Article Text

Abstract
Acute respiratory tract infections (ARIs) are a leading cause of ill-health and death globally. Individual or multiple micronutrients have been shown to modulate immune function and affect the risk and severity of a number of infectious diseases. We systematically reviewed the evidence on the impact of micronutrient supplements to reduce the occurrence of ARIs and shorten the duration of ARI symptoms among adults. Random effects meta-analyses were conducted to estimate the pooled effects of vitamin D, vitamin C, zinc and multiple micronutrient supplementation (MMS) on the occurrence of ARIs and the duration of ARI symptoms. Vitamin D supplementation reduced the risk of ARI (risk ratio (RR)=0.97; 95% CI 0.94 to 1.00; p=0.028) and shortened the duration of symptoms (per cent difference: −6% (95% CI −9% to −2%; p=0.003)). The RR of vitamin D to prevent ARI was farther from the null when diagnosis was based on clinical diagnosis or laboratory testing, compared with self-report and when the loading dose was <60 000 IU. Vitamin C supplementation reduced the risk of ARIs (RR=0.96; 95% CI 0.93 to 0.99; p=0.01) and shortened the duration of symptoms (per cent difference: −9% (95% CI −16% to −2%; p=0.014)). The effect of vitamin C on preventing ARI was stronger among men and in middle-income countries, compared with women and high-income countries, respectively. Zinc supplementation did not reduce the risk of ARIs but shortened the duration of symptoms substantially (per cent difference: −47% (95% CI −73% to −21%; p=0.0004)). Our synthesis of global evidence from randomised controlled trials indicates that micronutrient supplements including zinc, vitamins C and D, and multiple micronutrient supplements may be modestly effective in preventing ARIs and improving their clinical course. Further research is warranted to better understand the effectiveness that individual or multiple micronutrients have on SARS-CoV-2 infection and treatment outcomes.
- epidemiology
- nutrition
- prevention strategies
- respiratory infections
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Vitamin C and D supplementation reduce the risk of acute respiratory tract infections (ARIs).
Vitamin C and zinc supplementation shorten the duration of ARI symptoms.
What are the new findings?
The preventive effect of vitamin D against ARIs is greater when the diagnosis is based on clinical diagnosis or laboratory testing, rather than self-report. An optimal dosing regimen would include a daily dose ≥2000 IU vitamin D and a loading dose <60 000 IU.
Vitamin D supplementation shortens the duration of ARI symptoms mildly, though the effect did not differ by dose.
The preventive effect of vitamin C against ARIs is greater among men and residents of middle-income countries.
Zinc supplementation has no effect on the risk of ARIs.
What do the new findings imply?
Micronutrient supplementation may prevent (vitamin D and C) and treat (vitamin D, C and zinc) for ARIs, including SARS-CoV-2 infection. It is unclear whether the magnitude of the effects of these micronutrients are clinically meaningful.
The efficacy and safety of micronutrients, provided at the dose ranges at which their effects are strongest, need to be tested in randomised trials among patients with COVID-19 and other severe respiratory infections.
Introduction
Acute respiratory tract infections (ARIs) constitute a substantial global burden of disease. ARIs were the third leading cause of death globally in 2017.1 ARIs are caused by bacteria and viruses—and a large proportion of cases are due to RNA viruses. Every year, seasonal influenza epidemics affect 3–5 million cases and result in >300 000 deaths globally.2 SARS-CoV-2, a novel enveloped non-segmented RNA virus, is the cause of the ongoing COVID-19 pandemic.3 Between December 2019 and November 2020, there have been more than 60 million confirmed cases of COVID-19 and almost 1.5 million deaths. There is currently no known curative therapy for the disease.
Early reports suggest that severe COVID-19 disease and deaths have been more frequent among older adults, with lower risk and severity among children.4 5 Understanding the influence of nutrition in preventing and treating ARIs could guide the design of public health programmes. Previous studies have demonstrated the association of nutrient depletion and the risk of infectious diseases.6 A number of reviews have summarised findings from randomised trials of vitamin D,7–11 vitamin C12–14 and zinc15–18 to prevent and treat ARIs. These reviews were not focused on adults, and did not carefully consider the influence of dose or comprehensively consider the effect of multiple micronutrients towards identifying a suitable micronutrient package to prevent or treat ARIs.
The goal of this paper is to synthesise the evidence from randomised controlled trials (RCTs) of micronutrient supplementation to prevent and treat ARIs in adults. We evaluated the effectiveness of micronutrient supplements in (1) Preventing ARIs, and (2) Reducing the duration of ARI symptoms.
Methods
Systematic literature search and selection of studies
We searched the medical literature databases, Medline and EMBASE, for original research articles published as of March 2020. Medical subject headings and keywords representing micronutrients (vitamins A, B, C, D, E or zinc) and ARIs were employed (online supplemental table 1). No restrictions were made in the search based on pathogen, age, year or language of publication (however, articles for which there was no standard translation were excluded during full-text review). We also searched through the reference lists of included papers and published systematic reviews by hand. The titles and abstracts of identified studies were screened, and full texts were examined. Influenza, caused by enveloped RNA viruses, Influenzavirus A and B,19 was the main ARI of interest. We included RCTs that examined the influence of micronutrient supplementation on the occurrence of any ARIs or duration of symptoms. In vitro studies, case studies, case series and observational studies (prospective and retrospective) were excluded. Studies were also excluded if they included only individuals aged <18 years or if the mean age of included participants was <18 years.
Supplemental material
Data on study design, population characteristics, exposures, outcomes, covariates and findings were abstracted from the included studies, including point estimates with CIs, SEs and p values. These include means, medians and mean difference for continuous outcomes and risk ratios (RRs), ORs and HRs for categorical outcomes. The SD was assumed to be equal to the mean if the studies did not report any measures of uncertainty. For studies that reported summary data for exposed and unexposed participants, RRs and HRs were estimated as appropriate using the epiR package in R.20 Additional information on the prevalence of baseline 25(OH)D concentration <25 nmol/L was extracted from a published pooled individual patient data meta-analysis.10
Risk of bias was assessed using the Cochrane Collaboration’s revised tool for assessing risk of bias in randomised trials.21 No inclusion or analysis decisions were made based on risk of bias.
Meta-analysis
We pooled estimates for exposure-outcome relationships reported by four or more studies. If different approaches were used to measure the outcome, the more objective or precise outcome measure was preferred. Thus, for studies reporting on the occurrence of infection, RT-PCR and serology were preferred to clinical diagnosis, and self-report by patients was the least preferred diagnosis approach. If multiple doses of exposure were reported, the most extreme categories meeting the criteria for inclusion were included in the meta-analysis.
Random effects meta-analysis based on the maximum likelihood was conducted. The random effects approach was selected a priori because it accounts for variability in the true intervention effect. Pooled risk ratios (RR) were obtained for the occurrence of infection and percentage differences were obtained for the duration of symptoms. Percentage difference was estimated as the log-transformed ratio of the mean duration of symptoms in the treatment and control arms.22 Percentage difference was preferred to the weighted and standardised mean difference measures because, it is easily interpretable, and it accounts for differences in estimating the duration of symptoms.23 24
Heterogeneity was assessed with Higgins’ I2 statistic, a measure of the total variability due to between-study variation. I2 was regarded as substantial if 50%–90% and considerable if >90%.25 Heterogeneity was further assessed using meta-regression approaches and analysis within subgroups defined by country-income classification, age, diagnostic method, and loading and maintenance doses. The effect of micronutrient supplements in subgroups defined by the type of ARI (such as common cold) was examined where possible. Dose-response analysis was done using a single predictor and multiple meta-regression. Alternative models for multiple meta-regression were considered and the best model was the model with the lowest Akaike information criterion. In some cases, sensitivity analyses were conducted, by altering the parameters of inclusion in the main analyses and comparing findings. Publication bias was evaluated with visual inspection of funnel plots. Double-sided p values were estimated, and significance was set at p<0.05. Meta-analyses were conducted using the Metafor package26 in RStudio V.1.0.153.27
Results
We identified 80 RCTs (figure 1) that examined the effect of micronutrient supplements on the risk and clinical course of ARIs. These studies enrolled individuals across 17 high-income countries, and 5 low-income and middle-income countries. Meta-analyses of the effect of micronutrients on the risk of ARI and duration of symptoms were done when possible (tables 1–3). Risk of bias for all studies is presented in online supplemental table 2 and summarised in each section below.

Flow chart of selected studies.
Vitamin D—summary of meta-analyses findings—main and subgroups
Vitamin C—summary of meta-analyses findings—main and subgroups
Zinc—summary of meta-analyses findings—main and subgroups
Vitamin D supplementation
Occurrence of illness
Twenty studies examined the effect of vitamin D supplementation on ARI risk among 9902 adults (online supplemental table 3). These studies were conducted in Australia,28 Canada,29 Finland,30 Japan,31 32 the Netherlands,33 New Zealand,34–36 Sweden,37 the UK38–40 the USA.41–47 The studies provided daily doses alone,30 31 37 46 daily doses after a single loading or monthly dose,32 43 or large single, weekly or monthly doses only.28 29 34 35 38–40 44 47 Doses used were 400 IU30,32 1000 IU33,46 2000 IU41,42 or 4000 IU37,43 daily; 10 000 IU29 weekly; or 60 000 IU47 or 200 000 IU34,44 monthly. The durations of the trials varied from 6 weeks to 3 years. There was a low risk of bias in three trials,28 29 34 with some concerns in nine trials31 32 35 36 40 43–45 47 and a high risk of bias in eight studies.30 37–39 41 42 46
Vitamin D reduced ARI risk by 69% after 3 years of follow-up among 208 postmenopausal African-American women42 whose participation was not dependent on their baseline serum 25(OH)D level, but had no effect among a separate group of 260 African-American women when serum 25(OH)D level was maintained at ≥30 µg/L.41 Three other studies found a significant effect of vitamin D supplementation.29 37 44 These were conducted among 107 US nursing home residents,44 124 Swedish adults with a high burden of ARI37 and 600 university students in Canada.29
Four studies in the Netherlands,33 Finland30 and the USA43 46 examined the influence of vitamin D supplementation to prevent common cold, and none found significant effects.30 33 43 46 One study among 223 patients with inflammatory bowel disease in Japan found no significant effect of vitamin D on preventing influenza.31 The overall risk of upper respiratory tract infection (URTI), however, decreased by 41% (95% CI 2% to 65%). One study among 322 adults in New Zealand found no effect of vitamin D supplementation on preventing URTIs caused by adenovirus, coronaviruses, influenza viruses, rhinovirus, respiratory syncytial virus and parainfluenza viruses, diagnosed based on RT-PCR.34
Other studies found no significant impact of vitamin D on the risk of ARI. These were conducted among community-dwelling adults by age or health status,28 45 older adults and their carergivers,38 patients with chronic obstructive pulmonary disease 39 or asthma,40 or patients with a previous colorectal adenoma.46
The pooled RR of the impact of supplementation on ARI occurrence from 20 studies28–47 was 0.97 (95% CI 0.94 to 1.00; p=0.028, figure 2). There was no significant heterogeneity (I2=4%), and no evidence of publication bias on inspection of the funnel plot (online supplemental figure 1). None of the individual studies had significant influence on the pooled estimate. Among four studies reporting on vitamin D and common cold prevention,30 33 43 46 the pooled RR of the effect was 0.93 (0.84 to 1.02; p=0.12; online supplemental figure 2). There was no heterogeneity in the estimates (I2=0%). The funnel plot was asymmetrical, (online supplemental figure 3), suggesting possible publication bias. Trim-and-fill analysis suggests eight studies may be missing on the right side, and the corrected pooled RR would be 0.98 (0.96 to 1.01).

Vitamin D to reduce the risk of acute respiratory tract infection (ARI) among adults. RE, Random effects.
The pooled RR of ARI was 0.82 (95% CI 0.68 to 1.00; p=0.046) among six studies28 29 31 35 37 44 whose outcomes were based on clinical diagnosis or laboratory testing (that is, excluding self-report (table 1)). The pooled RR of ARI was statistically significant when monthly or loading dose <60 000 IU, but not when ≥60 000 IU. Weekly doses were also statistically significant. Using multiple meta-regressions, we identified an optimal dosing regimen from alternatives with different magnitudes of daily, weekly, monthly or loading doses. The best regimen included daily vitamin D ≥2000 IU following a loading dose <60 000 IU.
Duration of symptoms
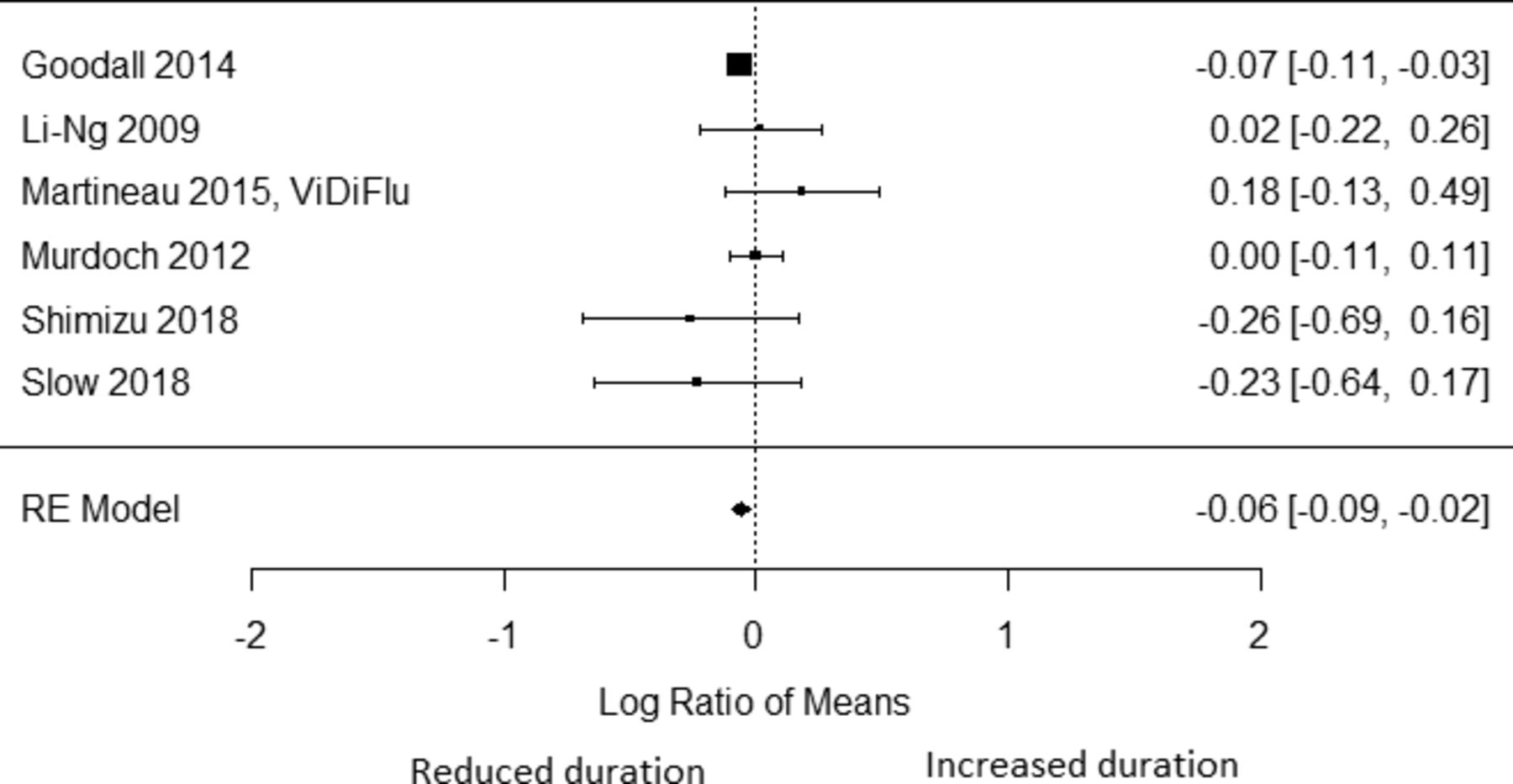
Six studies reported on the effect of vitamin D on the duration of symptoms due to ARI29 32 34 35 38 45 among 1400 adults. There was a low risk of bias for two studies,29 34 with some concerns for three studies32 35 45 and high for one study.38 Only one of these, a Canadian study, reported that vitamin D shortened the duration of symptoms—from 6.2 to 5.8 days.29 Vitamin D had no impact on the duration of symptoms among community-dwelling adults in the USA45 and New Zealand,29 older UK adults and their carers,38 and among patients admitted for pneumonia in New Zealand.35 The pooled per cent difference in duration was −6% (95% CI −9% to −2%; p=0.003, figure 3). There was no significant heterogeneity (I2=7%), and no evidence of publication bias on inspection of the funnel plot. The one study with a significant effect29 had substantial influence on the pooled estimate; if this study were left out of the analysis, the pooled percentage difference would be −0.5% (95% CI −9.4% to 8.5%, p=0.92). Heterogeneity was not influenced by the magnitude of the daily dose (p=0.51), weekly dose (p=0.22), monthly dose (p=0.28) or the loading dose (p=0.54).

Vitamin D to shorten the duration of symptoms of acute respiratory tract infection (ARI). RE, Random effects.
Vitamin C supplementation
Occurrence of illness
Twenty-four studies examined the effect of vitamin C on the risk of common cold among 10 961 adults (online supplemental table 4). The risk of bias was with some concerns for 19 studies48–66 or high for 5 studies.67–71 These studies were conducted in Australia,48 49 72 Canada,50 51 66 73 Japan,52 South Africa,53–55 Sweden,56 the UK57–60 67 74–76 and the USA.61–65 68–71 77 The studies provided daily doses alone48 49 51–54 57 59 63–67 69 70 75 or daily doses with loading doses. The daily doses were <250 mg,56 ,69 70 250 mg to <1000 mg,52–55 1000 mg48 49 51 57 59 62 64–67 75 or 2000 mg.63 The loading doses were 300 mg56 or 3000 mg.62 One study provided a range of daily (250 mg to 2000 mg) and loading doses (4000 mg to 8000 mg).50
Fourteen studies of vitamin C and common cold risk reported significant protective effects. Vitamin C was protective against common cold by 49% among 90 staff and students of a university in the UK, by 57% among 112 soldiers in Canada and by 45% among 28 men with marginal vitamin C status in the USA.65 Among 305 individuals in a village with high gastric cancer mortality in Japan, 500 mg/day of vitamin C led to 64% lower risk of common cold over 5 years.52
Vitamin C had no significant effect on the risk of common cold in 10 other studies conducted in Australia,48 49 Canada,51 66 the UK59 70 and the USA.62 63 69 78 Four of these studies had sample sizes >50051 59 63 70 and six had smaller sample sizes.48 49 62 66 69 75 Two of these studies were among military men or cadets in training.63 66 Four studies among marathoners in the USA (n=92) and South Africa (n=32), or among marathoners age-matched with non-runners (n=340 and n=167)53 found no effect of vitamin C on preventing ARIs.
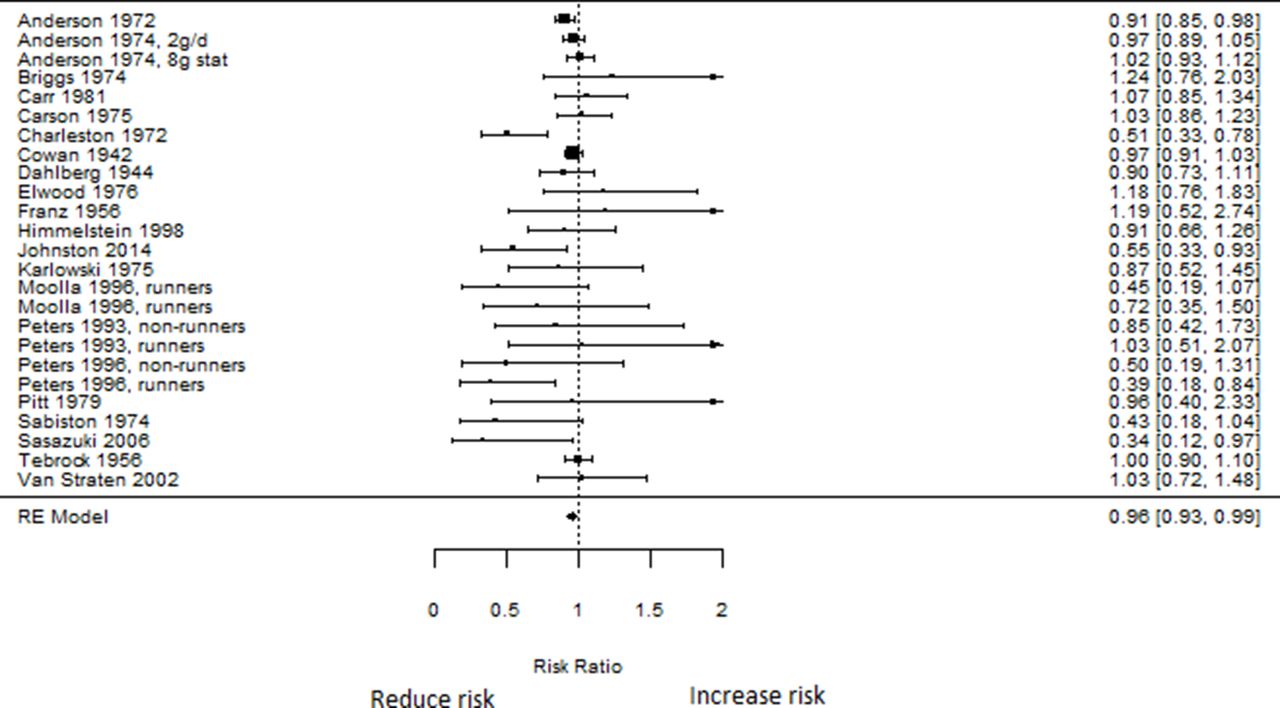
The pooled RR of vitamin C on preventing ARI (common cold and non-specific ARIs) was 0.96 (95% CI 0.93 to 0.99; p=0.01; figure 4). There was no evidence of heterogeneity (I2=0%), though asymmetry in the funnel plot suggests possible publication bias with fewer studies with estimates below the pooled RR than above it (online supplemental figure 5). Trim-and-fill analysis suggests five studies may be missing on the right side, though the pooled RR and CIs do not change.
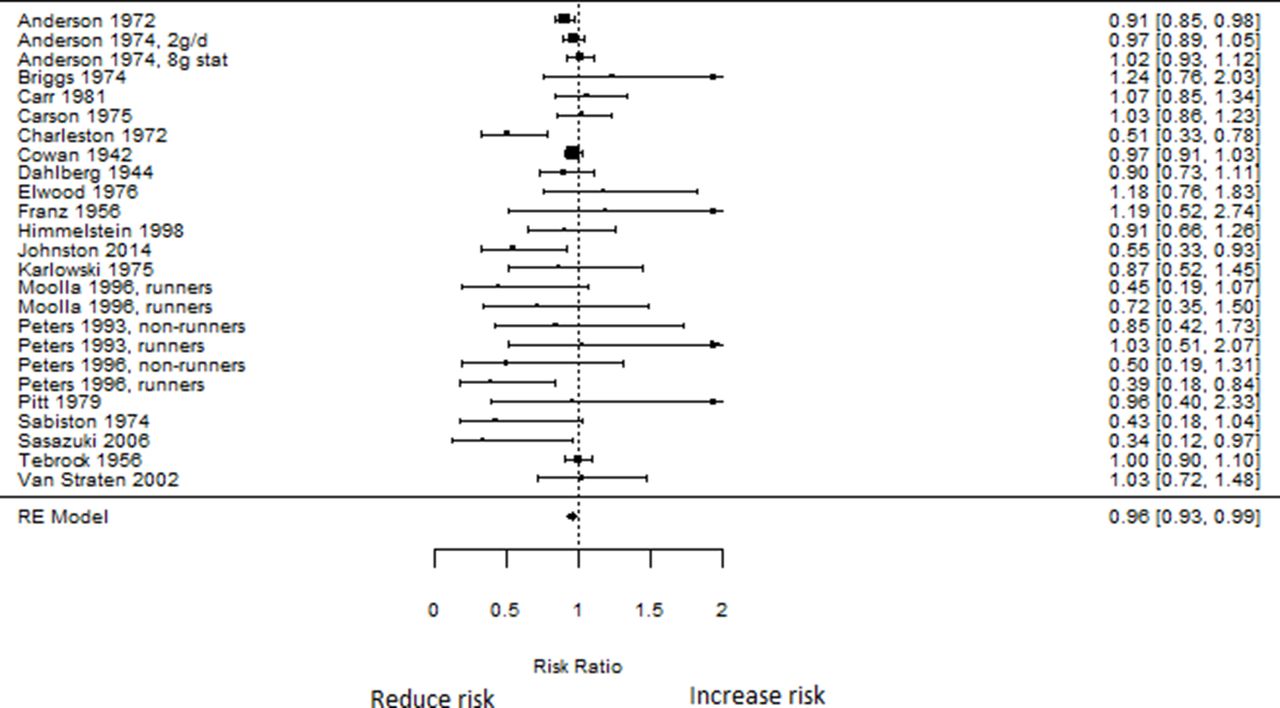
Vitamin C and the risk of acute respiratory tract infection (ARI) among adults. RE, Random effects.
Omitting one study51 with an RR of 0.91 (95% CI 95% CI 0.85 to 0.98) in influence analysis changed the pooled RR to 0.98 (95% CI 0.94 to 1.01). I2 did not change. The pooled RR significantly differed by sex (p=0.049). The pooled RR was 1.11 (95% CI 0.95 to 1.30) and 0.82 (95% CI 0.70 to 0.96) in women and men, respectively. The pooled RR significantly differed by country income classification (p=0.017). The pooled RR was 0.65 (95% CI 0.47 to 0.89) in middle-income countries and 0.96 (95% CI 0.93 to 0.99) in high-income countries. The pooled RR was neither influenced by the magnitude of the daily dose (p=0.63) nor the loading dose (p=0.18). The pooled RR was not significantly influenced by mean age, but none of the included studies were restricted to older adults (mean age of participants >60 years). The pooled RR was also not significantly influenced by mean age or duration of the trial.
The pooled RR of the effect of vitamin C on prevention of common cold was 0.96 (95% CI 0.93 to 0.99; p=0.022; online supplemental figure 6). There was no heterogeneity in the estimates (I2=0%). The funnel plot was asymmetrical, (online supplemental figure 7), suggesting possible publication bias. Trim-and-fill analysis suggests one study may be missing on the right side, and the corrected pooled RR does not change.
Duration of symptoms
Twenty-four studies evaluated the influence of vitamin C on the duration of common cold symptoms among 8344 adults. Study outcome was based on self-report, and the risk of bias of all studies was with ‘some concerns’. These studies were conducted in Australia,48 49 72 Brazil, Canada,50 51 66 73 Japan,52 South Africa,53–55 the UK58–60 67 75 76 and the USA.61 63–65 78 79 Included studies provided daily doses ranging from 0 mg to 3000 mg, with or without loading doses from 1500 mg to 8000 mg. Seven of these found that vitamin C shortened the duration of symptoms significantly.49 61 67 75 79 80 In one study, vitamin C shortened the duration of symptoms in men but not in women.60 In another study, vitamin C increased the duration of symptoms in women but had no effect in men.76 The other 11 studies48 50–52 58 59 63 65 66 72 73 78 found no significant effect of vitamin C on the duration of symptoms.
One study evaluated the proportion of participants who experienced symptom relief by the fourth and seventh days of supplementation among families in the UK randomised to 1000 mg/day of vitamin C compared with placebo.74 Vitamin C had no effect on whether symptoms were relieved by the fourth or seventh days.
In addition to the studies of common cold above, two studies evaluated the effect of vitamin C on the duration of URTIs among marathoners in South Africa and the USA, matched with non-runners. While vitamin C shortened the duration of URTI symptoms among marathoners and increased the duration in sedentary non-marathoners in the US study, vitamin C shortened the duration of URTI in non-marathoners in the South African study but had no effect on marathoners.53
Figure 5 presents the pooled percentage difference of the effect of vitamin C on the duration of ARI symptoms. Vitamin C shortened the duration of ARI symptoms by 9% (95% CI 2% to 16%; p=0.014). There was substantial heterogeneity in the estimates (I2=72%) and no evidence of publication bias on inspection of the funnel plots (online supplemental figure 8). None of the individual studies had significant influence on the magnitude or direction of the pooled estimates. The pooled percentage difference was neither influenced by the magnitude of daily dose (p=0.63) nor loading dose (p=0.92). None of the included studies was restricted to the older population, or had a participants’ mean age >65 years.
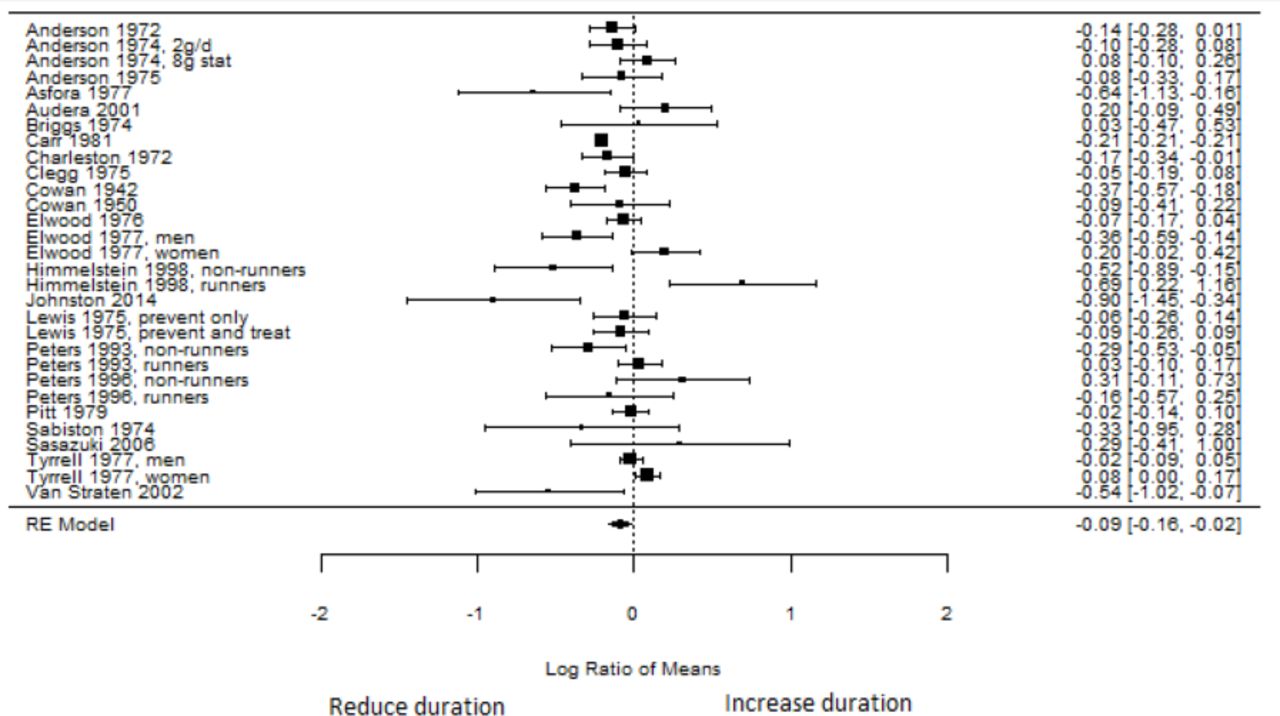
Vitamin C to reduce the duration of acute respiratory tract infection (ARI) symptoms. RE, Random effects.
The pooled percentage difference of the effect of vitamin C (online supplemental figure 9) on shortening the duration of common cold symptoms was −9% (95% CI −16% to −3%; p=0.007). There was substantial heterogeneity in the estimates (I2=65%) and no evidence of publication bias on inspection of the funnel plots (online supplemental figure 10). None of the individual studies had significant influence on the magnitude or direction of the pooled estimates.
Zinc supplementation
Occurrence of illness
Five studies examined the effect of zinc supplementation on prevention of common cold among 554 adults (online supplemental table 5).81–85 One study had a low risk of bias,84 while the risk of bias of the other four studies was high.81–83 85 Three experimental challenge studies in the UK and USA inoculated healthy volunteers with rhinovirus types 2, 23 or 39 and evaluated whether or not infection occurred based on detecting rhinovirus in viral cell culture.81–83 Two of these had additional antibody testing.82 83 Zinc had no effect on the risk of infection in all three studies, though their sample sizes were small (n=≤91).81–83 Zinc supplementation had no effect on the risk of common cold among 145 adults in Denmark or clinical URTI among 40 US air force cadets.84
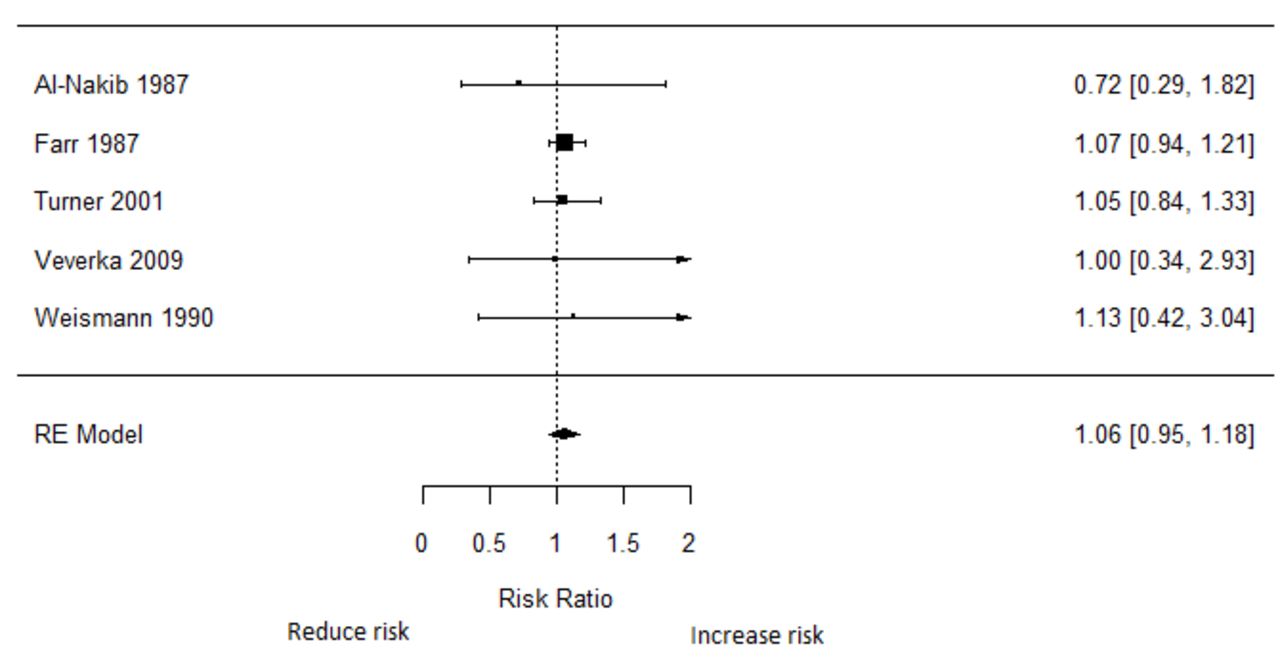
The pooled RR of zinc on the prevention of ARI (common cold and other ARIs) was 1.06 (95% CI 0.95 to 1.18; p=0.31; figure 6). There was no evidence of heterogeneity (I2=0%) and no evidence of publication bias (online supplemental figure 11). The pooled RR did not change on restricting to the four studies of zinc on common cold (RR: 1.06; 95% CI 0.95 to 1.18; p=0.31). The pooled RR was neither influenced by the magnitude of the daily dose, nor by sex, geographical location (continent) or study duration.
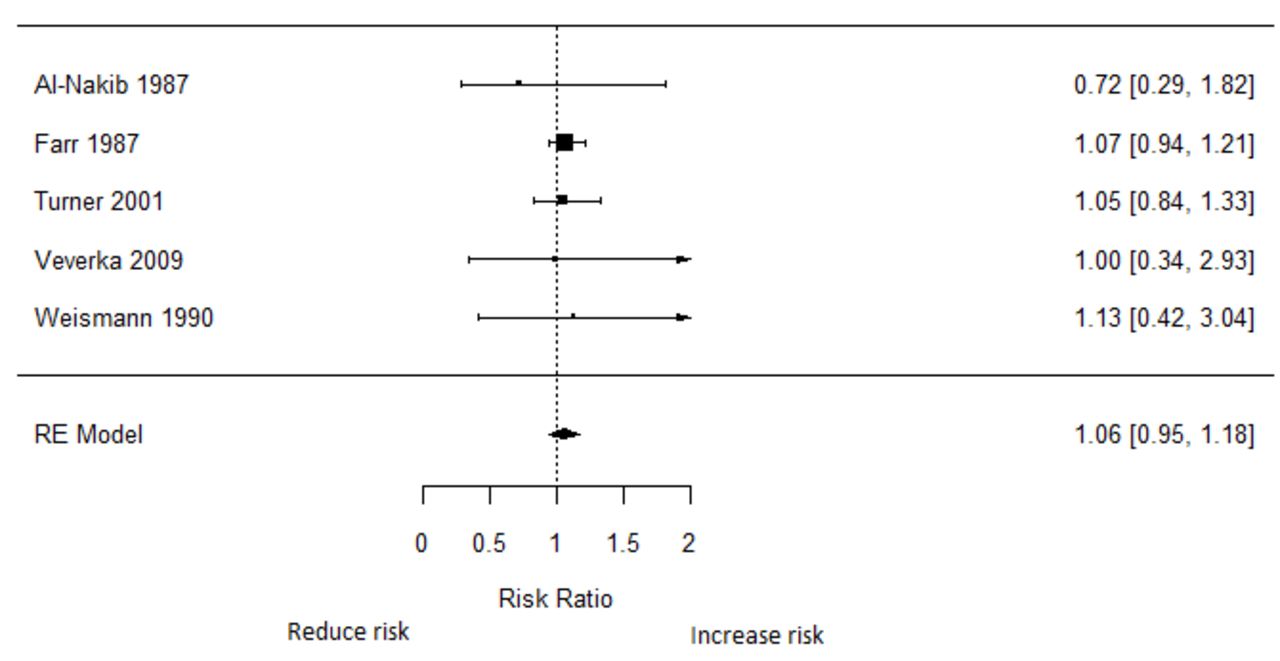
Zinc supplementation for reducing the risk of acute respiratory tract infection (ARI). RE, Random effects.
Duration of symptoms
Nine studies examined the effect of zinc supplementation on shortening the duration of common cold among 1038 adults, and all nine reported significant effects.86–94 There was a low risk of bias for one study,91 with some concern for four studies87 88 93 94 and high for four studies.86 89 90 92 These studies were conducted in Australia95 and the USA.86–94 In an experimental challenge study, zinc (13 mg every 2 hours) shortened the duration of symptoms from 3.5 days to 2.5 days, relative to placebo, among 91 volunteers.89
In terms of dose, most studies provided 23 mg of zinc82 86 90 96 or 13 mg88 92–94 every two to three wakeful hours. Among 99 adults in the USA, zinc supplementation significantly reduced the time to resolution of all symptoms (median reduction of 4.4 days compared with 7.6 days in the placebo group; p<0.001).88 The zinc group had significantly fewer days with most symptoms—coughing, headache, hoarseness, nasal congestion and sore throat—but did not differ in the number of fever days. Among 65 US adults, zinc supplementation was associated with a shorter duration of symptoms.86 Half of the participants were asymptomatic in 2.7 days in the zinc group and in 7.5 days in the placebo group. After 7 days, 86% in the zinc group were asymptomatic, compared with only 46% in the placebo group.
A few studies provided zinc in the form of nasal gels.87 91 For instance, among 213 US adults, the duration of symptoms was 2.3 (±0.9) days in the zinc group but 9.0 (±2.5) days in the placebo group.87 Among 80 US adults with recent onset of symptoms, nasal zinc supplementation reduced the duration of symptoms from 6 days to 4.3 days.
Two additional studies examined the effect of zinc supplementation on shortening the duration of symptoms of other ARIs. In the first, members of 34 families in Australia were randomly assigned to 10 mg of zinc acetate or placebo four or more times daily on developing respiratory symptoms.95 Zinc supplementation had no impact on the duration of symptoms of URTI. In the second study, zinc supplementation led to a 13% reduction in the proportion of individuals with symptoms of URTI among 174 volunteers in the USA.96 Most of the participants in this study were students.
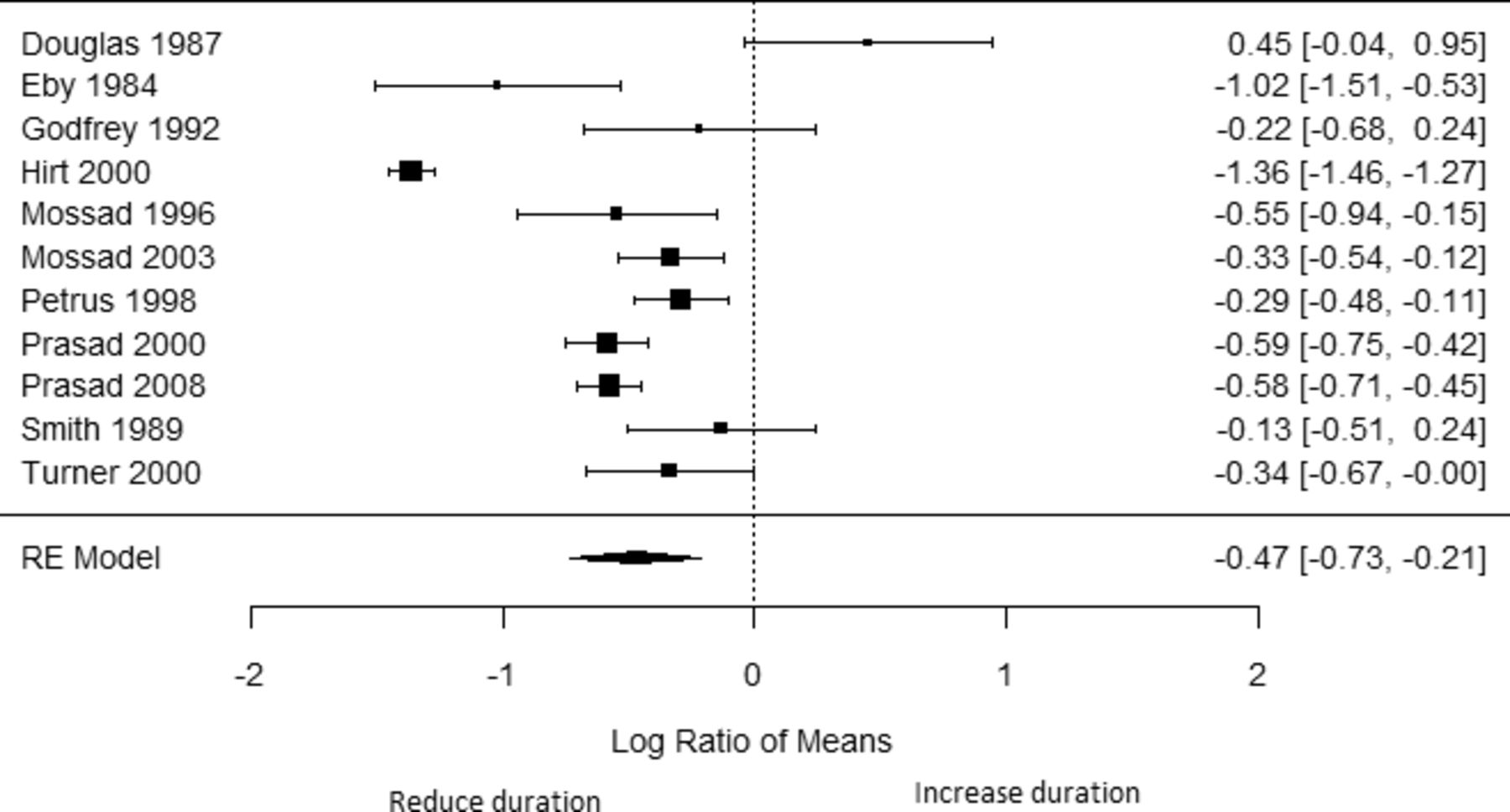
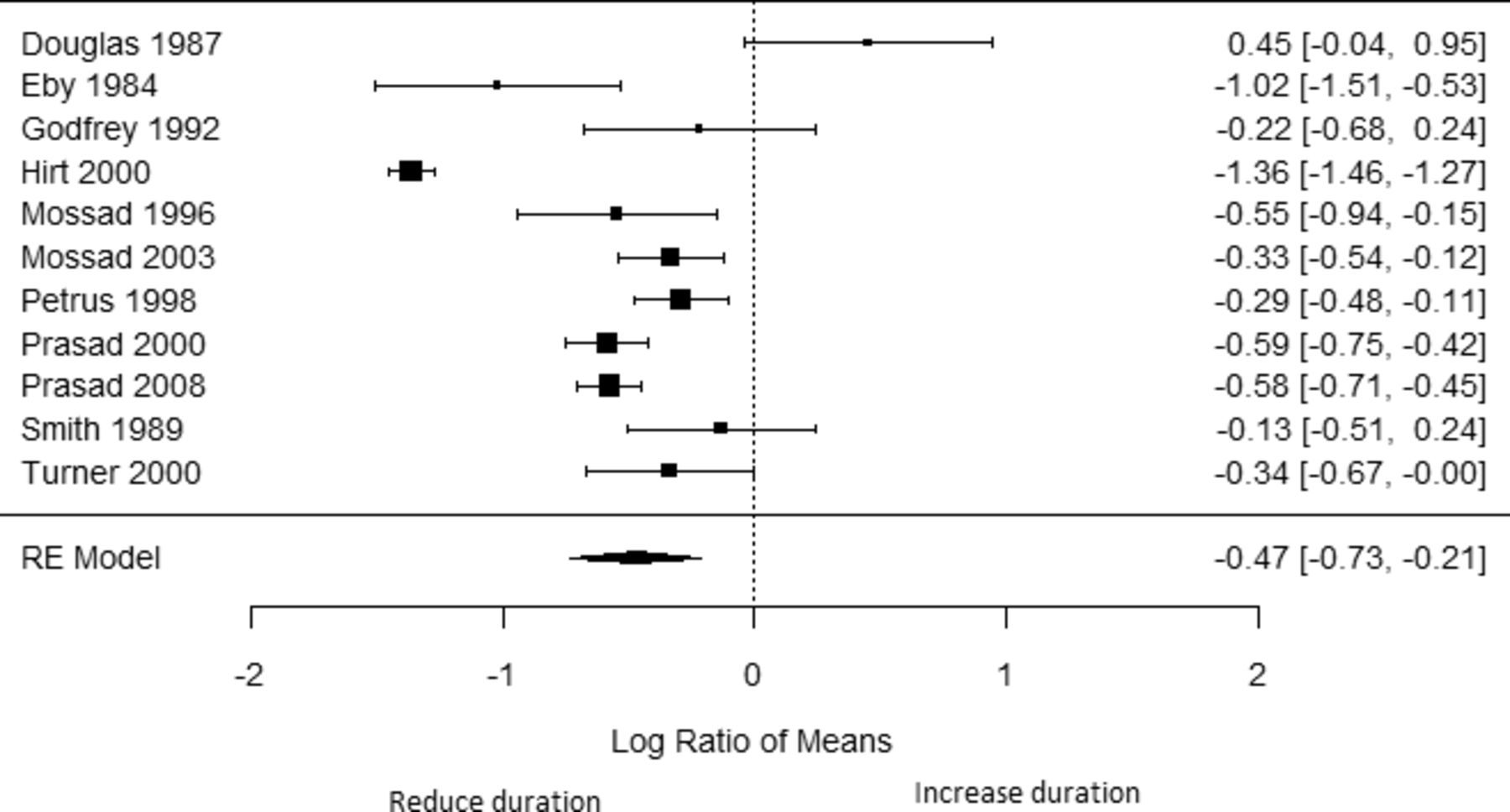
The pooled percentage difference for the effect of zinc supplementation on the duration of symptoms from 11 studies of common cold and other ARIs (figure 7) was −47% (95% CI −73% to −21%; p=0.0004). There was considerable heterogeneity in the estimates (I2=94%). The funnel plot was asymmetrical, (online supplemental figure 12), suggesting possible publication bias. Trim-and-fill analysis suggests three studies may be missing on the left side, and the corrected pooled percentage difference would be −63% (95% CI −90% to −36%).The pooled percentage difference was significantly different in the Australian study compared with the US studies (p=0.023). Dose of elemental zinc (>13.3 mg vs ≤13.3 mg; p=0.39) and the type of zinc compound (acetate vs gluconate) did not influence the pooled estimate (p=0.41). The pooled percentage difference was influenced neither by the magnitude of the daily dose and sex, nor by study duration.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Zinc supplementation to shorten the duration of acute respiratory tract infection (ARI) symptoms. RE, Random effects.
The pooled percentage difference for the effect of zinc supplementation on the duration of common cold symptoms from nine studies (online supplemental figure 13) was −59% (95% CI −84% to −35%; p<0.0001). There was considerable heterogeneity in the estimates (I2=93%), but no evidence of publication bias (online supplemental figure 14).
Multiple micronutrient supplementation
Occurrence of illness
Seven studies examined the effect of supplementation with combinations of micronutrients on ARI occurrence (online supplemental table 6) among 4510 adults.54 97–102 There was a low risk of bias for two studies,97 102 with some concerns for three studies54 98 100 and high for two studies.99 101 Three studies among older adults (>50 years) in India,98 the USA102 and the Netherlands101 provided MMS at the local recommended dietary allowances (RDAs) for each micronutrient and found no significant ARI-preventive effects. While the studies in India and the USA had small sample sizes, n=36 and n=61, respectively, the study in the Netherlands included 652 participants. There were small and statistically insignificant effects of MMS at 50% of local RDAs among 2799 older adults in Chile99 or a combination of vitamins B, C and E at the local RDAs among 725 nursing home residents in France.100
Studies among adults ≤50 years in South Africa and Mexico found MMS to reduce the risk of ARIs by 21% and 40%, respectively. These studies were short-term, with follow-up lasting 1–3 months. The first study was conducted among 178 ultramarathoners in South Africa, provided with a daily supplement containing 30 000 IU of vitamin A, 400 IU of vitamin E and 500 mg of vitamin C for 21 days prior to a marathon and 2 weeks postrace. The second was conducted among 59 individuals susceptible to ARI in Mexico, provided with supplementation for 90 days.97 The dose was at least twofold US RDAs for some nutrients (cobalamin, biotin and manganese), onefold to twofold RDAs for some nutrients (vitamins A, B, C and zinc) and below RDAs for others (vitamin D, calcium, selenium and copper).
Taken together, studies of MMS used diverse formulations making pooling and any inferences impossible.
Duration of symptoms
Among 36 individuals aged 51–78 years in India who received MMS at RDA level, MMS was associated with a twofold shorter overall duration of ARI symptoms.98 In addition, antibiotics were also used for fewer days in the MMS group. No other studies examined the impact of MMS on duration of symptoms.
Other micronutrients
Seven studies examined the effects of vitamin A and vitamin E, but could not be pooled (online supplemental table 7). There was a low risk of bias for one study,103 with some concerns for two studies54 55 and high for the others.101 104 105 Three of these examined the effect of vitamin A supplementation to prevent ARIs. One of these was in older adults. Among 29 133 smokers in a cancer prevention trial in Finland, vitamin A supplementation had no impact on the risk of hospital-treated pneumonia over 6 years of follow-up.103 The other two studies were conducted in younger populations of marathoners in South Africa (<50 years). Both 4.5 mg/day and 18 mg/day reduced the risk of URTI considerably (23% and 9%, respectively), though the CIs were wide. Vitamin A also reduced the risk of URTI by 16% in age-matched non-runners.55 Taken together, the effect of vitamin A on ARI risk appears to differ by age.
Four studies examined the effects of vitamin E on the risk of ARI.101 103 105 106 Among 617 elderly residents of 33 long-term care facilities in Massachusetts, USA, vitamin E supplementation was associated with a 17% lower risk of colds (RR=0.83; 95% CI 0.68 to 1.01), but had no influence on the risk of other ARIs or the duration of symptoms for either colds or other ARIs.104 Among 652 community-dwelling older adults in the Netherlands, vitamin E supplementation had no effect on the risk or duration of symptoms of ARIs during 2 years of follow-up.101
Two of the four studies were conducted in a cohort of male smokers in a cancer prevention trial in Finland. Vitamin E (50 mg/day) had no significant effect on the risk of hospital-treated pneumonia in the overall population of 29 133 individuals. However, vitamin E supplementation led to 69% and 72% lower rates of ARI among smokers who commenced smoking after 21 years of age,103 and among heavy smokers with ≥20 cigarettes/day.105 Vitamin E had no effect on the duration of symptoms in the overall population.
Discussion
We reviewed 80 RCTs that examined the effects of micronutrients on the occurrence and course of ARIs among adults. Vitamin D, vitamin C and MMS reduced the risk of ARIs by 3%–21%. Vitamin D, vitamin C and zinc shortened the duration of ARI symptoms by 6%–59%. Here we explore these results and identify gaps in published studies.
Our findings indicate that vitamin D supplementation reduces ARI risk by 3% overall, and by 18% when ARI was diagnosed based on laboratory testing or clinical diagnosis. This is comparable to findings in previous meta-analyses.7–11 The current study focuses on adults and includes recent trials.36 41 Vitamin D levels are insufficient in ≥50% of the global population, even though moderate sun exposure should be enough to prevent it.107 Vitamin D modulates immunity through effects on macrophage, dendritic and T cell function.108 Vitamin D promotes T-helper 2 (Th2) response and suppresses T-helper 1 (Th1) cells by enhancing interleukin (IL)-4, IL-5 and IL-10 production.109 110 In addition, many pathogens provoke oxidative stress and vitamin D enhances the production of antioxidative enzymes that counter it.108 Notably, the trials were conducted in temperate, high-income countries, limiting the generalisability of our findings to this setting. Further, the studies did not always report baseline levels of vitamin D and any adverse events of supplementation.
Vitamin C was observed to have a modest effect of preventing ARIs and shortening the duration of ARI symptoms. This is consistent with evidence from previously published meta-analyses.12 13 Vitamin C is an important cofactor for enzymes involved in tissue repair after an insult or injury.111 Vitamin C also has critical antioxidant properties, thereby limiting inflammation and improving recovery.112 This effect is stronger in people with vitamin C deficiency, as well as those undergoing stressful conditions.113 Though frank vitamin C deficiency or scurvy is rare, recent studies have shown the potential for adverse consequences in persons with subnormal vitamin C levels.114 Notably, the effect of vitamin C to prevent ARIs was considerably stronger in middle-income countries, compared with high-income ones. There was no significant dose-response relationship of vitamin C with the risk of ARI or duration of symptoms, and included studies did not evaluate the adverse events due to vitamin C.
Evidence from the current and previous meta-analyses demonstrate that zinc supplementation shortens the duration of ARIs considerably.15 17 In addition, zinc supplementation prevents mortality related to severe pneumonia.18 Zinc deficiency is widespread, affecting almost 20% of the global population, and regular intake of adequate quantities of zinc is required to prevent it.115 Zinc is a component of hundreds of enzymes and transcription factors, and plays critical roles in gene expression, cell division and immunity.116 It regulates the proliferation, differentiation, maturation, and functioning of epithelial cells and leucocytes.117 It also modulates the production of T lymphocytes, cytokines and reactive oxygen species.117 118 In addition, zinc improves appetite and its deficiency leads to anorexia, impairing intake of macronutrients and micronutrients essential to mount a robust immune response.117
Multiple micronutrient deficiencies have been previously associated with elevated risk of respiratory infections, especially among the elderly.119 The studies included in this review used diverse formulations, and any inferences regarding the preventive effect of MMS was not possible. MMS, however, shortened the duration of symptoms considerably in the one study among older adults in India that examined it.98 It is plausible that the absence of an observed effect on prevention could be related to the dose of the micronutrients, or the extent of dietary inadequacies and nutritional deficiencies in the study population. Micronutrients are often provided at or below RDA level, which could be inadequate to address existing deficiencies. Evidence from studies of the effect of supplement administration on other viral infections such as HIV also support the potential that MMS could significantly slow disease progression and reduce mortality among HIV-infected individuals.120 121
It is possible that supplementation with vitamin C, zinc and vitamin D, possibly as part of MMS, may prevent SARS-CoV-2 infection and shorten the duration of COVID-19 symptoms. No primary studies have examined the impact of these micronutrients on the risk of SARS-CoV-2 infection. One study that examined the influence of vitamin C on any coronaviruses had only a few cases, and found no significant effect.34 In addition to their general effects as modulators of immunity discussed above, both vitamin D and zinc have antiviral effects, including through induction of cathelicidin to disrupt viral envelopes or by combining with pyrithione to inhibit RNA polymerase activity.122 123 Vitamin D also acts on cellular and genetic pathways that regulate clotting, and may ameliorate COVID-induced coagulation, especially among those with vitamin D deficiency.124 There is preliminary evidence that lower vitamin D levels are present in patients with COVID-19 in comparison to hospital controls, and that the extent of COVID-19 mortality is proportional to the national severity of vitamin D deficiency.125 This evidence is however ecological, and any significant relationships could be due to intractable confounding or systematic differences in assessment of exposure or outcome. Further, the impact of individual or combination micronutrient supplements to shorten the duration of viral respiratory illnesses may be particularly critical to free up healthcare resources, especially bed space in intensive care units and in the general hospital wards. Individuals with the most severe nutritional deficiencies are observed to receive greater benefits from supplementation,10 113 strengthening the ethical imperative to evaluate utility of different supplements in treating and preventing COVID-19. RCTs of these micronutrients among patients with COVID-19 are therefore warranted, particularly during the current stage of the pandemic which provides a unique window to enrol large study populations. These studies should carefully consider differential effects among individuals who may be replete or deficient for the relevant micronutrient, as well as the potential role for supraphysiological amounts.
Determining whether to recommend supplementation and the relevant dose is critical for clinical and public health planning, especially in the context of the ongoing response to COVID-19. We examined the effect of different dose categories on the preventive and treatment effects of the micronutrients evaluated in this meta-analysis. Notably, we found that while vitamin D was 3% protective in the general population, it was 10% protective if the daily dose was ≥2000 IU. We found that providing a monthly or loading dose was beneficial if it was <60 000 IU, but not if it was ≥60 000 IU—possibly because large doses could disrupt enzyme metabolism of vitamin D.126 We also find that weekly dosing (10 000 IU or 20 000 IU) was 30% protective. Using multiple-predictor meta-regression, we identify the best dosing regimen provided a loading dose is >0 IU to <60 000 IU, and a daily dose is ≥2000 IU for prevention of infection. We found no differential effect of dose of vitamin D when used as treatment, and it is plausible that a high loading dose may be warranted particularly among deficient individuals so as to rapidly correct vitamin D status during the narrow window of illness, followed by lower daily maintenance doses. The effects of vitamin C and zinc supplementation were not modified by the dose of supplement provided.
Our review was limited by the availability and nature of primary studies. Most of the studies were conducted in high-income countries, limiting generalisability of our findings to those settings. Many studies classified the outcomes of interest based on self-report, resulting in error which could have reduced our power to identify significant associations. Many of the included studies had high risk of bias or some concerns—partly due to a dependence on self-report for outcome assessment. In addition, there were no studies conducted among pregnant women. Furthermore, it was impractical to examine the impact of micronutrients on the severity of symptoms due to the substantially different ways that severity was assessed in the studies, and this may have contributed to heterogeneity in pooled analyses. Studies used different assays to estimate baseline micronutrient status, due to changes in laboratory standards and techniques over time. There were no significant dose-response relationships for many of the exposure-outcome relationships assessed. Adverse event information was limited, and we are therefore unable to assess the safety of supraphysiological doses. Finally, minimum clinically important differences have not been established for these outcomes, and we are unable to conclude whether these findings are clinically meaningful. Given the mix of the quality or randomised trials reviewed and the sources of bias in the primary studies, we conclude that the evidence presented likely reflects the true effect of the micronutrients on the risk of ARIs, and strength of evidence is moderate. Further research may change some of our conclusions.
Conclusion
Our synthesis of global evidence from RCTs indicates that micronutrient supplements including zinc, vitamins C and D, and multiple micronutrient supplements may be modestly effective in preventing ARIs and improving their clinical course. Further research is warranted to better understand the effectiveness that individual or multiple micronutrients have on SARS-CoV-2 infection and treatment outcomes.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @drabioye
Contributors The paper was drafted by AIA, SB and WF. WF designed the study. AIA reviewed titles, abstracts and full texts, and extracted data as necessary. All authors contributed to the development of and approved the final version of the manuscript. The authors have full access to all of the data in the study and take responsibility for the integrity of the review.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information and are available via medical literature databases.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.