Article Text

Abstract
Background The objective of this study was to identify the prevalence of long COVID symptoms in a large cohort of people living with and affected by long COVID and identify any potential associated risk factors.
Methods A prospective survey was undertaken of an inception cohort of confirmed people living with and affected by long COVID (aged 18–87 years). 14392 participants were recruited from 24 testing facilities across Bangladesh between June and November 2020. All participants had a previously confirmed positive COVID-19 diagnosis, and reported persistent symptoms and difficulties in performing daily activities. Participants who consented were contacted by face-to-face interview, and were interviewed regarding long COVID, and restriction of activities of daily living using post COVID-19 functional status scale. Cardiorespiratory parameters measured at rest (heart rate, systolic blood pressure, diastolic blood pressure, oxygen saturation levels, maximal oxygen consumption, inspiratory and expiratory lung volume) were also measured.
Results Among 2198 participants, the prevalence of long COVID symptoms at 12 weeks was 16.1%. Overall, eight long COVID symptoms were identified and in descending order of prominence are: fatigue, pain, dyspnoea, cough, anosmia, appetite loss, headache and chest pain. People living with and affected by long COVID experienced between 1 and 8 long COVID symptoms with an overall duration period of 21.8±5.2 weeks. Structural equation modelling predicted the length of long COVID to be related to younger age, female gender, rural residence, prior functional limitation and smoking.
Conclusion In this cohort, at 31 weeks post diagnosis, the prevalence of long COVID symptoms was 16.1%. The risk factors identified for presence and longer length of long COVID symptoms warrant further research and consideration to support public health initiatives.
- COVID-19
- respiratory infections
- cohort study
- public health
Data availability statement
Data are available in a public, open access repository. All data collected in this study is confidential to the study and will be shared anonymously or following ethical principle and made available to others according to the necessity of the study. Data will be available at a public repository [https://www.kaggle.com/kmamranhossain/long-covid-bd].
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
In terms of prevalence of long COVID symptoms in different populations, a smaller study in China identified lingering symptoms in 1733 patients discharged from hospital at a 6-month follow-up time point post acute infection. However, this study was limited because it does not reflect the demographic representations as the data was taken from only one hospital. Another study from 508 707 samples depicts that prevalence of persistent symptoms was near about 6% where female were 1.51 times more vulnerable than men.
We found two studies conducted in Bangladesh, which identified persistent symptoms of COVID-19. However, one study was quite small and again focused only on in-patients admitted to hospital, while the other study, examined the links between COVID-19 and depression.
Key questions
What are the new findings
To our knowledge, this is the largest cohort study (n=2198) of mainly non-hospitalised people previously diagnosed as COVID-19 positive evaluated for long COVID symptoms over a 31-week period post confirmed diagnosis. In addition, this study also provides a detailed analysis of predictive risk factors associated with the presence and length of duration of long COVID symptoms in this inception cohort. We also present new data on the prevalence of long COVID symptoms to be 22·5% at 4 weeks and 16·1% at 12 weeks post diagnosis. Research data on relapsing remitting pattern in the course of these symptoms over time, which has only been previously reported anecdotally.
The predictive risk factors identified for long COVID symptoms were: female gender; COVID-19 severity; one or more comorbidities; an occupation as either a frontline healthcare professional, police worker, housewife or private sector job holder; rhesus positive blood group factor and prior functional limitations. Risk factors identified for a longer duration length of long COVID symptoms were: younger age, female gender, COVID-19 severity, smoking, rural geographical residence and prior functional limitations.
What do the new findings imply
This study showed that the prevalence of long COVID symptoms was 16.1%. The risk factors identified for presence and longer length of long COVID symptoms warrant further research and consideration to support public health initiatives.
Introduction
Individual recovery from COVID-19 infection varies, and it is not fully understood why some people experience persistent symptoms over a longer time period than others. Post-acute COVID-19 symptoms,1 and post COVID-19 conditions,2 are terms used clinically to describe ongoing or new symptoms that occur after the fourth week of recovery from an acute infection, that cannot be explained by an alternative medical diagnosis. The experience of longer-term symptoms has prompted some patient groups to use the pre-existed term long COVID,3 to describe their experience of ongoing symptoms, that persist beyond 4 weeks from suspected infection or positive diagnosis to over 12 weeks and longer.4 It is now understood that COVID-19 can impact on multiple organ systems,5 which can lead to a diverse range of persistent symptoms including fatigue, breathlessness, cough, loss of taste and/or smell, myalgia, memory issues and gastrointestinal problems.6 7 An integrative post COVID symptom model was recently proposed for symptom classification after confirmed diagnosis of COVID-19. There the symptoms were categorised by the duration of COVID-19 symptoms referring to transition phase (4–5 weeks), acute post COVID-19 symptoms (5–12 weeks), long post COVID-19 symptoms (12–24 weeks), persistent post long COVID symptoms (>24 weeks).8 This model incorporates reference to the ‘relapsing remitting’,9 pattern of symptoms experienced by many people living with and without long COVID. Moreover, these have been adopted to assist in presentation of results.
A survey conducted over a 4-week period in the UK found that nearly 1 million people self-reported long COVID symptoms, which equates to 1.5% of the population,.10 The survey also identified that 18.5% of participants reported that their daily activities had been affected a lot by the illness, indicating that long COVID has a detrimental challenge with day-to-day activities. Even many people who were suffering from long COVID reported that they had not be able to returned their previous levels of work and continuously experiencing the symptoms burden,11 so this should be taken seriously.12
It is acknowledged that there is an urgent need for further research on the nature, prevalence and duration of long COVID experienced by affected people,13 along with potential associated risk factors so that overall clinical management can be improved.14 This is especially pertinent in low-income to middle-income countries,15 like Bangladesh, where the majority of the population live in rural districts,16 outside of an extremely densely populated capital city, Dhaka. There are only two published studies so far in Bangladesh on persistent symptoms following COVID-19 infection. One survey of 1002 individuals reported that 20% had experienced persisting symptoms after COVID-19, with diarrhoea (12.7%) being the most common followed by fatigue (11.5%).17 A second smaller study of 355 individuals found that 46% of patients recovering from COVID-19 reported as long COVID symptoms,18 with fatigue being the most common symptom reported. Therefore, it is critical to gain research knowledge on the prevalence of long COVID and identify associated risk factors, as this study does, which will be of relevance to the global community.
The objectives of this study were to identify the prevalence of long COVID symptoms in people affected by COVID-19 and explore any potential associations between reported symptoms and the independent variables measured. Cardiorespiratory parameters and functional limitations were also measured to try to discern if there was an impact on the cardiac system and if functional daily activities were affected by long COVID symptoms.
Methods
Study design and participants
This prospective study used an inception cohort of people living with and without long COVID recruited from a large population sample frame of 14 392 COVID-19 positive cases. These cases were identified from 24 testing facilities across Bangladesh between June and November 2020. All COVID-19 positive and negative diagnoses were performed using a real-time PCR test (RT-PCR).19 Inclusion criteria were: age 18 years and over; people who reported persistent symptoms after positive diagnosis. Exclusion criteria were: individuals too sick to participate; those who declined consent and those we were unable to contact.
The sample size calculation was performed using ‘EPI INFO’ software V.7.4.2.0 developed by the Centers for Disease Control and Prevention in the USA. For the calculation, the reference figure of 535 139 was used (ie, the total number of COVID-19 positive cases reported up to January 2021),20 with a cluster figure of eight (the number of administrative divisions in Bangladesh). The total geographical areas of Bangladesh are divided in eight divisional areas: Dhaka, Chittagong, Sylhet, Rajshahi, Khulna, Comilla and Mymensingh. A calculation was then made with 50% of expected frequency, 5% margin of error and 1.0 design effect. The sample size was generated as a minimum of 1088 with a minimum of 136 samples per division.
Study procedure
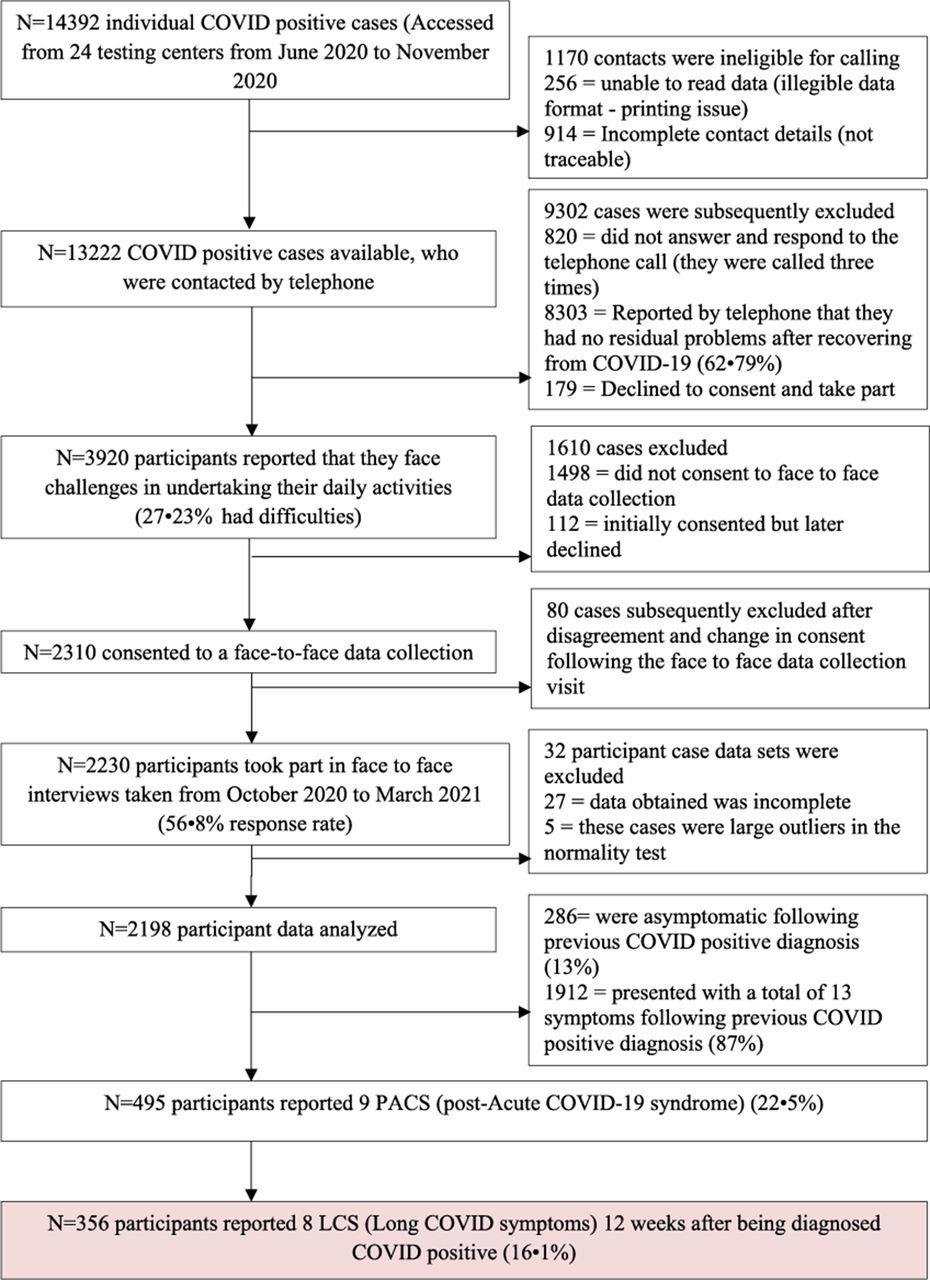
A clear flow diagram of the study process has been produced in figure 1 to meet the quality guidelines recommended by Strengthening the Reporting of Observational studies in Epidemiology.21

STROBE flow diagram of the study. STROBE, Strengthening the Reporting of Observational studies in Epidemiology.
Researchers invited the previously COVID-19 affected patients from the list supplied by the government via telephone call before starting the face-to-face data collection. After preliminary screening, the eligible participants were listed separately and further contacted (figure 1). Data were collected by eight trained data collectors from the Centre for the Rehabilitation of the Paralysed (CRP). Data collectors were comprehensively trained by the study team regarding study aims, ethical considerations, questionnaires and clinical outcome measures. Participants had briefly demonstrated the study process, voluntary agreement and assured the confidentiality of their information by the data collectors during face-to-face interview. The patients declared their involvement and communication was willing, voluntary and had no objection to use the data for research purpose. The data collection was undertaken via mutually convenient scheduled appointments either in the respondent’s house or workplace. All data collectors adhered scrupulously to the COVID-19 preventative precautions, use of personal protective equipment and health regulations. If there was an understanding issue then assessors rephrased the question with an easy sentence to enable completion. Data were then collated anonymously from these documents and transferred into an Excel workbook for audit and analysis. A small-scale pilot study using 17 respondents was initially conducted to test applicability and feasibility of the questionnaire. The process of finding the contacts of the previously affected COVID-19 people, contacting them and perform data collection in this pandemic were permitted and approved by the appropriate authority of the Government of the People’s Republic of Bangladesh.
Data collection and questionnaire
All contactable participants (N=13 222) were asked by telephone: ‘Do you feel that you have any challenges or have any persisting symptoms after receiving a negative test result for COVID-19?’ Participants who consented to face to face data collections (N=2310) were provided with a questionnaire consisting of three parts. The first part was designed to gather sociodemographic information with seven questions related to age, gender, marital status, education, residing area and occupation. The second part consisted of seven questions related to comorbidities, blood group and rhesus status, date of COVID-19 positive test, date of COVID-19 negative test, presenting symptoms during COVID-19 illness, persisting COVID-19 symptoms and treatment received during COVID-19 illness. We have included 18 symptoms according to the national guidelines22 and another study.7
The third part of the questionnaire focused on the measurement of cardiorespiratory parameters and included the Post COVID-19 Functional Status Scale (PCFS).23 Cardiorespiratory parameters measured included: resting heart rate (HR); blood oxygen saturation levels (SpO2 at resting); systolic and diastolic blood pressure; inspiratory and expiratory lung volumes; and maximal oxygen consumption (Vo2max).
The PCFS is an instrument that aims to identify and record the course of symptoms following infection with COVID-19 and their have an impact on functioning and disability. The scale covers six domains including: survival; constant care; basic activities of daily living; instrumental activities of daily living; participation in usual social roles and a symptom checklist. Each item in each domain is scored from five possible options on an ordinal scale from zero to four with the fifth grade being ‘Death’. An overall final scale grade is obtained from completion with a high-grade corresponding to more functional limitations and a low final grade indicates no persisting symptoms or restricted daily activities. The PCFS has adequate construct validity,24 and has a Cronbach alpha score of 0.879 in our study, which indicates a satisfactory level of internal consistency. The PCFS was translated into Bengali, however, the psychometric properties are not yet known and the language validation process was followed as per WHO guidance,.25
Statistical testing
Data analysis used the statistical SPSS V.20.0. The normality test was performed through Kolmogorov-Smirnov test. Descriptive statistics were performed separately for Acute COVID-19 Symptoms (Symptoms from the first day to less than 4 weeks from the day of COVID-19 infection),1 Post-acute COVID-19 symptoms (symptoms from 4 to 12 weeks from the day of COVID-19 infection)14 and the Long COVID symptoms (symptoms more than 12 weeks from the day of COVID-19 infection)4 (tables 1 and 2). Relationships between a categorical independent variable (eg, long COVID symptoms, PCFS) and a parametric sociodemographic dependent variable were determined through independent t tests. In addition, relationships among two or more categorical variables were explored using the χ2 test and Fisher’s exact test (table 2). To ascertain which factors were potentially related to long COVID, binary logistic regression was performed with the presence of long COVID symptoms as the dependent variable (table 3) and multiple linear regressions were performed with the duration of long COVID symptoms as the dependent variable (table 4). Figures 2–4 are presented as bar charts with an error bar (95% CI). Figure 5 presents the associated risk factors identified among multiple variables, for long COVID symptoms (independent variable) and duration of long COVID symptoms (latent variable) with demographic variables by using structural equation modelling (SEM) using SPSS AMOS V.24.0 (figure 5). The alpha value was set as p<0.05.
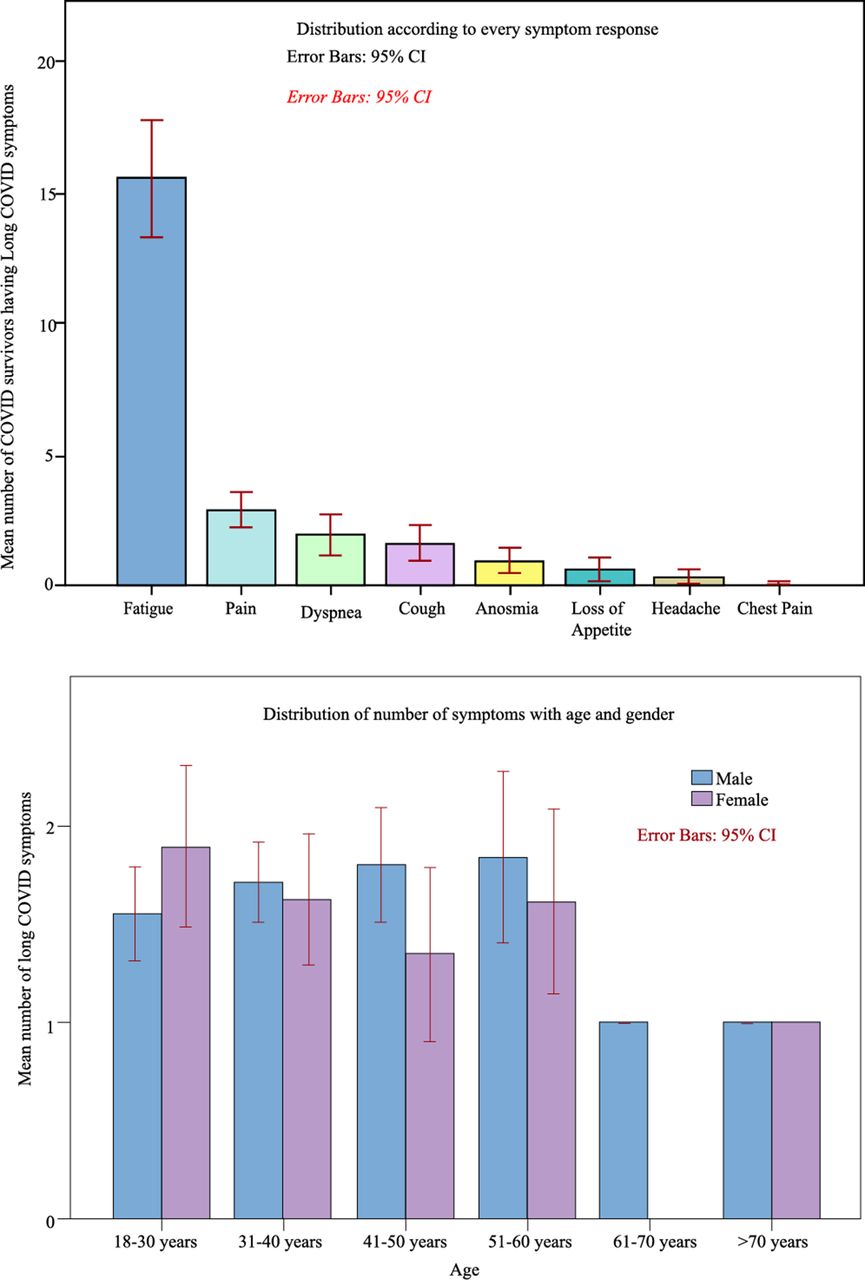
Distribution of long COVID-19 symptoms.
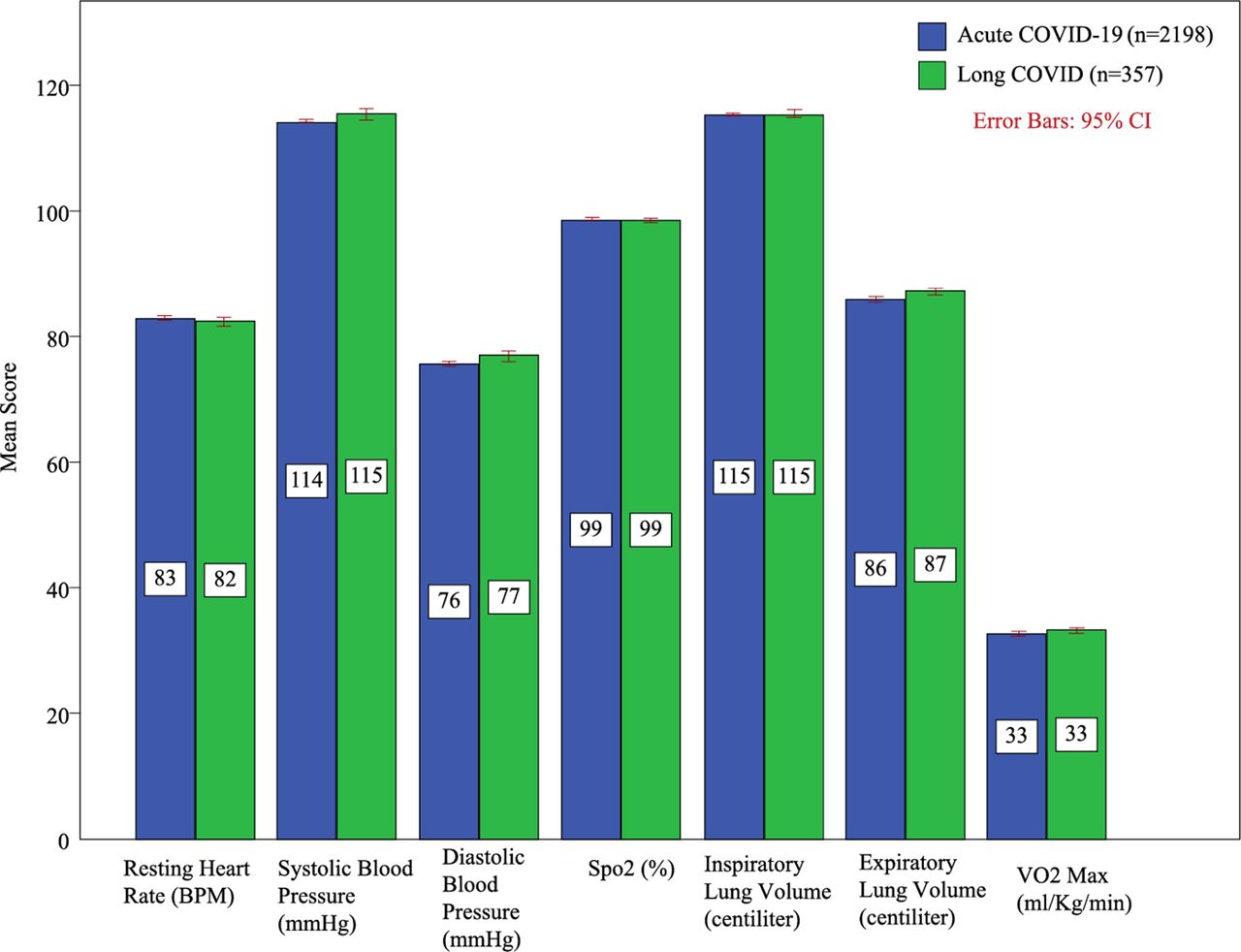
Comparison of cardiorespiratory system variables between people living with acute COVID-19 symptoms and long COVID symptoms. BPM, beats per minutes; SpO2, oxygen saturation levels; Vo2max, maximal oxygen consumption.
Baseline characteristics for inception cohort of COVID-19 positive cases
Relationship among sociodemographic variables and long COVID symptoms
Factors associated with long COVID symptoms
Factors associated with limited function in people having long COVID symptoms

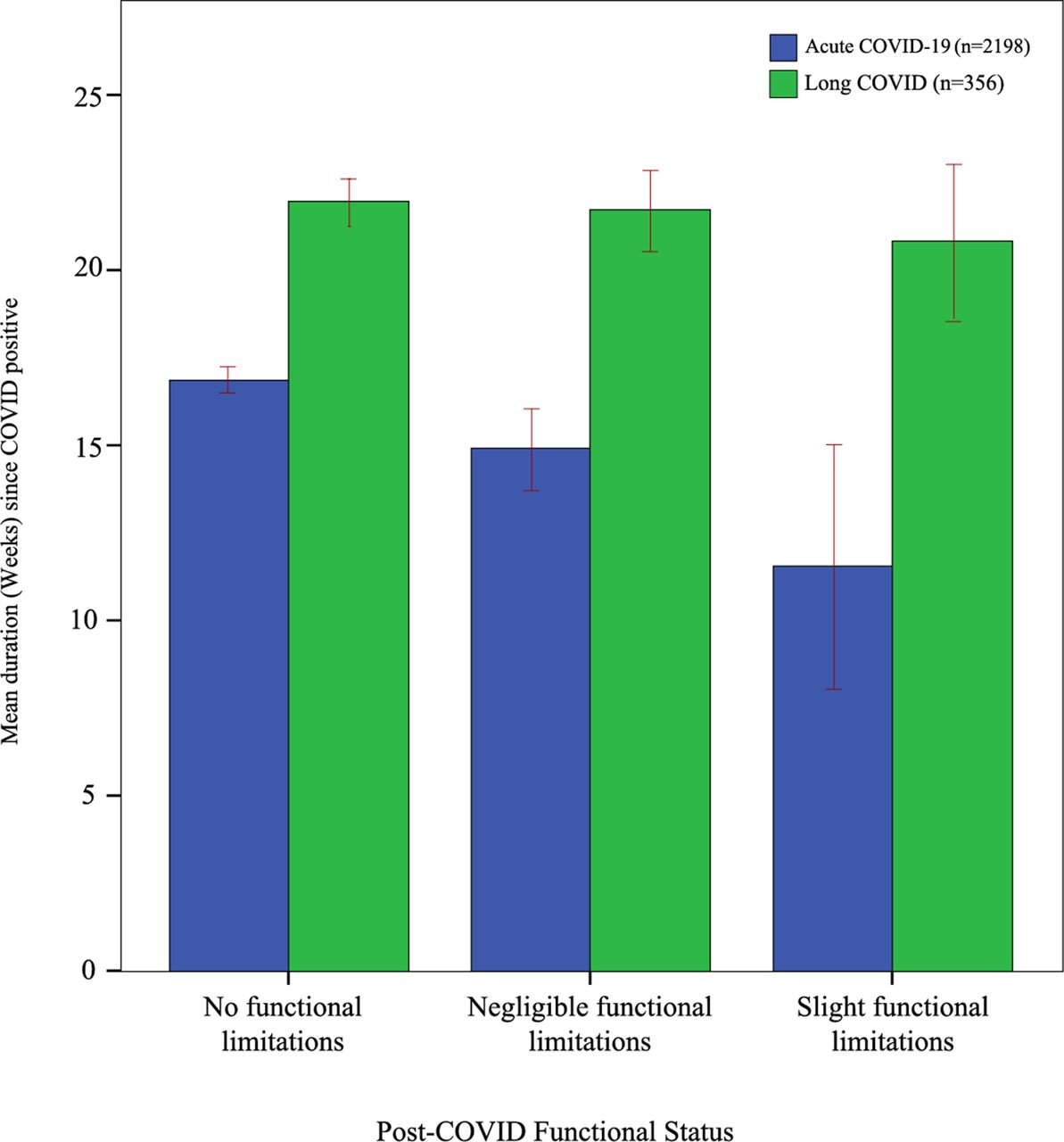
Comparison of Post COVID-19 functional status scale between people living with acute COVID-19 symptoms and long COVID symptoms.

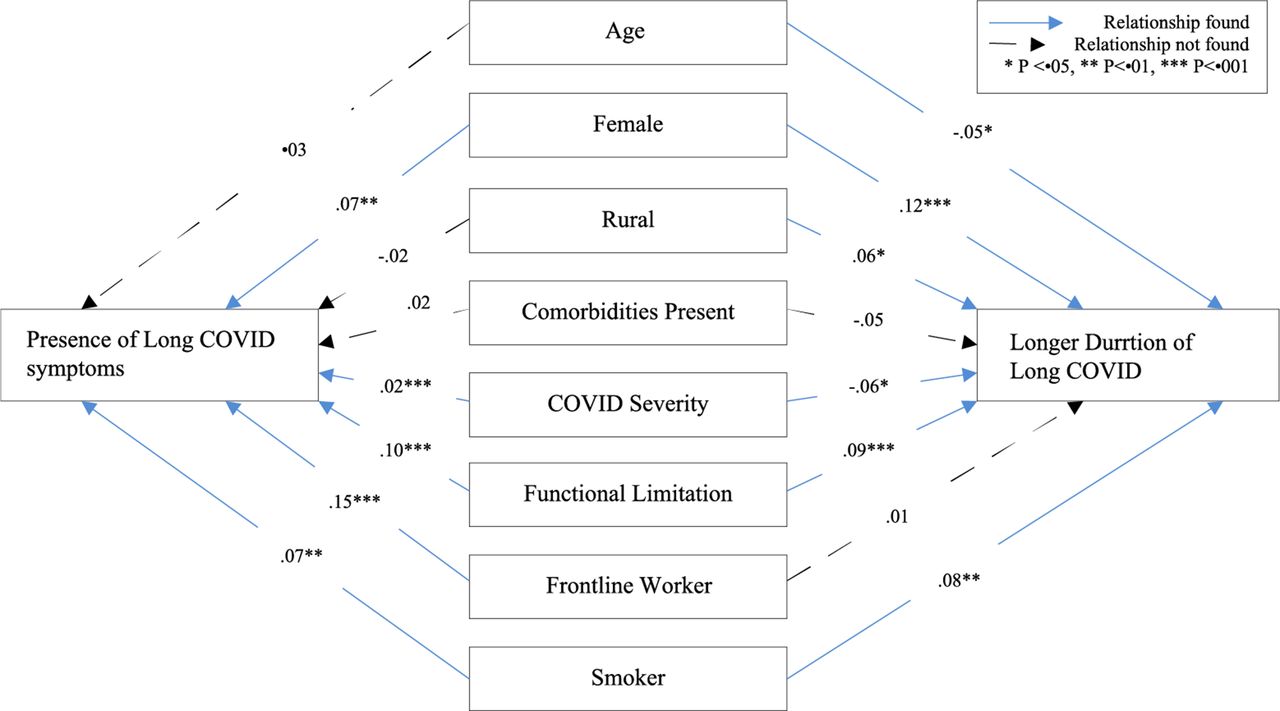
Structural equation model for predictors of long COVID symptoms.
Patient and public involvement
During conducting this research, patients and the public were not involved in developing the question, design, analysis and interpretation. As the study was self-funded and national based, so such involvement was quite difficult with limited funding.
Results
Prevalence
From 14 392 samples, 13 222 respondents were called by telephone. Sixty-three per cent of (n=8303) previously diagnosed as COVID-19 positive reported complete recovery and 27.23% (n=3920) stated that they experienced difficulties when undertaking daily activities. The study had a response rate of 56.8%. This study found that 22.5% (n=495) had post-acute COVID-19 symptoms at 4 weeks post diagnosis and 16.1% (n=356) had long COVID symptoms at 12 weeks post diagnosis (figure 1).
Sociodemographic variables and health-related information
The mean age of all acute COVID-19 symptoms (n=2198) was 38.07±11.4 years, post-acute COVID-19 symptoms (n=495) 38.86±11.3 and those people living with and affected by long COVID (n=356) had mean age 38.42±11.3. The majority of the acute COVID-19 symptoms were between 31 and 40 years of age 43.3% (n=718) and 30.4% (n=669) were aged 18–30 years. The male to female ratio of the respondents was 2.6:1. Respondents covered all eight administrative divisions in Bangladesh as follows: Dhaka 35.89% (n=789), Chittagong 8.50% (n=187), Rajshahi 8.37% (n=184), Sylhet 9.63% (n=212), Rangpur 9.13% (n=201), Barisal 10.62% (n=234), Khulna 8.04% (n=177) and Mymensingh 9.73% (n=214). There was a larger number of responses from rural areas 75.2% (n=1652). Eighty five percent (n=1868) of the participants were married and 50.1% (n=1101) were graduate or postgraduate. The most common occupation reported was that of private jobs, which comprised 55.1% (n=1212). Multiple response analyses found that the most common comorbidities for acute COVID-19 symptoms were as follows: 22.7% had diabetes, 25.6% had hypertension, 6% had heart disease and 6.9% had pre-existing lung disease 34.7% of the acute COVID-19 symptoms had blood group B positive and other major distributions were O positive 23.4% and A positive 23.1%. The detailed sociodemographic and health related information for participants is appended in table 1.
Symptom responses and duration
Figure 6 presents the results using the integrative post COVID-19 symptoms model8 and identifies that among the acute COVID-19 symptoms 13% (n=286) were asymptomatic. Among those with symptoms, the most common symptoms described were fever 76.6% (n=1683), fatigue 50.1% (n=1101), cough and upper respiratory tract symptoms 65.4% (n=1438), dyspnoea 23.8% (n=523), pain 33.1% (n=727), ageusia 29.3% (n=644), headache 38% (n=836) and anosmia 43.9% (n=966). In this study, we considered all the post-exertional symptoms like fatigue, prolonged weakness, weakness after activity or residual weakness as ‘fatigue’. After 4 weeks, the major post-acute COVID-19 symptoms were fatigue 84.8% (n=420), and pain 15.4% (n=76). After 12 weeks, long COVID symptoms presented as fatigue 82.9% (n=295), cough and upper respiratory tract symptoms 8.7% (n=31), dyspnoea 10.4% (n=37), pain 16.9% (n=60), chest pain .3% (n=1), ageusia 3.4% (n=12), headache 2.2% (n=8) and anosmia 5.1% (n=18). Fatigue was the prominent long COVID-19 symptoms. The number of long COVID symptoms experienced by a COVID-19 survivor ranged from 1 to 8 (figure 2). The overall duration of long COVID symptoms was 21.8±5.2 weeks. Duration of individual long COVID symptoms varied in weeks as follows: fatigue 21.7±5.2; pain 22.2±5.3; dyspnoea 22.7±4.9; cough and upper respiratory symptoms 22.4±5.1; anosmia 22.6±6, ageusia 20.6±5.5 and headache 22.5±5.7. There was a relapsing remitting pattern noted in the long COVID symptoms from week 13 onwards to week 31, with the highest increments of long COVID symptoms noted from 25th to 26th weeks (figure 7).

Acute COVID-19 symptoms, postacute COVID-19 symptoms and long COVID-19 symptoms response.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relapsing remittent pattern of long COVID symptoms.
COVID-19-related information
According to WHO working group classification,26 63.2% (n=1390) of the acute COVID-19 symptoms had mild COVID, 23.7% (n=520) had moderate COVID and 0.4% (n=8) had severe COVID-19. The ratio of the severity in acute COVID-19 symptoms, post-acute COVID-19 symptoms and long COVID symptoms were mostly similar (table 1). Ninety-four percent (n=2063) respondents opted to follow the advice of the government telemedicine team by resting at home, undertaking isolation and using advised medication. 5.7% (n=126) needed supplementary oxygen either at home or hospital, 0.2% (n=5) were admitted to hospital and required non-invasive ventilation and o.2% (n=4) were admitted to a dedicated COVID-19 intensive care unit with or without mechanical ventilation. Further detail of the COVID-19-related information of acute COVID-19 symptoms, post-acute COVID-19 symptoms and long COVID symptoms are appended in table 1.
Cardiorespiratory function
The mean resting HR for participants with post-acute COVID-19 symptoms and long COVID symptoms was 82.5±6.9, and 82.4±6.7 beats per minute; systolic blood pressure was 115.8±8.9, 115.4±8.7 mm Hg; diastolic blood pressure 77.3±7.6, 76.9±7.3 mm Hg; SpO2 at resting 98.5±0.6, 98.6±0.7%; inspiratory lung volume 1155±62, 1154±61 mL/min; expiratory lung volume 872±54, 871±56 mL/min; and VO2Max 33.0±3.4, 33.1±3.3 respectively. However, figure 3 shows no notable changes of mean in long COVID-19 compared with the people not affected by long COVID.
Post-COVID-19 functional status scale
Eighty-eight percent (n=1939) of acute COVID-19 symptoms had no residual functional limitation and 74.9% (n=371) of post-acute COVID-19 symptoms and 73.3% (n=261) of long COVID also had no residual functional limitations. However, 20.2% (n=100) of post-acute COVID-19 symptoms and 20.2% (n=72) of long COVID symptoms reported negligible functional limitation and 4.8% (n=24) of post-acute COVID-19 symptoms and 6.5% (n=23) of long COVID reported slight functional limitations. Overall, the mean PCFS in post-acute COVID-19 symptoms was 12.41±8.7 and in long COVID symptoms was 12.14±8.8 in 0 to 100 scores. Compared with acute COVID-19 symptoms, participants with long COVID had higher mean scores in relation to progression of weeks (figure 4), indicating that functional limitation is more progressive with time in people living with and affected by long COVID compared with others.
Relationship of long COVID with sociodemographics
Table 2 represents a segregated relationship of sociodemographic and health related factors with long COVID in correlation model. Categorical age was associated with long COVID (p<0.05), whereas pain was associated separately with overall age of the population (p<0.05). Long COVID was associated with gender (p<0.01), marital status (p<0.05), area of residence (p<0.01), occupation (p<0.001) and severity of COVID (p<0.001).
Factors associated with long COVID
Table 3 describes the binary logistic regression model to determine the factors associated with long COVID. People living in rural areas had a relationship with long COVID (β=0.41, p<0.01). Other relationships included being a housewife and private employees (β=0.48, p<0.001), frontline worker (police and health professionals) (β=0.12, p<0.001,), people with comorbidities (β=0.365, p<0.01) and smokers (β=0.50, p<0.01). The PCFS was also found to be positively associated (β=0.14, p<0.001). However, male gender had a reverse relationship with long COVID symptoms (β=−0.36, p<0.01), and the presence of a rhesus positive factor in the blood group also had similar reverse relationship (β=−0.596, p<0.05).
Factors associated with limited function in long COVID people
Table 4 shows the factors associated with limited functional scores in participants with long COVID in a multiple linear regression model. Female gender was related with functional limitation (β=.064, p<0.05). Other linear associations were fatigue (β=0.094, p<0.001), pain (β=0.17, p<0.001), systolic blood pressure (β=.71, p<0.01), diastolic blood pressure (β=0.75, p<0.01), inspiratory lung volume (β=0.27, p<0.01), expiratory lung volume (β=0.69, p<0.01) and Vo2Max (β=0.213, p<0.01). A reverse relationship was found with males (p<0.05), people aged below 50 years (p<0.001) and people who had mild COVID-19 (p<0.001).
Predictors of long COVID
Figure 5 predicts the presence of long COVID symptoms and longer duration of long COVID symptoms through the SEM. Goodness of fit indicates a satisfactory level of ‘good fit’ of assumptions for external validity (χ2 1302.88, df 29, p .001, χ2/df 44.92, root mean square error of approximation 166 (90% CI 0.158 to 0.174), root mean square residual 1.449, CFI .147, GFI .882). Presence of long COVID was positively associated (R20.098) with frontline workers (police and health professionals) (β.15, p<0.01), limited function (β.10, p<0.001), being female (β.07, p<0.001) smokers (β.07, p<0.001) and the severity of COVID-19 (β=0.02, p<0.001). A longer duration of long COVID symptoms was positively associated (R20.041) with being female (β=0.12, p<0.001), limited function (β=0.09, p<0.001), smokers (β=0.08, p<0.01) and people living in rural areas (β=0.06, p<0.05). Interestingly, age has a reverse relationship with a longer duration of long COVID symptoms (β=−0.05, p<0.05).
Discussion
In this study, the prevalence of long COVID symptoms was 22.5% at 4 weeks and 16.1% at 12 weeks post diagnosis, respectively. This is slightly higher than that reported by the UK study,13 which reported the prevalence of post-acute COVID-19 symptoms and long COVID symptoms as 20% and 10%, respectively. A recent study reported that the ongoing health issues of ‘fatigue or exhaustion, sleep difficulties and anxiety or depression’,7 were experienced within a cohort of 1733 survivors discharged from hospital in China, when followed up at a 6-month time point. The limitation of that study was that all participants had been treated as in-patients in hospital, unlike this research study, in which the majority of participants did not receive hospital treatment and remained at home during recovery. Our study adds valuable research knowledge to the gap in understanding the prevalence and nature of long COVID symptoms, who have remained at home during their illness. Our study is larger than the two previous studies conducted in Bangladesh,15 16 and provides new research knowledge on associated risk factors for long COVID, in addition to identifying risk factors associated with a longer time length of these symptoms.
In this study, the most common symptom during the acute phase was fever, closely followed by fatigue and upper respiratory tract symptoms. This is consistent with literature that has reported similar symptoms.27–29 The study found eight long COVID symptoms, with fatigue being the most common symptom closely followed by muscle pain and dyspnoea. In another study,30 after 3–9 months, 14% of individuals had fatigue problems. Most available literature unanimously reports fatigue,1 17 18 as the most common long COVID symptoms. After this, many studies report breathlessness,1 7 31 as the second most common long COVID symptoms with other studies citing anosmia, cough and myalgia to also be common.32 Augustin et al33 reported a study where non-hospitalised COVID-19 patients had more anosmia (12.4%) and ageusia (11.1%) than fatigue (9.7%) and shortness of breath (8.6%) over a recovery period of 4–7 months. However, our data show a little difference with other study11 where the authors reported fatigue, post exertional malaise and cognitive dysfunction as most frequent symptoms while in our study fatigue followed by muscle pain and dyspnoea.
This study reported that the majority of respondents had mild to moderate COVID-19 and approximately 93% symptoms managed outside of hospital settings. Sixty-two percent (308) of respondents with long COVID-19 reported mild disease, which would not require hospitalisation. There is a paucity of literature in this area, which perhaps reflects the challenge of how to collect and gather data from people at their community setting who managed their treatment outside of hospital based facilities and also considering that Bangladesh is an under-resourced country and the hospital system is private so usually hospital admission and treatment costs money.
Figure 7 highlights the relapsing remitting nature of long COVID symptoms reported over time between 13 and 31 weeks with maximum symptoms reported between 25 and 26 weeks, which is consistent with other researches.1 6 8 14 19 34 In figure 3, it is apparent that there was little difference noted between the cardiorespiratory function variables measured for people living with acute COVID-19 symptoms and long COVID symptoms. In terms of functional limitations, it is clear from figure 4, that people with long COVID symptoms had more functional limitations when compared with all acute COVID-19 symptoms.
Overall, this study found that age (<30 years); rural geographical residence; housewife role or private sector occupation; one or more comorbidities; smoking; a longer acute COVID-19 recovery period, a positive rhesus factor in the blood group and prior functional limitations were all predictive risk factors for long COVID symptoms. To our awareness, this is the first study to identify specific risk factors for long COVID within the general population with RT-PCR positive and while the specific context is Bangladesh, we think that these risk factors warrant further investigation in all global community populations.
Previous studies on long COVID in Bangladesh focused on urban areas and did not include rural regions, as this study did, which is now identified as a risk factor while males (m) comprised the majority of respondents with long COVID symptoms (69.0%), it was the females (f) who reported a greater proportion of long COVID symptoms, (over all f=25.2%, m=21.2%). This may be due to the overall higher incidence of COVID-19 diagnosed and reported by men in Bangladesh and the lack of sex disaggregated data in previous studies. The female sex was significantly associated with a longer duration of COVID-19 symptoms. In addition, women reported slightly higher levels of fatigue, followed by pain, anosmia and insomnia (f=1.3%, m=0.3%). In contrast, men reported slightly higher levels of dyspnoea, ageusia, cough and chest pain.
A significant positive association was found between gender and functional limitations. Women and those with cardiorespiratory comorbidity were more likely to develop functional limitations during the long COVID period. In contrast, men and those with mild COVID symptoms were inversely associated with functional limitations.
The limitations of this study include that the sample was taken from twenty-four testing centres, and it is appreciated that people, who have attended these centres for diagnosis may not be truly representative of all communities within the Bangladeshi population. However, it will be possible for the team to contact and follow-up on this cohort for longitudinal data in the future. In addition, the limited nature of resources meant that a proportion of potential participants could not be contacted due to system and educational constraints and the researchers had limited access to the electronic database. Davis et al11 reported 203 symptoms while we reported fewer symptoms as our study was an inception cohort. The differences might be happened because of follow the structured symptoms listed from Directorate General of Health Services in Bangladesh as well as from the literature.7
Conclusion
In this study, the prevalence of long COVID symptoms was identified to be 22.5% at 4 weeks and 16.1% at 12 weeks post diagnosis. In addition, the study identified some key predictors for the presence of long COVID, in terms of associated risk factors and also risk factors associated with a longer duration of long COVID illness. Further research is needed to gain more insight into these identified risk factors and what can be done to support communities affected by it.
Supplemental material
Data availability statement
Data are available in a public, open access repository. All data collected in this study is confidential to the study and will be shared anonymously or following ethical principle and made available to others according to the necessity of the study. Data will be available at a public repository [https://www.kaggle.com/kmamranhossain/long-covid-bd].
Ethics statements
Patient consent for publication
Ethics approval
Ethical permission was obtained from The Institutional Review Board, Institute of Physiotherapy Rehabilitation and Research, BPA (Ethical review committee at Bangladesh Physiotherapy Association) on September 17, 2020 (BPA-IPRR/IRB/17/09/2020/028) and CRP Ethics Committee, Centre for the Rehabilitation of the Paralysed (CRP) on October 10,2020 (CRP-R&E-0401-336), respectively. The study was registered retrospectively at WHO Primary Clinical trial registry platform (CTRI/2020/09/028165) on 30/09/2020 with the title 'Symptoms presentation among the COVID-19 survivors in Bangladesh'. Written approval for data collection obtained from the Directorate General of Health Services (DGHS) of the Ministry of Health and Family Welfare in Bangladesh (online supplemental file A). Verbal consent was obtained during the initial telephone call and written consent was obtained at interview. The principles of the Declaration of Helsinki were followed throughout the research to ensure confidentiality, ethics and privacy.
Acknowledgments
We thank all individuals who participated in this study and their families.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @KMAmranHossain1, @K_neurorobotics
Contributors MAH, KMAH, KS, ZU, LMW, VR, MS, RS, MSH, MFK, RF, SR, MSA, SKC, MAH and IKJ conceptualised the study. MAH, KMAH, LMW, VR, RS, SR, MSAa nd IKJ curated and collated the data. MAH, KMAH, KS, ZU, LMW, VR, MS, RS, MSH, MFK, RF, SR, MSA, SKC, MAH and IKJ did validation. KMAH, KS, ZU, LMW, VR, MS RS, SR and MSA visualised the data. MAH, KMAH, KS, ZU, LMW, VR, MS, RS, MSH, MFK, RF, SR, MAH and IKJ contributed to the model development. MAH, KMAH, KS, MS, RS, RF, SR, MSA and IKJ did the formal analysis. MAH, KMAH, KS, LMW, VR and RS wrote the manuscript. KS, ZU, LMW, VR, MS, MSH, MFK, RF, SR, MSA, SKC, MAH and IJK reviewed the manuscript. All author had full access to all the data in the study and the corresponding author IKJ act as a guarantor and had final responsibility for the decision to submit for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.