergency use, the global community is grappling with how to equitably allocate the first available doses of vaccines that are proven safe and effective. Clinicians at all levels of engagement—from global and national health advisors to decision makers in health regions and facilities—are being confronted with this dilemma. We argue that international human rights, which have been ratified and are legally binding on 171 states, can help in resolving this quandary by integrating an intersectional approach to allocation processes.
Current allocation frameworks are inadequate for fully realising the right to health because they overemphasise epidemiological concerns.1 An intersectional approach to the right to health prioritises population groups who experience vulnerability, marginalisation and multiple forms of discrimination. Thus, we argue that vaccine allocation frameworks ought to prioritise the needs of population groups with pre-existing social, health and economic vulnerabilities. We argue that an intersectional human rights approach provides the best mechanism for dealing with overlapping vulnerabilities of deprivation, ethnic diversity and (baseline) health status, as it considers the social determinants of health and the impact of structural inequalities.
In this article, we first briefly map the current approaches to vaccine allocation, before analysing their shortcomings from a human rights perspective. We then argue that human rights principles are vital when allocating scarce healthcare resources and what these principles could entail at the national level for the first doses of a COVID-19 vaccine. Finally, we outline an intersectional model of how this could be achieved, together with some limitations that we foresee in practice.
Existing approaches to COVID-19 vaccine allocation
Four main schemes have been proposed for the equitable allocation of vaccines (see table 1). The first is the COVAX Facility, led by Gavi, the Vaccine Alliance, the WHO and the Coalition for Epidemic Preparedness Innovations, which intends to purchase vaccines for fair distribution across countries.2 At the moment, this scheme does not stipulate how national allocation should take place. The other three schemes are the WHO/SAGE values framework3, the Nuffield Council on Bioethics proposal4 and the Fair Priority Model by Emanuel et al.5 While the WHO/SAGE values framework mentions human rights principles and refers to some of the ‘global equity obligations’ of states with regard to vaccine allocation, we argue that the relevant obligations of states need further emphasis and clarification to assist states to comply with human rights law. Likewise, while the correlation between human rights principles and equitable vaccine allocation has been emphasised by the Nuffield Council on Bioethics, their meaning and potential for practical application have not really been fleshed out. In contrast to these, the Fair Priority Model does not explicitly mention human rights.
Four schemes of vaccine allocation
In addition to these four schemes, some countries have devised different country-level schemes for vaccine allocation (see table 2). The UK has prioritised older people at the expense of other groups, leading for calls to prioritise other key groups such as health workers, nursery workers and teachers,6 whereas in the USA the focus has been on front-line workers. In most jurisdictions, these allocation mechanisms have been sharply criticised. In the UK, for instance, some argued that health workers ought to have been prioritised, and in the USA, there have been allegations that certain groups, such as university or marketing staff in healthcare settings, were prioritised inappropriately.7 The question of overlapping vulnerabilities plagues most national allocation systems. For instance, in the USA, a subgroup of the Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP) developed a five-tier prioritisation scheme, which borrowed interim allocation groups from a previous influenza pandemic vaccination plan. The full ACIP committee raised concerns about the vague nature of the tiers and questioned how the criteria would address race and ethnicity, low-income populations and pregnant women.8
National prioritisation groups as of 22 December 2020
When the H1N1 vaccine was allocated, decisions to prioritise vulnerable groups, such as prisoners and obese people, were met with hostility by some members of the public who were not prioritised for vaccination.9 Public perceptions of fairness in relation to vaccine allocation are likely to be influenced by ‘social and economic inequalities, racially-biased health systems, and a politicized pandemic environment’ in the absence of clear and transparent communication of vaccine allocation processes and the evidence behind them.10
How human rights principles can inform vaccine allocation in pandemic conditions
Early in the COVID-19 pandemic, the United Nations (UN) stipulated that a COVID-19 vaccine ‘should be provided without discrimination’, and acknowledged that ‘the human rights-based approach’ is an ‘effective pathway in the prevention of major public health threats’.11 The higher rates of severe COVID-19 illness and mortality among some systemically disadvantaged populations (eg, Black, Asian, and minority ethnic and Latinx communities, Indigenous people and refugees) provide a compelling case for determining how vulnerabilities are embedded in structural inequities that affect health. Justice requires that disparities in health risk and adverse outcomes across systemically disadvantaged groups be addressed in the collective COVID-19 response, including in the design of vaccine prioritisation schemes.
International human rights law provides a universal framework for advancing global health with justice, transforming moral imperatives into legal entitlements. Box 112 13 Every state has signed at least one human rights treaty and there is empirical evidence that all states have to some extent internalised human rights norms into legislation, policy and governance, even where compliance with such norms is demonstrably lacking.14 15 Here we argue that human rights legal principles have the potential to guide a more equitable allocation of a COVID-19 vaccine.16 A human rights approach reframes commitments as obligations and rights, and imposes accountability measures on states. International human rights law enshrines a range of individual and collective rights related to access to an essential vaccine for pandemic prevention (see Box 2).
Human rights related to access to an essential vaccine for pandemic prevention
Right to health
States should take actions to translate the right to health, as articulated in the International Covenant on Economic, Social and Cultural Rights (ICESCR), into practice.47 For a pandemic vaccine, these steps include making it available in sufficient quantity, and distributing it in priority to people who are more likely to contract COVID-19, those whose health is at higher risk of being seriously compromised by COVID-19 and also those who may be most likely to transmit the virus. This entails ensuring non-discriminatory access to a vaccine.
Right to life
The universal right to life is enshrined in the International Covenant on Civil and Political Rights (ICCPR, Article 6). Its monitoring body, the United Nations Human Rights Committee, has recognised that state obligations under this right extend to ensuring universal access to essential medicines.48
Right to benefit from scientific progress
The right to enjoy the benefits of scientific progress and its applications is enshrined in the International Covenant on Economic Social Cultural Rights (ICESCR) (Article 15). The Committee on Economic Social and Cultural Rights (CESR) has indicated that the ‘right to science’ includes a duty to the equitable distribution of scientific advances, especially for vulnerable and marginalised populations.49
Availability, accessibility, acceptability and quality (AAAQ) explained
According to the highly authoritative interpretation of the right to health in General Comment No 14, a COVID-19 vaccine should be:
Available in sufficient quantity, and in the absence of sufficient quantities, priority should be given to people who are more likely to contract the disease and those whose health is at higher risk of being seriously compromised to it.
Affordable for all.
Distributed so as to be respectful of transparency requirements and key medical ethics concepts, such as patients’ protection, consent and confidentiality.
Safe and of good quality.23
Provided without discrimination, especially to the most vulnerable and marginalised groups. The term vulnerability can be seen as including elderly people, people with comorbidities that predispose them to poorer health outcomes, people in settings like prisons and group homes, marginalised and minority groups, and healthcare workers who are particularly at risk of infection. Equitable distribution within these minimum core obligations has been interpreted to include duties to reduce substantive inequalities such as socioeconomic differences and other forms of disadvantage.50 In the next section, we discuss how an intersectional approach can ensure a more equitable and non-discriminatory distribution under human rights law.
Several vaccines for COVID-19 are already authorised in numerous countries.17 However, most countries will not immediately have the requisite number of vaccines for the entire population and so will have to make decisions about who they should prioritise.18 Article 12 of the International Covenant on Economic, Social and Cultural Rights states that states have obligations to prevent and control epidemics.19 In General Comment No 14, which interprets states’ obligations under the right to health, the UN Committee on Economic, Social and Cultural Rights (CESCR) has stated that the provision of vaccines would be critical to fulfilling this objective.20 (See box 1 for how these rights relate to access to a vaccine for pandemic prevention.) The Committee has also firmly positioned the provision of essential medicines defined by WHO as a ‘core obligation’ under the right to health. Such obligations are defined in General Comment No 3 as the minimum standards that must be met by states to give meaning to the enjoyment of Covenant rights.21–23 Therefore, providing a COVID-19 vaccine would fall within the core minimum obligations of states under the right to health, making it a priority.
Human rights frameworks insist that allocation decisions (including those for vaccines) meet some core minimum thresholds. This has been dubbed the availability, accessibility, acceptability and quality (AAAQ) standard—see box 3. Additionally, the WHO has recently considered the question of prioritisation in the context of universal health coverage.22 Three principles were used which are embedded in the right to health: fair distribution (priority services are based on need and priority is given to the worst-off groups (as discussed under the AAAQ)), cost-effectiveness and fair contribution (contributions based on ability to pay, not need).
Intersectionality and Public Health
What is intersectionality?
Intersectionality is a theoretical framework for understanding how multiple social identities such as race, gender, sexual orientation, socioeconomic status and disability intersect at the micro level of individual experience to reflect interlocking systems of privilege and oppression.51
Intersectionality and public health
Public health scholars are increasingly using intersectionality to conceptualise and address disparities and social inequality in health.52 53
The CESCR’s statements in the early stages of the pandemic, that ‘States must make every effort to mobilize the necessary resources to combat COVID-19 in the most equitable manner, in order to avoid imposing a further economic burden on these marginalized groups’ and that ‘Allocation of resources should prioritize the special needs of these groups’,24 support a human rights-compliant approach to vaccine allocation. General Comment No 3 takes account of state resource constraints in the fulfilment of minimum core obligations. Thus, the issue of prioritisation becomes doubly important if a country’s available resources must be considered, as is the case with most low and middle-income countries. The efficient allocation of available resources necessitates that states consider value for money, meaning that given similar efficacy, states choose the cheapest vaccine available on the market. Given the many varied vaccines being offered at different prices,25 states must ensure that vaccine candidates that have particular expensive requirements (such as refrigeration) should not be prioritised in circumstances where there are poor resource constraints. States also have obligations to pool resources to buy vaccines more cheaply so as to benefit more people (see box 1).
Although human rights law tends to focus on universal access, there have been attempts to use human rights to conceptualise what equitable access ought to look like when resources are limited.26 For instance, in prioritising AIDS funding, scholars have called for an approach based on intersectional vulnerabilities as a way of prioritising how groups are represented and allocated resources.27 This is particularly important where these vulnerabilities are linked to underlying determinants of health.
Using an intersectional approach to consider underlying determinants of health within the human rights regime
Intersectionality has come to shape the practice of UN Human Rights bodies, becoming a ‘major theme within the wider topic of discrimination’ to define and prioritise the most vulnerable and marginalised groups of people.28
In several places, human rights law refers to multiple grounds of discrimination, which have more than an additive effect on individuals, even though the term ‘intersectionality’ is not used explicitly. The Convention on the Rights of the Child contains protections for children with disabilities (Article 23) and refugee children (Article 22), the Convention on the Rights of Persons with Disabilities specifically mentions that women with disabilities are subject to multiple discrimination (Article 6(1)), and the preamble of the Convention on the Elimination of All Forms of Discrimination Against Women (CEDAW) recognises the issues of race and poverty that affect women. In its work on prioritisation for universal health coverage, the WHO also specifically recognises that multiple characteristics based on social practices may help states to prioritise those most in need.29
Additionally, the UN Committees which give normative guidance to the treaties have referred to intersectionality. The CESCR noted that discrimination may occur on ‘multiple grounds’, and in 2016, the CESCR further demonstrated the intersectional nature of underlying determinants of health by highlighting ‘intersectional discrimination’ and ‘intersecting forms of discrimination’.23 The CEDAW, in its General Recommendation No 28 on the Core Obligations of State Parties under Article 2, specifically recognises the intersectional harms on women due to discrimination based on race, ethnicity, religion or belief, health status, age, class, caste, sexual orientation and gender identity.30
The recommendations and statements issued by international human rights bodies in the context of COVID-19 also acknowledge the intersectional effects of the pandemic among vulnerable groups, such as migrants, women, children, people with disabilities, older people and front-line workers.31–35
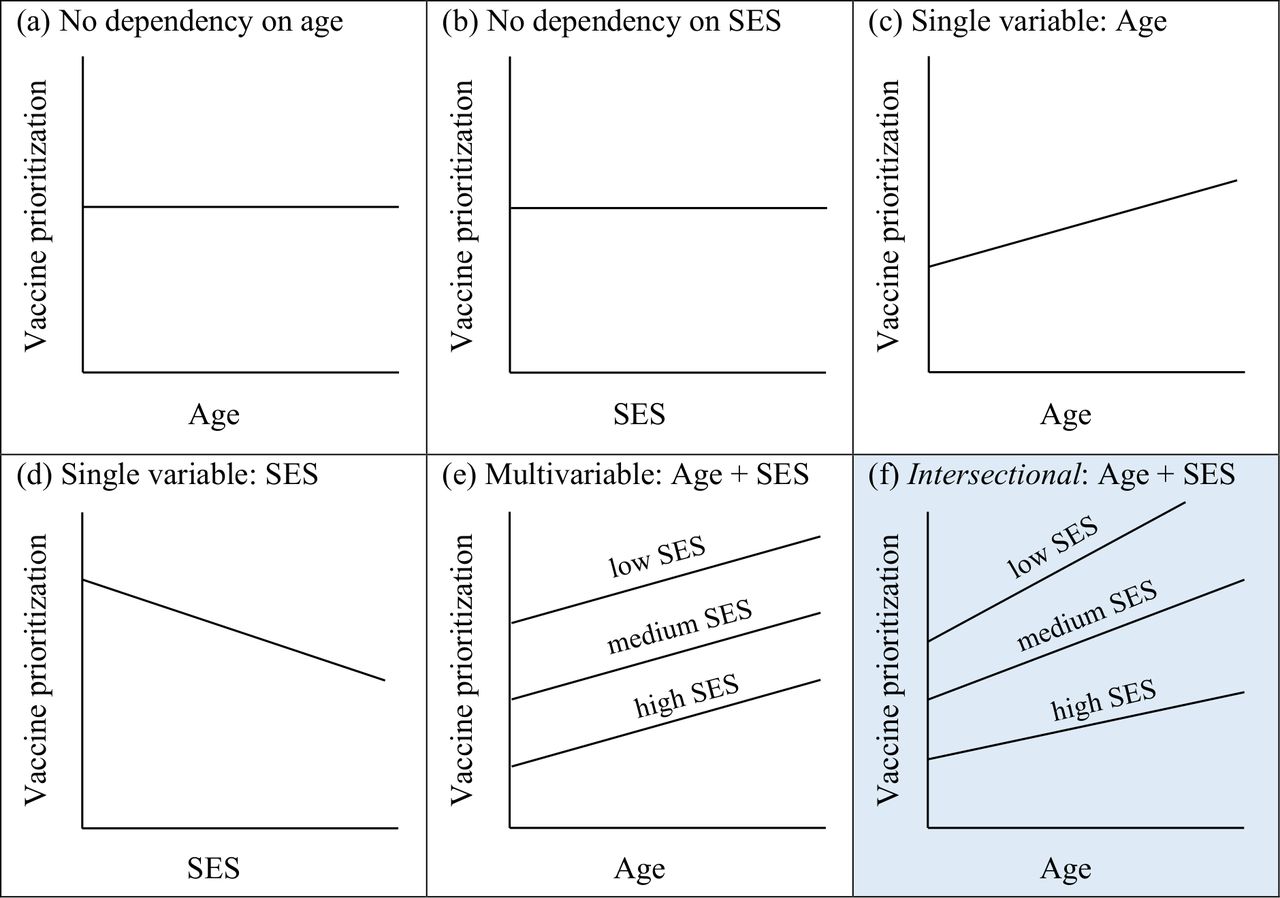
The potential value of an intersectional model is illustrated in figure 1 in the simple case of two demographic variables: age and socioeconomic status (SES). For additional simplicity, in this discussion we treat SES as a three-level variable (low, medium, high), but the argument is the same if SES is measured on a finer scale, or even on a continuous scale, and if more than two variables are included. Similarly, we use linear relationships here to show schematically the general features of the models.
{kind=link}
Six schematic models of vaccine prioritisation. SES, socioeconomic status.
In the simplest possible case (figure 1A,B), neither variable contributes to the model, and vaccine prioritisation is independent of age or SES. In figure 1C,D, we see vaccine prioritisation dependent on each variable separately, with higher age resulting in higher vaccine prioritisation (figure 1C) and lower SES resulting in higher vaccine prioritisation (figure 1D). Figure 1C, in which priority depends only on age, is the current model in use in England. A more sophisticated multivariable model allows both variables (age and SES) to influence vaccine prioritisation. In figure 1E, this is cumulative: the increase in prioritisation from age 50 to 60, for example, is the same, regardless of the SES of the person. Once we have given an increase in priority for being low SES, we operate as though we have taken account of SES, and do not consider it again. However, in an intersectional model, as shown in figure 1F, the variables age and SES interact, meaning that the increase in prioritisation from age 50 to 60, for example, is greater for low SES people than it is for medium SES people. This reflects the way in which being older matters more for a lower SES person than it does for a higher SES person. A low SES person is likely to have a lower life expectancy and is effectively aged beyond their years, due to their relatively greater deprivation, worse access to healthcare, and so on. An intersectional model, as shown in figure 1F, attempts to account for that by increasing the prioritisation for a low SES person as they age beyond what a non-intersectional model would do.
Prioritising COVID-19 vaccines based on intersectional human rights needs
A human rights-inspired focus on intersectional vulnerabilities in vaccine allocation would recognise epidemiological factors as one of the elements of vulnerability but should also include other axes of discrimination that make groups vulnerable.36 This is defined by the WHO as those who are relatively disadvantaged with respect to health prospects, outcomes and SES, and captures the social determinants of health. This approach is emancipatory in that it seeks to improve the health outcomes of these groups in the short term while also aiming to redress underlying health inequities that have contributed to their discrimination in the first place. A human rights intersectional approach would require national actors to prioritise vaccine allocation to minority groups who simultaneously face different kinds of discrimination on the basis of up-to-date and disaggregated civil registration, vital statistics and health data.37 This approach would complement deliberative approaches to bioethical models that apply similar values, but with the added benefit of normativity derived from the human rights framework.
Although some states may be tempted to charge for a vaccine because there is overwhelming need, the COVID-19 vaccine should be free at the point of access. Therefore, states with multitiered insurance schemes should ensure that they work collectively to ensure that those without insurance (eg, migrants) are prioritised as they will be among the categories that fit the intersectional requirements identified above.
People experiencing socioeconomic conditions which make the spread of the contagion more likely should be identified using models which rely on epidemiological markers and on other vulnerabilities due to social determinants of health. The UK model t, for instance, focused only on age at the beginning of the vaccination process, although (see figure 1C and table 2). By additionally including variables such as income, education, occupation, gender, race/ethnicity, which shape specific determinants of health status, vaccine prioritisation frameworks could better conform to the human rights principle of non-discrimination and temper political agendas when decisions to prioritise vulnerable groups for a vaccine are perceived to be unpopular.
In order to make these hard decisions, a human rights approach requires that states pay attention to procedural fairness around how decisions were made. Thus, the process should be transparent, participatory to the greatest extent possible during a crisis and should involve accountability. Allocation decisions (eg, the parameters of an intersectional model, such as the appropriate slopes of the lines) should be accompanied by a transparent national justification for these decisions.38 Given the time constraints, there may be other ways of organising participation, such as involving civil society activists/social justice groups, that would give legitimacy to the process.
Criteria for prioritisation of COVID-19 vaccination
In building a model, we adapt the prioritisation criteria specified by the WHO in achieving universal health coverage, described above.39 We suggest three health-related criteria: increasing vulnerability to infection, social vulnerability that prioritises the worse off and financial and social risk protection (see box 4). We suggest prioritising people or groups who meet multiple criteria. This intersectional stance goes beyond a cumulative prioritisation (ie, adding a fixed number of points for each additional category), as we illustrated in figure 1E,F. In order to do this, decisions would have to be made about the levels of disadvantage due to the intersectional harms that individuals face within different country settings, requiring greater representation and transparency about the decision-making processes.
Criteria for prioritisation of COVID-19 vaccination*
Infection risk and severity of disease criteria: criteria related to individual health-related risk factors
Comorbidities.
Age.
Disability.
Criteria related to social vulnerabilities: criteria related to sociodemographic factors increasing the vulnerability
Socioeconomic status.
High-risk occupation: for example, healthcare workers, other front-line staff, delivery workers, garbage collection workers.
Housing and living conditions: for example, crowded places, limited access to clean water and sanitation facilities.
Place where one lives: for example, prisons, group homes for people with disabilities, homeless people, nursing homes or longer term care facilities, refugee settlements.
Gender, race, ethnicity, religion and sexual orientation-related factors that lead to stigma and limit access to healthcare.
Criteria related to protection against the financial and social effects of ill health
Caring responsibilities.
Catastrophic health and other expenditures if individuals get infected.
*The criteria are based on the analysis by Norheim et al40.
Adopting an intersectional human rights approach to vaccine prioritisation: the challenges
As seen in figure 1, an intersectional human rights prioritisation process would be more administratively complex and more expensive to run than a system that relies on single variables, and such a process might be slower. Adopting an intersectional approach would also involve making concrete distinctions about some vague concepts, such as race or ethnicity. Due to the intersecting nature of many social variables, intersectional categories are not always clear-cut, and states may struggle to identify people who do not fall neatly into set categories. There would also be incentives for privileged people to try to game the system so as increase their prioritisation, but this problem exists with any model, as older people, for instance, can move to countries which prioritise age more. (See box 4)
Creating models for prioritisation may be complex, given that most public health statistical methods have not been intersectional. Some scholars recognise that while existing statistical methods of analysing social data may pose a methodological challenge, given the ‘complex tenets of intersectionality’, and ‘more qualitative methodologies are critically needed’ to address such complexity, it is not necessary for public health scholars and policymakers to wait for such challenges to be resolved prior to incorporating intersectionality into public health interventions.40 41 Additionally, transparent and participatory approaches which involve individuals and experts who have studied those social categories can help states to determine priority categorisations. We recognise that participation with all affected groups may not be possible, but human rights regimes have a long tradition of using civil society organisations and cross-sectional representation to engender participation.
Politically, an intersectional approach which prioritises minority groups may be unpopular with some. However, as the proponents of intersectionality argue, it was always meant to be a political project, and if it is grounded in a human rights approach, using the best scientific evidence and making attempts at redistribution, courts will struggle to overturn decision-making processes that are procedurally correct. This approach, which deals with historically oppressed or marginalised populations, could be used as a springboard to facilitate and inform the development of other health interventions. As we have seen from the COVID-19 crisis, health outcomes are interlinked with social vulnerabilities, because we rely on the most socially vulnerable groups to run our economies. Thus, adopting an intersectional human rights approach to COVID-19 vaccine allocation would be an opportunity to shape a more just and equitable society.
References
Footnotes
Handling editor Seye Abimbola
Twitter @sharifasekalala, @lforman, @maxwellsmith
Contributors SS conceived and led the writing of study and each of the other coauthors contributed to the framing and writing of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are include in the article.