Article Text

Abstract
Singapore, one of the first countries affected by COVID-19, adopted a national strategy for the pandemic which emphasised preparedness through a whole-of-nation approach. The pandemic was well contained initially until early April 2020, when there was a surge in cases, attributed to Singapore residents returning from hotspots overseas, and more significantly, rapid transmission locally within migrant worker dormitories. In this paper, we present the response of Singapore to the COVID-19 pandemic based on core dimensions of health system resilience during outbreaks. We also discussed on the surge in cases in April 2020, highlighting efforts to mitigate it. There was: (1) clear leadership and governance which adopted flexible plans appropriate to the situation; (2) timely, accurate and transparent communication from the government; (3) public health measures to reduce imported cases, and detect as well as isolate cases early; (4) maintenance of health service delivery; (5) access to crisis financing; and (6) legal foundation to complement policy measures. Areas for improvement include understanding reasons for poor uptake of government initiatives, such as the mobile application for contact tracing and adopting a more inclusive response that protects all individuals, including at-risk populations. The experience in Singapore and lessons learnt will contribute to pandemic preparedness and mitigation in the future.
- health systems evaluation
- public health
- respiratory infections
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Singapore was among the first countries affected by COVID-19. Its health system resilience was tested as the pandemic continued to spread following a surge in the number of infected people in early April.
The strength in the response of Singapore to the COVID-19 pandemic was in part due to coordination between government agencies. However, we identified a few areas of improvement that may provide important learning points for other countries.
Understanding reasons for poor uptake of initiatives, such as the mobile application for contact tracing, may help design of future initiatives that garner more public support.
Adopting a more inclusive response that protects all individuals, including at-risk populations such as migrant workers living in dormitories, is vital to curb community transmission of outbreaks.
Introduction
On 30 January 2020, WHO declared coronavirus disease 2019 (COVID-19) as an international public health emergency. Singapore, a city state of 5.7 million people, densely populated at 7866 people per square kilometre, was among the first countries affected.1 Since then, progressive measures were in place to detect and contain the disease. As of 20 August 2020, Singapore has 56 099 confirmed cases, reflecting more than 50-fold increase since April, but has kept case fatality rate lower than 0.1% (27 deaths).2 The surge in cases started in early April and was attributed to Singapore residents returning from hotspots overseas, and more substantially, rapid transmission locally within migrant worker dormitories.
Singapore received initial recognition from WHO for its approach in COVID-19 containment.3 However, its health system resilience was tested as the pandemic continued to infect more people. Health system resilience is the ability of populations to prepare for and effectively respond to crises, by reorganising systems to manage the new conditions while maintaining core functions.4 In this paper, we present the COVID-19 pandemic response of Singapore based on core dimensions of health system resilience during outbreaks, as elaborated by Nuzzo et al4 and Legido-Quigley et al.5 We have adapted the core dimensions into eight critical functions for our paper, including leadership and governance, risk communication, public health outbreak containment measures, financing, health service delivery, human resources, legal foundation, as well as political factors and values that shape the response, experiences and behaviours of individuals and communities during the outbreak. Considering the surge of cases since April 2020, we also reviewed its significance and highlighted interventions to contain it.
Leadership and governance
The national strategy for pandemic in Singapore emphasised preparedness through a whole-of-nation approach. Since the 2003 Severe Acute Respiratory Syndrome (SARS) outbreak, nationwide efforts were implemented to prepare institutions and individuals for pandemic response. Organisations simulated possible scenarios of pandemics and developed corresponding outbreak management plans.6 A multiministry government taskforce was convened to coordinate actions between clinical and non-clinical stakeholders, centralise efforts and disseminate information.7 The taskforce, comprising heads of ministries, led and coordinated actions between different agencies. For example, Ministry of Health (MOH) worked closely with academic institutions to provide timely epidemiological and clinical data about COVID-19 in the population. The taskforce designed and implemented measures which were guided by scientific evidence.
Risk communication
Clear communication channels between the government and all sectors are essential to translate policy into intended actions. The taskforce was transparent and frequent in providing situational updates, as well as new guidance and its associated rationale through traditional and social media channels, and regular press conferences. These nationwide communication channels were vulnerable to misinformation. MOH regularly clarified misinformation, encouraging the public to follow accurate and reliable information on official channels.
Public health outbreak containment measures
Singapore adopted a three-pronged approach to contain COVID-19: (1) reducing spread from imported cases; (2) detecting and isolating cases early; and (3) emphasising and supporting social responsibility.8
Reducing spread from imported cases
Since identification of the first imported case in Singapore, various phases of travel restrictions were implemented as the global situation worsened. Starting from outbound and inbound short-term travellers to and from China, restrictions progressively expanded to other countries internationally.9 Travellers and returnees exhibiting fever or respiratory symptoms had to undergo COVID-19 swab tests at the checkpoint. All returnees had to serve a 14-day ‘Stay-Home Notice (SHN)’.10 Following a rise in number of cases linked to Singapore residents returning from hotspots overseas, the SHN was observed in dedicated facilities to reduce exposure to household members. Progressive reopening in June 2020 allowed returnees from selected countries to serve their SHN at home if they remained in those countries the last consecutive 14 days.11 Deferment of outbound travel was still advised. Short-term visitors were still not allowed entry, except for official travel permitted under special arrangements.
Detecting and isolating cases early
Singapore employed complementary detection methods when the outbreak started.12 Case definitions were based on clinical and epidemiological data, updated regularly according to evolving global situations. There was enhanced surveillance for patients with pneumonia or prolonged acute respiratory symptoms and patients in intensive care units (ICUs). Physicians were given discretion to test patients for COVID-19 based on clinical suspicion even if case definition was not fulfilled. Laboratory testing capacity was scaled up in phases, expanding to all public hospitals and major private laboratories. As of 1 June 2020, more than 408 000 tests were conducted (71 700 tests per million population), with plans to increase testing capacity from 8000 to 40 000 tests per day.13
Individuals who tested positive were immediately isolated and interviewed for contact tracing. Contact tracing operations led by MOH were aided by dedicated contact tracing teams at the hospitals, the Singapore Armed Forces (SAF) and the Singapore Police Force.14 Hospital contact tracers interviewed confirmed cases to map their activity history over the last 14 days prior to onset of symptoms, until diagnosis and isolation. This information was passed to MOH where their contact tracers called people whom the patient had interacted with, to fill information gaps, and to identify close contacts. Close contacts and lower-risk contacts identified were placed under quarantine and phone surveillance, respectively. More than 1300 personnel from SAF and Ministry of Defence helped trace and monitor all contacts via phone during the 14-day period, referring those who reported symptoms to hospitals.15 Importantly, cases were isolated at hospitals or community isolation facilities, akin Fangcang hospitals in China, rather than at home where they might infect household members.16
More than 800 Public Health Preparedness Clinics (PHPCs) were activated to enhance detection and management of potential cases. PHPCs were private primary care clinics responsible for screening and referring severe cases to hospitals, while advising patients with mild influenza-like symptoms to isolate at home and prevent community transmission. PHPCs also performed COVID-19 diagnostic testing through the Swab and Send Home (SASH) programme. A web-based COVID-19 Symptom Checker helped individuals navigate care options based on their symptoms, age and travel history.17
To strengthen contact tracing efforts, the TraceTogether application was launched.18 It used Bluetooth signals exchanged between mobile phones to identify individuals who have come into close contact with a COVID-19 patient, thereby minimising recall limitations. The application’s developer code was made publicly available.19 However, uptake was not yet sufficient to replace manual contact tracing, as only 1.1 million people (less than one-fifth of total population) have downloaded the application 2 months after its launch.20 In view that low uptake could be attributed to technical limitations of the application and necessity for a smartphone for participation, a wearable device using the same technology was developed.21 The device was intended for nationwide distribution for universal coverage. Privacy was also an issue. Despite reassurance from the government, many still expressed concern about personal data being used for surveillance purpose. SafeEntry, a national digital location check-in system, was implemented as well.22 Individuals visiting public spaces including workplaces and social venues had to scan a Quick Response (QR) code to check-in before they were allowed entry.
Emphasising and supporting social responsibility
MOH consistently emphasised that social responsibility is the key to slowing transmission: practise good hand hygiene, avoid touching face unnecessarily, use masks appropriately and minimise contact with others when unwell, seek medical aid at the earliest onset of any respiratory symptoms and refrain from doctor shopping.
A series of physical distancing measures were progressively implemented prior to a nationwide partial lockdown, termed as a ‘circuit breaker’, in April 2020.23 Public gatherings were initially restricted to below 250, and subsequently less than ten people. Temperature screenings were required before entry to facilities, and dining venues required a seating distance of at least 1 m apart for unrelated parties. Ambassadors were deployed at various premises to facilitate compliance to social distancing measures. Real-time updates of crowd levels in parks and malls allowed individuals to make informed visits while maintaining social distance. Other initiatives to help individuals during the outbreak were made publicly available on official websites.24
Wearing of masks was initially encouraged only if unwell, as little evidence suggested protection for healthy individuals. Since April 2020, based on new evidence about presymptomatic and asymptomatic transmission, wearing of masks was mandatory outside the household, except for children below 2 years and adults engaged in strenuous activities such as running.25 To ensure public access to some protection, three nationwide reusable cloth mask distribution drives were conducted.
Following announcements of enhanced social distancing measures, workplaces were advised to implement business continuity plans, including work from home or team segregation arrangements.26 Other recommendations included developing plans to screen visitors and employees at work premises. Schools employed measures including suspension of large group activities and staggering of recess times. In line with the ‘circuit breaker’ and parents telecommuting from home, full home-based learning (HBL) was implemented in April 2020.27 Limited care services were provided for parents in essential services without alternative care arrangements for their children. Midyear school holidays were brought forward from June to May, to provide a respite from the month of HBL.28
Health systems financing and economic issues
It is vital to reduce financial barriers to healthcare and encourage care-seeking behaviours during disease outbreaks if infection is suspected. When the outbreak started, the government declared that it would finance treatment costs incurred by COVID-19 patients in public hospitals.29 Most private insurers have also extended coverage for hospitalisation due to COVID-19. To deter non-compliance with guidelines, residents and long-term pass holders who disregarded travel advisories would not be subsidised at public hospitals, if admitted as suspected or confirmed COVID-19 patients within 14 days on return.30 From June 2020, all travellers entering Singapore were required to self-fund their COVID-19 tests and stay at dedicated facilities if necessary.
This pandemic threatened not only the health but also the livelihood of many. The government has committed 60 billion Singapore Dollars (SGD) (~42.4 billion USD, 12.2% of Singapore’s gross domestic product) to help businesses stay viable, preserving jobs and protecting livelihoods.31 The Quarantine Order Allowance Scheme allowed self-employed individuals or employers whose employees were serving Quarantine Orders to claim 100 SGD per day, while the Temporary Relief Fund and COVID-19 Support Grant helped low-to-middle-income Singaporeans tide through the crisis. For example, low-income workers who have lost jobs were entitled to 800 SGD monthly for 3 months.
Health service delivery
Following the SARS outbreak, Singapore prioritised building a specialised infectious disease centre for outbreak management.12 The National Centre for Infectious Diseases (NCID), inaugurated in 2019, is a 330-bed purpose-built infectious diseases management facility with integrated clinical, laboratory and epidemiologic functions. It houses a screening centre, isolation and cohort wards, ICUs, laboratories, imaging facilities and operating theatres.
Adaptation of care and surge capacity
Hospitals in Singapore scaled down non-critical operations to provide both clinical and non-clinical manpower for outbreak response. Separately, the government sourced for additional manpower. The Singapore Healthcare Corps, managed by MOH, was formed as a call for former healthcare professionals to support the healthcare workforce.32 Volunteers were referred to areas of need if there was a match with available opportunities.
Drawing lessons from previous SARS outbreak, the government ensured adequate national stockpiles of personal protective equipment (PPE) and essential medicines for up to 6 months.33 Health Sciences Authority (HSA) granted waivers on importer’s licences to accelerate PPE importation.34 Local companies initiated mask manufacturing lines and donations to alleviate supply shortage.35 Existing tests based on real-time PCR viral detection required a turnaround time of at least 3 hours. Research groups in Singapore developed point-of-care test kits capable of viral detection within minutes.36 One of which was already allowed for sale in the European Union, and have received relevant HSA approvals.37 Ventilator production was expected to scale up significantly in the months to follow.38
Avenues were explored to ensure sufficient facilities for treating patients. The capacity of NCID could be increased from 330 to over 500 beds during outbreaks. Collaboration with private and community hospitals and conversion of non-healthcare buildings to community care facilities allowed transfer of COVID-19 patients with mild symptoms for monitoring, reducing the load on public hospitals.39
Maintaining core health service capabilities
Patients with chronic conditions had their clinic appointments postponed unless immediate medical attention was required.40 Provisions were made for patients with postponed appointments to obtain medication refills via home delivery.41 Telemedicine services, where patients could consult physicians through mobile video conferences, have expanded following an increased demand with implementation of social distancing measures.42
Human resources
In Singapore hospitals, mask fitting sessions and structured training were organised to ensure appropriate handling of PPE for all deployed healthcare workers (HCWs).40 HCWs changed PPE in between care for each isolated patient, as well as during movement between a COVID-19 cohort ward and a designated clean area. Innovative solutions were developed, including the ‘Swab Assurance For Everyone’ (SG SAFE) booth for large-scale screening of potential COVID-19 patients to protect HCWs behind the booth while reducing PPE utilisation.43 To maintain full crisis capability, team segregation within each discipline was practised, ensuring provision of continued care in the event a team was quarantined due to suspected exposure to COVID-19. Movement of HCWs between hospitals was limited to reduce cross infection. As of 4 May 2020, there were 66 COVID-19 cases among HCWs.44 Although these cases, except for one, had no established epidemiological link to indicate nosocomial transmission, and vulnerabilities of HCWs in this health crisis were clear from the experiences of other countries.45 Timely, accurate and honest reporting from hospital leadership helped alleviate concerns among HCWs. This, together with messages of support and gratitude from the community, helped boost resolve and morale of HCWs.
Legal foundation
The COVID-19 (Temporary Measures) Act and COVID-19 (Temporary Measures) (Control Orders) Regulations 2020 was enforced to complement policy measures in managing the outbreak.46 This legislation allowed the government to requisition any land, undertaking or other resources for the purpose of control order. It also provided legal basis to enforce social distancing measures, such as a limitation on mass gatherings, and hold individuals as well as business owners accountable for violation.
Political environment and values of the community
Initial success for COVID-19 containment was attributed to Singapore’s dexterous political environment, which allowed the government space to swiftly institute measures.47 The Disease Outbreak Response System Condition (DORSCON) framework, which was part of the standing national pandemic preparedness plan, was adopted for the COVID-19 outbreak. The colour-coded framework provided guidance on outbreak severity and on the required public response to prevent and reduce impact of infections.48 The taskforce stepped up risk assessment from DORSCON Yellow to DORSCON Orange on 7 February 2020. This led to sporadic instances of public panic purchasing essential supplies.49 The prime minister made national addresses to assure Singapore residents of sufficient medical supplies and daily necessities, provide an assessment of the COVID-19 situation and urge strict adherence to containment measures. These national addresses were followed by press conferences to reinforce specific adjustments to guidelines.
Experience from previous SARS outbreak has prepared Singapore residents on what to expect and how to react. Some similar measures implemented before included school closures, temperature checks, screening for fever and travel history to affected countries and home quarantine, although at a smaller scale. In addition, Singapore residents’ respect for authority, coupled with stringent regulations, has allowed smooth implementation of governmental measures. The advent of social media allowed faster information dissemination while providing a platform for community and emotional support. It has also allowed online vigilantism to become more prevalent.50 While this could aid compliance to rules, reporting potential infringements directly to the authorities have been recommended.
Rise in cases from April 2020
A timeline of significant events and implementations is shown in figure 1. Despite rigorous containment and mitigation efforts, there was a sharp rise in local transmissions, likely due to imported cases, from early April 2020. On 7 April 2020, the government initiated a 1-month ‘circuit breaker’ measure, which was later extended for another month.51 Most workplace premises were closed, and the public were asked to stay home and avoid unnecessary outings. Schools migrated to HBL. Only essential services, including pharmacies, hospitals, clinics, supermarkets, food establishments, banking services and transport, could operate. All public gatherings were prohibited during this period. The government escalated efforts to protect the vulnerable, particularly seniors, during the ‘circuit breaker’ period. Volunteers were deployed to educate seniors who lived by themselves about these precautionary measures. Those who required additional support were identified and connected with relevant service providers.
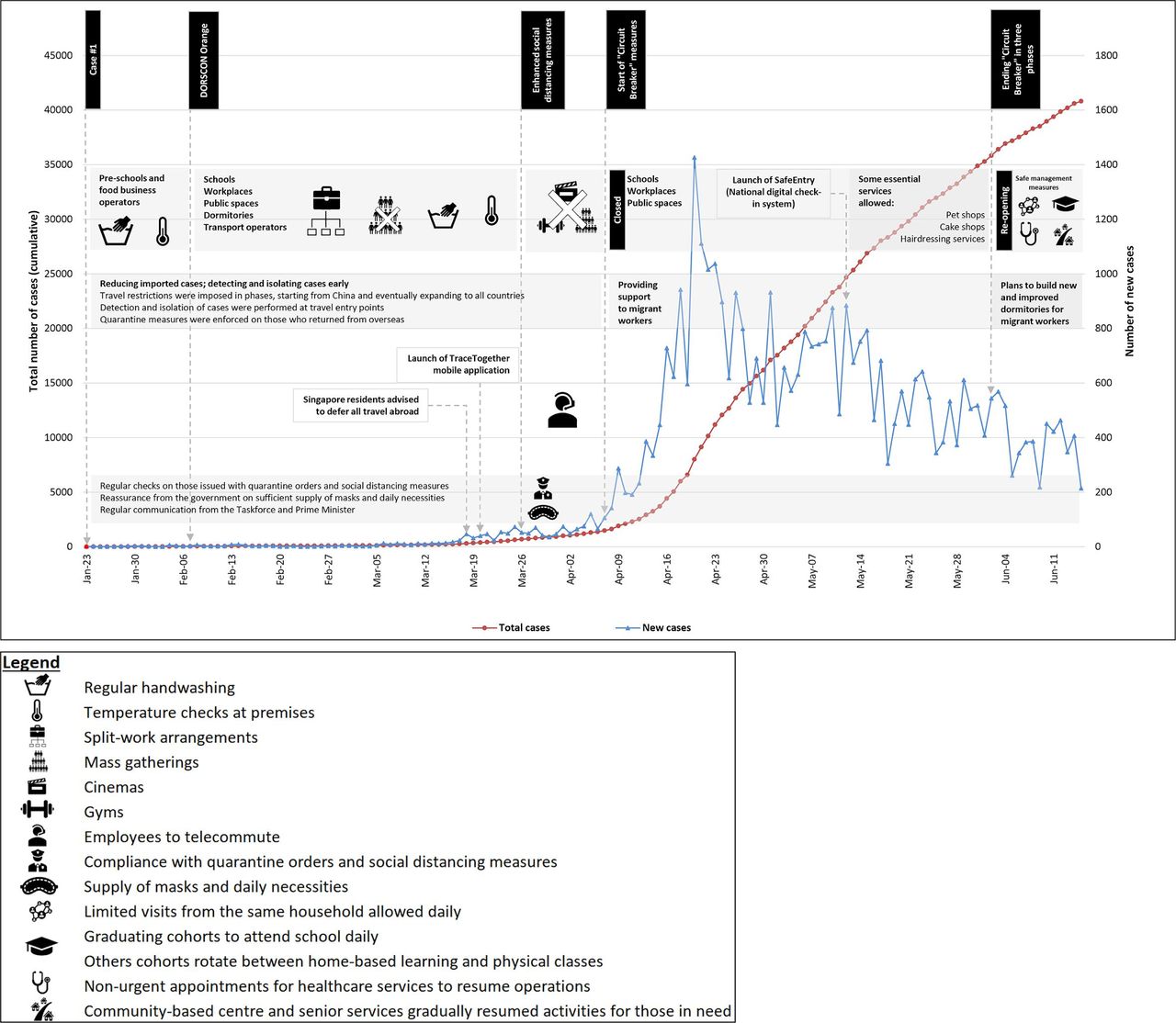
{kind=link}
Timeline of significant COVID-19 events and implementations in Singapore updated to June 2020. Source: Ministry of Health, Singapore. DORSCON, Disease Outbreak Response System Condition.
A large portion of the increase was attributed to rapid transmission within migrant worker dormitories. In response, a second taskforce was set up to support this outbreak.52 Various measures were implemented to interrupt transmission in this community, including: (1) active testing of potential cases in dormitories and provision of good medical care;53 (2) identifying new housing areas to accommodate healthy workers;54 and (3) providing translated health information to empower self-protection. By the time of writing, these measures have contained further spread of virus within the dormitories and in the community.55 However, conditions in these dormitories must be improved to prevent similar outbreaks. The government announced short-term and long-term plans for improvement. Migrant workers were housed temporarily in unused state properties, while the upcoming quick-build dormitories were being developed.56 These temporary accommodations were proposed to be replaced by permanent and less dense purpose-built dormitories once ready.
Singapore embarked on a planned three-phased approach to resume activities safely once the ‘circuit breaker’ ended on 1 June 2020.57 Phase 1 involved allowing household visits of up to two immediate family members and reopening of workplaces and schools. Those who could telecommute had to continue working from home, while students had to rotate between HBL and returning to school. Phase 2 involved resumption of most businesses that ceased operations during the ‘circuit breaker’ and small-group gatherings of up to five people. Phase 3 would involve resumption of higher-risk activities with larger numbers of people including religious services and entertainment venues. There was no fixed duration for each phase and transition between phases was determined by community transmission rates and the testing, contact tracing and healthcare capacity.
Lessons learnt from Singapore
Four important lessons from the Singapore experience could inform future strategies in managing pandemics in other high-income countries. First, consistency and transparency in information communicated by a trusted figure and team promotes acceptability of policy measures. Concise public messages tailored to the community and cultural norms accelerate public awareness of health crises. These, in turn, facilitate public trust in leadership and cooperation in containment efforts. Next, an established and clear legal framework reduces the possibility of misinformation during crisis and enhances clarity in risk communication. Third, vigorous testing and contact tracing to identify and isolate cases promptly are important for outbreak containment. Technology helps facilitate contact tracing efforts. However, more work needs to be done to mitigate potential issues such as privacy concerns, and to design methods to improve uptake of information technology (IT)-based contact tracing tools. Providing reassurance on how contact tracing personal data will be collected, used and stored could strengthen public support. Lastly, greater emphasis on dense or at-risk populations, for example, migrant workers living in dormitories, was vital to curb community transmission of COVID-19. More efforts are required to prevent potential recurrence, including dormitory housing expansion and enhancement of migrants workers’ social cohesion with the rest of the society.55 An equitable and inclusive response that protects the health and rights of all individuals, especially the most vulnerable, is necessary to overcome such crises.
Conclusion
We have explored the COVID-19 pandemic response of Singapore based on dimensions of health system resilience during outbreaks. There was: (1) clear leadership and governance which adopted flexible plans appropriate to the situation; (2) timely, accurate and transparent communication from the government; (3) public health measures to reduce imported cases and detect as well as isolate cases early; (4) maintenance of health service delivery; (5) access to crisis financing; and (6) legal foundation to complement policy measures. Areas for improvement include understanding reasons for poor uptake of initiatives such as the mobile application for contact tracing and adopting a more inclusive response that protects all individuals, including at-risk populations. The experience in Singapore and lessons learnt will contribute to pandemic preparedness and mitigation in the future.
Footnotes
Handling editor Seye Abimbola
Twitter @alvinchuaqj, @melisamjtan, @monica_v17, @hsuliyang, @legidoquigley
Contributors AQC, MMJT, MV, EKLH and HL-Q conceived the paper and prepared the initial draft. AQC led the writing process. All authors contributed to the original content and revisions to the text. All authors gave final approval of the version to be published.
Funding This research is funded through the Singapore Population Health Improvement Centre (SPHERiC) Collaborative Centre Grant from the National Medical Research Council, Singapore (NMRC/CG/C026/2017_NUHS).
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.