Article Text

Abstract
Congenital adrenal hyperplasia (CAH), if untreated, carries high morbidity and mortality. A higher incidence of CAH is expected in countries where consanguinity is common, such as in the countries of the WHO Eastern Mediterranean Region (EMRO). CAH is managed through lifelong treatment with fludrocortisone and hydrocortisone. In this analysis, performed in the 22 EMRO countries and territories plus Algeria, we review which countries offer a neonatal screening programme for CAH and describe the barriers and opportunities to access oral fludrocortisone and oral and injectable hydrocortisone. Neonatal CAH screening was only available nationally in Qatar, Kuwait and partially in Lebanon and Saudi Arabia. We reviewed the national lists of essential medicines (NEMLs) and found that 13/23 (57%) countries included fludrocortisone and 18/23 (78%) included oral hydrocortisone. Fludrocortisone was not included by any of the low-income countries and oral hydrocortisone was only included by one low-income country. We then contacted paediatric endocrinologists in each country to assess perceived availability of these medicines. Overall, there was a relatively good consistency between inclusion of fludrocortisone and hydrocortisone in the NEML and their actual availability in a country. We propose several mechanisms to improve access, including prequalification by the WHO, a common registration process for groups of countries, pooled procurement, working with local pharmaceutical companies, special access status for medicines not yet registered in a country and compounding. We suggest that access to medicines requires a collaboration between health professionals, families of patients, health authorities, pharmaceutical companies and the WHO.
- child health
- treatment
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Congenital adrenal hyperplasia (CAH) is an autosomal recessive condition that is managed through lifelong treatment with oral fludrocortisone and hydrocortisone, and, in case of emergency, injectable hydrocortisone.
It can be diagnosed early through neonatal screening, which is commonly performed in high-income countries.
Despite a scarcity of data, we found a higher incidence of this autosomal recessive condition in the countries of the WHO Eastern Mediterranean Region (EMRO), where consanguinity is highly prevalent.
Neonatal screening was only available in 4/23 countries.
We also observed that access to oral fludrocortisone and hydrocortisone was poorer in EMRO countries with a lower Gross National Income and highlight differences in the local channels used by paediatric endocrinologists to improve medicine access to patients.
We propose several approaches to improve access to medicines in general, and to fludrocortisone and hydrocortisone in particular, and emphasise the importance of collaborations between health authorities, patient groups, the pharmaceutical industry, health professionals and the WHO.
We also suggest that the higher incidence of CAH in the WHO EMRO should prompt more countries to develop a national neonatal screening programme for CAH.
Introduction
Congenital adrenal hyperplasia (CAH) is a genetic condition characterised by low or absent activity of the enzyme 21-hydroxylase in the adrenal gland. It causes decreased cortisol and aldosterone synthesis and, indirectly, increased production of testosterone by the adrenal gland. Clinically, the most important consequences are virilisation of the female fetus (while the genitalia of the male fetus have near normal appearance). In two-thirds of patients, salt wasting is present, resulting in hyponatraemia, hyperkalaemia and dehydration during the second week of life and, if left untreated, death.1
Many high-income countries have implemented a newborn screening (NBS) programme for CAH, whereby an elevated concentration of 17-OH progesterone, a substrate for the enzyme 21 hydroxylase, draws attention to the diagnosis.2 3 Early confirmed diagnosis of CAH ensures that management is initiated before clinical signs of adrenal insufficiency are present. Management of CAH is commonly performed with hydrocortisone and, when salt wasting is present, fludrocortisone (with or without salt supplementation). For emergencies, when hydrocortisone cannot be taken orally, such as in case of vomiting or a surgical procedure, injectable hydrocortisone is the treatment of choice.
Oral and injectable hydrocortisone and oral fludrocortisone are included in the WHO Model Lists of Essential Medicines (EMLs) for children4 and for adults.5 The WHO EMLs serve as a template for the development of national EMLs (NEMLs) by member states. Interestingly, while fludrocortisone and oral hydrocortisone are included in Section 18 of the WHO EMLs (‘Medicines for endocrines disorders’), injectable hydrocortisone is included in Section 3 (‘Antiallergics and medicines used in anaphylaxis’) and Section 8 (‘Immunomodulators and antineoplastics’).
Personal communications with Global Pediatric Endocrinology and Diabetes (GPED),6 a non-governmental organisation led by J-PC, and with other paediatric endocrinologists suggest that the availability of these medicines remains poor in Northern Africa, the Middle East and Western Asia.
The objectives of this analysis performed in the 22 countries and territories that are served by the WHO office for the Eastern Mediterranean Region (EMRO)7 and in Algeria, were first to review whether a NBS programme for CAH had been implemented, and second, to understand the barriers and opportunities in accessing oral fludrocortisone and oral and injectable hydrocortisone. Algeria was included in our analysis, despite being officially associated with the WHO African Region, because its language and culture are closer to those of countries included in the WHO EMRO. The information reported in this analysis was originally collected through a questionnaire in 2017. A follow-up to these survey responses (see Appendix 1) was conducted between December 2020 and June 2021 through email communications with one to four practicing paediatric endocrinologists in each country and a virtual discussion (J-PC or AR). The list of contributors per country is highlighted in the description of the GPED CAH Working Group.
Supplemental material
Most countries in the Eastern Mediterranean Region do not offer neonatal screening for CAH
In contrast to high-income countries, neonatal screening for CAH is not routinely performed in low-income countries, resulting in a delay in diagnosis and in high morbidity and mortality.8 Clinical recognition of this disease is particularly difficult in male neonates who do not present with abnormal genitalia. In these countries, the ratio of female to male neonates with CAH is greater than 1, reflecting the death of male neonates often without a diagnosis.9 10 In addition, in the absence of a registry or of established patient groups, the actual number of children with CAH is unknown.
The need for a NBS programme for CAH, a recessive condition, is particularly important in countries where consanguinity and birth rate are high such as in the EMRO region11 12 and was recently emphasised in Algeria.13 In Saudi Arabia14 and in the United Arab Emirates (UAE),15 published CAH incidences are 1:7908 and 1:9030, respectively. The incidence of CAH in the EMRO seems higher than the incidence of CAH determined through NBS in Japan (1:19 859 in Tokyo),16 Canada (1:19 510, in British Columbia, a province where 64% is from European ancestry and 28% from Asia),3 UK (1:18 000)17 or China (1:23 024).18 Assuming that the most conservative incidence of 1:9030 applies to the EMRO region, an estimated 2170 affected neonates would be diagnosed with CAH every year and treated early if the 19.6 million neonates born annually in this region were screened. Unfortunately, within the 23 countries we surveyed, we found that only Qatar and Kuwait, two countries that rank first and third, respectively, for Gross National Income (GNI) (table 1), offered a NBS programme. In addition, Saudi Arabia has a programme that covers more than 50% of the population and Lebanon offers NBS in a private hospital (table 2). A potential explanation is that high screening costs and logistic issues constitute a major constraint in initiating NBS for CAH in low-income countries. However, in those countries where a NBS programme for congenital hypothyroidism (CH) is already implemented, the existing infrastructure should make the addition of a NBS programme for CAH much easier.
Inclusion of fludrocortisone and hydrocortisone in the 22 NEMLs from WHO Eastern Mediterranean Region countries and Algeria available for review
Status of the neonatal screening for CAH and perceived availability of oral fludrocortisone, oral hydrocortisone and injectable hydrocortisone in the WHO Eastern Mediterranean Region and in Algeria
Fludrocortisone and hydrocortisone: two life-saving medicines
Overall, the market for oral fludrocortisone and hydrocortisone is relatively small. Fludrocortisone was patented in 1953 and is unique in its class. Its indication is mainly limited to the treatment of salt wasting in patients presenting with CAH or Addison’s disease. Assuming that two-thirds of patients are salt wasters and require an average dose of 0.1 mg per day of fludrocortisone, a ballpark estimate of the annual needs of fludrocortisone in the EMRO region for children aged 0–18 years is 9 410 000 0.1 mg tablets/year or 94 100 bottles of 100 tablets. Hydrocortisone was patented in 1936. In contrast to fludrocortisone, oral hydrocortisone is prescribed for a variety of reasons that include central and primary adrenal insufficiency. In addition, hydrocortisone, if not available, can be substituted for other corticosteroids such as prednisone and prednisolone.19 20 According to the recently developed WHO electronic EML,21 both fludrocortisone and hydrocortisone tablets have been included in the WHO EMLs since 2009.
Inclusion of fludrocortisone and hydrocortisone in the National Lists of Essential Medicines in the Eastern Mediterranean Region
We reviewed the 23 national EMLs for inclusion of oral fludrocortisone and of oral and injectable hydrocortisone. The mean GNI in the WHO EMRO and Algeria is US$10 373, similar to the average for the world in 2019 (US$11 558) but with major variability between countries (table 1).22 According to the World Bank, the 23 countries/territories that published a list of medicines were from the following income groups: six high-income (=26%: Bahrain, Kuwait, Oman, Qatar, Saudi Arabia, United Arab Emirates), four upper-middle-income (=17%: Iraq, Jordan, Lebanon, Libya), eight lower-middle-income (=35%: Algeria, Djibouti, Egypt, Iran, Morocco, Pakistan, Palestine, Tunisia) and five low-income (=22%: Afghanistan, Somalia, Sudan, Syria, Yemen). The most recent NEMLs were identified through the WHO website in two complementary locations21 23 and through a web search using the name of the country/territory and the key words ‘Essential List of Medicines’, ‘Drug reference price’, ‘Formulaire thérapeutique’ or ‘Nomenclature’. Information about a NEML (or a list of registered medicines if no NEML was found) was available for all 23 countries in the EMRO (plus Algeria) (table 1).
Thirteen (57%) countries we evaluated included fludrocortisone and 18 (78%) included oral hydrocortisone. Fludrocortisone was not included by any of the low-income countries and oral hydrocortisone was only included by one low-income country. In contrast, all countries included injectable hydrocortisone (table 1). Inclusion of medicines in the NEML only reflects current policies in the public health system of a country (vs reality) relating to essential medicines.
Availability of fludrocortisone and hydrocortisone in the Eastern Mediterranean Region
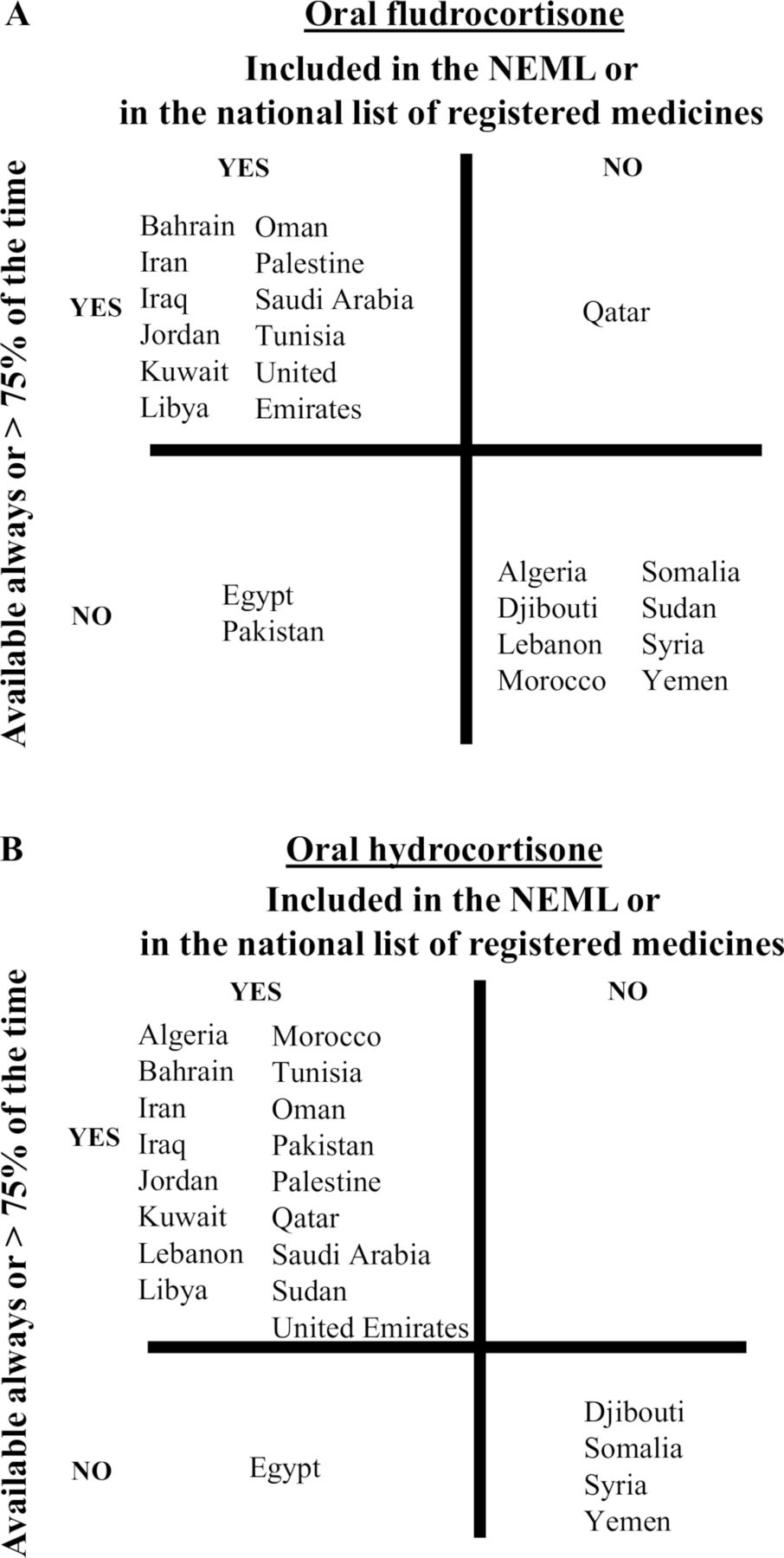
Overall, there was consistency between the inclusion of medicines in the NEML and their perceived availability in the country (figure 1). In countries at war or where the political situation is unstable, the availability of medicines varied periodically, such as in Libya. There was no available data for Afghanistan.

{kind=link}
Countries in the WHO Eastern Mediterranean Region plus Algeria according to the inclusion of fludrocortisone (A) and hydrocortisone (B) in the NEML and to whether the medicine was available more than 75% of the time as per the judgement of the local paediatric endocrinologist(s). Note that Afghanistan is not included in the figure as no information could be obtained concerning availability. NEML, National List of Essential Medicines.
In 11/13 countries that included fludrocortisone in their NEML, it was available more than 75% of the time. In 8/9 countries that did not include fludrocortisone in their NEMLs, it is available 50% of the time or less. In Qatar, a high-income country, fludrocortisone is not included in the national registry but is always available in hospitals for the treatment of specific diseases. In 17/18 countries that included oral hydrocortisone in their NEML, it is available more than 75% of the time. In contrast, in all four countries that did not include oral hydrocortisone, it is available 50% of the time or less (figure 1). Finally, consistent with its inclusion in the NEMLs, injectable hydrocortisone is available in all countries more than 75% of the time at least in hospitals, except in Yemen where it was identified as being available 50% of the time (table 2).
While an availability of 75% or more may be regarded as a good result at a country level, it means that the medicine remains unavailable up to 25% of the time, usually in an unpredictable manner, which remains suboptimal at the patient level.
The availability of oral fludrocortisone and hydrocortisone differs markedly in each country
To illustrate the variability in access to oral fludrocortisone and hydrocortisone, we highlight seven countries from the EMRO region (+Algeria) with GNIs that range from US$590 to US$43 470. We also compare the availability of a NBS programme for CH and for CAH in these countries and review whether education material on CAH was developed to improve the understanding of this condition in affected families.
Algeria (lower middle-income) has a generous public health system whereby many essential medicines are provided free of charge to the patient. NBS programmes for CH and CAH are not available. The only educational resources for families are Arabic translations of booklets published by the European Society for Pediatric Endocrinology. Oral and injectable hydrocortisone are included in the NEML and are available. In contrast, fludrocortisone, which is not included in the NEML, has never been available through the Algerian National Health Plan. It is either imported from Spain two times a year in bulk by compassionate health professionals and provided at cost or for free to the patients at the discretion of the paediatric endocrinologist or shipped directly by family relatives living abroad. In 2021 the Ministry of Health defined a process for access to medicines that are not currently registered in Algeria.24 A list of patients requiring fludrocortisone has been sent to the Ministry of Health by paediatric endocrinologists for funding consideration, and it is hoped that fludrocortisone will become available for these patients. Local production of fludrocortisone is also considered. Finally, a Facebook page for families of patients with CAH has been created to promote advocacy for this condition that affects at least 1000 patients in the country, with a majority of girls.
In Egypt (lower middle-income), NBS programmes for CH and CAH are not available and there are no educational publications on CAH. Fludrocortisone has been included in the NEML since at least 2006, before its inclusion in the WHO EML in 2009. Despite the presence of a local manufacturer (Amoun Pharmaceutical Co. S.A.E., Egypt, www.amoun.com), oral fludrocortisone is only available 50% of the time to the patient in some private pharmacies (US$0.025/0.1 mg tablet). A less common, different oral fludrocortisone tablet also produced by Amoun under licence from Merck (Merck KGaA. Germany, www.merckgroup.com) is intermittently available in some private pharmacies at a higher cost (US$0.038/0.1 mg tablet). In contrast, oral hydrocortisone was not included in the most recently updated EML and is rarely available to patients despite being produced locally (Misr Company, misrpharma.co/). When available, it is free to patients in the public system.
In Morocco (lower middle-income), NBS for CH is only available as a pilot programme in several academic centres and a NBS programme for CAH is not available. There is no educational material for families. Fludrocortisone is not included in the NEML and is never officially available in the country. However, for those who have the appropriate contacts, it is sent by relatives living abroad or is bought in pharmacies in Spain and brought back to Morocco by Moroccan citizens who regularly cross the border (US$0.18/0.1 mg tablet). To make the best use of limited fludrocortisone supplies, paediatric endocrinologists prescribe a low dose of fludrocortisone that is sufficient to prevent symptomatic salt wasting and increase the dose of hydrocortisone to increase its salt-retaining effect. There is presently no plan to add fludrocortisone to the NEML. Oral hydrocortisone is included in the NEML and is almost always available at a very affordable price (US$0.17/10 mg tablet, although it can be partially or completely covered by the government).
In Pakistan (lower-middle income) there is a pilot NBS programme for CH but no NBS programme for CAH. Information is available through an Urdu translation (by JR) of a booklet published in English by the Royal Children’s Hospital in Melbourne and given for free to families. Basic information on the diagnosis and management of CAH is also available on a mobile application prepared by the Society of Paediatric Endocrinology and Diabetes in Pakistan. Both oral fludrocortisone and hydrocortisone are included in the 2018 NEML but were not available to patients until recently. In 2020, thanks to the advocacy of a coalition of health professionals led by one of the authors (JR) and to several years of discussion between local and global manufacturers and the Health Authorities, a national manufacturer is now making and marketing hydrocortisone using an active pharmaceutical ingredient (API) imported from China. The tablets are available in pharmacies of the largest government hospitals where it is free, as well as in a few community pharmacies where it is available at a low cost (US$0.02/10 mg tablet). A concern raised by health professionals is that the sale price, mandated by the drug regulatory authority, may be unsustainable as the manufacturer may not be able to make a profit. Fludrocortisone is awaiting government clearance and it is hoped that after a transition period, it will be available for less than US$1 for 30 tablets through the same mechanism used for oral hydrocortisone. It is currently available less than 25% of the time and sold at US$1.5/0.1 mg tablet.
The Ministry of Health in the Occupied Territory of Palestine (lower middle-income) is the primary healthcare provider in the West Bank and Gaza, in which a socialised healthcare system provides universal and compulsory enrolment for most citizens. There is a NBS programme for CH, but not for CAH. No educational material is available for families. The government provides medicines to patients at a very low cost. Fludrocortisone and oral hydrocortisone are included in the NEML. Fludrocortisone is imported by a global manufacturer (Bristol Myers, https://www.bms.com/). If it is not available, families import the medicine through friends and family or from Israel. Oral hydrocortisone is manufactured by a Palestinian pharmaceutical company (Birzeit, http://bpc.ps/). Overall, the cost of a 0.1 mg fludrocortisone tablet is US$0.30 and the cost of a 10 mg hydrocortisone tablet is US$0.15.
In Sudan (low-income), oral and injectable hydrocortisone are included in the NEML. There are no NBS programmes for CH or CAH. Education material is being developed but is not yet available. Oral fludrocortisone was included in the 2014 NEML but was deleted from the 2019 NEML and is not registered in the country despite many discussions with health authorities. However, after requesting coverage from the national Medical Supply Department and the Government, hydrocortisone is sold at a low cost (US$0.2/10 mg tablet) and is available 75% of the time in medical supply pharmacies in Khartoum state. Tablets of fludrocortisone are obtained from various manufacturers at a similar price as hydrocortisone but are presently available less than 25% of the time. Availability is often lower in other states. If not available, patients get the medicines at a higher price in private pharmacies or import them with help from the patient’s family living abroad. Many efforts are led by Sudanese paediatric endocrinologists to secure these medications, to advocate with the health authorities and to try to get some supply from abroad whenever affordable. In the absence of fludrocortisone, paediatric endocrinologists add more salt to the diet and increase the dose of hydrocortisone by 25% to increase its salt-retaining effect. In the absence of hydrocortisone, paediatric endocrinologists prescribe prednisolone which is a relatively available and affordable option.
In the UAE (high-income), both NBS programmes for CH and CAH are available. There is no educational material in Arabic for families. Similar to other high income WHO member states, there is no perceived need for a NEML in the UAE. However, the Department of Health in Abu Dhabi, the capital, publishes a comprehensive list of registered medications which includes hydrocortisone and fludrocortisone tablets. Both fludrocortisone and hydrocortisone are readily available and are fully covered for the UAE citizens, while expatriates, who represent 80% of the residents, are covered through private insurance. Families of patients with CAH are often prescribed a vial of injectable hydrocortisone for home use in case of emergency.
Short-term and long-term opportunities to improve access to oral fludrocortisone and hydrocortisone
We have shown that the cost to the patient for hydrocortisone varied from US$0 to US$0.2/10 mg tablet and of fludrocortisone from US$0 to US$1.5/0.1 mg tablet in seven EMRO countries selected among the 23 countries we surveyed, emphasising the need to promote access to oral fludrocortisone and hydrocortisone in countries where they are not available. To officially market a medicine in a country, a pharmaceutical company typically needs to apply for registration. The process can be time consuming and costly, and requirements vary from country to country, which decreases the willingness of pharmaceutical companies to initiate this procedure especially for smaller markets. Importantly, some—but not all—manufacturers require fludrocortisone to be kept at 4°C versus room temperature. Registration of a brand of fludrocortisone that does not require a cold chain can make the logistics of storing and distributing the medicine much easier in particular in LMICs. Several approaches exist which, if implemented, could facilitate sustainable access to oral fludrocortisone and hydrocortisone. First, prequalification: in 2001, the WHO initiated a stringent review process whereby pharmaceutical companies apply to have their medicines or API prequalified by the WHO.25 The assumption is that registration of a product by national health authorities would be easier if it is included in the list of prequalified medicines. In addition, the WHO has also developed a Collaborative Registration Process26 27 that aims to actively support individual countries to achieve national registration of a prequalified medicine. As fludrocortisone and hydrocortisone are not presently prequalified, they are not included in the list of medicines eligible for accelerated registration. Of the EMRO countries, only Sudan is included among the countries presently participating in the Accelerated Registration of Prequalified of Finished Pharmaceutical Products. Second, a common registration process for groups of countries: in Europe, pharmaceutical companies submit a single marketing authorisation application to the European Medicines Agency. Once granted, a centralised marketing authorisation is valid in all European Union states. Several initiatives with similar goals such as the African Medicines Regulatory Harmonisation28 and the Regulatory Harmonisation in Maghreb (Tunisia, Algeria and Morocco)29 have been initiated but are, to our knowledge, not yet functional. Third, pooled procurement is a process by which several countries work together to develop a common approach towards medicines ordering.30 This approach makes it possible to place larger orders and to negotiate better prices and has already been championed by the Pan American Health Organization for a range of medicines.31 Fourth, working with local pharmaceutical companies/distributors: a global pharmaceutical company has little incentive to go through a sometimes-cumbersome registration and distribution process for a product where profit is expected to be modest. Working with a local pharmaceutical company that is familiar with the country’s regulations and that will take responsibility for registration and distribution, is another approach to promote registration of a medicine in a country. Five, special access to medicines that are not registered in a country: many countries have developed an official process whereby healthcare professionals may request access to non-marketed drugs to treat patients with serious or life-threatening conditions. For instance, Algeria is in the process of clarifying such a process that could ease access to fludrocortisone.24 Finally, compounded capsules or oral suspensions are potentially an affordable manner of providing hydrocortisone and fludrocortisone to patients in countries where commercial preparations are not available. The API for fludrocortisone and hydrocortisone can be bought in bulk and cost a fraction of the price of the tablet marketed by a manufacturer. The shelf life for compounded capsules or oral suspensions is however usually shorter compared with commercially available tablets. Many academic centres have posted recipes approved by their pharmacies for suspensions of hydrocortisone32 or fludrocortisone.33 Health professionals should investigate the national regulations for importation of API and for compounding of API by pharmacies in their country.
We propose that implementation of one of the options described above requires the collaboration of several stakeholders. Paediatric endocrinologists and patient organisations have a major role to play. Caring and Living as Neighbours (CLAN), an Australian non-profit organisation, champions a model based on the participation of patients and their families.34 The success of CLAN’s concept lies on the development of communities of patients that collaborate nationally and globally to increase awareness and connectivity.
Conclusion: it takes a village
Access to well known, affordable and life saving medicines such as oral hydrocortisone and fludrocortisone remains poor in many low-resource countries. Implementation of a NBS programme for CAH can provide incidence data and support the need for better access to treatment. It is hoped that the information included in this article will generate interest from the various stakeholders (patient organisations, paediatric endocrinologists, health authorities, manufacturers, WHO) to collaborate with each other and work on practical solutions to what seems to be a relatively simple problem. We also suggest that the various options proposed for the registration of fludrocortisone and hydrocortisone can be extended to access to medicines across a range of chronic health conditions. Beyond the management of patients, paediatric endocrinologists have a major role to play by bringing stakeholders together and advocating for change.
Ethics statements
Patient consent for publication
Ethics approval
The research ethics committee of the University of British Columbia felt that the use of publicly available data and the secondary use of anonymous data, with no involvement of human and animal participants, did not require approval by an institutional ethics committee.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Collaborators GPED CAH Working Group: Algeria: Bouferoua Fadila, Delileche Hana, Djahlat Larbi, Noumi Mustapha; Bahrain: Haya Alkhayyat; Djibouti: Abdourahman Douksie; Iran: Ali Rabbani; Iraq: Ali Al-Jumaili; Jordan: Rasha Odeh; Kuwait: Hessa Alkandari; Lebanon: Hala Tfayli; Libya: Suleiman Abusrewil, Millad Ghawil; Oman: Aisha Al senani; Occupied Palestinian Territory: Abdulsalam Abu-Libdeh; Qatar: Fawziya Alkhalaf; Saudia Arabia: Abdelhadi Habeb; Noman Ahmad; Somalia: Omer Elshareef; Sudan: Mohamed Abdullah, Olivia Al-Hassan; Syria: Dima Karah; Tunisia: Mongia Hachicha; Yemen: Mohammed Alshakka.
Contributors AR collected the majority of the data and wrote the draft of the manuscript; AD, AL, RH, SAM, JR, FJ and AA-L wrote a description of the health system with regard to access to fludrocortisone and hydrocortisone in their country/territory and provided a critical review of the manuscript drafts; JP-C designed the study, contributed to data collection and performed the final revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.