Article Text

Statistics from Altmetric.com
Summary box
The COVID-19 pandemic has exposed weaknesses of the Indian health system, highlighting the urgency of fundamental reforms.
There is a need to conceptualise health system reforms in a multidimensional way keeping complementarity across levels of government.
An adaptive governance framework that relies on shared accountability while reconciling varying levels of flexibility across three dimensions—operational processes, institutional linkages and health system values, is the way to build a resilient health system in India.
We identify three reforms as illustrative examples of how a process of continuous consultation, coordination and collaboration across central, state (provincial) and local levels of government, with an underlying adaptive governance logic ought to be driving these reforms.
The reforms include an integrated national health data system, improving purchasing and regulation of the private sector and intersectoral delivery of health services.
We identify the operational processes associated with each of these reforms that are delivered through interlocking institutional mechanisms and unified by a common understanding of the values underlying them across all levels of government.
Introduction
Crisis as an opportunity for change has been part of historical and development literature and is an oft-repeated theme. The Chinese word for crisis (危機), for example, consists of two symbols often characterised in popular literature as denoting ‘danger’ and ‘opportunity’.1 For India’s healthcare system, the COVID-19 crisis has highlighted the urgency of reform. We have learnt that no matter how long or how stringent a lockdown is, we cannot flatten the curve effectively, nor fairly, without a robust health system. In the pre-COVID-19 world, practitioners and policy-makers were gathering around the Universal Health Coverage (UHC) agenda that sought to expand the number of health services provided to the largest number of beneficiaries at the cheapest possible cost, constituting the three dimensions of UHC.2 This pandemic has made it clear that incremental progress along those three dimensions while necessary, is insufficient to move towards a health system that is responsive, resilient and fair.
India’s health system is highly heterogeneous and fragmented with multiple agencies at central and provincial levels governing various aspects of health policy-making and service delivery.3 Public expenditure on health remains among the lowest making up just over 1% of gross domestic product (GDP). Public health governance, therefore, remains underdeveloped and relatively neglected among both researchers and practitioners. In this article, we make a case for an adaptive governance approach that actively embraces multidimensionality with respect to health system reforms in India, taking into account simultaneous technical and political engagement at central, state (provincial) and local government levels.
Locus of change: central, state and local
Among the core elements of a strong health system ought to be an ability to leverage the strengths at different levels and complement them in responding to a crisis. Typically, higher levels of the system are geared towards strategic functions, while the lower levels (closer to people) are organised for operational functions. The constitution of India lists health under the jurisdiction of the provincial governments.4 The provinces (states) are, thus, responsible for priority-setting and organisation of health services. However, the central government continues to play a substantial role in policy-making and resource provision as well as regulating information flow and research. The administration of health facilities and community engagement are usually the domain of district and subdistrict agencies. At the grassroots, frontline workers are called on to deliver a range of services tailored to local needs and capacity. The burden of adapting vertically flowing instructions and administrative logic into a people-centred service logic, thus, falls disproportionately on the frontline workers. Between these levels of government there are glaring gaps which the pandemic has exposed, placing the burden of delivering an essentially top-down stream of services, onto the lower levels.5 6 However, local governments at subdistrict levels lack resources and capacity to plug the gaps. Further, priorities at higher levels of government can seem disconnected to operational realities on the ground in the absence of active coordination and feedback.
Towards change frameworks that prioritise adaptiveness
At the heart of improving our ability to face crises is adaptiveness; how can we improve governance at multiple levels of our health system, while being mindful of expected and unexpected impacts of such changes.7 Adaptive governance frameworks were originally posited by Eleanor Ostrom and applied to the governance of ‘common pool resources’ and since then have been gaining prominence in the context of social-ecological systems, particularly natural disasters and climate change.8 Adaptiveness here is an emergent property, arising out of the interactions between self-governing networks. Hill and Hupe develop this further in their multi-level governance framework for implementation of social policies.9 Literature on health systems governance has moved from government-led institutionalism towards theories emphasising principal-agent relationships.10 11 More recent adaptive governance frameworks such as Abimbola et al12 apply a multilevel adaptive framework to analyse primary healthcare governance in low and middle-income countries (LMICs). Here, we posit a novel framework that draws from the idea of adaptiveness but situates it within a multilevel framework that emphasises the need for legitimate institutions and processes for feedback on strategic, tactical and operational aspects.
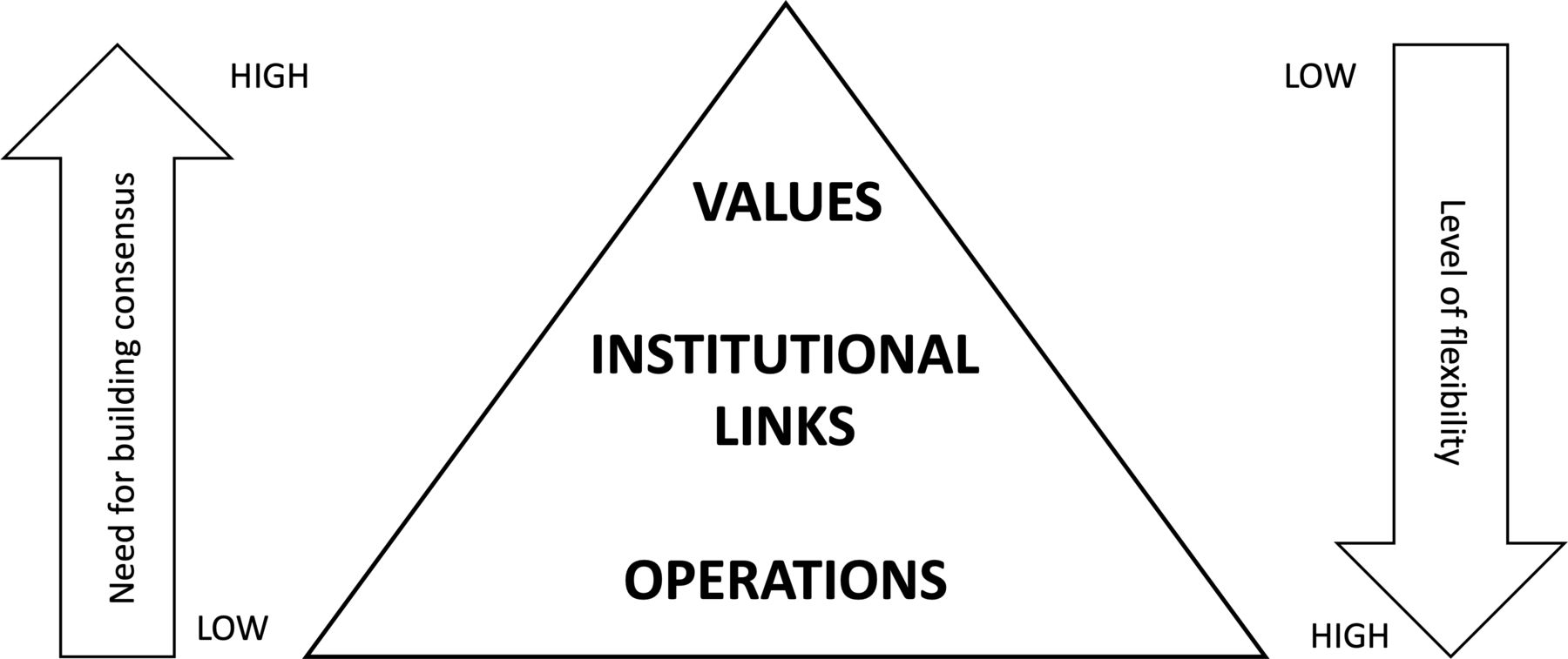
We envision the health system as having shared accountability across the levels of government along three interconnected dimensions (figure 1). The first and most visible are the operational aspects that enable the delivery of health services. The second dimension constitute the institutional linkages that exist across and within each level of government and determine how health is delivered. The third dimension and of the highest order are the values that determine the choices made at all levels about what constitutes good health, how it is to be delivered and by whom. This adaptive governance approach recognises the need for constant negotiations across the levels of government along these dimensions such that there is a high degree of flexibility at local implementation levels, bound together by a coherent set of values.
{kind=link}
Adaptive governance pyramid. An adaptive governance approach in a multilevel health system rests on linkages and feedback along three hierarchical dimensions of operational processes, institutional linking mechanisms and values underlying decision making. Adaptiveness requires deliberate, ongoing negotiation and consultation such that increasing operational flexibility is available to local governments while ensuring greater consensus around values and principles of the health system.
We illustrate adaptiveness through examining three important post-COVID-19 reform agendas for India’s health system from a lens of interconnectedness of different levels of government, the linkages and feedback among them. The implementation approach for each of the reforms requires an adaptive governance approach that acknowledges, facilitates and engages with government and other institutions at all levels and scales (table 1). This is neither a top-down nor a bottom-up approach; instead distributing constituent functions but unified based on a common pool of values and expected outcomes. The three examples we use to illustrate our framework are reforms of national importance in India. They apply not just to one setting or any one level of government but to all although with distributed accountability. Further, the three proposed reforms are themselves interdependent such that progress along these fronts can mutually reinforce (or hinder) each other.
Examples of values, institutional linking mechanisms and operational processes for each of the proposed reforms for the Indian health system
Favouring fairness over markets in a mixed pluralist health system
While price regulation of commodities is typically seen from a macroeconomics lens, when it comes to pricing of medicines, vaccines and health technologies this lens is inappropriate, and unjust as it aggravates inequalities in a system where out-of-pocket expenditure on healthcare is already driving impoverishment among the poorest.13 The pricing of diagnostic and treatment packages in the private sector in particular emerged as a major point of contention during the pandemic. Following news reports of price-gouging, India’s drug-price regulator issued an advisory about the prices of hand sanitisers and surgical masks.14 15 The Supreme Court of India also stepped in at various points to advise on treatment of patients in the private sector.16 However, the pricing and usage of personal protective equipment, N95 masks, face shields in healthcare facilities remains largely unregulated. Reports on the ground have demonstrated how hospitals used this lack of regulation to overcharge patients.17
The majority of India’s curative healthcare services is in the private sector. The public sector provides only about 30% of all healthcare in India.18 The rest is provided by a mix of private for-profit hospitals, charitable hospitals, individual private doctors and informal care providers. Thus, the private healthcare providers are an indispensable part of India’s health service provision and need to be effectively and efficiently integrated.
The Clinical Establishments’ Act of 201019 was meant to allow the government to accurately enumerate health facilities, keep track of the quality and availability of health services across the country as well as provide a framework for their regulation. Several state governments have promulgated their own versions of this law with provisions for data sharing and price control. The private sector vigorously resisted the legislation both at the national and state levels resulting in the dilution of several provisions, especially with regard to price control.20 21 The private sector resistance combined with the lack of regulatory capacity among the government cadres has led to very poor implementation of the policy.
In addition to weaknesses as a regulator, states also lack the capacity to be an effective purchaser. Even as most states have set up some version of the national health insurance scheme—the Pradhan Mantri Jan Arogya Yojana (PMJAY), it is only applicable to hospitalised care. Less than 1% of COVID-19 patients claimed cashless treatment under PMJAY across the country, which empanels both private and public sector hospitals.22 In any case the majority of COVID-19 cases do not require hospitalisation and there are no purchasing arrangements for outpatient treatment from the private sector.
While the National Health Authority that runs the PMJAY has made considerable strides in supporting purchasing decisions, it needs to reflect India’s federal character much more closely and be more integrated with preventive and primary health services. State governments need to invest more in needs and capacity assessments for their own jurisdictions through inputs from local public health authorities, civil society partners and private health providers. While leveraging the technical inputs and negotiating power provided by national health authorities, states can focus on building a professional workforce with the technical capacity to adapt and refine guidelines, policies and processes to the local context.
The final arbiter of whether and how to implement a given programme or policy is up to officers, at district and subdistrict administrations, and to others further down the hierarchy.23 Local administrators, thus, have to be involved in the process of defining regulatory and purchasing parameters with feedback from community-level stakeholders. Implementing officers need to be empowered through institutional support while governmental actions acquire legitimacy and local ownership through continuous community engagement.
Integrated national health data system
The pandemic response has seen the proliferation of COVID-19 dashboards to collate and visualise data. The public availability of these dashboards has provided transparency and leveraging of expertise outside government to inform health decision-making. These lessons are also applicable to other health conditions and functions of the health system.
Health data collection and management in the country currently, like in many LMICs, is grossly inadequate and largely unreliable. National health data are fragmented, often not validated and can often vary substantially in quality across different regions of the country.24 Apart from significantly hampering research, the lack of a robust health data system forces arbitrary and intuitive decision-making. One of the major trade-offs in this kind of decision making is equity; those individuals and populations for which data is either poor or unavailable, thus contributing to an ‘invisibilisation’ of the problem by the system.25 Health services utilisation reported by a multispecialty private hospital in a large urban centre, for example, is likely to be very different from the health needs of a low-income rural population or a health facility with relatively low levels of educated or insured patients.
Among the structural reasons is the differences in the systems of data management, followed by various stakeholders. Even within the government system, different pieces of data may be held by different offices with limited resolution and disaggregation possibilities, providing only a partial picture, making it virtually useless for policy-making or research. Much of this data is also not transparent and difficult to access, despite data accessibility initiatives in place.26 These underlying problems were illustrated even for COVID-19,27 despite close monitoring in real-time by decision-makers, experts and the lay public. While many of these appear to be technical problems, underlying their pervasiveness within the system is an apathy and a lack of a data culture pertaining to public services.
There is, thus, an urgent need for a unified public health data system across all schemes/programmes, from all states and private healthcare facilities. The National Digital Health mission (NDHM), announced by the Prime Minister is a step in this direction.28 It envisages a unique health ID for every citizen that can help track service usage across an individual’s lifetime and allow interoperability across various producers and users of healthcare data. While the current NDHM seems to largely target population health record, a unified national health data system should ideally have a much larger mandate.
Health machineries should move to incorporate the shift in thinking on health from a purely biomedical function to a complex outcome resulting from an interplay of physiological, environmental and sociological factors. Thus, the kinds of data being collected should be expanded to include socioeconomic parameters and environmental factors that we now know are determinants of health. In the section below, we suggest a new intersectoral institutional architecture to facilitate this kind of data collection and management. Rather than envisaging health data as a digital ecosystem for actors within the healthcare industry such as insurance providers, hospitals and pharmacies, the data system ought to facilitate better local decision making and improve equitable access to health.
The central government can anchor such an effort by pushing for standardisation of processes. The data protection laws on privacy, confidentiality, access and localisation of health data that have been in draft stages need to be legislated and implemented on a priority basis.24 State governments will have to identify state-level priorities as well as establish norms around processes of data collection and usage. Healthcare workers will require ongoing training in data management. Additional rigorous quality control measures at various levels of information-flow may be incorporated. Understanding and expertise at local levels of how, why and when e-health services are accessed in their respective contexts needs to be incorporated in the design of the health information system.
Intersectoral preventive public health system
As has often been said, COVID-19 was not just a public health crisis, but also a humanitarian crisis. It demonstrated the impact of health on our livelihood, nutrition, economy and the environment, underscoring the intersectoral nature of the issue. The response in turn has aimed for sectoral convergence, proactive cooperation by the private sector and civil society as well as large-scale community mobilisation for preventive health. These lessons are also applicable to other issues such as air pollution, malnutrition and climate change.
Health services on the ground are in fact part of an intersectoral matrix of social services that mutually reinforce each other to meet the felt needs of the citizen. Frontline health workers are routinely called on to coordinate with self-help groups, political functionaries and others that are outside the purview of the health department. District health authorities similarly carry out planning processes in coordination with the district magistrate whose mandate is multisectoral and spanning beyond health. The systemic processes for coordinating these intersectoral functions however are not institutionalised.
Past zoonotic disease outbreaks such as Nipah virus outbreak and the Kyasanur Forest Disease outbreak have also highlighted the dire need for integrative approaches on ground such as OneHealth and intersectoral action for health.29 Dealing with India’s current health challenges as well as long-term health system preparedness and resilience can only be achieved through prioritisation of intersectoral outcomes and processes at national, regional, state, district and subdistrict levels.
The current institutional system consisting of technocrats managing vertical disease control programmes is not well suited to the kind of intersectoral convergence necessary for long-term preparedness. Initiatives such as the nutrition programmes involving convergence between departments of women and child development and health have found some success but challenges of communication, data sharing, inadequate resource allocation, trust and accountability persist.30 31
Therefore, the first step would be to achieve an architectural change in how a ministry of public health ought to function (as opposed to how the current ministry of health and family welfare is conceived). The central government should support augmentation of existing health ministries with an integrated public health department with exclusive focus on disease prevention and health promotion. The functions of the new integrated public health department would be (1) conducting routine, large-scale public health surveillance, (2) systematic data analysis and impact assessments for decision support and (3) intradepartmental and interdepartmental coordination across the government. This integrated public health department would have to actively recruit field epidemiologists, entomologists, animal health experts, microbiologists, ecologists, sanitation engineers and others to ensure a multidisciplinary approach to preparedness because we cannot predict what the nature of the next public health crisis will be.
The existing integrated disease surveillance project allows for outbreak reporting from the ground-up but has been limited due to poor human resource capacity, infrastructure limitations and has not been meaningfully used.32 33 Preparedness and response to crises like COVID-19 or indeed climate change will also require real-time analysis of data as well as translation into relevant policy input. This is where a multidisciplinary team within the public health department can help to analyse the data into meaningful policy support at local levels. These analyses could contribute to decentralised decision making on district health infrastructure planning, human resource training, intersectoral coordination.
Reconciling value underlying policy-making
Instead of a hierarchical government structure flowing from central to local levels, we envision a series of interlocking institutions at each of these levels of government. This implies a commonality of normative values underlying policy-making at all levels. A national health information system that conflicts with policy goals of state governments or fails to take into account cultural imperatives of local government will find limited utility even if it vastly improves efficiency or effectiveness for some functions. Similarly, local health authorities cannot deliver integrated social services without explicit buy-in and ownership of intersectoral processes at higher levels of government. These reforms need to share not just operational linkages but also feedback around values and principles. In other words, health system reforms require ongoing negotiation around both the ‘means’ and the ‘ends’ of policy-making.
The COVID-19 crisis should enable a coalescing around broad ideals of equity and resilience across the health system. We recognise, however, that these broad philosophical imperatives may translate into differing principles and practical judgements about what needs to be done (table 1). This is particularly true given the diversity of stakeholder interests both within and outside government who influence policy-making at all levels. A complex health system such as India’s has inherent tensions that need to be proactively embraced for sustainable reform. An adaptive governance framework accommodates differences in principles and judgements between actors within and across levels of government, through a continuous process of negotiation and reflectiveness. Operational processes on the ground as well as cross-cutting institutional structures provide the channels for this negotiation.
Conclusion
The pandemic response necessitated increased operational decentralisation around testing, containment, treatment, as well as other non-health-related social and economic decision making.34 This trend needs to be reinforced with greater autonomy, consultation, cooperation and coordination among different level actors. Instead national reform initiatives so far seem to have perversely moved away from principles of cooperative federalism.35 Transformative reform can only be sustainable through active collaboration across all levels of government. Centralised governance cannot account for the complexity of a health system as large as India and rarely provides effective solutions for highly contextualised situations as illustrated by the COVID-19 crisis. Adaptive governance delivered through a multidimensional, integrated health system and agenda setting starting at the lowest level possible is the way to overcome this and future crises.
Data availability statement
Data sharing is not applicable as no data was generated or analysed in the current commentary.
Ethics statements
Patient consent for publication
Acknowledgments
We would like to acknowledge helpful comments and inputs from colleagues at the Institute of Public Health, Bengaluru, Seye Abimbola and the anonymous reviewer for their suggestions on improving the draft.
Footnotes
Handling editor Seye Abimbola
Twitter @NeethiVR, @prashanthns, @dr_hebbar
Contributors NVR wrote the first draft of the document. NSP and PBH provided inputs and helped revise the draft. All authors read and approved the final version.
Funding NVR would like to acknowledge Azim Premji University, Bangalore for supporting her time contributions. NSP’s time contributions were supported by the DBT/Wellcome Trust India Alliance Fellowship to him (IA/CPHI/16/1/502648). PBH’s time contributions were supported by the DBT/Wellcome Trust India Alliance Fellowship awarded to her [IA/ CPHE/17/1/503338].
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.