Article Text

Abstract
Background Sub-Saharan Africa (SSA) experienced a burden of organised violence within 18 low-income and middle-income countries and hosted over 33 million displaced persons in 2019. Community-centred mental health and psychosocial support (cc-MHPSS) programmes may provide insights to address the psychosocial well-being of conflict-affected individuals, though literature is mixed on community impact. This review aimed to synthesise qualitative evidence to understand the kind of experiences conflict-affected participants have and how these experiences occur during cc-MHPSS programme engagement in SSA.
Methods We searched Global Health, MEDLINE, Psychological Information Database, Embase Classic+Embase, Social Policy and Practice, Web of Science, Africa-Wide Information, PubMed and Global Index Medicus databases. Eligible publications qualitatively reported on conflict-affected participants’ experiences of engagement in cc-MHPSS programmes. Data were extracted to summarise publication characteristics. The results were synthesised using a thematic synthesis analysis.
Results The search yielded 953 records, of which 20 publications were included in the review. Included publications were located in Rwanda (n=8), the Democratic Republic of the Congo (n=3), Mozambique (n=3), Sierra Leone (n=1), Ghana (n=1), Uganda (n=1), Zimbabwe (n=1) and South Sudan (n=1); one publication included three countries (Sierra Leone, Liberia and Uganda). Findings include the themes of (1) the experience of change in time and space, and (2) the sharing and silence of participants’ experiences. Findings demonstrate that elements transferred by participants from a cc-MHPSS programme to a natural community, and vice versa, contribute to participants’ healing. Elements’ transfer, or non-transfer, was often related to participants’ disclosure, or non-disclosure, of experiences.
Discussion Findings suggest that there are elements from a cc-MHPSS programme and a wider community which aid participant engagement and work therapeutically. More rigorous research is needed concerning how participants experience change during cc-MHPSS programme engagement in proximity to their relationship with the wider community.
PROSPERO registration number CRD42020197300.
- systematic review
- public health
Data availability statement
Data are available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Sub-Saharan Africa (SSA) experienced a burden of organised violence and the highest global total of displaced persons. Community-centred mental health and psychosocial support (cc-MHPSS) programmes may provide insights into local psychosocial well-being, though current literature is mixed on community impact. Qualitative evidence is lacking on conflict-affected participants’ experiences of cc-MHPSS programme engagement in a SSA context.
What are the new findings?
Findings demonstrate that elements (eg, conflict-related experiences, communal activities) transferred from a cc-MHPSS programme to a natural community, and vice versa, seem to contribute to participants’ healing experiences.
The elements’ transfer, or non-transfer, was often related to participants’ disclosure, or non-disclosure, of experiences in both cc-MHPSS and natural community settings.
What do the new findings imply?
Allowing participants to bring therapeutic community elements (eg, communal activities) and to share comfortable topics (eg, income-generation) may aid in cc-MHPSS programme engagement.
Background
In 2019, sub-Saharan Africa (SSA) experienced 85 events of organised violence across 18 countries, all of which are low-income and middle-income countries.1 According to the United Nations High Commissioner for Refugees’s Global Report 2019, the SSA region hosts over 33 million—39% of the global total—displaced persons, the highest in the world. Conflict-related occurrences are credited as a contributor of displacement in SSA.2 Individuals affected by conflict are exposed to traumatic events, forced displacement, social support loss, poverty and unemployment stressors.3 Conflict exposure is linked to psychological distress symptoms and disorders4 5; and conflict-affected communities experience vulnerabilities related to accessing resources among the fragmentation of governance, economic and healthcare structures.6
Since the 1980s, there has been great focus on the development of mental health and psychosocial support (MHPSS) programmes to address the psychological well-being needs in communities affected by conflict.4 The Inter-Agency Standing Committee’s (IASC) standards define MHPSS as ‘any type of local or outside support that aims to protect or promote psychosocial well-being and/or prevent or treat mental disorder.’7 (p16) Currently, there has been increasing interest in a community-centred approach to MHPSS programmes in conflict-affected settings. Flaspohler et al define the community-centred approach as ‘the evolution of practice in local contexts…(with an emphasis on) the user of that source (the programme) when conceptualising dissemination…the improvement of existing practice and service delivery over the introduction of something new.’8 (p184) In this approach, the role to determine the programme development, outcomes, and implementation is shared among the local community and programme providers.9 This approach has arisen in response to criticisms of the trauma-focused and local idioms of distress (ie, conceptualisations of distress in relation to personal and cultural meaning) approaches to MHPSS programmes.10 From these perspectives, there is a top-down application of Western-originated outcomes and an overemphasis of research focused on the deficits (eg, post-traumatic stress disorders, psychological distress) into the sociocultural context of a local conflict-affected community.11 Though the trauma-focused and local idioms of distress approaches are problem-focused, it is not sufficiently addressing local needs and desires. The community-centred approach may provide beneficial insights in targeting local needs.
The increased inclusion of conflict-affected communities’ perspectives is needed in the development and implementation of MHPSS programmes.12 Few studies report MHPSS programmes that target the local needs and desires of conflict-affected communities. For example, studies conducted in Sierra Leone13 and Rwanda14 have shown the facilitation of high ownership and receptivity among community members and programme staff. Contrasting to those studies, negative impacts of community-centred MHPSS (cc-MHPSS) is also reported. Study conclusions in Rwanda11 and Sierra Leone15 suggest cc-MHPSS participants can be socially isolated from their surrounding local community and experience an increase in psychological distress symptoms and disorders, respectively. Though these studies are reporting participants’ experiences, their conclusions of cc-MHPSS programmes are diverging.11 13–15 It is not known why cc-MHPSS programmes show such contradictory findings. By understanding participants’ in-depth experiences through the synthesis of qualitative evidence, this review attempts to contribute to resolving the contradictory cc-MHPSS results and further, improve programme development that is tailored to local structures and culture. Thus, this review investigated two objectives: (1) the kind of experiences participants have through their engagement in cc-MHPSS programmes and (2) how participants’ experiences happen as they engage in cc-MHPSS programmes.
Methods
This review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.16
Inclusion criteria
To be considered for inclusion in this review, studies had to be a primary qualitative study or mixed-methods study, peer-reviewed, full-text and in English. There were no restrictions on the publication year.
Participants who live in a conflict-affected community within a SSA country and were recipients of a cc-MHPSS programme were included. Participants originating from a conflict-affected community within a SSA country and were displaced, immigrated or resettled into a SSA host country were also eligible. There was no limit on age. For this review, conflict-affected communities refer to communities affected by man-made disasters (eg, armed conflict, genocide or political violence). SSA countries refer to the current World Bank classification.17
The inclusion of cc-MHPSS programmes was defined according to IASC’s classification of MHPSS programmes7 (p16) and Flaspohler et al’s definition of community-centred approach.8 (p184) These include, but are not limited to, practices of care from traditional healers, primary care, and non-governmental organisations.
Studies with reports of participants’ experiences during cc-MHPSS programme engagement were eligible. Participants’ experiences reported qualitatively were eligible for inclusion. These include, but are not limited to, author descriptions, direct participant quotes, participant observation (eg, fieldnotes), questionnaires (eg, open or closed answers), interviews (eg, structured and semistructured) and focus group discussions.
Search strategy
Searches were conducted on 14 July 2020–15 July 2020. The following nine databases were used: Global Health, MEDLINE, PsycINFO, Embase Classic+Embase, Social Policy and Practice, Web of Science, Africa-Wide Information, PubMed and Global Index Medicus. Forward and backward citation searching was used to complement the search. As there were no restrictions on the publication year, a date filter was not used when conducting the searches .
Search terms, applicable synonyms and Boolean operators were used to determine five concept domains: (1) community-centred, (2) mental health and psychosocial support, (3) qualitative or mixed-methods studies, (4) conflict-affected and (5) SSA. These concept domains are organised within a Population, Intervention, Control/Comparison, Outcome, Study design/Setting (PICOS) framework (online supplemental material). The search strategy for MEDLINE is found in online supplemental material.
Supplemental material
Study selection and quality appraisal
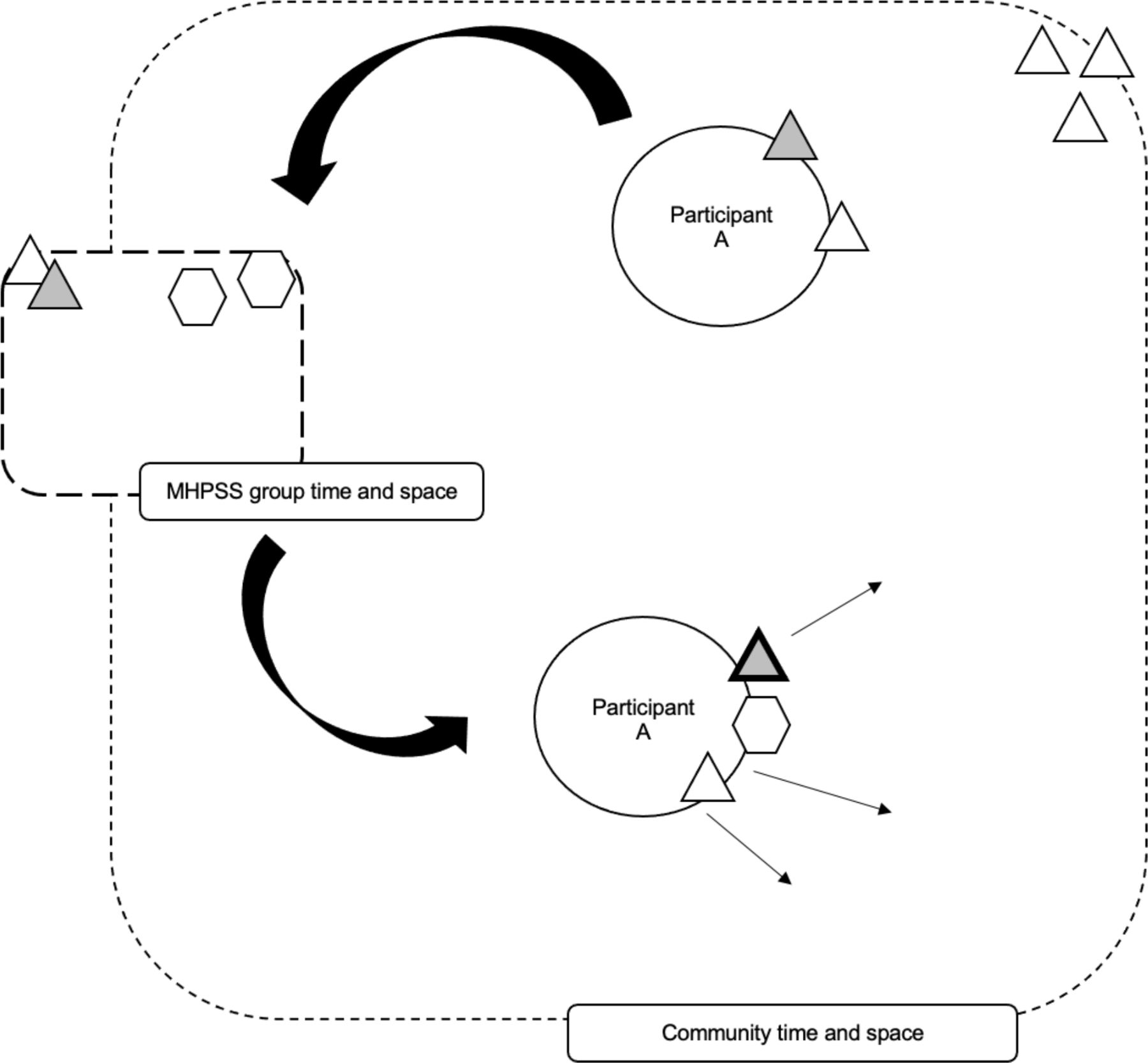
The author, CCA, screened records at the title and abstract phase, full-text phase, and extracted data to summarise study characteristics from included studies.18 The selection process is illustrated in a PRISMA diagram (figure 1).

PRISMA flow diagram. Exclusion reasons: (1) primary focus on traditional healer or healthcare/programme staff experiences, (2) qualitative study related to the assessment of resources, risk/protective factors and barriers/facilitators for intervention development, (3) qualitative study related to the assessment of local conceptualisations of well-being, resilience or healing, (4) not related to this review topic, (5) policy brief and (6) unable to access the record.
The quality of each included study was assessed with the Critical Appraisal Skills Programme (CASP) Qualitative Checklist (online supplemental material).19 This checklist provides 10 questions, 9 of which have a marking criteria of ‘yes,’ ‘no,’ or ‘not enough information.’ For question 10 (ie, how valuable is the research?), there is no marking criteria. In this review, the ‘value of research' was considered as the included studies’ relevance and usefulness in answering this review’s research questions and objectives. This was determined by CCA using three collective considerations: (1) the breadth of the data (ie, the quantity of detail provided in the ‘results’ section of the included study), (2) depth of the data (ie, severity of detail) and (3) whether the data could directly answer the review’s research questions and objectives. CCA did not create a detailed criterion or scoring system of the three collective considerations (eg, one to two sentences, one paragraph, or one page of data determining a score of ‘narrow’, ‘moderate’ or ‘wide’ breadth of data). The value of the research (ie, study relevance/usefulness) was assessed as ‘valuable’, ‘less valuable’ or ‘not valuable’.
The 10 marked questions were equally considered to assign ‘strong,’ ‘moderate’ or ‘weak’ to the overall study quality. The CASP Qualitative Checklist does not produce a scoring system for the overall study quality (eg, meeting nine or more criteria produces a ‘strong’ quality score); CCA determined a scoring system, for this review, in the interest of distinguishing study quality. The overall quality determined for each study include the following assessments: weak (0–4 of the criteria were fulfilled), moderate (5–7 fulfilled criteria) and strong (8–10 fulfilled criteria).
Data extraction, analysis and synthesis
All data extraction, analysis and synthesis processes were conducted by CCA. This review used thematic synthesis to analyse and synthesise qualitative evidence, following Thomas’ and Harden’s guidelines.20 The coding and generation of themes was an inductive process. The ‘results’ sections of each included publication were manually coded line-by-line. As all the included articles did not have the same research objectives as this review, CCA ‘inferred’ the kinds of MHPSS participant experiences and how these experiences occurred during the line-by-line basic coding phase.20 (p7) The basic codes were categorised and developed into descriptive themes to describe participants’ experiences. Descriptive themes were used to directly answer this review’s questions and were discussed among CCA and YO until analytical themes were generated. The review questions were considered cyclically through the development of analytical themes and modifications were made as needed. A thematic synthesis coding framework is detailed in table 1.
Thematic synthesis coding framework
Results
Selected studies and quality appraisal
A total of 955 records were identified: 953 records through database searching and 2 records through forward and backward citation searching. After the removal of 356 duplicates, the remaining 599 records were title and abstract screened for eligibility, 78 of which were considered at the full-text screening; 58 full-text articles were excluded. Twenty publications were included in this review, which came from 16 unique programmes carried out in the following 9 SSA countries: Rwanda (4 programmes, 8 publications),11 21–27 Democratic Republic of the Congo (DRC) (3 programmes, 3 publications),28–30 Mozambique (3 programmes, 3 publications),31–33 Sierra Leone (1 programme, 1 publication),34 Ghana (1 programme, 1 publication),35 Uganda (1 programme, 1 publication),36 Zimbabwe (1 programme, 1 publication),37 South Sudan (1 programme, 1 publication),38 and 1 publication included three countries (Sierra Leone, Liberia and Uganda).39 Two publications focused on refugee populations (Congolese refugees in Rwanda27 and Liberian refugees in Ghana35) and two were mixed-methods studies.36 38 The process of selection is detailed in figure 1. The study characteristics of included publications are in online supplemental material.
The quality of each study was assessed using the CASP Qualitative Checklist;19 appraisal ratings are found in table 2. Details of the quality appraisal ratings are in online supplemental material.
Quality assessment of included articles
Themes
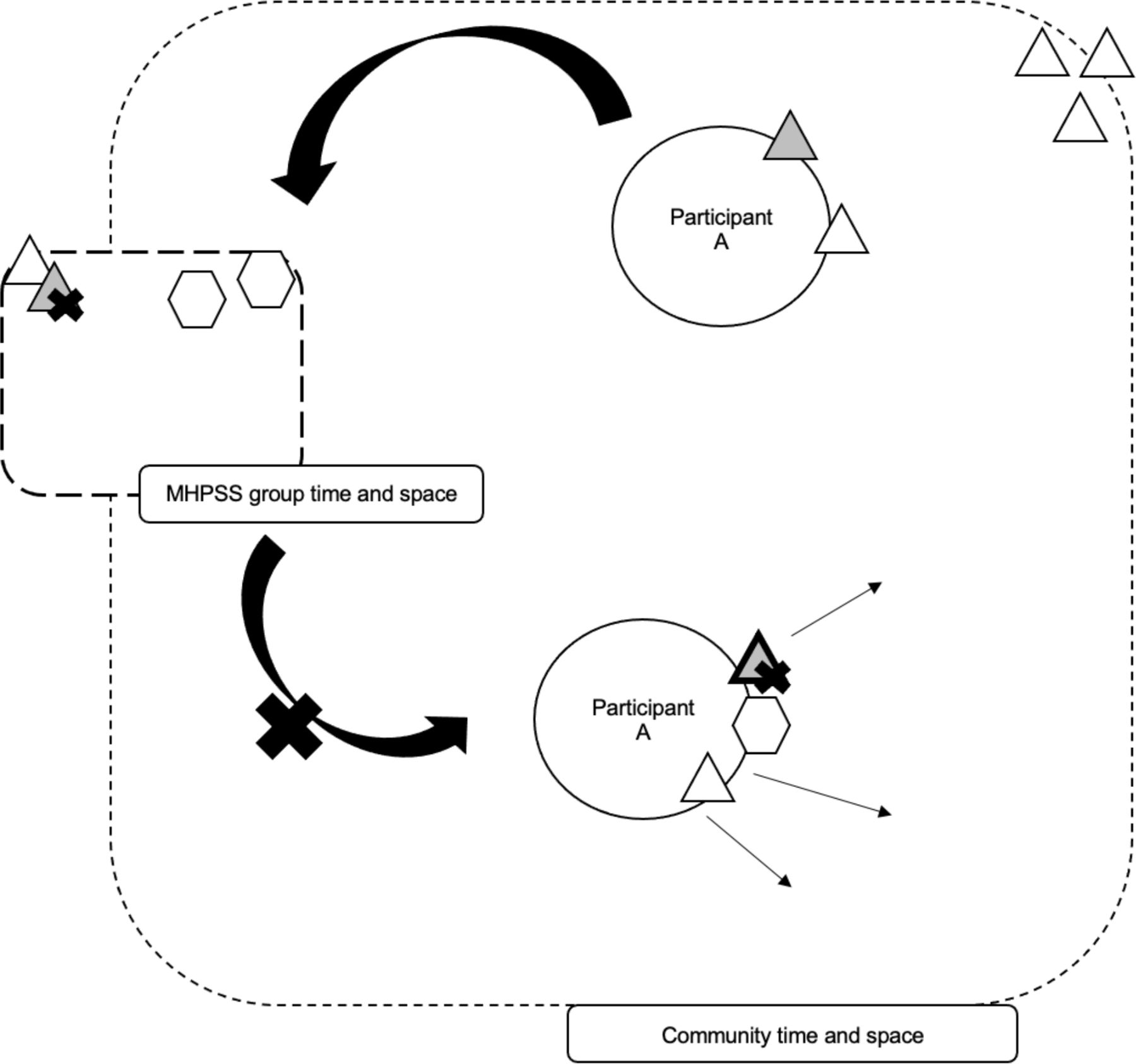
Thematic synthesis coding was conducted to answer the research questions concerning participants’ experiences of cc-MHPSS programme engagement and how these experiences happen. Analytical themes of participants’ experiences through their engagement in cc-MHPSS programmes include: (1) the experience of change in time and space, and (2) the experience of sharing and silence. These themes relate to each other in that elements from a cc-MHPSS programme and natural community are transferred between these settings and work therapeutically in participants’ process of engagement and healing. The transfer, or non-transfer, of elements among the cc-MHPSS programme and community settings relates to the sharing and silence of participants’ experiences. A thematic synthesis coding framework is in table 1. Visualisation of a transfer or non-transfer of elements may be found in figures 2 and 3, respectively.
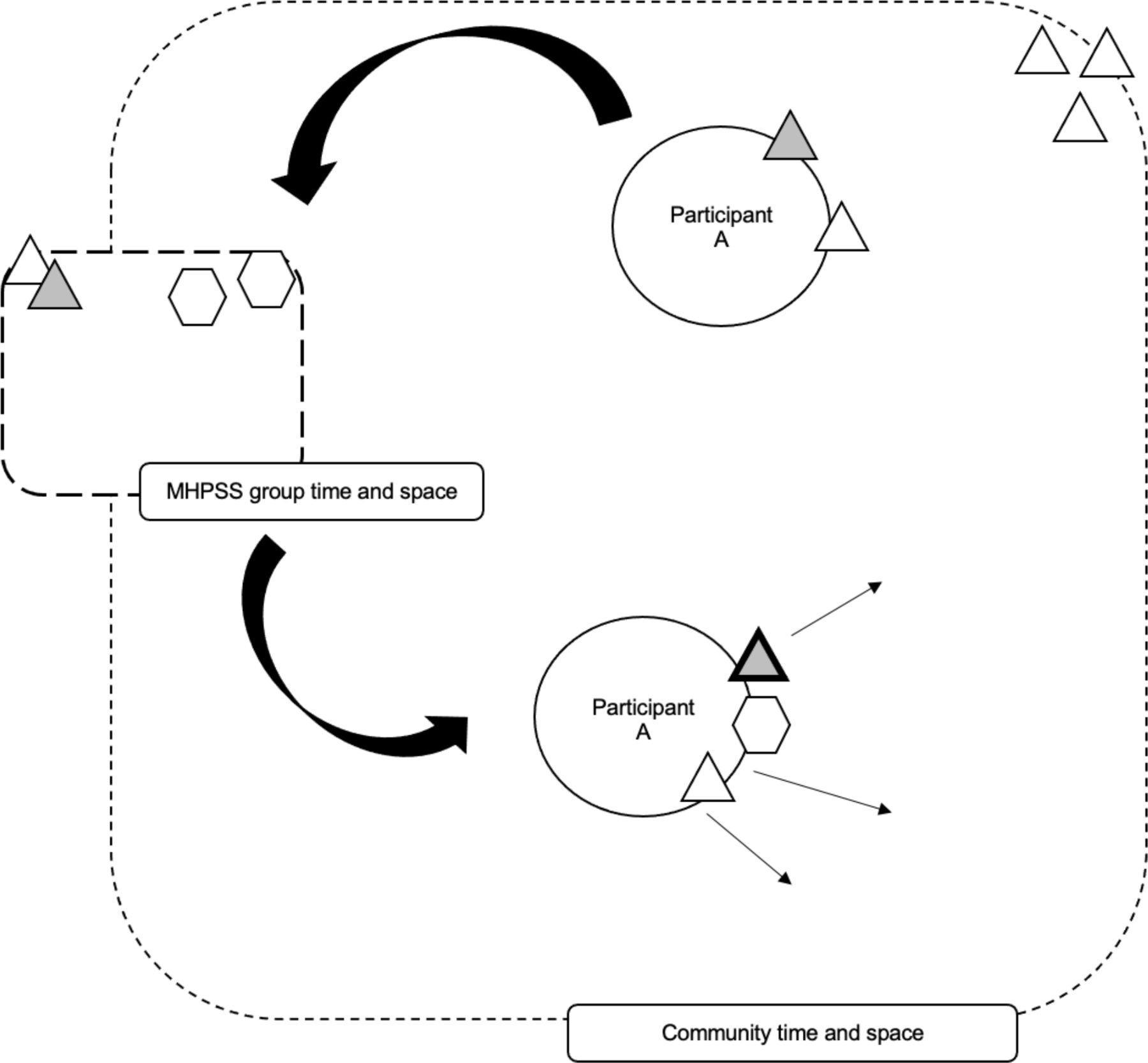
Visual of the transfer of elements between community and MHPSS group time-space. If, for example, conflict-related experiences (shaded triangle) from the natural community are labelled as ‘appropriate’ to share by the MHPSS group, this facilitates the transfer of this element from the natural community to the MHPSS group. This element is processed and transferred back into the community. Circle, participant A: the participant transfers the element (eg, conflict-related experience) from the community into the MHPSS group time-space, and back out to the community. Triangle: an element, such as a conflict-related experience or communal activity, from the community setting. Bolded triangle: a processed element from MHPSS group time-space. The participant is transferring this element back into the community. Hexagon: an element, such as a learnt session teaching, from the MHPSS group setting. MHPSS, mental health and psychosocial support.

{kind=link}
{kind=link}
{kind=link}
Visual of the non-transfer of elements (related to the silence of experiences) between community and MHPSS group time-space. If, for example, a community narrative of social categorisation is present in a MHPSS group and a participant’s categorisation does not fit within that narrative, then the sharing of a conflict-related experience (shaded triangle) may not occur in the MHPSS group. This is the non-transfer of that element. Thus, the processed element is not brought back into a community setting by the participant. Circle, participant A: the participant transfers the element (eg, conflict-related experience) from the community into the MHPSS group time-space, and may not transfer the processed element back out to the community. Triangle: an element, such as a conflict-related experience or communal activity, from the community setting. Bolded triangle: a processed element from MHPSS group time-space. The participant is not transferring this element back into the community. Hexagon: an element, such as a learnt session teaching, from the MHPSS group setting. MHPSS, mental health and psychosocial support.
The two themes are present throughout all included publications.11 21–39 As all data events are unable to be included, the following examples presented, best illustrate the themes.11 22–25 29 30
Theme 1: change in time and space
The theme of ‘the experience of change in time and space’ refers to the participants’ transfer of elements between the time and space of the cc-MHPSS programme and that of the wider community. By doing so, there is a change in participants’ perceptions and attitudes of their conflict-related experiences, identity, social connections and relationship to their community, which occur overtime. In this review, ‘time-space,’ will be used interchangeably with ‘time and space’. ‘Group(s)’, indicating the group-based nature of most of the included publications, is used interchangeably with ‘cc-MHPSS programme(s)’ (online supplemental material, ‘Programmes Description’).
‘Time’ refers to the planned and natural schedule of events, in which participants experience healing, whether within cc-MHPSS programmes or a wider community. ‘Space’ refers to the psychological and social structures in which participants experience healing, whether within cc-MHPSS programmes or a wider community. Psychological structures refer to instances in which participants may experience or narrate psychological or psychosomatic well-being (eg, distress, change or relief). Social structures refer to the instances in which participants interact, form or reform social connections.
Interaction between cc-MHPSS programme time-space and a natural community time-space
In the initiation of engagement in a cc-MHPSS programme, participants are transferring elements they experience in a wider community time-space into a group time-space, and elements they experience in a group back into a wider community. Elements that participants brought from communities into groups include conflict-related suffering (eg, narratives of the loss of family members, rape, torture or trauma),11 21–26 29–34 37 everyday issues (eg, daily stressors, issues related to agriculture, finances, family),22 24 25 27–29 32 35 36 38 39 community narratives (eg, societal norms or attitudes of what is acceptable and non-acceptable),21–27 29 31 34 39 and communal activities (eg, singing, dancing, advice giving).11 22–27 32 34 35 38 39 This is demonstrated throughout all synthesised articles.11 21–39 Through the act of transferring elements, a processing of elements occurs, in which there is a change in participants’ perceptions and attitudes.
Some elements from natural communities, such as communal activities, worked as community assets within groups. One such example is from participants of the Healing of Life Wounds (HLW) programme. The HLW programme is a community-based, group-based, mental health programme for adults and was implemented following the 1994 genocide in Rwanda. Following the session end, participants in the HLW programme would engage in communal activities, such as visit with each other to talk about the day’s session, sing, dance, recite poetry together, or attended a morning church service.39 These elements from a natural community were present within the group time-space and according to participant observations, the group ‘seemed to rekindle and nurture the practices that had been expelled from postgenocide life.’39 (p423) This is evidence that elements from the natural community time-space are integrated into the group time-space, along with evidence of change in the social connections among participants of the group.
However, some elements from the natural community, such as sensitive topics of the 1994 genocide in Rwanda were difficult for participants to present in the community time-space. Participants were more comfortable presenting these elements in the group time-space. Oftentimes, these participants were sharing their conflict-related experiences among a diverse group, which may mirror the wider community population and community narrative of the genocide. In King’s and Sakamoto’s 2015 study of the HLW programme, groups were made up of ‘survivors,’ those who were directly targeted by genocide and ‘nonsurvivors,’ those who were not targeted by the genocide.37 In this particular case, tensions that are present within the community narrative, arise in the group context. Rosa, a ‘survivor’ participant, remarked in the first session of the HLW programme:
‘I am tired of telling and hearing stories of the survivors alone about this and that, all about the genocide they experienced. I do not understand why those who were not hiding cannot tell us what they saw or know. If they did not do anything, or did, they were not hiding, if we are lucky to be gathered here, in a protected space, why cannot they tell us?’37 (p386)
King and Sakamoto indicate that Rosa’s remarks ‘seemed to be the expression of a desire for an audience that would confirm and legitimise the suffering of survivors.’37 (p386) Rosa’s remarks were not addressed by other participants in the first session. Emma, a ‘nonsurvivor’ participant, in the second session addresses Rosa’s remarks:
‘I was very hurt by the question that Rosa asked at the end of the first session. When she mentioned those who were not hiding, I felt she was talking about the Hutu and I happen to have that identity. And I am not saying that the Hutu did not do bad things. Sometimes I feel ashamed to talk about the genocide because it is almost like a family sin, committed by the members of the group to which I belong.’37 (p387)
This interaction demonstrates how elements from the community (eg, community narrative of the genocide) are transferred and integrated by participants into the group, which is an assumed ‘protected space’. Later, King and Sakamoto explain some instances of change, evidenced by the interpersonal connection and humanisation of the wider community within the group structure among the ‘survivors’ and ‘nonsurvivors.’ Such interactions and change within the group are suggested to have been translated to the wider community’s time-space.37
By contrast, some elements were shared within a natural community’s time-space but not transferred to a group time-space. In Otake’s ethnography, many study participants of the Musanze region in Rwanda were victims of the abacengezi war, the insurgency of the northwest event (1997–2003) (abacengezi meaning ‘infiltrators’), in which the majority Hutu inhabitants were massacred. Victims of the abacengezi war have received little government support (eg, MHPSS programmes), as the majority of the population are not survivors of the 1994 genocide. Since many victims of the abacengezi war did not have MHPSS programmes available to them, they engaged in other social groups within the community that facilitated healing experiences. For example, members of a church-based group would ‘visit(ing) and talk(ing)’ (‘gusura na kuganira’) with those who had socially withdrawn due to family loss. In these visits, talking would aid in socially withdrawn individuals’ social reconnection to the community. These topics would focus on talking with each other about scripture or events in the Bible, which would bring comfort to the participating group members. In this case, talking with each other did not focus on talking about traumatic conflict-related experiences, as is present in the groups of the reviewed articles.11 Otake suggests that the act of ‘visiting and talking’, through social reconnection, impacted participants’ healing. In this example, elements of the natural community, like this process of ‘visiting and talking’ with each other, are not transferred to group time-space since MHPSS programmes were not available to victims of the abacengezi war.
How then, does the transfer of elements happen from natural communities to groups, and vice versa? Across the reviewed articles, elements that were labelled by the programme as ‘appropriate’ to share and perceived by participants as ‘safe’ to share among the groups were likely to be easily moved from natural communities’ time-space to groups’ time-space. For example, a husband participant of a multicouple therapy (MCT) programme in the DRC shared his experience of witnessing others of the group share elements from the natural community. MCT was a group-based programme for torture-surviving, heterosexual Congolese couples, following the 1998–2003 conflict:
‘There was, for example, a diminishment of strength, for sexual relationship, and I thought it was just me in my marriage with my wife. Listening to/witnessing the others, it happened to others, too. They didn’t have strength from working, and the body was exhausted… I thought I lost a lot in the war. Then I got into the group, and I found that there were others who had lost, too. And to see friends who continued to have the same marriage, despite the suffering, that really encouraged me to say, ‘We, I can keep going with my wife in this marriage.’24 (p11)
One of the treatment goals of the MCT programme included ‘talking to one another (the respective spouse), as well as other couples about their experiences during war, including its effects on their relationship’ (online supplemental material, p5).24 Experiences during the war, elements from the natural community, are labelled as ‘appropriate’ to share based on the MCT treatment goals and perceived as ‘safe’ to share by participants. This facilitates the transfer of elements from the natural community time-space into the group time-space. This is evidenced by group participants sharing their experiences from conflict-time in the group time-space. In this husband’s experience within the group, ‘listening to and witnessing’ others share their experiences facilitated his recognition that he was not alone in his suffering of his marriage. The time-space within the group to share conflict-related experiences and receive others’ experiences (ie, listening and witnessing of others’ experiences) seems to allow for a processing of elements (eg, conflict-related experiences) from the natural community, as is also evidenced in King’s 2014 publication (ie, Anatole’s and Emma’s comments on [making] my story theirs, and I [making] theirs mine’).39 (p422) This example is visualised in figure 2.
Further, sharing experience and witnessing others’ experiences provides a starting point in the development of group member connections and relationships. This was the case of some of the participating women within a sociotherapy group programme, which was a community-based, peer counselling programme for adults in Rwanda following the 1994 genocide. The participating women in the programme shared their conflict-related experiences of rape and experiences of discrimination and social isolation:
‘[The women] discovered in the course of the sociotherapy sessions that they are not alone in their suffering…The women started to care for each other […] They even started to meet with some of the people they had deeply hated.’33 (p588)
In this case, the sharing and reception of conflict-related experiences among the women of the sociotherapy group also facilitated the recognition that they were not alone in their suffering. Following a processing of this element (eg, conflict-related experiences), the women formed social connections within the group and natural community. This is evidence that through participants, elements from the group time-space are successfully transferred and integrated into the natural community time-space.
Another instance of the transfer and integration of elements from the group time-space into the natural community time-space was that of a wife participant of the MCT programme in the DRC. She commented on how she was able to speak about the experience of rape from conflict-time within a group session: ‘The husband can understand the difficulty that I have. The man can hear what you asked there.’24 (p11) Markedly, processing within the group time-space allowed for the further processing of issues within the marriage in the natural community time-space. Morgan et al reported ‘many couples expressed that after in-group processing of the sexual violence, they could discuss the issue within their marriages.’24 (p11) In this case, wife and husband participants transfer the elements from the group time-space to be used in their marriages in the natural community time-space.
In addition, other elements from the group time-space such as the session teachings and materials were transferred by participants to the natural community time-space. Martha, a participant of the HLW programme, comments on sharing her HLW handouts with her daughter, who did not participate in the HLW programme: ‘I gave her the handouts to read and I encouraged her to come and sit with me and we did the exercises together.’39 (p423) Other participants of the HLW programme, who had limited readings skills, shared and completed their programme handouts with community members:
[The HLW participants] appreciated that they were able to remind themselves of the discussions held by asking another person to read the material aloud. They reported using these occasions to share what they had learnt.’39 (p423)
This is further evidence that participants facilitate a transfer of elements between the group and natural community time-space. This introduction and integration of elements from the group into that of the natural community time-space promote sharing reflections and communal sharing among group participants and community members. This suggests that healing and the process of engagement are not solely confined and designated to the group time-space. Healing and engagement processes may also happen in the natural community time-space.
The relationship between a cc-MHPSS programme and a natural community is dynamic. It is uncertain the extent of the elements brought into and out of each of the settings’ time-space, in which participants facilitate the transfer. Further, it is uncertain of the specific pathways of participants’ process of healing (ie, mechanisms which contribute to processing elements in and between the group and natural community time-space, how elements change, etc).
Theme 2: sharing and silencing, in relation to time and space
The previous section of ‘the experience of change in time and space’ described how various elements are transferred by participants between a cc-MHPSS programme and a wider natural community time-space. The elements’ transfer, or non-transfer, was often related to the ‘sharing and silencing’ of different experiences. The theme of ‘sharing and silencing’ refers to the disclosure, or non-disclosure, of participants’ conflict-affected experiences in the group and natural community time-space. Various topics elicited varying responses from participants.
Topics shared comfortably
In the previous theme, ‘the experience of change in time and space,’ some participants expressed appreciation for having the group time-space to share and listen to other group members’ experiences. These participants expressed that the time for sharing in the group was constructive and facilitated healing. Topics that were safe to speak about were most-commonly those representative of community life, collective identity, and topics accepted by culture and society. ‘Safe’ topics are related to the facilitated transfer of elements between the group and natural community time-space. These included shared farming,35 entrepreneurship,34 religious (Christian) events, singing, reciting poetry, dancing39 and extramarital sex, in which it is deemed non-acceptable behaviour in the community culture.33
Some participants reported the positive impacts of speaking about ‘safe’ topics in the group time-space. Ana, who participated in the solidarity groups in the DRC, spoke about the social improvement she experienced since joining the programme:
‘My situation has changed since joining the group. We meet each Saturday and learn how to herd…and how to farm vegetables that help life. We are beginning to work together in the home. In the community we talk together about the group, and share food.’35 (p364)
In Ana’s case, speaking of ‘safe’ topics, such as best herding and farming techniques, resulted in social connection with the solidarity group members and communal sharing (eg, shared farming and food). Another participant of the solidarity group, Nadia, speaks about how her relationship with the wider natural community has improved:
‘In the community it has changed because people know how to talk together through education of children and families. In the community, we set an example for the rest of the community to follow. The leader of the village tells children to listen to the group members.’35 (p367)
For Nadia’s case, participation in the solidarity group has increased her social connection with her community. This is evidence that elements, such as ‘safe’ topics, from the group time-space are transferred into the natural community time-space. Topics that are ‘safe’ to speak about in the group are also easily spoken about in the natural community time-space. For Nadia and other women of the solidarity group, it is evident that ‘their relationship within the community improved because they gained respect,’35 (p367) as ‘safe’ topics facilitated participant change, through the reformation of social connections in the community.
Uncomfortable topics
When a topic was not accepted by the community but was encouraged to share and voice in the boundaries of the group time-space, participants needed ‘courage’ to talk about it. For example, Faina, shared her experience of conflict-related sexual violence and issues with her husband within the sociotherapy group in Rwanda. Richters et al observed that Faina had the ‘courage’ to share only ‘part of her story’ with the group.33 Morgan et al observed that many of couples, participating in the MCT group in the DRC, had ‘developed the courage and strength to speak about their experiences, especially on learning that other couples had similar experiences.’24 (p11) This is related to the theme of ‘the experience of change in time and space,’ in that listening to and witnessing others share their conflict-related experiences facilitated the subsequent sharing of experiences from other couples and recognition that they were not alone in their suffering.
Differently, there were situations in which some group participants’ experiences did not fit a wider community narrative. In such cases, ‘the freedom to talk did not come immediately’ for these participants.39 (p422) King and Sakamoto explain that many Rwandans use the social categorisation of ‘survivors’ and ‘nonsurvivors’ to distinguish people who were or were not targeted by the genocide, respectively.37 (p385) ‘Survivors’ refer to ‘Tutsi and, in some cases, Hutu women who were married to Tutsi men, and their children.’ ‘Non-survivors’ refer to ‘Hutu men and women, perpetrators or bystanders. Tutsi women married to Hutu men may identify with either group (survivors or nonsurvivors), based on their experiences during and after the genocide.’37 (p385) The community narrative and social categorisation of ‘survivors’ and ‘nonsurvivors’ indicate that only some were affected or suffer from events of the genocide. In one of the first sessions of the HLW programme, King observes some survivors sharing experiences of familial death. Alternatively, she reports nonsurvivors’ non-disclosure on the experiences of familial death:
‘The survivors who were able to talk shared stories of the genocide and loved ones who were killed without going into detail or showing any emotion. The non-survivors did not talk about family members that had died, although it is well known that almost every Rwandan lost relatives in either the violence or the mass flight from the country. Many nonsurvivors focused on family and land-related conflicts, (including) theft of crops…these initial exchanges…created tensions between the members of both subgroups.’37 (p384-385)
Initially, a community’s narrative of social categorisation may impact the sharing and silencing of experiences in the group time-space. The experience of Emma, a ‘nonsurvivor’ participant of the HLW programme and whose experience did not fit in the community narrative, is presented:
‘The freedom to talk did not come immediately. At first, I did not feel that I had anything to tell those who were with me in the group…my small group members were people who have had problems during the war [genocide] and I did not feel that I could say anything… I wished I was transferred to another group.’39 (p422)
This is noteworthy in that Emma’s labelled social identity, of a ‘non-survivor’ among a group of mainly ‘survivors,’ could have contributed to her not disclosing her experience within her group. This example is visualised in figure 3.
By contrast, there were instances in which a group narrative was different from a wider community narrative. Otake suggests that implemented MHPSS programmes in Rwanda apply a Western-derived understanding of trauma and healing to post-genocide mental health, which did not fit with the natural community’s understandings of trauma and healing processes.11 One such example is the offered cc-MHPSS programme within the Association des Etudiants et Éleves Rescapés Du Genocide (AERG), a support organisation for genocide survivors. This AERG cc-MHPSS programme was a group-based psychological counselling programme. Murekatete, an active participant, expressed her connection with the AERG cc-MHPSS group, but also shared that she experienced social isolation from the local community:
‘I have not been able to be sociable with other people (of the local community). In fact, I do not do so. I ask myself what I can talk about with them […] Our lives are not similar so I haven’t been able to feel confident with others.’11 (p6)
In this case, Murekatete’s ethnic identity, a Tutsi genocide survivor, could have impacted her not forming social connections within the local community, in which the majority of the community members were Hutu victims of the abacengezi war.11 Though Murekatete disclosed her experiences within the group time-space, she did not disclose in the wider community; there was not a transfer of elements from the group to the natural community.
Discussion
This qualitative synthesis of cc-MHPSS programmes in conflict-affected communities within SSA investigated two objectives: (1) the kind of experiences participants have and (2) how participants’ experiences happen as they engage in cc-MHPSS programmes. Findings demonstrated that there is a transfer of elements between a group and a wider community time-space, which worked therapeutically in the engagement and healing processes. These processes may be demonstrated in both the group and natural community time-space. Global health programmes have emphasised the importance of community engagement,14 39–41 and previous literature has explained that a community-centred approach to MHPSS programmes is particularly important in order to ‘minimise risk of harm, maximise benefit and optimise efficient use of resources,’42 (p1) in the community. Engaging in the existing sociocultural contexts and systems within a natural community through a community-centred approach may impact the delivery, effectiveness, and sustainability of MHPSS programmes in humanitarian settings, though there could be resource limitations for delivery platforms due to the effects of conflict.6 These findings offer an additional explanation as to why cc-MHPSS programme engagement works therapeutically. That is, in order for this approach to be successful, it is important to let participants take initiative in bringing elements they know are therapeutic from their community to aid in the programme engagement process. There is also a cautionary note, as aspects that may have contributed to pre-conflict normality and tensions (eg, community narratives of discrimination or social categorisation) could be present and impede cc-MHPSS programme delivery and receptivity.
On the other hand, other elements, such as conflict-related experiences, were also transferred from everyday settings in natural communities and then addressed in groups through the engagement process. In particular, this review found such engagement happens when participants would share experiences and/or witness others’ conflict-related experiences in groups. Also, it is suggested that there is a processing of transferred elements present in programme engagement, though the specific mechanisms and extent is uncertain. Future research may be useful in determining the scope of transferred elements into MHPSS programmes and how these elements are processed during programme engagement, in relation to the natural community.
The sharing of experience among participants was vital in the treatment of negative elements, such as conflict-related experiences. Sharing is exactly the purpose of group-based therapy and previous reviews have shown its effectiveness.43 44 However, this review also highlighted silence, or non-disclosure, within both groups and natural communities. In this review, silence within groups happened when some participants’ experiences did not fit the wider community narrative. Meanwhile, silence in a wider community—a situation in which participants do not transfer elements from group to natural community—was reported when participants’ experiences were supported within a group but did not fit within the wider community. Previous studies of MHPSS programmes have focused on therapeutic impacts of sharing experiences.23 45 This review’s findings on silence shed light on a new aspect of cc-MHPSS programmes which may explain why some are ineffective, or even harmful. Namely, sharing uncomfortable topics, such as conflict-related experiences or ‘talking’ of trauma, can be an overemphasised MHPSS programme narrative. This may exclude or silence some participants seeking engagement in these programmes. These findings further justify the need to understand the cultural processes of healing and well-being in a SSA context, as the top-down, Western-derived application of psychological improvement is often overstressed. Other forms of engagement, such as sharing comfortable topics like shared farming or income-generation, are easily spoken about in both the group and community context and may aid in programme engagement.
These findings are valuable to the field because they expound on the relevancy of transferred elements by participants and the location of healing in participants’ experiences. This may be helpful in the determination of what is essential (ie, active ingredients) in the healing process of individuals in conflict-affected communities. Specifically, subsequent research may build on these findings by addressing (1) the scope of transferred elements into MHPSS groups and the natural community (and vice versa), (2) how MHPSS programme components can use or target participants’ transferred elements for healing and (3) the specific mechanisms of how participants’ transferred elements are processed while engaged in MHPSS programmes and natural communities. Future cc-MHPSS programme development, adaptation and implementation efforts may apply these findings, if considered contextually appropriate.
There are some limitations that have impacted this review’s synthesis of qualitative evidence. One such limitation includes the exploration of participants’ experiences through existing interpretations of data. As the included publications had distinct research questions, aims, methodology, and analyses, these foci differed from this review’s research objectives. For example, a hypothetical primary qualitative study exploring participants’ experiences and how the experiences occur in cc-MHPSS would ask different research questions, objectives, etc. Researchers’ ability to ask participants follow-up questions to further clarify experiences is not possible to conduct in a qualitative systematic review. To mitigate this limitation, the reviewer ‘inferred’ the types of participant experiences from the included publications’ differing contexts.20 (p7) This is a strength of this review in that identifying common themes across these various contexts may be applicable to the field of MHPSS programmes.
Additionally, due to time constraints in data collection, there were limitations present in the search strategy. The search terms used, in combination with the five concept domains, resulted in less than a 1,000 publication yield. For example, further expansion of the ‘MHPSS’ concept to include terms of therapies (eg, ‘cognitive–behavioural therapy’ or ‘narrative exposure therapy’) may yield greater publication search results in future reviews.
Lastly, only articles reported in English were included in this review; findings from other languages may have provided additional evidence concerning participants’ experiences.
Conclusion
In summary, this review highlighted that the processes of engagement and healing may be demonstrated in both the group and natural community structures. The transfer, or non-transfer, of elements is related to the sharing and silence of participants’ experiences in the group and natural community time-space. In the future, based on determined appropriateness and relevancy, these findings may be considered and assessed in the design of MHPSS programmes.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This review was detailed a priori in a research protocol and submitted to the Research Governance & Integrity Office at the London School of Hygiene and Tropical Medicine. Ethical approval was not required.
Acknowledgments
We aimed to remain cognizant and sensitive of the power dynamics between ourselves as foreign researchers removed from the current environment of conflict-affected communities within SSA and that of the participants who have contributed their lived experiences. The authors would like to show their gratitude to the participants who have contributed their lived experiences and researchers for documenting those experiences in the original studies. We would also like to thank Dr. Ritsuko Kakuma for her support of this project.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Stephanie M Topp
Contributors CCA is the guarantor of the research and accepts full responsibility. CCA designed the study, extracted data and analysed the data. CCA and YO both contributed to the search strategy, analysis of the descriptive and analytical themes, and contributed to the manuscript writing. Both have read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.