Article Text

Abstract
Background While much progress was made throughout the Millennium Development Goals era in reducing maternal and neonatal mortality, both remain unacceptably high, especially in areas affected by humanitarian crises. While valuable guidance on interventions to improve maternal and neonatal health in both non-crisis and crisis settings exists, guidance on how best to deliver these interventions in crisis settings, and especially in conflict settings, is still limited. This systematic review aimed to synthesise the available literature on the delivery on maternal and neonatal health interventions in conflict settings.
Methods We searched MEDLINE, Embase, CINAHL and PsycINFO databases using terms related to conflict, women and children, and maternal and neonatal health. We searched websites of 10 humanitarian organisations for relevant grey literature. Publications reporting on conflict-affected populations in low-income and middle-income countries and describing a maternal or neonatal health intervention delivered during or within 5 years after the end of a conflict were included. Information on population, intervention, and delivery characteristics were extracted and narratively synthesised. Quantitative data on intervention coverage and effectiveness were tabulated but no meta-analysis was undertaken.
Results 115 publications met our eligibility criteria. Intervention delivery was most frequently reported in the sub-Saharan Africa region, and most publications focused on displaced populations based in camps. Reported maternal interventions targeted antenatal, obstetric and postnatal care; neonatal interventions focused mostly on essential newborn care. Most interventions were delivered in hospitals and clinics, by doctors and nurses, and were mostly delivered through non-governmental organisations or the existing healthcare system. Delivery barriers included insecurity, lack of resources and lack of skilled health staff. Multi-stakeholder collaboration, the introduction of new technology or systems innovations, and staff training were delivery facilitators. Reporting of intervention coverage or effectiveness data was limited.
Discussion The relevant existing literature focuses mostly on maternal health especially around the antenatal period. There is still limited literature on postnatal care in conflict settings and even less on newborn care. In crisis settings, as much as in non-crisis settings, there is a need to focus on the first day of birth for both maternal and neonatal health. There is also a need to do more research on how best to involve community members in the delivery of maternal and neonatal health interventions.
PROSPERO registration number CRD42019125221.
- maternal health
- child health
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
The insecurity, population displacement and health service disruption that are associated with armed conflict may increase both maternal and neonatal mortality.
While there is guidance available on the essential interventions for mothers and newborns in humanitarian crises, there is still a lack of guidance on how best to deliver these interventions, especially in conflict settings where there are even more barriers to the access of services.
What are the new findings?
Maternal health interventions were mostly delivered by skilled health workers including doctors and nurses and in hospitals and clinics; the majority of reported interventions focused on antenatal care and its different components.
Although few, the reported newborn interventions focused on essential newborn care such as neonatal resuscitation and kangaroo mother care, and were also mostly delivered by skilled health workers in clinics and hospitals.
Among the reported barriers to intervention delivery were the lack of safety, population displacement, and the lack of resources and skilled health workers; however, facilitators included the availability of funding, multisectoral collaboration and the availability of training for staff.
There is still a wide gap in reporting on newborn health, with very few eligible publications reporting on interventions targeting newborns.
Key questions
What do the new findings imply?
There is a need to do more evaluations on the use of lower-cadre health workers and community-based sites in the delivery of maternal health interventions.
It is also important to assess the feasibility and importance of deploying people from the affected communities, especially in out-of-camp settings where there may not be as many services/resources available.
There is an urgent need to prioritise newborn health interventions. More research is needed on how best to deliver newborn interventions using lower-skilled health workers and at the community level.
Introduction
Maternal and newborn mortality remain two of the biggest challenges in global health. Although much progress was made throughout the Millennium Development Goals era, about 810 women still die from pregnancy-related or childbirth-related complications every day. This is especially true in low/middle-income countries (LMICs) where 94% of these deaths occur.1 Approximately 7000 newborns also die every day,2 accounting for 47% of all under-5 child deaths, and with 36% of them occurring during the first 24 hours after birth and 73% within the first week.3 Although it has been shown that increasing coverage of antenatal care (ANC), skilled birth attendance and postnatal care for both the mother and the baby can prevent high maternal and neonatal mortality rates,4 data from existing surveys still show that many women and newborns are not reached with these essential interventions.1
Within humanitarian settings and especially in the context of armed conflict, insecurity coupled with displacement and service disruption produce an instability that may lead to a higher risk of maternal mortality.5 While increased maternal mortality may be a direct effect of armed conflict, it has also been shown that maternal mortality may remain elevated even 1–3 years post-conflict, indicating the longer terms effects of conflict on the disruption of essential health services for pregnant women.5 Newborn mortality has also been shown to increase in the context of armed conflict,6 and is highest in fragile settings and in countries that have recently experienced a humanitarian crisis.7
Comprehensive global guidance exists for addressing maternal and neonatal health (MNH) in non-crisis settings, including the interventions and services outlined in the Every Newborn Action Plan launched in 2014.8 Guidance is also available to support MNH in humanitarian crises, including the latest version of the Inter-Agency Field Manual on Reproductive Health in Humanitarian Settings and the Newborn Health in Humanitarian Settings–Field Guide, both released in 2018.9 10 However, guidance on how best to deliver recommended interventions for pregnant women and newborns in humanitarian settings, and especially in conflict settings, is still very limited. A review on public health interventions that was included in the 2017 Lancet Series on Health in Humanitarian Crises highlighted the need for higher quality studies on MNH that focus on the most effective means of delivering those interventions in crisis contexts.11 12
The present review aimed to systematically synthesise the available indexed and grey literature reporting on the delivery of maternal and newborn interventions in conflict settings. We sought to characterise how and by whom such interventions have been and are being delivered to conflict-affected women and newborns and, if possible, to what extent and with what effectiveness.
Methods
Literature search
A systematic search of published literature from 1st January 1990 to 31st March 2018 was conducted; records were retrieved in MEDLINE, Embase, CINAHL and PsycINFO using OVID and EBSCO interfaces. We used sets of terms related to three concepts: (a) conflict; (b) women and children; and (c) MNH. Conflict-related terms included war, crisis, refugees and internally displaced persons (IDPs). Population-related terms included: women, children, pregnant, adolescents and newborn. MNH-related terms included: pregnancy, obstetrics, labour complications and neonatal care, among others. The full MEDLINE search syntax is provided in the online supplemental appendix A. Relevant publications from key systematic reviews11 13–15 were also hand searched for potentially relevant publications.
Supplemental material
We searched the websites of 10 major humanitarian agencies and organisations that are actively involved in responding to or researchin conflict situations for grey literature on the implementation of health interventions in pregnant and postpartum women or newborns. These websites included: Emergency Nutrition Network, International Committee of the Red Cross, International Rescue Committee, Médecins Sans Frontières, Save the Children, United Nations (UN) Population Fund, UN High Commissioner for Refugees, UNICEF, Women’s Refugee Commission and World Vision. We used broad terms for conflict and health interventions tailored to the search functionality of each website. Documents published from 1 January 2013 to 30 November 2018 were reviewed.
Eligibility criteria
Our eligibility criteria included publications reporting on populations affected by conflict in LMICs, as classified by the World Bank.16 Eligible publications must have described an MNH intervention targeting or including pregnant or postpartum women or neonates, and delivered during or within 5 years of cessation of a conflict. Where needed, we consulted online encyclopaedic sources as well as the UN Office for the Coordination of Humanitarian Affairs website for information on the duration of a specific conflict, to assess whether the time period of intervention delivery reported in a candidate publication was eligible. In order to identify the most informative resources from the large volume of grey literature available, the same inclusion criteria set for indexed literature was applied, with the additional requirement of explicit reporting on the delivery site and personnel for each intervention.
Non-English publications; case reports of a single patient; or publications reporting on military personnel, refugee populations in high-income countries, surgical techniques, or economic or mathematical modelling studies were excluded from our review. We also excluded systematic and other literature reviews, editorials, commentaries, first-person narratives, newspaper and magazine articles, opinion pieces, guidelines and studies where no specific health intervention was described (eg, prevalence studies).
Data extraction and analysis
All identified indexed records were downloaded into EndNote software17 and duplicates were removed. Unique records were subsequently added into Covidence software for screening.18 Two reviewers independently screened titles and abstracts for relevance, and any discrepancies were resolved through discussion or by a third reviewer, if necessary. A single reviewer then screened the full texts of potentially relevant publications to determine their eligibility for inclusion in this review. The same approach was applied to the grey literature, with two reviewers screening titles of retrieved publications for relevance and one reviewer assessing the full text to determine eligibility.
We used a customised form on the REDCap platform19 to extract relevant quantitative and qualitative information from all included publications. Data and information on key variables including setting, population characteristics, study design, intervention details and delivery characteristics including reported delivery barriers and facilitators, as well as quantitative data on coverage and effectiveness (when available), were extracted. Two reviewers entered the data in duplicate independently and any inconsistencies identified were resolved through a discussion or by a third reviewer.
Descriptive statistics were performed to summarise key characteristics of the intervention, including displacement status of the target population, delivery characteristics, and reported factors impeding or facilitating delivery. We plotted intervention delivery frequencies stratified by population displacement status, and we mapped reported interventions against reported delivery personnel and site, stratified by intervention type. We tabulated coverage and effectiveness estimates that were reported for pregnant or postpartum women or newborns, but meta-analysis was not conducted due to extensive variability in interventions, outcomes, study settings and populations. All descriptive analyses were conducted using Stata V.14.0 statistical software.20 Finally, we narratively synthesised reported information on delivery barriers and facilitators by classifying related information into subgroups and then into broader themes.
Patient and public involvement
Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this systematic review of the literature.
Results
Characteristics of the included literature
From 37 714 indexed publications retrieved through our database search, 101 met our eligibility criteria. An additional 14 eligible publications were identified from our grey literature search, and from the reference lists of other reviews. A total of 115 publications were therefore included in this review (figure 1).21–135 Of these, only 26 reported on neonatal interventions.24 26 28 29 33 38 42 44 55 60 63 71 75 97 106 110–113 116 118 120 123 124 133 135 The characteristics of all included publications are presented in the online supplemental appendix B.

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram: publication selection process for systematic review on the delivery of maternal and neonatal health interventions in conflict settings.
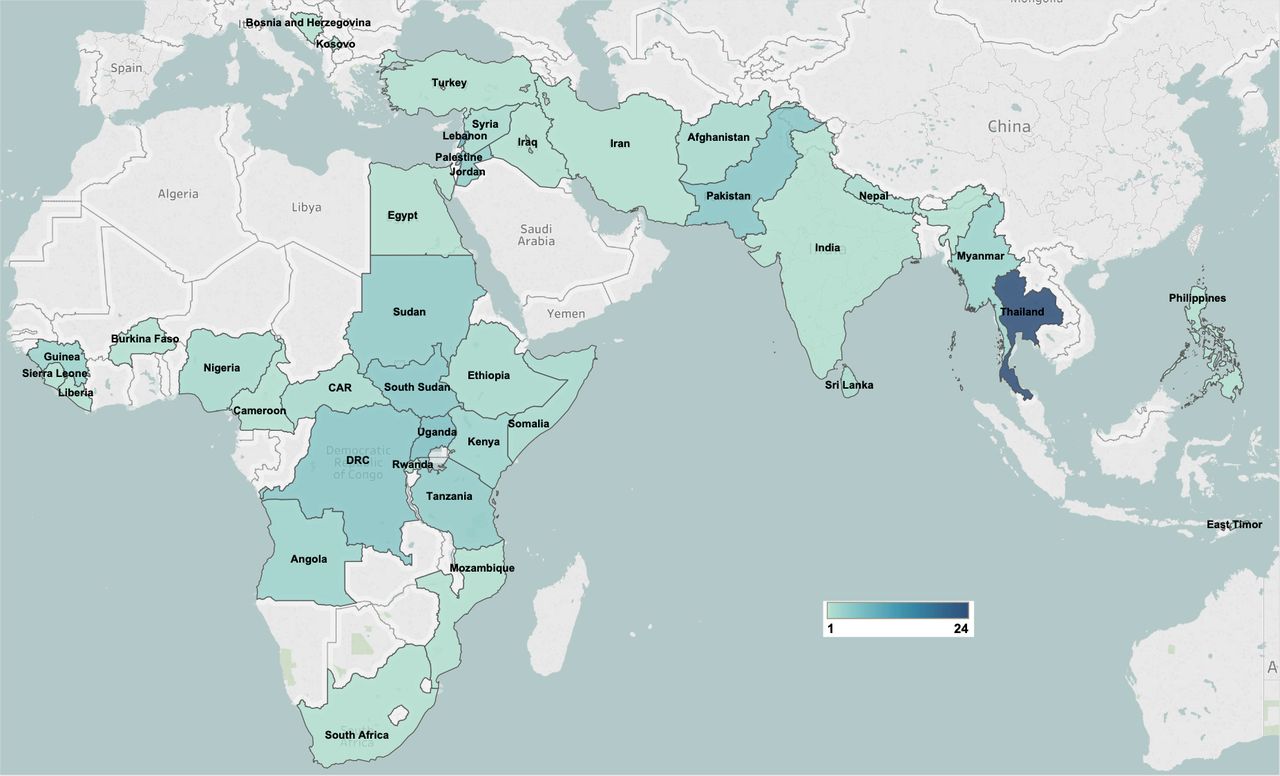
Of the 115 included publications, MNH intervention delivery was most frequently reported in the sub-Saharan Africa region (43%), followed by the East Asia and Pacific region (27%), mainly in Thailand (figure 2). There were no studies reporting on interventions delivered within the Latin America and Caribbean region. The majority of included publications reported on observational studies (68%), and 17% were non-research reports (table 1).
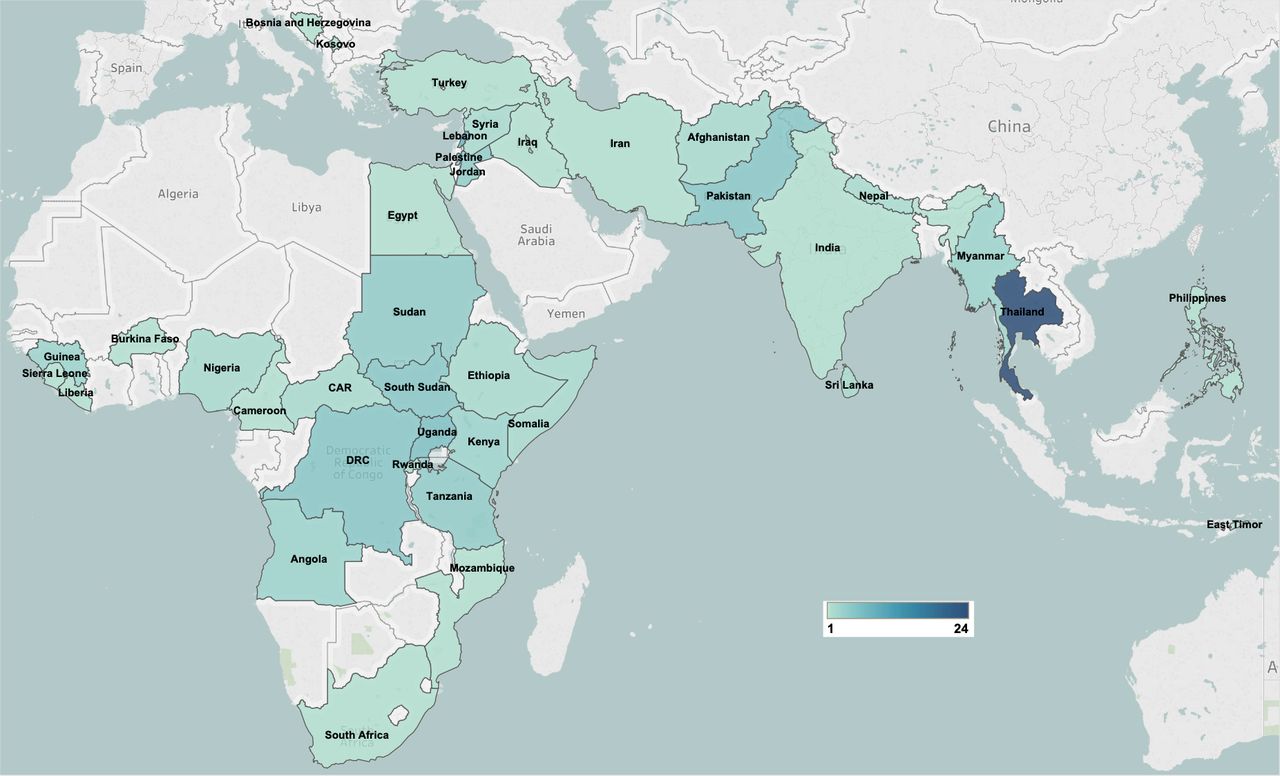
Geographical distribution of included publications.
Characteristics of included publications and included interventions
More than half of the included publications reported on interventions delivered to refugees (62%), and about one-third of those delivered to IDPs (27%). There were also a few publications reporting on interventions delivered to non-displaced but conflict-affected populations and to host communities in countries with refugees. Among those publications reporting population displacement settings, intervention delivery to refugees and IDPs was reported most frequently in camp settings (45%). Pregnant women were the most frequently reported intervention target populations, and most reported interventions were delivered by non-governmental organisations (NGOs) (including community-based organisations) or UN agencies, either through the existing healthcare system or in parallel.
Maternal health interventions
The reported interventions targeting pregnant or postpartum women covered different components of maternal health such as antenatal, obstetric and postnatal care, as well as general maternal health (figure 3). Within ANC, the most commonly reported interventions were screening interventions for HIV, sexually transmitted infections (STIs), malaria and anaemia; micronutrient supplementation; malaria prevention and treatment; and behavioural education activities. Of the publications that reported on the delivery of ANC, about 35% of them did not specify the components provided. Reported obstetric care interventions were mostly safe delivery care interventions and the provision of basic and comprehensive emergency obstetric care (EmOC), including caesarean sections. Other obstetric care interventions included training of healthcare workers and referral for care. Reported postnatal care interventions included postnatal check-ups within 48 hours of delivery, education activities and micronutrient supplementation among others. Reported general maternal health interventions mainly included training healthcare workers and counselling interventions.

Maternal health interventions in pregnant and postpartum women. ANC, antenatal care; MH, maternal health; STI, sexually transmitted infection.
When comparing mothers living in camps with those living outside of camps, more interventions were reported to be delivered to mothers based in camps (figure 3). Some interventions were not reported at all for women living outside of camps, such as training of health workers or interventions targeting the prevention of HIV and STIs during ANC. There were also very few postnatal care interventions and no general maternal health interventions reported to be delivered to out-of-camp mothers.
Delivery characteristics of maternal health interventions
Personnel
Trained health professionals were commonly reported personnel for maternal health interventions. These included doctors, nurses, health workers, skilled birth attendants (SBAs) and OB/GYN specialists (figure 4). NGO staff and researchers were also reported to have delivered most maternal health interventions such as ANC, behavioural education, postnatal care and training. Community health workers (CHWs) were reported to deliver ANC interventions such as malaria treatment and prevention, micronutrient supplementation, behavioural education and counselling among others. Traditional birth attendants (TBAs) were not only involved in delivery care, but were also able to deliver some ANC interventions such as malaria prevention, medication and postnatal check-ups. There were no interventions delivered by community members such as civic leaders or trained civilians and there was only one training intervention where teachers were involved, which was a literacy programme for women.
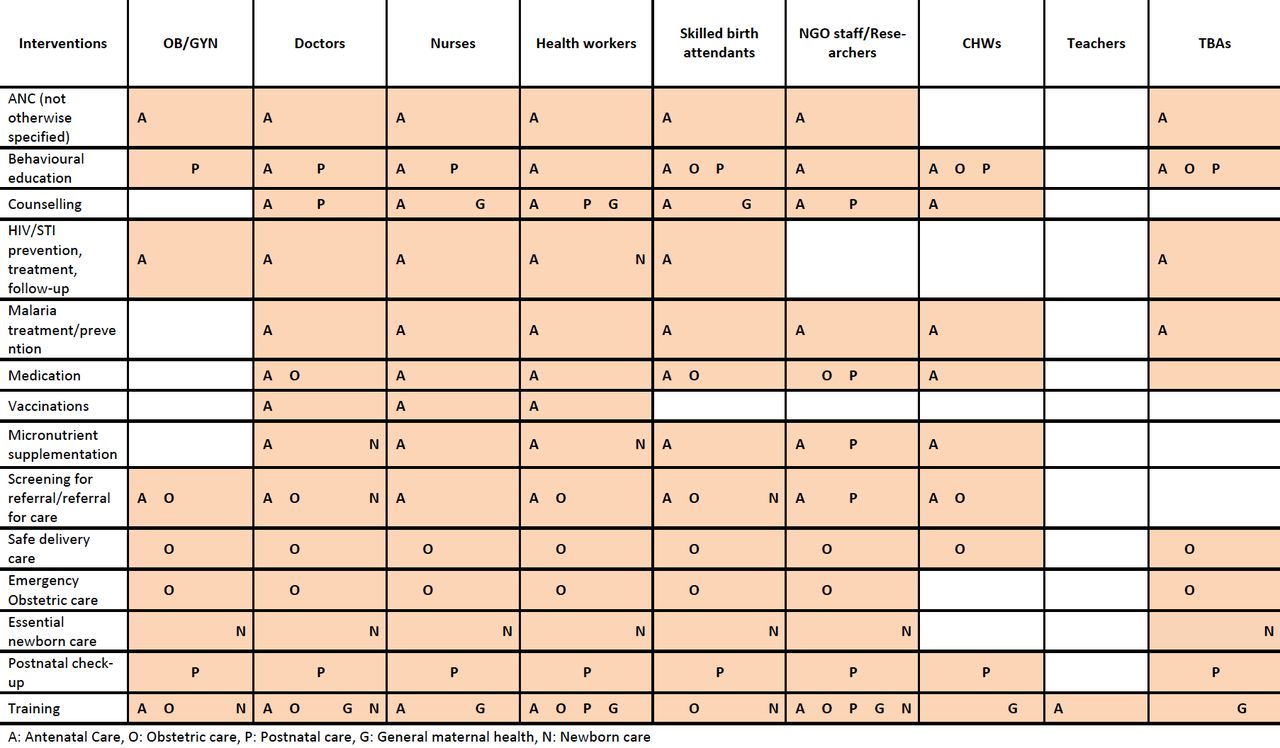
Reported maternal and neonatal health interventions by delivery personnel and intervention type. ANC, antenatal care; CHWs, community health workers; NGO, non-governmental organisation; STI, sexually transmitted infection; TBAs, traditional birth attendants.
When we compare in-camp and out-of-camp populations, in-camp mothers were reported to have access to a wider range of personnel compared with out-of-camp populations (data not shown). In-camp interventions were delivered by health workers, nurses, doctors and OB/GYN specialists, while for out-of-camp populations, health workers were the most reported delivery personnel, but with fewer specified professionals reported such as OB/GYN specialists, doctors and nurses. There was also only one reported instance of a TBA being used in an out-of-camp population and very few interventions were reported to be delivered by SBAs or NGO staff. There were few differences in delivery personnel between refugees and IDPs (data not shown), except that while CHWs are mainly used for behavioural education and referral in refugee populations, they were also used for the ANC interventions such as micronutrient supplementation or malaria prevention in IDP populations.
Sites
Maternal health interventions were mostly delivered using the inpatient and outpatient platforms, with most interventions reported to be delivered within either hospitals or clinics (figure 5). Other common delivery sites included health posts and mobile clinics, mostly for the delivery of ANC interventions. Community-based sites such as homes and communal spaces were also used for ANC and postnatal care interventions. There were few differences between in-camp and out-of-camp populations in terms of delivery sites (data not shown). There were no MNH interventions reported to be delivered in a hospital within out-of-camp populations, and there was also more use of communal spaces for delivery reported within these populations. Interventions targeted towards refugees were delivered more often in clinics and hospitals, with no reports of delivery using outreach sites such as health posts and mobile clinics and very few reporting delivery at the household (data not shown). Interventions targeted towards IDPs used outreach approaches more frequently, with interventions delivered at health posts and through mobile clinics.
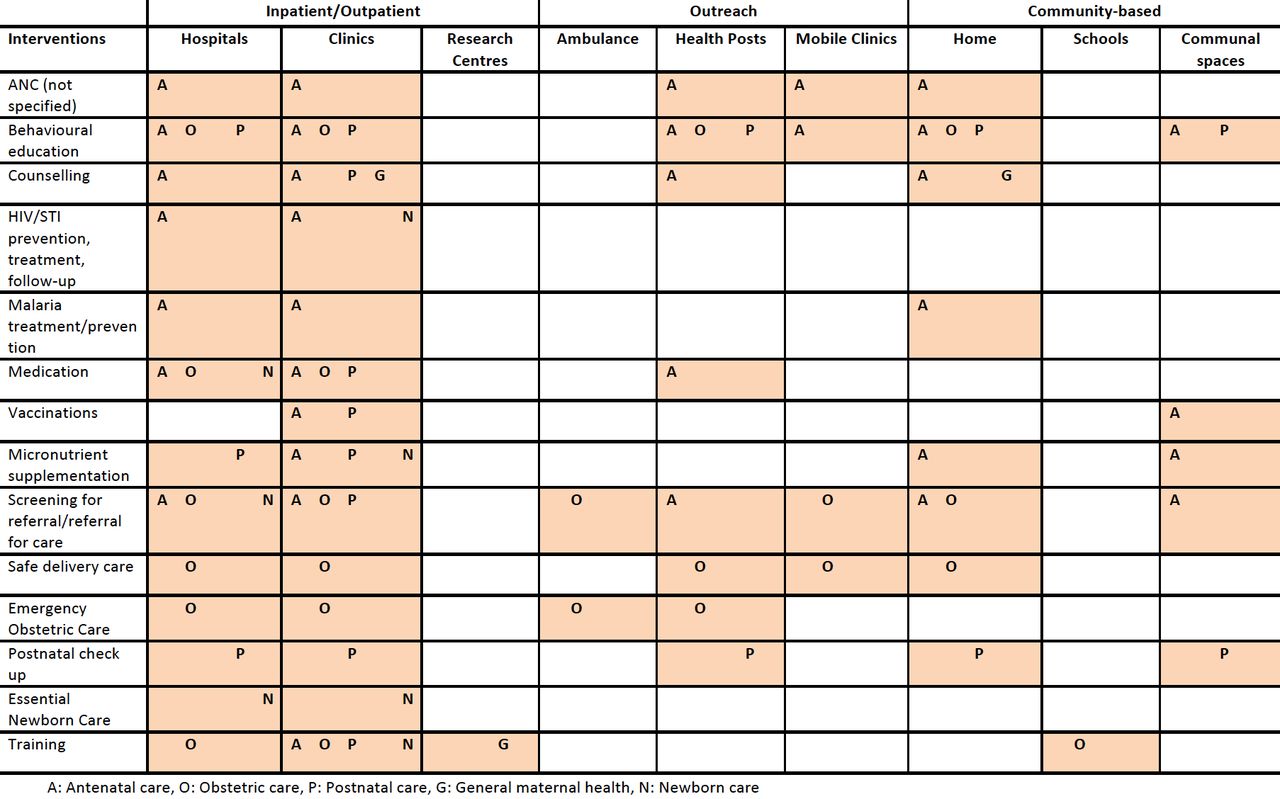
Reported maternal and neonatal health interventions by delivery site and intervention type. ANC, antenatal care; STI, sexually transmitted infection.
Newborn health interventions
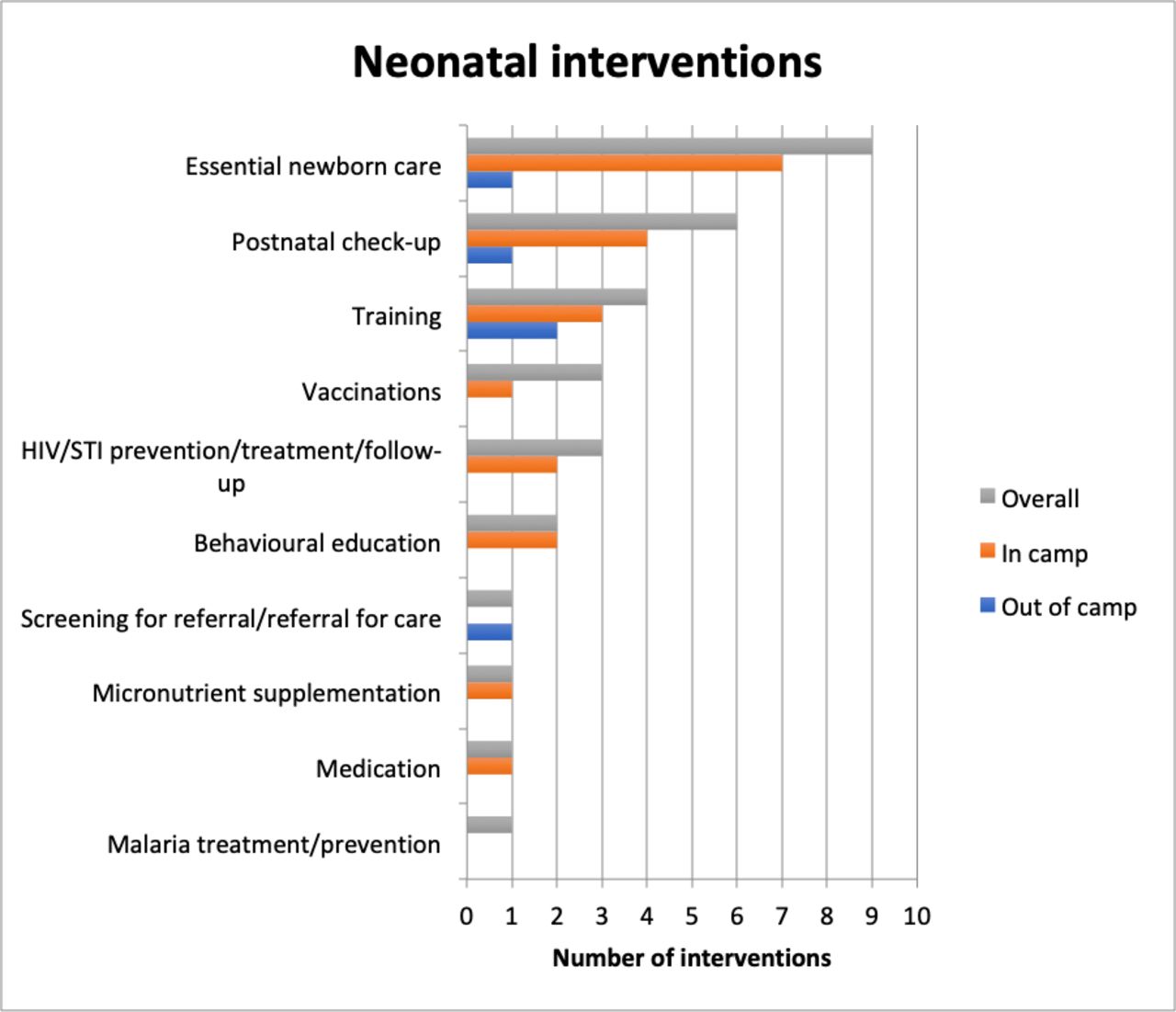
Very few studies reported on newborn care, and only about 10% of all interventions reported were targeting newborns. These interventions were focused mostly on essential newborn care such as neonatal resuscitation, kangaroo mother care and infection prevention. Other common interventions were postnatal check-ups, training of health workers and HIV prevention or follow-up through prevention of mother-to-child transmission (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Neonatal health interventions. STI, sexually transmitted infection.
There were more reported interventions on newborns living in camps (69%) compared with those living out of camps (16%). The three most common newborn interventions in camps were essential newborn care, postnatal check-ups and training, while the most common intervention outside of camps was health worker training (figure 6). There were no reported instances of interventions targeting HIV or malaria or delivering vaccinations or micronutrient supplementation among newborns outside of camps.
Delivery characteristics of newborn health interventions
Personnel
Newborn interventions were delivered by SBAs, doctors, nurses, health workers and NGO staff (figure 4). NGO staff were reported to deliver essential newborn care and training interventions. Trained TBAs were also reported to deliver essential newborn care. There were no reports of interventions delivered by CHWs or trained community members. There were no major differences between delivery personnel used for refugee compared with IDP populations. However, there were no reports of OB/GYN specialists being used to deliver newborn interventions among IDP populations. There were also no reports of nurses delivering newborn interventions in refugee populations. There were very few observations of interventions delivery among non-displaced newborns.
Sites
All newborn interventions were delivered in hospitals and clinics (figure 5) There were no reported newborn interventions delivered from an outreach or community-based platform. With very limited reporting on newborn interventions delivered outside of camps, it is not possible to compare delivery sites by camp status.
Reported coverage and effectiveness of MNH interventions
Full details of the retrieved intervention coverage and effectiveness data are presented in the online supplemental appendices C and D. Most estimates were derived from camp-based refugee populations. The majority of reported outcomes in pregnant women assessed coverage of ANC interventions such as the proportion of women accessing four or more ANC visits or the proportion of women receiving different components of ANC such as behavioural education, HIV/STI testing or malaria treatment. Other commonly reported coverage outcomes were on obstetric care such as the rate of caesarean sections and other major obstetric interventions. There were very few outcomes on postnatal care, with only two publications reporting on the proportions of postpartum women attending a postnatal consultation.
The majority of maternal intervention effectiveness estimates reported on the odds of receiving all ANC medical tests or visits, or of delivering at home in women who had received a maternal and child health handbook or maternal education compared with those who had not. There were also a small number of estimates reported regarding the effect of having a CHW in a village on the likelihood of a pregnant women receiving ANC or of having SBA at birth.
The included publications reported very few coverage or effectiveness estimates for newborn interventions. Coverage estimates included those for initiation of breast feeding, kangaroo mother care, antiretroviral (ARV) prophylaxis and healthcare worker training. Effectiveness estimates reported on the rate of exclusive breast feeding after an educational intervention and the rate of death in infants in a special care baby unit after training health workers.
No meta-analysis of intervention coverage or effectiveness data was undertaken given the wide variation in outcome definitions and measures, population characteristics and study designs.
Barriers to and facilitators of intervention delivery
There were multiple reported barriers to delivering MNH interventions in conflict settings; key barriers and examples are presented in table 2. The most commonly reported barriers were security constraints and displacement. Populations are often not able to access healthcare facilities due to security issues, and in some cases, because facilities have been destroyed. Continuous population movement also limits women’s access to services, and as health workers are likely also affected by the conflict, there may be staff shortages and high turnover. Other reported barriers include lack of infrastructure and resources to provide EmOC services, lack of specialised health workers and stigma towards refugees. A few publications also mentioned a lack of guidelines, such as newborn-specific protocols.
Reported barriers and facilitators in the implementation of MNH interventions
Despite the barriers, there were other factors that were reported to facilitate the delivery of interventions. The presence of skilled and dedicated staff, as well as having a trained doctor/midwife present to provide mentorship for other staff, were noted as facilitators. Another important facilitator reported was the further training of existing healthcare workers. Involving CHWs and training TBAs from the same populations as those being served were also noted as facilitators; these are usually trusted members of the community with whom local women may feel more comfortable. Other reported facilitators include multisectoral collaboration between NGOs and the existing health system, having adequate funding, and refugee participation, among others (table 2).
Discussion
Principal findings
The majority of reported maternal health interventions delivered in conflict settings focused on ANC and its different components. Caesarean sections and the availability of EmOC more broadly were also reported relatively commonly, but with little detail on EmOC components. Postnatal care was reported relatively infrequently, also with little detail about what such care was composed of. Maternal health interventions were reported to be delivered mainly by skilled health workers and within hospitals and clinics, but health posts and mobile clinics were also cited, as well as homes and communal spaces at the community level. We did note some differences in delivery personnel and sites between in-camp and out-of-camp mothers, where out-of-camp mothers are mostly attended to by lower cadres of health workers and where communal spaces are used more often.
There were very few reported newborn health interventions, focusing mostly on essential newborn care delivered by trained health workers, or in some cases, by TBAs. Nearly all reported newborn interventions were delivered within hospitals or clinics, with only one (postnatal check-up) delivered in a health post, and none were delivered using a community-based approach. Due to the limited literature, it is difficult to compare the delivery of interventions for neonates born in camps with those born outside of camps.
Conflict hinders the delivery of MNH interventions and common barriers reported include the lack of safety, population displacement, limited resources and services, and a lack of skilled health workforce. Where the workforce is available, there are other barriers such as lack of clear guidelines. However, other factors such as availability of funding, multisectoral collaboration, training and supervision of staff, as well as involving CHWs and refugees, were all reported to have facilitated the delivery of MNH interventions.
Most publications that included quantitative data reported on intervention coverage, and the majority on ANC coverage specifically. There were very few publications that reported on effectiveness of MNH interventions; some studies did compare the rates of caesarean sections or other major obstetric interventions before and after the introduction of an intervention such as the training of health workers. Reported quantitative data on newborn health were mainly coverage estimates of the initiation of ARV prophylaxis in infants exposed to HIV and on initiation of breast feeding. It was not possible to infer differences in intervention coverage or effectiveness by delivery characteristics because of the large variability in outcome measures and populations.
Evidence gaps
No publications reported on the use of lay community members in the delivery of MNH interventions in conflict settings. It has already been shown that involving community members, including men and community leaders, in the promotion and delivery of maternal health interventions such education/campaigns can be highly effective,136 and refugee participation was also noted as a facilitator in one of the studies.
We found very limited literature on newborn care, perhaps reflecting the relative neglect that this area continues to endure in LMICs more generally. However, this may also simply reflect relatively limited reporting of newborn care interventions in the literature to date, rather than actual intervention priorities in the field. While it is encouraging that most reported neonatal interventions were able to be delivered in hospitals and clinics, there may be missed opportunities to use outreach and community-based sites such as health posts or homes, especially when it comes to postnatal care and follow-up for diseases such as HIV. Lower cadre health workers such as CHWs, who seem to be underused when it comes to newborn health, could also be used to deliver these interventions.
There was limited literature on the implementation of the Minimal Initial Service Package (MISP), which is considered key, universal guidance for sexual and reproductive health at the onset of an emergency, including for reducing maternal and neonatal mortality. While a few articles did mention following the MISP guidelines, these did not provide further details on which components. Few publications reported quantitative data, and of those that did, most reported on intervention coverage, mainly ANC coverage. However, even within this one area, there is much variability between publications with respect to how coverage is defined and reported, including with respect to whether such care was provided by skilled health personnel. There is also very limited evidence reported about the effectiveness of these interventions.
Overall, despite the inclusion in this review of many publications reporting on the delivery of MNH interventions, there remains limited information in the literature on how interventions are delivered, and limited consistency with respect to which aspects of delivery are reported and in how much detail. Stronger scientific reporting of intervention delivery in both the indexed and grey literature, including more detailed information on how interventions were implemented, where and by whom, could ultimately inform and improve future programmatic decision-making in the field.
Study strengths and weaknesses
While we sought to retrieve a comprehensive selection of the grey literature reporting on MNH intervention delivery in conflict settings, the very large volume of potentially relevant reports meant that we had to restrict our search, and we may not have captured the full range of relevant interventions and their delivery characteristics. Moreover, at least some gaps in the existing literature likely reflect reporting gaps rather than actual programmatic gaps, given the many constraints on data collection in conflict settings and on humanitarian health responders’ time and research capacities. Nonetheless, this is the first review, to our knowledge, to systematically capture and synthesise reported information in both the indexed and grey literature on how MNH interventions targeting conflict-affected populations have been and are being delivered in the field.
Conclusion
While the challenges of research in humanitarian crises make it difficult to determine how well the existing literature on MNH intervention delivery in conflict settings reflects what is actually happening in the field, our results indicate a number of potential implications for research, programming and policy. There is a clear need for more and better reporting on how, where and by whom essential interventions are delivered in conflict settings, and more and better evaluation of the effectiveness of the delivery platforms used. In particular, robust evaluation of the wider use of lower level health workers, including those recruited from affected communities, to deliver a range of MNH interventions outside of camp settings would be especially useful. Further, despite the continued high burden of neonatal mortality in crisis settings, the delivery of newborn health interventions in conflict settings still does not appear to be sufficiently prioritised. This needs to change, urgently.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @fjsepi
Contributors ZAB, MFG and FJS conceptualised the review. FJS created the search strategy and conducted the literature search in electronic databases. DSK conducted the grey literature search. MM, DSK, SM, DA, MK, RPJ, SS and AR screened studies for eligibility and performed data extraction. MM and SM conducted the analysis with support from MFG and FJS. MM drafted the manuscript, and MFG and ZAB critically revised it. All authors approved the final version.
Funding As coordinator of the BRANCH Consortium (Bridging Research & Action in Conflict Settings for the Health of Women & Children), the Sick Kids Centre for Global Child Health has received funding for research activities from the International Development Research Centre (IDRC) (108416-002 & 108640-001), the Norwegian Agency for Development Cooperation (Norad) (QZA-16/0395), the Bill & Melinda Gates Foundation (OPP1171560), and UNICEF (PCA 20181204). Aga Khan University has received funding for BRANCH activities from the Family Larsson-Rosenquist Foundation.
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplemental information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.