Article Text

Abstract
Introduction Sierra Leone, one of the countries with the highest maternal and perinatal mortality in the world, launched its first National Emergency Medical Service (NEMS) in 2018. We carried out a countrywide assessment to analyse NEMS operational times for obstetric emergencies in respect the access to timely essential surgery within 2 hours. Moreover, we evaluated the relationship between operational times and maternal and perinatal mortality.
Methods We collected prehospital data of 6387 obstetric emergencies referrals from primary health units to hospital facilities between June 2019 and May 2020 and we estimated the proportion of referrals with a prehospital time (PT) within 2 hours. The association between PT and mortality was investigated using Poisson regression models for binary data.
Results At the national level, the proportion of emergency obstetric referrals with a PT within 2 hours was 58.5% (95% CI 56.9% to 60.1%) during the rainy season and 61.4% (95% CI 59.5% to 63.2%) during the dry season. Results were substantially different between districts, with the capital city of Freetown reporting more than 90% of referrals within the benchmark and some rural districts less than 40%. Risk of maternal death at 60, 120 and 180 min of PT was 1.8%, 3.8% and 4.3%, respectively. Corresponding figures for perinatal mortality were 16%, 18% and 25%.
Conclusion NEMS operational times for obstetric emergencies in Sierra Leone vary greatly and referral transports in rural areas struggle to reach essential surgery within 2 hours. Maternal and perinatal risk of death increased concurrently with operational times, even beyond the 2-hour target, therefore, any reduction of the time to reach the hospital, may translate into improved patient outcomes.
- health systems evaluation
- health systems
Data availability statement
Data may be obtained from a third party and are not publicly available. Restrictions apply to the availability of these data. Data were obtained from the National Emergency Medical Service Operation Center and from the Referral Coordinators Database and are available from the authors with the permission of the Ministry of Health and Sanitation of Sierra Leone.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Maternal and perinatal mortality disproportionately affects low-income countries (LICs), where timely access to emergency and surgical care is often compromised by lack of transportation infrastructure and geographical distance, as described by the ‘Three Delays’ framework recommended by the Lancet Commission on Global Surgery.
A 2-hour threshold is internationally recognised for obstetric emergencies to access healthcare. A recent review identified only three studies in low-income and low-middle-income countries describing successful interventions implemented to increase the availability to timely surgical access.
The development of emergency medical services (EMS) in the African context represents a targeted intervention that has the potential to address the geographical and transportation barriers that contribute to the delay in reaching care, thus reducing the avoidable burden of disease associated to obstetric emergencies. However, available literature reports that only 16 African countries have a functioning EMS, to which is added the development of the first National Emergency Medical Service (NEMS) in Sierra Leone in 2018.
What are the new findings?
To our knowledge, this is the first nationwide study directly documenting prehospital operational times in relation to obstetric emergencies in an LIC.
Our results, based on more than 6000 obstetric emergency referrals, highlight a great heterogeneity countrywide regarding NEMS operational times.
There is a clear association between increasing prehospital time and maternal and perinatal mortality.
Key questions
What do the new findings imply?
Geographical distance to reach hospitals still poses a major barrier for timely access to care.
Different interventions, such as the strengthening of the existing primary health system and appropriate decentralisation of maternal care to peripheral facilities able to provide quality care, could reduce maternal and perinatal mortality.
Any reduction of prehospital times, even exceeding the 2-hour threshold, could translate into improved maternal and neonatal outcomes, a wake-up call for other LICs to invest in prehospital transportation infrastructure.
Introduction
Maternal and perinatal mortality constitutes a substantial proportion of burden of disease in low-income countries (LICs) and its reduction worldwide is included among the sustainable development goals to be reached by 2030.1 2 Timely access to prompt and safe surgical care constitutes one of the most important determinants for maternal and perinatal mortality.3 An indicative threshold of 2 hours is generally accepted for emergency obstetric surgical care, based on the estimated average interval between the onset of major obstetric complications and death, in the absence of interventions.4 In its 2015 report, the Lancet Commission on Global Surgery proposed to measure access to timely and essential surgery using the proportion of population that can access essential surgical resources, defined as the Bellwether procedures, within a 2-hour travel time (TT), an indicator that was also included in the WHO 100 Core Global Health Indicators.3 5 At present, however, little is known regarding the compliance to this target in LICs, and the few studies available show that serious gaps exist in accessing emergency obstetric surgical care within the above-mentioned time frame.6–10 To this regard, it is broadly acknowledged that poorly developed transportation infrastructure, lack of ambulance systems and geographical barriers play a major role in the so-called ‘second delay’—the delay in reaching care—described in the Three Delays framework,3 thus limiting access to timely emergency care in these countries.11
In the past 10 years, many sub-Saharan African countries have tried to develop emergency medical services (EMS) with the aim of providing prehospital care alongside prompt and safe transport to hospitals, in particular for obstetric emergencies.12 Despite the efforts, prehospital EMS currently exist in only one-third of African countries, and, when present, are generally limited in terms of population coverage, referral and communication network.13
Sierra Leone, one of the world’s poorest LIC that has long strived to tackle its high maternal and perinatal mortality, launched the first National Emergency Medical Service (NEMS) in 2018.14 The NEMS was designed to function as a tiered system of care initiated by peripheral health units (PHUs), responsible both for the primary assessment and care of patients and for the activation of the emergency medical dispatch of ambulances through a centralised operation centre (OC). NEMS is a free-of-charge service, and its fleet includes 81 ambulances, all of which are operative at the same time, and a total number of 450 paramedics and 450 prehospital care drivers, working to ensure timely and medically appropriate responses to each request for prehospital care and transportation to the nearest district hospital.14
The implementation of NEMS contributed to enhance access to healthcare especially for obstetrics and gynaecology cases and for people residing in the rural areas of the country.15 To understand countrywide variability in access to timely essential obstetric surgery following the implementation of NEMS, we aimed to perform an assessment of prehospital operational times for obstetric emergencies in Sierra Leone, and to evaluate the association between operational times and maternal and perinatal mortality.
Methods
Study design
This was a retrospective study analysing NEMS operational times in response to obstetric emergencies recorded countrywide between 1 June 2019 and 31 May 2020, thus including both the rainy (June to November) and the dry (December to May) season.
Study setting
The study facilities consisted of 1368 PHUs and 33 referral hospitals, including government district hospitals, faith-based clinics, and health centres managed by non-governmental organisations (figure 1). PHUs provide different levels of care, which can be described as ‘level one PHUs’ providing basic ante-natal and post-natal care and assistance to uncomplicated deliveries, and ‘level two PHUs’ offering basic emergency obstetric and neonatal care (BEmONC) services, which included the administration of antibiotics, oxytocics and anticonvulsants, manual removal of placenta and retained products of delivery, assisted vaginal delivery and basic neonatal resuscitation.16 Comprehensive emergency obstetric care (CEmOC) services, including all the BEmOC functions plus caesarean section and blood transfusion, were provided only at the district hospital level. Healthcare professionals in the PHUs were responsible for activating NEMS after providing primary assessment and care to pregnant women. The emergency requests received via phone from the PHUs were evaluated and managed by trained nurses at the NEMS OC. Subsequent phases entailed the dispatch of ambulance teams, composed of trained paramedic and an ambulance driver, and contact with the proposed referral facility.14 At the district level, ambulance to population ratio ranged from 0.8 to 1.8 ambulances per 100 000 inhabitants and ambulance distribution in the different districts was based on population density and the dimension of the geographical area covered.14 Treatment provided in the ambulances entailed oxygen delivery, administration of rectal misoprostol for prevention of postpartum haemorrhage, fluid resuscitation, assistance to labour and delivery, and basic life support manoeuvres. Ambulance personnel underwent a series of ad hoc basic training courses that included the management of medical, trauma, obstetrics, gynaecology and paediatric emergencies and basic life support and resuscitation manoeuvres without the support of automated external defibrillator.14
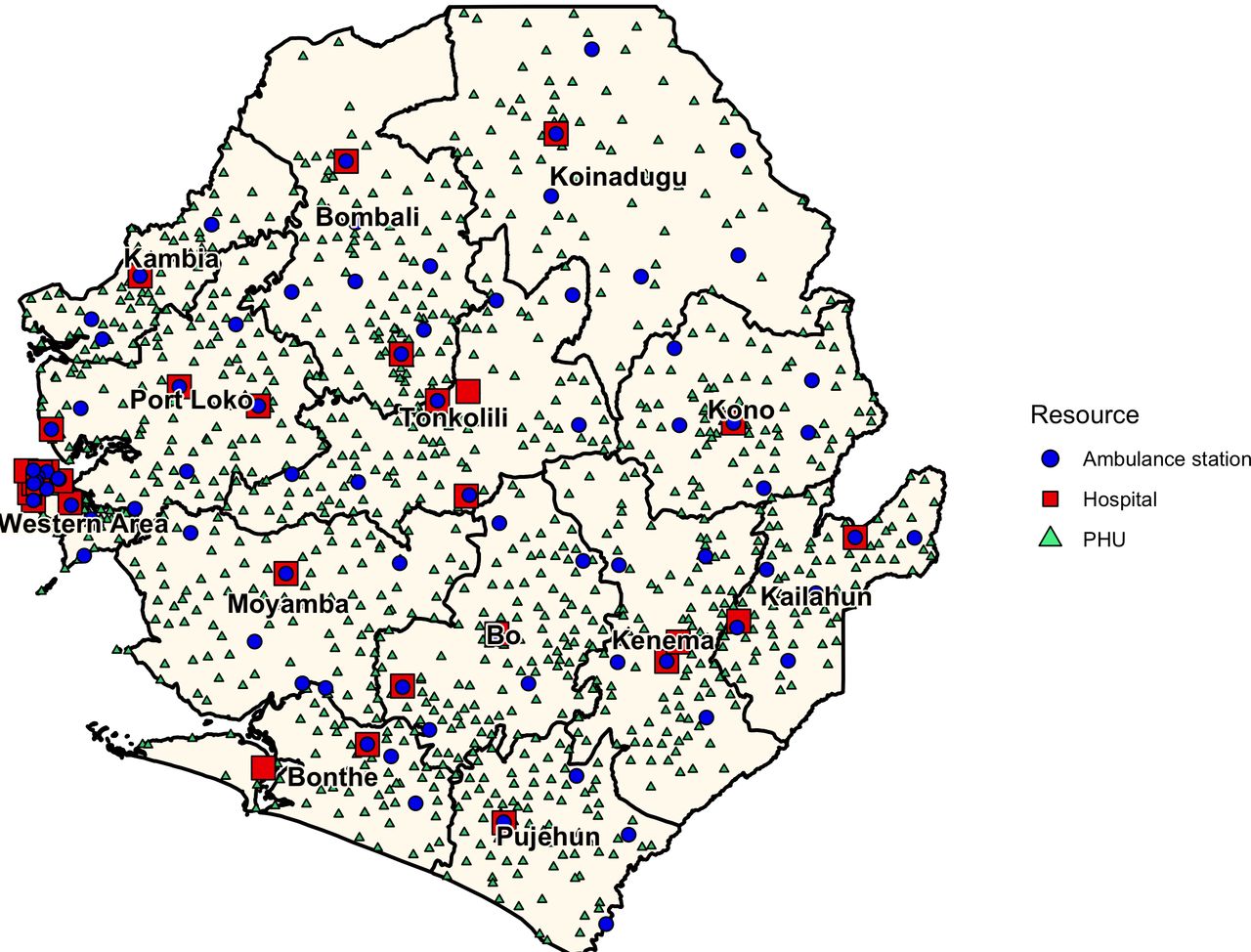
Distribution of district hospitals, peripheral health units (PHUs) and National Emergency Medical Service ambulances in Sierra Leone.
While currently managed by the Ministry of Health and Sanitation and financed though governmental budget, during the study period the NEMS has been managed and coordinated by a government-backed joint venture comprising Doctors with Africa (CUAMM, Padua, Italy), the Regional Government of Veneto (Italy) and the Research Center in Emergency and Disaster Medicine (Università del Piemonte Orientale, Italy) and financed by the World Bank.14
Although in July 2017 the new administrative division of Sierra Leone increased the number of districts from 14 to 16, the NEMS design and implementation was based on the initial district subdivision. Moreover, in this study the two districts of Western Area Urban and Western Area Rural, which included the densely inhabited capital city of Freetown and its surroundings, were analysed together as ‘Western Area’.
Data collection
Assessment of prehospital operational times
We retrieved prehospital data from the OC software, an in-house developed software for call-taking, triage, aided dispatching, mission monitoring and data collection. The OC software also recorded data on operational times received from the 81 ambulance units dispatched on the ground, as paramedics were required to contact the OC by cell phone at the following time points: (1) when leaving ambulance station, (2) when arriving at the PHU, (3) when departing from the PHU, (4) when arriving at hospital, (5) when departing from hospital and (6) when arriving at ambulance station. We used this information to calculate the prehospital time (PT), defined as the time elapsed between the receipt of the emergency call from the PHU and the arrival at the hospital facility. In addition, we defined other time variables of interest, which included dispatch time (DT), response time (RT), time on scene (ToS) and TT, described in figure 2. Additional data extracted by OC software included age of the patient, mission priority, mission complaint. We included in the analysis 6387 obstetric emergencies classified as ‘Red’ triage codes, clinically defined as ‘immediately life threatening’, while we excluded ‘Yellow’ triage codes, clinically defined as ‘not life-threatening but still serious’. Evaluation and triage of obstetric cases was performed by the OC operators through codes and scripted questions adapted from the Medical Priority Dispatch system,17 available on request from the authors. Data on the population of Sierra Leone and its districts were extracted from the 2015 Sierra Leone Census, as reported on the Sierra Leone Statistics website.18
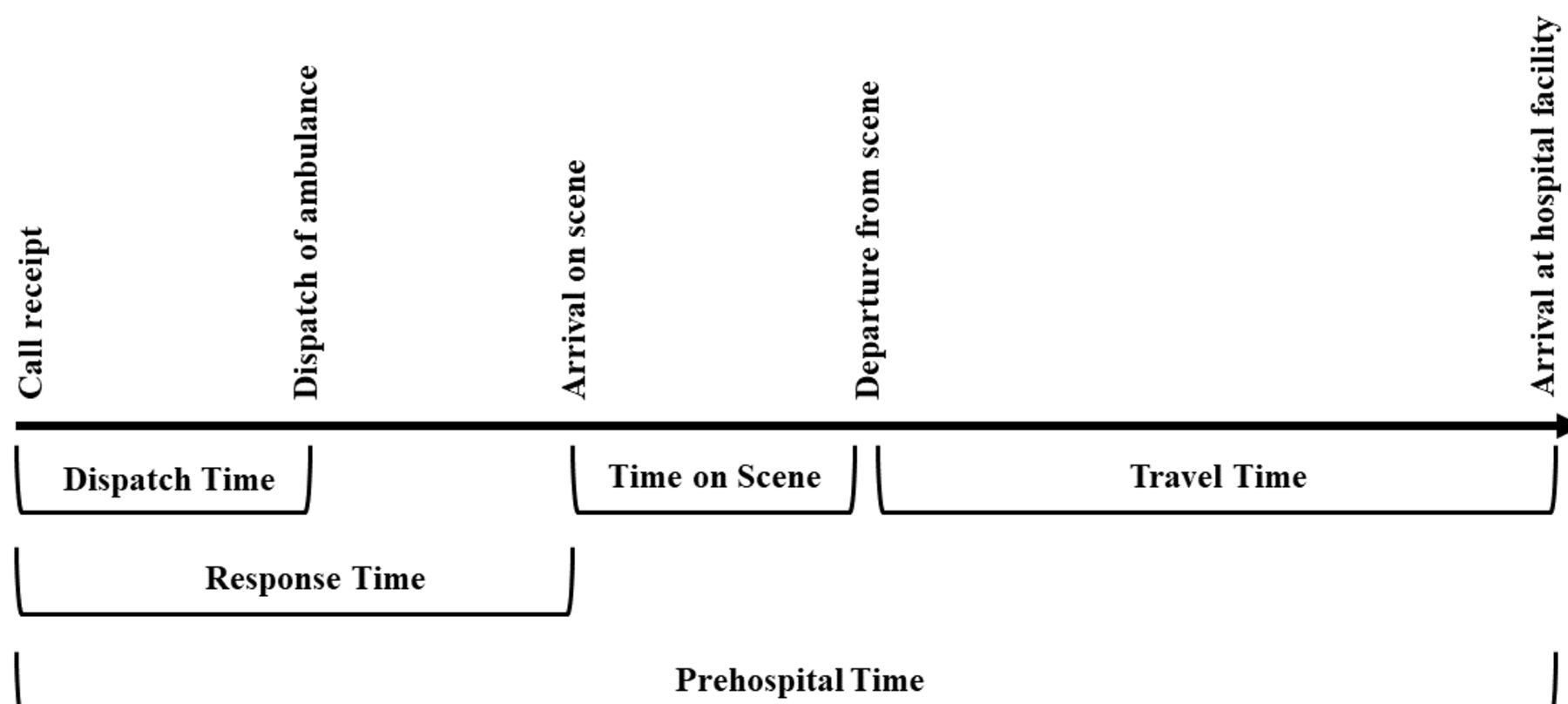
Prehospital operational times of the National Emergency Medical Service (NEMS) in Sierra Leone dispatch time: time between the receipt of the emergency call and the dispatch of NEMS ambulance. Response time: time between the receipt of the emergency call and the arrival at the peripheral health unit (PHU).Time on scene: time between the arrival at the PHU and departure from the PHU. Travel time: time between departure from the PHU and the arrival at the hospital facility. Prehospital time: total time elapsed between the receipt of the emergency call and the arrival at the hospital facility.
Evaluation of maternal and perinatal outcomes
We adopted the 10th Revision of the International Classification of Diseases (ICD-10) to define maternal mortality as ‘deaths from any cause related to or aggravated by pregnancy or its management (excluding accidental or incidental causes) during pregnancy and childbirth or within 42 days of termination of pregnancy, irrespective of the duration and site of the pregnancy’. According to ICD-10, the perinatal period included the ‘time frame that begins before birth and ends 28 days following the delivery.’ To evaluate the association between PT and maternal and perinatal mortality, we retrieved data from the national referral coordinators’ database, storing details on all incoming referrals collected at each hospital facility including in-hospital patient outcomes, a piece of information that was only available from January 2020 onwards. For this reason, we used a unique mission code to merge the above-mentioned database with a subset of data from the OC software, corresponding to 1717 referrals of obstetric emergencies recorded from 1 January 2020to 31 of May 2020. Among these 1717 obstetric emergencies, 1606 missions included maternal conditions also affecting the neonate, while the remaining 111 missions referred to conditions limited to the mother (eg, postpartum haemorrhage). All emergency obstetric referrals were classified according to the type of emergency recorded by the OC and based on patient assessment at the PHUs level.
Statistical analysis
For each district, we used median and IQRs to display the operational times and we estimated the proportion of missions that had a PT within 2 hours. The association between PT and mortality was investigated using modified Poisson regression models for binary data with robust estimate of the variance.19 Natural cubic splines were incorporated into the models to assess the shape of the association and allow for possible non-linear effects. The optimal degree of smoothing was chosen using a model selection procedure proposed by Royston and Sauerbrei.20 21 All the analyses were performed using Stata V.15 (StataCorp. 2017. Stata Statistical Software: Release 15. StataCorp).
Patient and public involvement
Patients and the public were not involved in the design of this study and in the dissemination plans of our research.
Results
Among the 6387 emergency obstetric referrals included in the analysis of the operational times, the majority of pregnancy-related complaints were antepartum haemorrhages (18.7%) and hypertensive disorders (16.7%), while delivery-related emergencies were mostly represented by obstructed labours (25.2%) and postpartum haemorrhages (15.8%) (table 1).
National Emergency Medical Services obstetric emergencies presented by type
Prehospital operational times
Except for the Western Area, which reported a median PT of 65 min, in all the other districts median PT ranged between 92 and 204 min (table 2). An analysis of the different operational times showed that DT and ToS contributed very little to the PT (overall median DT and ToS were 14 and 11 min, respectively), and were quite similar among districts. In contrast, median RT and TT differed greatly among districts (from 23 to 69 min and from 28 to 87 min, respectively) proving to be the determining factor for longer PT. At the national level, the proportion of emergency obstetric referral with a PT within 2 hours was 58.5% (95% CI 56.9% to 60.1%) during the rainy season and 61.4% (95% CI 59.5% to 63.2%) during the dry season (table 3). Results were substantially different among districts, with the Western Area reporting more than 90% of missions with a PT within the target and some rural districts reporting less than 40% (table 3).
Median (IQR) National Emergency Medical Services operational times for obstetric emergencies presented by district
Proportion of National Emergency Medical Services obstetric emergencies within the 2-hour target in the districts of Sierra Leone during the rainy and the dry season
Maternal and perinatal outcomes
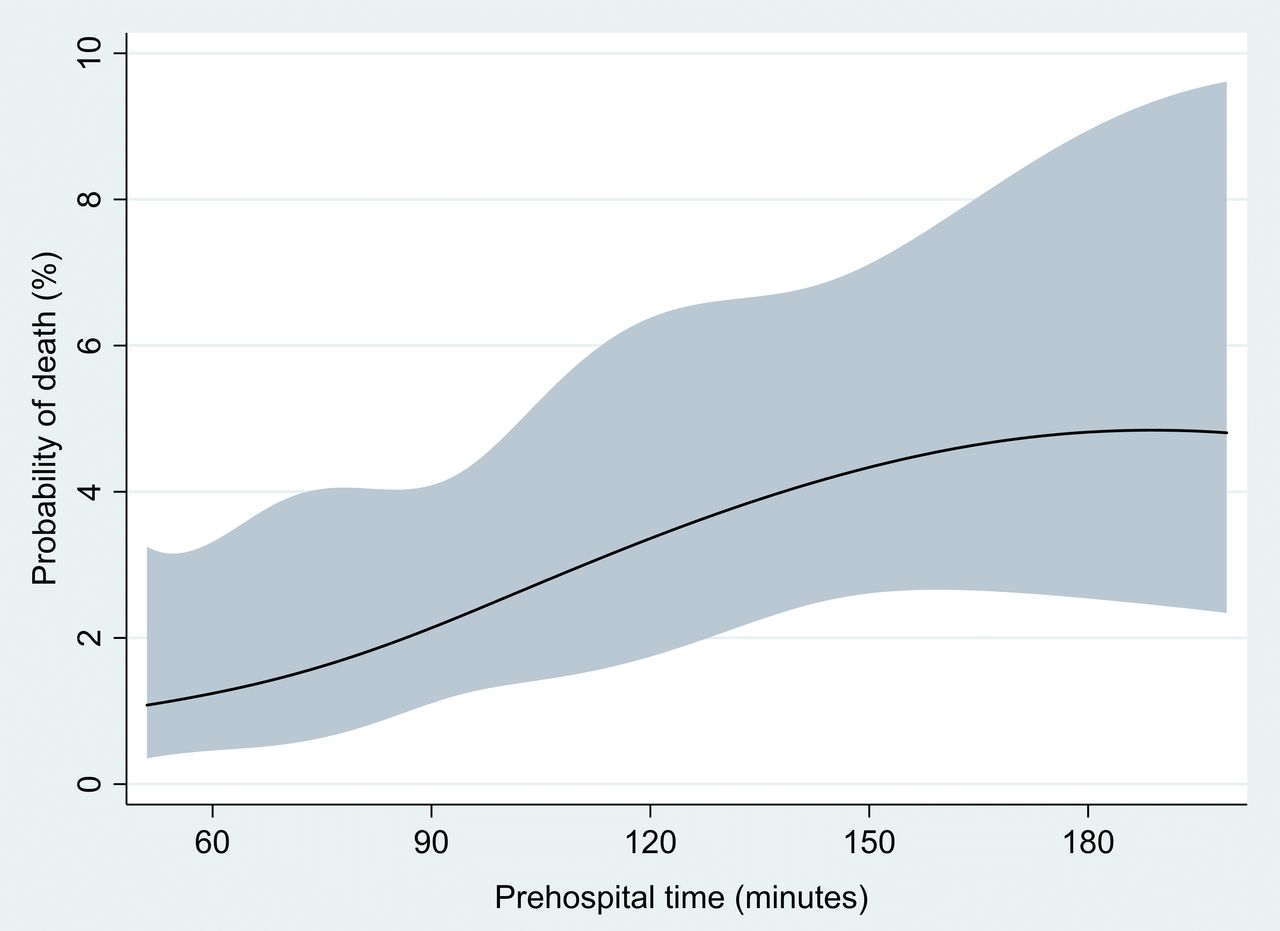
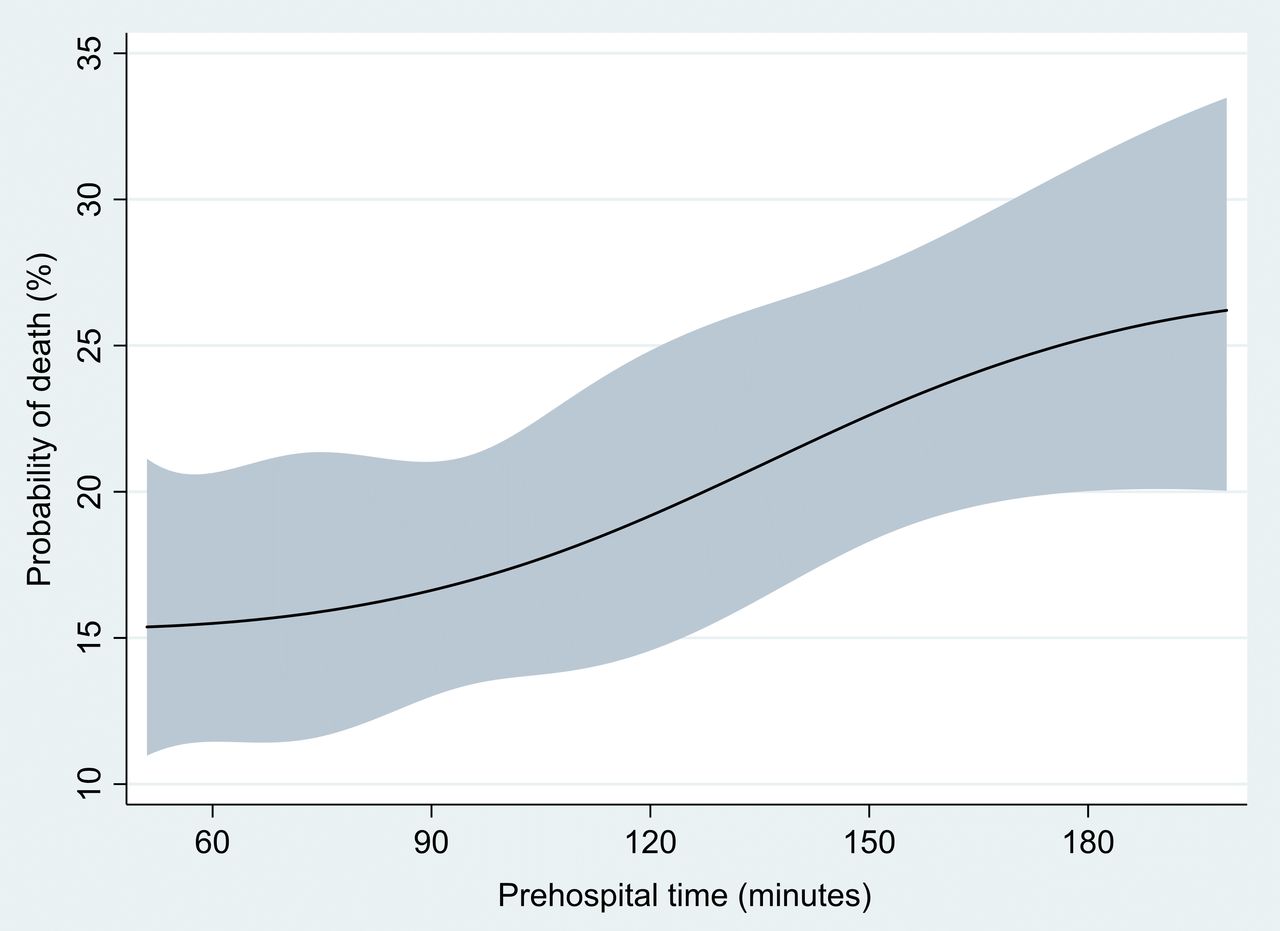
Between 1 January 2020 and 31 May 2020, out of the 1717 referrals of obstetric emergencies retrieved from the referral coordinators’ database, 41 and 211 missions resulted in the subsequent death either of the mother or the child, respectively. Specifically, we report two maternal deaths during transport and three on arrival to the hospital facility. With respect to perinatal death, we report 55 (26%) neonatal deaths and 156 (73%) stillbirths. Figures 3 and 4 show the association between PT and maternal and perinatal mortality. A continuous, monotonic increase in the risk of death for both mother and child was evident with increased duration of PT. Risk of maternal death at 60, 120 and 180 min of PT was 1.8%, 3.8% and 4.3%, respectively. Corresponding figures for perinatal death were 16%, 18% and 25%. On the relative scale, the association with PT was stronger for mothers, whose risk of death increases 2.4 times (from 1.8% to 4.3%) when passing from a PT of 60 min to a PT of 180 min. However, on the absolute scale the increase in risk was much larger for perinatal mortality, which increased from 16% to 25% in the same range of PT (figures 3 and 4).

Association between prehospital time and maternal risk of death.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between prehospital time and perinatal risk of death.
Discussion
In this study, we report the first countrywide evaluation of prehospital operational times for obstetric emergencies in Sierra Leone and its association with maternal and perinatal mortality.
Overall, the proportion of obstetric emergencies able to access hospital care within 2 hours using NEMS ambulances varied greatly among the districts, highlighting a significant difference between urban and rural areas. In the capital city of Freetown and its surroundings, characterised by the highest concentration of healthcare facilities and paved roads, emergency obstetric referrals were within 2 hours in more than 90% of cases. Conversely, the remaining districts, where districts hospitals are considerably fewer and road conditions are generally poor, reported different degrees of delay, contributing to the substantial burden of maternal and perinatal deaths in the country.
Not surprisingly, the underlying reason for longer PTs in rural areas was longer RT and TT intervals, thus reflecting the geographical distance between the PHUs and the district hospitals rather than possible system shortcomings. These findings are corroborated by other studies performed in African LICs where attempts to reduce PT are often hindered by long-distance travels,22 23 and confirm that distance is one of the most influential contributing factors to the second delay.24 Therefore, the addition of more ambulances distributed in strategic locations could represent a potential solution to cover the emergency demand and reduce RT, TT and therefore PT. Nonetheless, a cost-effectiveness analysis should be performed prior considering this option, as estimated NEMS current recurrent costs per ambulance ride and yearly cost per inhabitants are moderately higher compared with other African countries.15
Together with geographical distance, road conditions represent an important factor influencing NEMS ambulances’ speed and therefore time variables. As only 20% of the roads in Sierra Leone are paved,25 mostly concentrated in the area of Freetown, efforts to improve the public road network would lead to reduced ambulance TT.
Alternative solutions to obtain a reduction in time needed to reach proper obstetric care demand the strengthening of the existing health system. Specifically, in those areas reporting longer PTs and when the starting point is represented by a level one PHU, an intermediate stop to a level 2 PHU able to offer BEmONC services could be advised either to obtain patient stabilisation before further referral to district hospitals or to achieve definitive care, according to the type of obstetric emergency.
A second approach entails appropriate decentralisation of maternal care in selected PHUs, after being upgraded to provide CEmOC services, similarly to what has been developed in Tanzania.26 Although the long-standing debate between centralisation and decentralisation of maternal care is still ongoing and different strategies have been proposed to improve health systems in LICs,27 28 our findings suggest that Sierra Leone could benefit from a partial redesign of its health system, enabling some PHUs to support the existing hospital network in providing comprehensive obstetric care. While in the past years the country has witnessed an impressive growth in the number of PHUs nationwide,16 where however the quality of care provided is generally low, future strategies could envisage a quality-over-quantity approach, with the aim of better supporting pregnant women facing geographical barriers to reach district hospitals, and in line with WHO recommendation of having at least one CEmOC facility for every 500 000 population.4 As one of the major challenges in Sierra Leone is the chronic shortage health qualified workforce,29 the effort to scale up the current BEmONC PHUs should entail strategic measures such as the education and training of non-physician clinicians in providing CEmOC services, to obtain an adequate staffing level. This has been already achieved in Tanzania,30 where hands-on training, coaching, mentoring and supervision activities improved the safety and quality of care provided by non-physician clinicians.26
Beside the specific strategies adopted, it is noteworthy that any reduction of operational times is expected to substantially improve patient outcomes. Our study shows a clear association between PT and risk of maternal and perinatal death during obstetric emergencies. While the association between PT and perinatal mortality is well studied in high-income countries,31–33 only few studies evaluated the relationship between longer TT and adverse perinatal outcomes in low-income and low-middle-income countries,34–36 and quantitative data on maternal risk of death are even less investigated. The high rates of perinatal deaths reported in our study concur with the results of van Duinen et al,34 who reported a 19% perinatal mortality following emergency caesarian sections in Sierra Leone. Similar to what observed by van Duinen et al,34 our findings show that the 2-hour target did not represent an exact cut-off point, as both maternal and perinatal risk of death increased continuously and especially in the PT interval between 120 and 180 min, where the majority of PT values in rural districts are. These results further emphasise that every minute is crucial and even small reductions in operational times can translate into substantial improvements of maternal and perinatal survival, which should act as a wake-up call to action for investment on transportation infrastructure in LICs.
Nonetheless, it should be reminded that the 2-hour target mainly refers to the critical time from postpartum haemorrhages and death if no intervention is provided.4 There are other obstetric emergencies that might actually benefit from more advanced hospital care even when TT extend beyond 2 hours. In the current Sierra Leonean context, in case of prolonged and obstructed labour, when operative delivery is needed and not provided at the PHU level, centralisation may in fact be the only appropriate intervention to provide quality care especially as risk for complications dramatically increases with advanced stages of labour.37 In spite of international recommendation suggesting a 30 min decision-to-delivery interval in case of emergency caesarean sections,38 39 the achievability of this goal in low-income settings is still largely aspirational, while a more realistic target emerging from the literature is a time frame ranging from 2 to 5 hours.40 41 Therefore, improvements at the NEMS OC level to perform a more thorough triage of obstetric emergencies in order to establish different strategies within the ‘red’ codes category could support more targeted referral pathways especially in those districts experiencing longer TT. To this regard, future studies are needed to better investigate the relation between time and maternal and perinatal risk of death in the different categories of obstetric emergencies.
Some limitations of the study need to be considered. First, data on operational times were collected via mobile phone, a procedure that is not exempt from errors and inaccuracy, also considering the poor mobile phone reception in remote areas of the country. However, a quality check of the data of each mission showed consistency in the values of the reported operational times, suggesting that, overall, this approach was reliable. Second as we did not have any information regarding the TT from patients’ home to the PHUs, our study underestimates the total time elapsed between the occurrence of an emergency and the arrival at the hospital, which might represent a considerable part of patients’ journey time-wise. The degree of such underestimation is expected to be larger in the rural compared with urban areas, as the average distance between homes and PHUs is usually longer. Therefore, our estimate of the proportion of missions within the 2-hour target should be considered conservative and not completely comparable with those from studies using other methods, including total time from home.33 On the other hand, according to the 2016 annual report or Maternal Death, Surveillance and Response,42 before NEMS inception, when patients could reach hospital facilities either through private vehicles or paying public transport, the high number of maternal deaths reported at the hospitals’ level were associated with late referral from the PHUs. Therefore, while not providing a comprehensive evaluation of the ‘second delay’, we believe that in this context the estimate of the time elapsed from the first clinical assessment at the PHU to the arrival at the hospital constitutes an objective, reliable and useful indicator of the performance of the newly developed prehospital health system, highlighting existing gaps and area fur further improvements.
Conclusions
This was the first nationwide evaluation of prehospital operational times of Sierra Leone.
Apart from the capital city of Freetown and its surroundings, obstetric emergencies referred by NEMS still struggle to access hospital care and therefore essential surgery within a 2-hour time frame. The main reason for the delay in access to obstetric emergency care was related to the geographical distance from PHUs to district hospitals. Maternal and perinatal risk of death increased concurrently with operational times and any reduction of time to reach the hospital, even if still exceeding the 2-hour target, might translate into improved patient outcomes.
Data availability statement
Data may be obtained from a third party and are not publicly available. Restrictions apply to the availability of these data. Data were obtained from the National Emergency Medical Service Operation Center and from the Referral Coordinators Database and are available from the authors with the permission of the Ministry of Health and Sanitation of Sierra Leone.
Ethics statements
Patient consent for publication
Ethics approval
Comitato Etico Interaziendale AOU 'Maggiore della Carità' di Novara, ASL BI, ASL NO, ASL VCO, Protocollo 895/CE, ID CE 203/20; Office of the Sierra Leone Ethics and Scientific Review Committee.
Acknowledgments
The study was conducted in the framework of the International PhD in Global Health, Humanitarian Aid and Disaster Medicine jointly organised by Università del Piemonte Orientale (UPO) and Vrije Universiteit Brussel (VUB).
References
Footnotes
Handling editor Seema Biswas
Twitter @mirrorsandmaps
LR and FB-A contributed equally.
Contributors MC guarantor, conceived the presented idea, participated in project administration, data curation, formal analysis and investigation, drafted the article, designed figures and tables, and provided final approval of the version to be submitted; GP participated project administration, investigation and interpretation of results, critical revision of the article and provided final approval of the version to be submitted; AC designed figures and tables, critically revised the article and provided final approval of the version to be submitted; FT provided study resources, participated in critical revision of the article, interpretation of results, and provided final approval of the version to be submitted; AJ, MJV, DY, RB, SP and PR provided study resources, participated in critical revision of the article and provided final approval of the version to be submitted. IH and FDC supervised the present research, participated in critical revision of the article and provided final approval of the version to be submitted. LR participated in the study design, project administration and supervision, participated in critical revision of the article, interpretation of results and provided final approval of the version to be submitted. FB-A participated in the study design, project administration and supervision, performed formal analysis, provided study validation and designed figures, participated in critical revision of the article, interpretation of results and provided final approval of the version to be submitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The inclusion of any map (including the depiction of any boundaries therein), or of any geographic or locational reference, does not imply the expression of any opinion whatsoever on the part of BMJ concerning the legal status of any country, territory, jurisdiction or area or of its authorities. Any such expression remains solely that of the relevant source and is not endorsed by BMJ. Maps are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.