Article Text

Abstract
Introduction Conditional economic incentives are shown to promote medication adherence across a range of health conditions and settings; however, any long-term harms or benefits from these time-limited interventions remain largely unevaluated. We assessed 2–3 years outcomes from a 6-month incentive programme in Tanzania that originally improved short-term retention in HIV care and medication possession.
Methods We traced former participants in a 2013–2016 trial, which randomised 800 food-insecure adults starting HIV treatment at three clinics to receive either usual care (control) or up to 6 months of cash or food transfers (~US$11/month) contingent on timely attendance at monthly clinic appointments. The primary intention-to-treat analysis estimated 24-month and 36-month marginal risk differences (RD) between incentive and control groups for retention in care and all-cause mortality, using multiple imputation for a minority of missing outcomes. We also estimated mortality HRs from time-stratified Cox regression.
Results From 3 March 2018 to 19 September 2019, we determined 36-month retention and mortality statuses for 737 (92%) and 700 (88%) participants, respectively. Overall, approximately 660 (83%) participants were in care at 36 months while 43 (5%) had died. There were no differences between groups in retention at 24 months (86.5% intervention vs 84.4% control, RD 2.1, 95% CI −5.2 to 9.3) or 36 months (83.3% vs 77.8%, RD 5.6, –2.7 to 13.8), nor in mortality at either time point. The intervention group had a lower rate of death during the first 18 months (HR 0.27, 95% CI 0.10 to 0.74); mortality was similar thereafter (HR 1.13, 95% CI 0.33 to 3.79).
Conclusion These findings confirm that incentives are a safe and effective tool to promote short-term adherence and potentially avert early deaths at the critical time of HIV treatment initiation. Complementary strategies are recommended to sustain lifelong retention in HIV care.
Trial registration number NCT01957917
- HIV
- treatment
- randomised control trial
- health services research
- epidemiology
Data availability statement
Data are available on reasonable request. Deidentified participant data, which were collected for the study, will be made available after obtaining relevant institutional research ethics board approval of a proposal and providing a signed data access agreement that can be obtained from SIM.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Clinic-based conditional economic incentives are a proven short-term strategy for bolstering global HIV treatment targets, including retention in HIV care and adherence to antiretroviral therapy (ART).
In a previously conducted randomised controlled trial of 800 adults starting ART in Tanzania, we found that a 6-month cash and food incentive programme improved retention in HIV care for up to 6 months after the programme ended.
No previous studies have assessed longer-term effects of incentivising retention in HIV care, however, theoretical concerns suggest potential negative effects after incentives are withdrawn because of a ‘crowding out’ of intrinsic motivation to engage in care.
What are the new findings?
After following up with participants in the previous trial of a 6-month cash and food transfer programme in Tanzania, we found no effects—either positive or negative—of the incentives on retention in HIV care at 2 or 3 years.
Individuals allocated to the incentive programme had a lower mortality rate than the control group for up to a year after the programme ended.
What do the new findings imply?
These findings support the use of short-term incentives as a simple, effective and low-cost intervention to support individuals through the critical first months of HIV treatment.
Complementary strategies are recommended to sustain long-term retention in HIV care.
Introduction
Conditional economic incentives such as cash and in-kind transfers have shown success at improving healthcare utilisation and health outcomes across a variety of domains, from maternal and child health to chronic disease management.1 While influential examples include national cash transfer programmes that provide large, sustained incentives for engaging in various health and education services,2 much of the incentive literature evaluates discrete interventions that offer smaller, short-term incentives targeting specific health behaviours and outcomes. An increasingly common use of incentives focuses on medication adherence, a global challenge that threatens treatment success and contributes to increased healthcare costs.3 Incentive strategies for medication adherence show short-term effectiveness across a range of conditions, including substance abuse, tuberculosis, HIV and stroke prevention.4 5 However, few such studies measure outcomes beyond the end of the intervention period, leaving uncertainty around the potential long-term harms or benefits of short-term incentives.
In the context of HIV, medication adherence poses a critical challenge offering a high reward. Efficacious, widely available treatment for HIV with antiretroviral therapy (ART) can enable individuals to lead long and healthy lives, while also preventing transmission, thereby offering an end to the HIV epidemic.6 However, these benefits rely on lifelong retention in HIV care and adherence to ART, a difficult undertaking especially considering the myriad socioeconomic barriers commonly faced by people living with HIV. Well-known obstacles include poverty, food insecurity and stigma; and the direct and indirect costs of visiting the clinic for regular check-ups and medication refills, including transportation and missed work.7 8 Short-term incentives are shown to bolster retention in care and ART adherence in low-income and middle-income countries (LMICs), which shoulder the greatest burden of HIV, and have been recommended by the Joint United Nations Programme on HIV/AIDS (UNAIDS).8–11 Still, to our knowledge, no studies in LMICs have evaluated long-term effects of incentives for engagement in HIV treatment. Across the broader literature on incentives for medication adherence, the rare examinations of long-term results indicate diminishing benefits after incentives end, but no evidence of eventual harm.5 Incentives for other outcomes such as HIV prevention, smoking cessation and education have found mixed results in terms of sustainable benefits, again with limited evidence of negative outcomes; however, most incentive studies have not gone beyond 12 months of postintervention follow-up.11–13
To better understand the effectiveness of conditional economic incentives for improving global HIV treatment targets, we sought to determine long-term outcomes from a previously conducted study of cash and food incentives for individuals starting HIV treatment in Tanzania. Compared with a control group that received usual care, the original trial (2013–2016) found that both types of incentives substantially improved retention in care and medication possession during the 6-month incentive period, with smaller effects persisting 6 months after the incentives ended.9 This study followed up with the original study participants to evaluate 2–3 years effects of the incentive programme on retention in care and mortality.
Methods
Study design
We evaluated 24-month and 36-month outcomes for a three-arm parallel-group randomised controlled trial that was conducted from 2013 to 2016 at three HIV primary care facilities in Shinyanga Region, Tanzania. The study procedures have been previously described in detail within the published protocol and results from the original trial.9 14 The present follow-up study was preregistered as an extension of the original trial (ClinicalTrials.gov, NCT03351556), and here we report the study according to Consolidated Standards of Reporting Trials 2010 guidelines.15
Participants
Study participants in the original trial were recruited from the population seeking care at three HIV primary care clinics. Eligible individuals met the following inclusion criteria: (1) ≥18 years old; (2) living with HIV infection; (3) initiated ART ≤90 days before and (4) food insecure, according to the Household Hunger Scale16; participants provided written informed consent. This study followed up with the same participants.
Randomisation and masking
The original trial individually randomised participants in a 1:3:3 allocation ratio to receive usual HIV care provided by the health facilities (control) or to additionally receive a monthly incentive for up to 6 months, conditional on visit attendance, in one of two forms: a food basket (12 kg maize meal, 3 kg groundnuts and 3 kg beans) or an equivalently valued cash transfer (TZS22 500≈US$11). Site-stratified random assignment was conducted by research assistants using opaque sealed envelopes in randomly permuted blocks (7, 14 or 21) generated by the investigators. There was no masking of intervention arm after assignment.
Procedures
All participants received standard clinical care as provided by the health facilities, both during the 6-month intervention and thereafter. Following national guidelines for individuals starting ART, participants were directed to visit the clinic on a monthly basis for clinical evaluation and medication dispensing, including antiretroviral drugs to treat HIV.17 Along with this usual care, participants in the two intervention arms could receive food or cash transfers once per month—conditional on timely attendance at a scheduled clinic visit (within ±4 days)—during the six consecutive months following trial enrolment. Participants could receive up to six transfers, for a maximum total value of TZS135 000 (≈US$66). This value was selected to prevent undue coercion and be comparable to the Tanzania Social Action Fund national social protection programme; it was somewhat larger than a previous trial in the Democratic Republic of Congo that offered US$5 cash incentives (increasing in value by US$1 on each visit) to pregnant women living with HIV, which found improved retention at 6 weeks post partum but not ART adherence or viral suppression.18 A more recent trial in Tanzania has also demonstrated the effectiveness of the monthly TZS22 500 TZS cash incentive at improving 6-month retention and viral suppression compared with the standard of care.10
For the present follow-up study, after 36 months had elapsed since original enrolment in the trial, research assistants worked with clinic staff to trace all former participants, re-enrol them in the study, and measure long-term HIV care outcomes. Tracing procedures followed the US President’s Emergency Plan for AIDS Relief (PEPFAR) guidelines,19 using phone calls, engagement with community health workers who conduct routine tracing, and triangulation with other facilities (online supplemental figure 1). First, the last known status for each participant was abstracted from medical records at the original facilities. Individuals confirmed to be in care at the original facility or another facility within Shinyanga region were approached by research assistants during a scheduled clinic visit, after clinic staff obtained the individual’s permission for study contact. If an individual’s medical record specified an out-of-region transfer or that the most recent scheduled appointment was missed, clinic staff attempted to call or text; those who could not be reached by phone were referred to community health workers for tracing. Given successful tracing and agreement to be contacted by study staff, research assistants scheduled either an in-person meeting at a location preferred by the individual (home, community location or clinic) or a phone call if the individual no longer lived within the region.
Supplemental material
Efforts to trace each participant continued until successful location or the conclusion of ‘exhaustive’ tracing efforts as defined by PEPFAR (≥3 attempts using at least two tracing methods). After contacting former participants, research assistants confirmed each individual’s identity and participation in the original trial, obtained consent to participate in the follow-up study, completed an interview, and abstracted all available medical records from facilities attended since starting ART. In-person written informed consent was obtained for contacted individuals who were still living within Shinyanga region; verbal consent was obtained over the phone for individuals who had moved out of the region; and a waiver of informed consent to access medical records applied to individuals found to be deceased or who could not be located after exhaustive tracing (as defined above).
All interviews were conducted in Kiswahili and collected information about experiences and preferences regarding HIV care along with socio-demographic characteristics. Clinical visit and appointment dates, medication dispensing and other routinely collected HIV care data were abstracted from all available facility and individual-held medical records, including both electronic and paper-based records.
Outcomes
The primary prespecified outcome was retention in care, measured by clinic attendance records at 24 and 36 months after enrolment. Following the same outcome definition used in the original study, individuals considered lost to care included those who died, disengaged from care or had no evidence of care for ≥90 days after a missed appointment as of 24 and 36 months.9 19 As recommended by PEPFAR, participants who could not be found after exhaustive tracing efforts were classified as lost to care.19 However, we conservatively considered retention to be missing for former participants whose last known status indicated a transfer that we were unable to verify (ie, complete medical records from the facility could not be accessed, primarily in the case of out-of-region facilities as these were not visited in-person).
All-cause mortality, a component of retention, was assessed as a secondary outcome at 24 and 36 months and in a time-to-event analysis. Mortality status and date of death were obtained through medical records or contact with family members during tracing. While we also intended to evaluate adherence to ART using the medication possession ratio over 12–36 months, this was deemed infeasible due to often incomplete medication dispensing records obtained at follow-up.
Statistical analysis
Sample size was determined for the original trial.9 For the follow-up study, we first conducted descriptive analyses regarding participant mobility and continuity of care over time, as crucial and often poorly understood aspects of retention in HIV care. This included summarising survey responses about moving and distance-related clinic preferences, the proportions attending their original facility versus new facilities at follow-up, and the frequency of out-of-region transfers.
The primary analysis followed the same methods as in the pre-specified analysis of the original trial.9 14 We conducted an intention-to-treat analysis to evaluate the primary outcome of retention in care and the secondary outcome of mortality at 24 and 36 months. Using predicted probabilities from logistic regression models, outcomes were expressed as marginal mean differences between the combined incentive and control groups with 95% CIs.20 21 We controlled only for enrolment site in the primary analyses to account for stratified randomisation.
In secondary analyses, we additionally adjusted for baseline characteristics including age, sex, and characteristics that were imbalanced at baseline of the original trial (WHO clinical stage, occupation and language).9 We also examined effects disaggregated by incentive type (cash vs control, food vs control and food vs cash). In addition, we explored effect heterogeneity across the same subgroups as in an analysis of the original trial results (sex, age, wealth index and treatment delay between HIV diagnosis and ART initiation) with a Wald test of the interaction term at alpha=0.20, while expecting these analyses to be underpowered.22
Lastly, we examined the effect of incentives on time to all-cause mortality. We used an unadjusted Kaplan-Meier plot stratified by study group and a Cox proportional hazards model to compare the relative mortality rates by group. The Cox model was adjusted for clinic, as in the primary analysis. We also added a time interaction after detecting evidence of a proportional-hazards violation (Schoenfeld residuals p=0.006), using two equal 18-month time periods (0–18 months, 18–36 months) to satisfy the proportional-hazards assumption. As such, we reported HRs by time interval.
The primary intention-to-treat analyses of effect estimates at 24 and 36 months included all randomised participants. We used multiple imputation to estimate retention in care and mortality for participants who were missing values for each outcome. This approach incorporates uncertainty about the missing data by creating numerous plausible imputed datasets and then combining results from each. We implemented sequential multiple imputation with 20 iterations separately for intervention and control arms using logistic models, including the same fully observed predictors used for this purpose in a similar trial (clinic, age, sex and WHO clinical stage).10 Parameter estimates were combined according to Rubin’s rules.23 24 As a sensitivity analysis, we also report complete-case estimates for all outcomes (excluding participants with missing data). For the survival analysis, individuals missing 36-month mortality status were instead censored at the date last known to be alive. All statistical analyses were conducted using Stata V.14.
Patient and public involvement
We worked closely with government, health facility and community stakeholders during the trial design process to ensure that the intervention amount was appropriate, unlikely to be coercive and yet likely to be effective to change the desired health outcomes.14 Postintervention feedback was also collected from patients and used in designing subsequent trials.10 25 26
Results
Descriptive findings
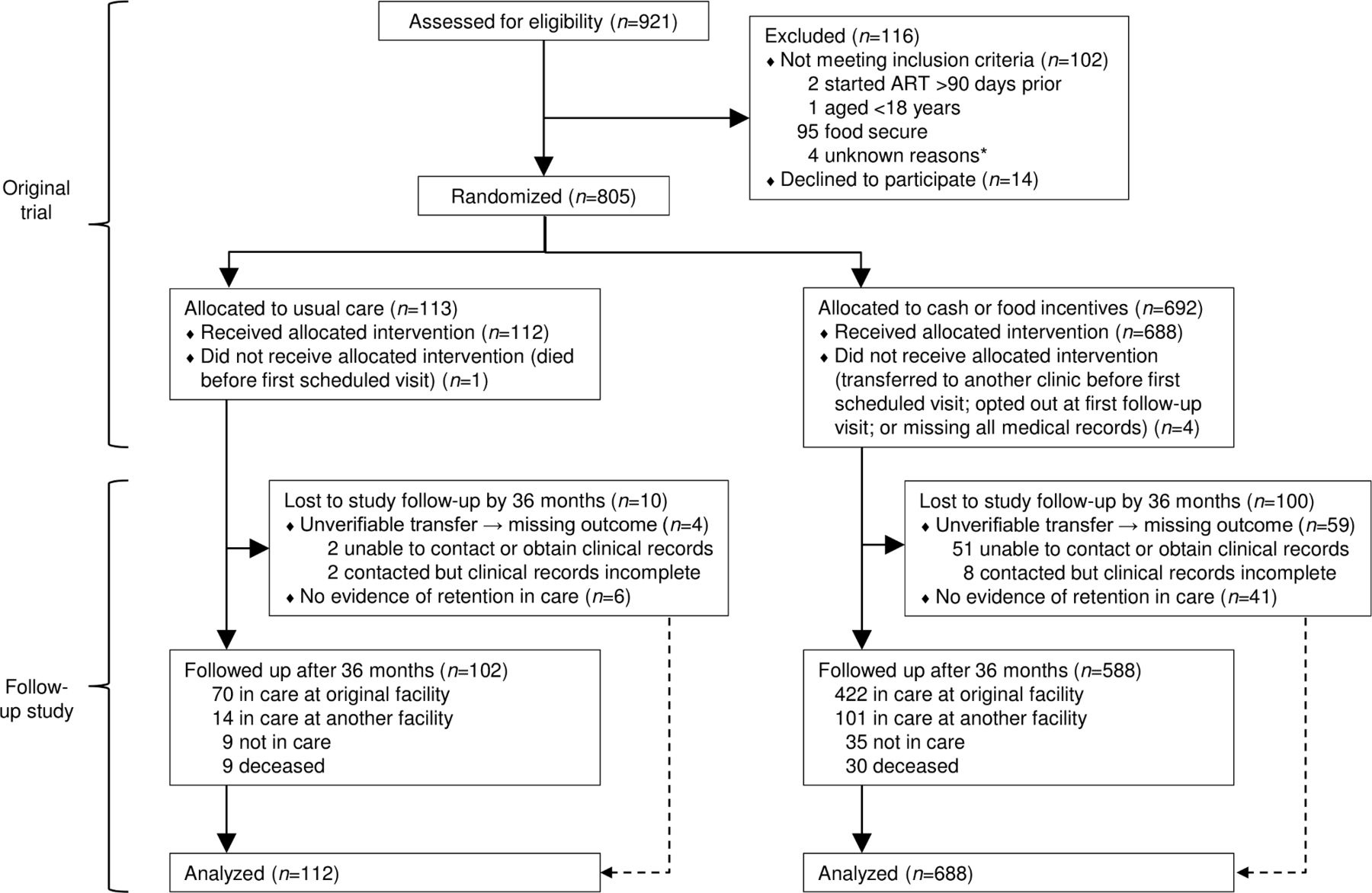
Follow-up to ascertain 24-month and 36-month outcomes occurred between 3 March 2018 and 19 September 2019, with all 800 original participants (509 (64%) women (table 1)) included in the primary analysis (figure 1). Medical records were abstracted for all 800 participants and a total of 530 (66%) participants completed the follow-up interview.

Trial profile, adult HIV treatment initiates in Tanzania, 2013–2018. ART, antiretroviral therapy. *Four screened patients were excluded for unknown reasons (missing screening data).
Participant characteristics at baseline, HIV treatment initiates in Tanzania, 2013–2015
Most interviews (408 (77%)) were conducted at the original health facilities, along with 94 (18%) at another facility or location within Shinyanga region and 28 (5%) over the phone with participants who had relocated to another region. The median follow-up period at the time of the interview was 48 months since enrolment (IQR 43–52). Participant responses indicated high mobility: one in three (162 (31%)) reported moving to a different place of residence since enrolment in the original trial. Additionally, a quarter of those in care at the time of the interview (135 of 521 (26%)) reported currently attending a facility other than the one nearest to their home, with the most cited reasons including continuing care at the same facility where they started treatment (35 (26%)), fear of stigma or HIV status disclosure at their local facility (28 (21%)) and quality of services (16 (12%)).
According to medical records at 24 and 36 months, respectively, 556 (70%) and 492 (62%) participants were engaged in care at the same health facility as at trial enrolment, with no differences between intervention and control groups. We verified receipt of care at another facility for 84 participants (26 out-of-region) at 24 months and 115 participants (35 out-of-region) at 36 months. Records also indicated potential transfers for an additional 56 (7%) participants before 24 months and 63 (8%) before 36 months, but records could not be obtained to verify these transfers (due to of out-of-region or long past transfers); retention in care was therefore estimated using multiple imputation for these participants, whose baseline characteristics did not generally vary from participants with observed retention in care status (online supplemental table 1).
Supplemental material
A total of 57 participants were found to be deceased by the end of follow-up activities, including 24 and 39 deaths that respectively occurred by 24 and 36 months (table 2); only 18 of these deaths had been recorded in original clinical records when follow-up study activities began, while the remainder were documented through study-initiated tracing procedures involving community health workers. In total, mortality status was confirmed through medical records or tracing activities for 710 (89%) participants at 24 months and 700 (88%) at 36 months.
Observed outcomes over time by randomisation group, HIV treatment initiates in Tanzania, 2014–2018
Effect estimates
In primary intention-to-treat analyses (table 3), retention in care did not differ between the incentive and control groups at 24 months (86.5% vs 84.4%; risk differences (RD)=2.1, 95% CI −5.2 to 9.3) nor at 36 months (83.3% vs 77.8%, RD 5.6, 95% CI −2.7 to 13.8). Likewise, there was no difference in all-cause mortality at 24 months (2.5% vs 7.7%, RD −5.2, 95% CI −10.5 to 0.1) or 36 months (4.7% vs 9.0%, RD −4.3, 95% CI −10.2 to 1.6).
Durability of intention-to-treat effects from short-term conditional economic incentives for clinic attendance provided to HIV treatment initiates for 6 months, Tanzania, 2015–2018
Adjusted analyses yielded similar results (table 3), although with a reduction in 24-month mortality among the incentive group compared with the control (RD −5.7, 95% CI −11.3 to −0.1). Estimates from complete-case analyses were also similar (online supplemental table 2). Analyses disaggregated by incentive type also yielded similar results, with no differences in outcomes between the cash and food arms (online supplemental table 3).
In subgroup analyses, estimated incentive effects on 24-month retention varied by age, wealth and clinic, with larger point estimates among younger individuals, those with low relative wealth at baseline, and those enrolled at the regional hospital or health centre as opposed to the large district hospital (online supplemental table 4): P-interaction <0.20). There was no evidence of effect heterogeneity for retention at 36 months or death at either time point.
Lastly, analysis of time to all-cause mortality did not reveal a difference in survival over 36 months (figure 2). The incentive group had a lower mortality rate during the first half of follow-up, including 12 months after the 6-month incentive period (0–18 months: HR 0.27, 95% CI 0.10 to 0.74); thereafter, mortality rates did not vary by intervention group (18–36 months: HR 1.13, 95% CI 0.33 to 3.79).

{kind=link}
{kind=link}
Kaplan-Meier survival plot of time to all-cause mortality among adult HIV treatment initiates in Tanzania, 2013–2018.
Discussion
We used gold-standard tracing procedures in a rare long-term follow-up study of short-term conditional economic incentives for treatment adherence to understand the durability of effects and assess any long-term harms or benefits. After following up with participants 3 years after the original study enrolment, our results show that immediate improvements in retention and mortality from a 6-month cash and food incentive programme for HIV treatment initiates9 were not sustained in the long term. Importantly, the intervention group outcomes did not drop below the comparison group as could be expected given a ‘crowding-out’ effect of external rewards on intrinsic motivation to attend the clinic.27 These findings help to address a dearth of information across the medication adherence literature regarding long-term impacts of short-term incentives. To our knowledge, this is the first study to assess post-intervention effects beyond a year after the withdrawal of incentives for engagement in HIV treatment.
We did not find strong evidence that time-limited incentives produced lasting improvements in ART adherence. However, nor did we find evidence for long-term harm, an often-cited hypothetical concern.27 On the contrary, our results suggest that adherence gains during the incentive period may have averted early deaths at the start of HIV treatment, with lower mortality still perceptible at 24 months in adjusted analyses. One possible explanation of these findings comes from a livelihood framework, whereby cash and food incentives are a ‘provision-type’ intervention that is recommended to meet basic needs of those most vulnerable; alternate interventions aimed at protecting and promoting livelihoods are recommended after providing this temporary stabilising support.28 Another plausible mechanism for these findings is through the price pathway, whereby incentives lowered the cost associated with clinic attendance and triggered the initial adherence effect, then once removed the behaviour gradually reverted towards that of the control group as any habit formation effects wore off.
These findings support the use of short-term incentives as a simple, effective and low-cost intervention for bolstering retention and adherence through the difficult first months of ART initiation, a time commonly defined by stigma, illness, and loss of economic productivity29 as well as peak lost to follow-up from clinical care.30 However, complementary (eg, ‘cash plus’31) interventions may be necessary after ART initiation to address ongoing social and structural barriers to lifelong ART, along with behavioural challenges such as treatment fatigue32; linking additional incentives to clinic attendance may also be important if the price pathway is key. Additionally, the effectiveness of incentives may vary by setting. In our results, there was some evidence of stronger effects at the two clinics with relatively small patient populations (including a regional referral hospital and a health centre, located in/near a medium-sized town) compared with the busy, urban district hospital where implementation may have been more challenging.
This study had several limitations. First, the trial was powered to detect effects at the end of the 6-month incentive period,9 not the smaller effects anticipated at longer follow-up intervals. Next, although exhaustive efforts were made to trace every original study participant, some individuals could not be located due to challenges including high mobility and frequently changed phone numbers. Although there were no meaningful differences in baseline characteristics of participants who could not be traced at 36 months, it is possible these participants differed in other ways that could be associated with the outcomes of interest. For example, participants who remained in care at the original clinics were more likely traced, which could perpetuate differences observed in the original trial’s analysis. Additionally, potentially incomplete HIV care attendance records obtained at follow-up may have resulted in an underestimation of retention in care at intermediate time points, although we do not anticipate any such misclassification to vary by study group. Further, this analysis measured outcomes at discrete points in time, thus it is possible that outcome patterns differed at intermediate time points. Lastly, participants in the original trial were recruited during a period when ART availability was limited to individuals with advanced disease progression, before recent policy changes extended universal access to ART immediately after HIV diagnosis; further long-term research on incentives for individuals starting ART in the current era may be warranted. This study also had key strengths, including the original randomised design and unique focus on ART initiates, along with a rigorous tracing strategy to reduce outcome misclassification for participants no longer attending the original participating health facilities.
In conclusion, findings from this study suggest that small conditional economic incentives are a safe and effective strategy to promote retention and adherence at the critical time of HIV treatment initiation; however, these effects diminish over time. Complementary, longer-term strategies focused on sustaining lifelong retention and adherence are recommended after ART initiation to encompass a comprehensive approach to ending the HIV epidemic.
Data availability statement
Data are available on reasonable request. Deidentified participant data, which were collected for the study, will be made available after obtaining relevant institutional research ethics board approval of a proposal and providing a signed data access agreement that can be obtained from SIM.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the National Institute for Medical Research, Tanzania (Ref. NIMR/HQ/R.8a/Vol. IX/1631) and the Committee for Protection of Human Subjects at the University of California, Berkeley (Protocol ID: 2017-11-10508).
Acknowledgments
The authors are grateful to the local research team, clinic staff, and study participants. Publication made possible in part by support from the Berkeley Research Impact Initiative (BRII) sponsored by the UC Berkeley Library.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Lei Si
Contributors The study was designed by SIM and PFN. SIM, PFN, CAF and NKK implemented the study and collected data with input from RSM. CAF did the statistical analysis with input from SIM, WHD and PTB. CAF drafted the initial manuscript and all authors participated in reviewing the draft for intellectual content and assisting with revisions. All authors approved the final version of the manuscript. CAF had full access to all the data in the study and the final responsibility for the decision to submit for publication.
Funding This work was supported by the National Institute of Mental Health at the National Institutes of Health (grant number R21MH115802 to SIM).
Disclaimer The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.