Article Text

Abstract
Introduction Healthcare providers in resource-limited settings rely on the presence of tachypnoea and chest indrawing to establish a diagnosis of pneumonia in children. We aimed to determine the test characteristics of commonly assessed signs and symptoms for the radiographic diagnosis of pneumonia in children 0–59 months of age.
Methods We conducted an analysis using patient-level pooled data from 41 shared datasets of paediatric pneumonia. We included hospital-based studies in which >80% of children had chest radiography performed. Primary endpoint pneumonia (presence of dense opacity occupying a portion or entire lobe of the lung or presence of pleural effusion on chest radiograph) was used as the reference criterion radiographic standard. We assessed the sensitivity, specificity, and likelihood ratios for clinical findings, and combinations of findings, for the diagnosis of primary endpoint pneumonia among children 0–59 months of age.
Results Ten studies met inclusion criteria comprising 15 029 children; 24.9% (n=3743) had radiographic pneumonia. The presence of age-based tachypnoea demonstrated a sensitivity of 0.92 and a specificity of 0.22 while lower chest indrawing revealed a sensitivity of 0.74 and specificity of 0.15 for the diagnosis of radiographic pneumonia. The sensitivity and specificity for oxygen saturation <90% was 0.40 and 0.67, respectively, and was 0.17 and 0.88 for oxygen saturation <85%. Specificity was improved when individual clinical factors such as tachypnoea, fever and hypoxaemia were combined, however, the sensitivity was lower.
Conclusions No single sign or symptom was strongly associated with radiographic primary end point pneumonia in children. Performance characteristics were improved by combining individual signs and symptoms.
- pneumonia
- child health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Pneumonia is the leading cause of morbidity and mortality among children 1–59 months of age worldwide.
The diagnosis of childhood pneumonia is often established based on clinical findings, as the definitive aetiological diagnosis can only be made using invasive testing.
Antibiotic treatment decisions for children with suspected pneumonia in low-income and middle-income countries rely largely on clinical findings, including tachypnoea and chest indrawing.
What are the new findings?
Our study of over 15 000 children from geographically diverse parts of the world is the largest to date to assess the test characteristics of clinical signs and symptoms for radiographic pneumonia among children 0–59 months of age.
Individual findings commonly used to identify pneumonia in resource-limited settings, including tachypnoea and lower chest indrawing, had low specificity for the diagnosis of radiographic pneumonia.
The combination of tachypnoea and fever, tachypnoea and hypoxaemia, and fever and hypoxaemia led to improved specificity with only a modest decrement in sensitivity for radiographic pneumonia.
What do the new findings imply?
Individual symptoms and physical examination findings are not highly predictive of primary endpoint pneumonia on chest radiograph.
Combining temperature, respiratory rate, and oxygen saturation improves specificity in the identification of radiographic pneumonia.
The diagnostic performance of a combination of signs and symptoms should be explored in a prospective fashion to allow for a judicious approach to antibiotic treatment in children with suspected pneumonia.
Introduction
Pneumonia is the leading cause of morbidity and mortality among children 1–59 months of age worldwide.1 2 Annually, there are over 800 000 deaths from pneumonia among children worldwide.2 Such morbidity and mortality from childhood pneumonia disproportionately affects children in low-income and middle-income countries, with nearly 90% of pneumonia-related deaths occurring in sub-Saharan Africa and South and Southeastern Asia alone.2 3 Despite the large global burden of disease of childhood pneumonia, a commonly agreed upon standardised approach to the diagnosis of pneumonia is lacking.4
The diagnosis of childhood pneumonia is often established based on clinical findings, as the definitive diagnosis can only be made using invasive testing such as lung biopsies, which are reserved for patients in whom traditional therapeutics have failed.5 As such, chest radiography is often used in clinical practice for the diagnosis of childhood pneumonia and has been used as a reference standard in previous investigations.6–10 In a large, multicountry study in Asia and sub-Saharan Africa, chest radiography correlated with clinically diagnosed pneumonia in over half of patients included.11 Nevertheless, the routine use of chest radiography for the diagnosis of childhood pneumonia in the outpatient setting is not recommended by the Infectious Disease Society of America.5 Similarly, the World Health Organization’s (WHO) integrated management of childhood illness (IMCI) chart booklet used in many low-income and middle-income countries, recommends the diagnosis of pneumonia be made clinically, with reliance on tachypnoea or lower chest indrawing in a child with cough or difficulty breathing.12 13 However, recent analyses suggest that the sensitivity (54%–62%) and specificity (59%–64%) of tachypnoea and sensitivity (38%–48%) and specificity (72%–80%) of lower chest indrawing is lower than originally estimated.9 10 14 Concerns around the low specificity of the WHO pneumonia signs, and potential excess antibiotic prescribing, prompted further evaluation of these clinical criteria for the diagnosis of pneumonia in children.
The development of sensitive and specific diagnostic clinical criteria for childhood pneumonia is imperative as chest radiography is not routinely available in many low- and middle-income countries. Previous systematic reviews evaluating the utility of symptoms and physical examination findings for the diagnosis of childhood pneumonia have relied on data reported in published articles, without access to individual patient-level data.9 10 Additionally, the overwhelming majority of these investigations were conducted in high-income countries. The reliance on predetermined cut-points from published articles for clinical criteria such as respiratory rate (RR) and oxygen saturation (SpO2) may lead to imprecision in the analysis of diagnostic clinical criteria for childhood pneumonia.
With the aim of better understanding the clinical diagnostic criteria for childhood pneumonia, the WHO established the Pneumonia REsearch Partnership to Assess WHO Recommendations (PREPARE) study group. The PREPARE study group obtained patient-level data from 30 study groups, comprising 41 separate datasets on childhood pneumonia from across the world. Using the large, representative PREPARE dataset, our objective was to determine the sensitivity and specificity of key clinical features and combination of clinical features in the diagnosis of childhood pneumonia against a radiological reference standard. Accurate identification of children with pneumonia using clinical factors could potentially allow providers to more accurately diagnose childhood pneumonia and, subsequently, more appropriately target antibiotic therapy.
Methods
Study design
We conducted an analysis using datasets from the WHO’s PREPARE study group. The WHO PREPARE study group assembled datasets through retrospective identification of primary data on childhood pneumonia from over 20 low- and middle-income countries in Asia, Africa and Latin America as well as two high-income countries (ie, the USA and Australia). Study sites were considered for inclusion in WHO PREPARE study group if they included data from control arms of vaccine trials, community-based cohorts, and hospital-based studies with clinical and epidemiological data collected. Potential study sites were identified from a list of contributors to a systematic review of global burden of hospital admissions for severe acute lower respiratory infections in children.15 Based on a review of the paediatric pneumonia literature, we identified 50 groups who were involved in pneumonia research who had published articles between 2005 and 2018. These groups had conducted pneumonia research with and without interventions, randomised controlled trials, epidemiological studies, and vaccine trials. We invited all 50 study groups to participate by attending an inception meeting in Ferny-Voltaire, France. Representatives from 38 groups attended that meeting where each investigator presented their site data. As a result of that meeting, 30 study groups agreed to participate and provided 41 unique databases for the WHO PREPARE study group. Datasets were limited to include only data on children 0–59 months of age, despite potentially containing data from older children.
For this study, to include datasets in which chest radiography was performed in a generalisable fashion, we limited our analysis to datasets of hospital-based studies that included data on chest radiography and had a chest radiography performed in >80% of cases. Studies in which chest radiography was performed in <80% of cases may have suffered from selection bias as chest radiography may have been performed only in children with severe illness and at higher risk of pneumonia and were excluded. Community-based studies were not included as chest radiography was rarely performed.
Patient and public involvement statement
The development of the research question was informed by the large disease burden of pneumonia among children worldwide. Patients were not involved in the design, recruitment, or conduct of the study. Results of this study will be made publicly available through publication where study participants may access them. Patients were not advisers in this study.
Pneumonia case definition
Datasets were included in this analysis if they included data on children presenting acutely with cough or difficulty breathing and included pneumonia as defined by the WHO radiological criteria for primary endpoint pneumonia6 (n=8) or if they used lobar consolidation on chest radiography as diagnostic criteria for pneumonia (n=2). Though originally created for use in vaccine trials, primary endpoint pneumonia has been applied to large cohorts of children with pneumonia in several low- and middle-income countries with good inter-rater reliability.16 A majority of the datasets (n=6) included in this analysis enrolled children with tachypnoea, as this is the primary determinant of pneumonia based on the WHO IMCI chart booklet. Primary endpoint pneumonia was selected as the radiographic reference standard as it is clearly defined, is reliable across studies, is independent of predictor clinical variables that are often studied in work evaluating childhood pneumonia, is a clear indication of pneumonia and not viral acute lower respiratory tract infection, and highlights bacterial pneumonia that requires antibiotic treatment. Lobar consolidation was used as a reference standard in two included datasets and has shown high inter-rater reliability among paediatric radiologists in prospective studies.17 All radiographs in the included studies were interpreted by a radiologist; many of the studies required review by two or more radiologists.
Data analysis
Using radiographic pneumonia as the reference standard, we evaluated the sensitivity, specificity, and likelihood ratios (LRs) for individual clinical findings. We calculated 95% CIs for all +LR and −LRs. Candidate variables from patients’ histories that were used to calculate test characteristics included history of cough, fever, difficulty breathing, vomiting, and poor feeding. We evaluated the test characteristics of tachypnoea as defined by the WHO IMCI age-specific cutoffs (ie, RR of ≥60 breaths per minutes in children <2 months old, >50 breaths per minute in children 2–11 months old, and >40 breaths per minute in children 12–59 months old)18 as well as the addition of five and 10 respirations per minute to the age-specific WHO classification of tachypnoea.
Using radiographic pneumonia as the reference standard, we also evaluated the test characteristics of lower chest indrawing, nasal flaring, grunting, wheezing, body temperature, SpO2, presence of rales or crepitations, inability to drink, presence of convulsions, cyanosis, head nodding/bobbing, presence of irritability, lethargy and presence of any danger sign (ie, inability to drink, convulsions, cyanosis, head nodding/bobbing, irritability, abnormally sleepy, lethargy, nasal flaring, grunting, and SpO2 <90%). We stratified analyses by age (<2 months, 2–11 months, and 12–59 months) and by the presence or absence of wheezing. We assessed the test characteristics of varying age-specific RR and SpO2 in patients both with and without wheezing to eliminate children who may have asthma who are sometimes included in studies evaluating pneumonia. We also assessed the sensitivity, specificity, and LRs of combinations of clinical signs and symptoms compared with the reference standard of radiographic pneumonia. We had a study power of >95% to detect a difference in radiographic pneumonia of at least 7% between children who had some clinical features of pneumonia (eg, presence of chest indrawing, any danger sign, temperature >38°C, or SpO2 <90%) and those who did not have these clinical features. All analyses were conducted using Stata V.14 (StataCorp, College Station, TX, USA).
Results
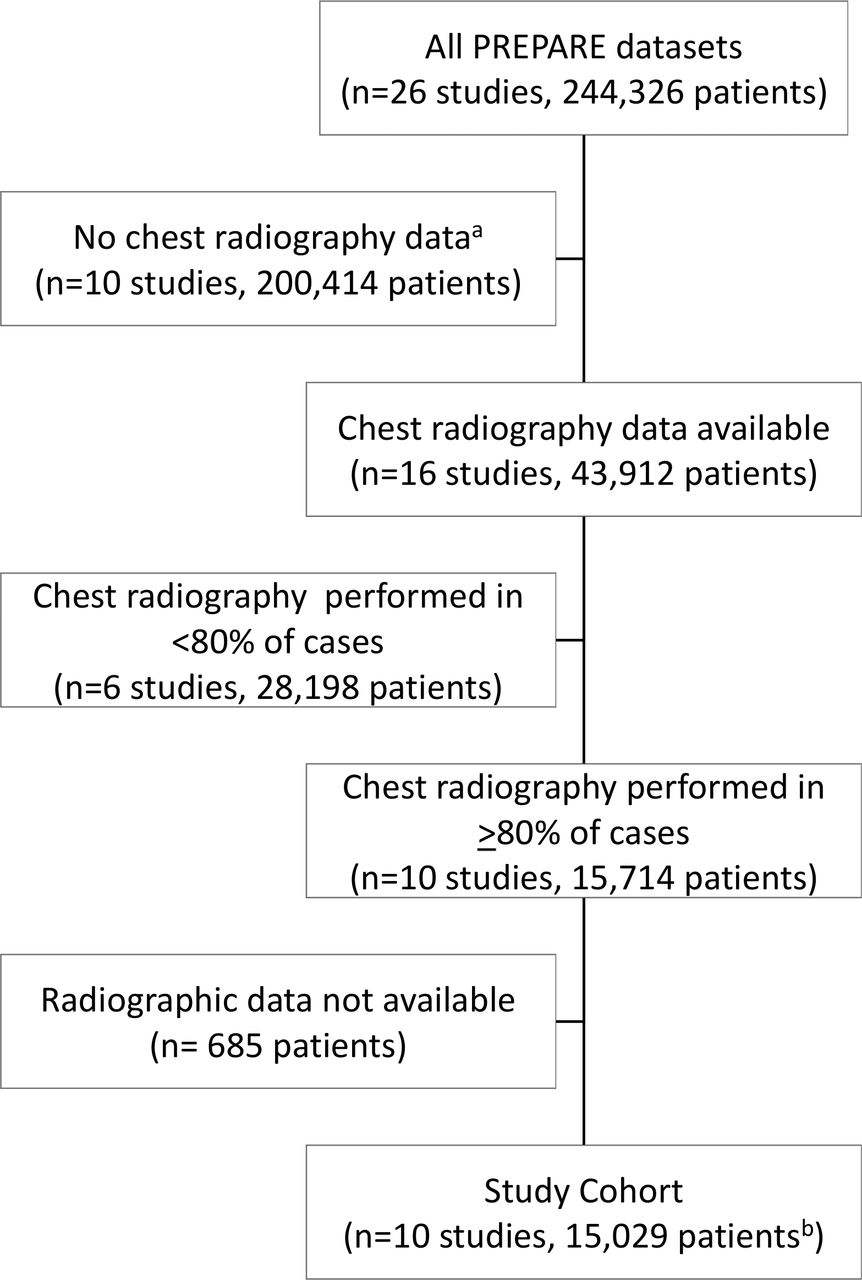
Of the 41 separate datasets, 26 were hospital based, of which 10 met inclusion criteria, containing a total of 15 029 patients (figure 1). The mean age of patients was 13.0 months (standard deviation ±12.3) with median of 9.0 months (4.4–16.9). Details regarding the setting and patient population for the 10 included datasets are shown in table 1. Of the 15 029 patients included, 24.9% (n=3743) had radiographic pneumonia.
{kind=link}
Hospital-based studies including children 0 to <59 months of age. aChest radiography not performed or data regarding presence of pneumonia/infiltrate not recorded. bRadiographic pneumonia in 3743 patients (24.9%). PREPARE, Pneumonia REsearch Partnership to Assess WHO Recommendations.
Study characteristics
The sensitivity and specificity of individual symptoms and physical examination findings for the diagnosis of radiographic pneumonia are shown in table 2. No single sign or symptom was strongly associated with radiographic pneumonia. The presence of poor feeding (+LR 1.67 (95%CI 1.29 to 2.16)), axillary/body temperature >38°C (+LR 1.36 (95%CI 1.31 to 1.41)), head nodding/bobbing (+LR 1.84 (95%CI 1.38 to 2.45)), grunting (+LR 1.72 (95%CI 1.27 to 2.33)), and hypoxaemia at SpO2 <85% (+LR 1.42 [95%CI 1.27 to 1.59)) were weakly associated with the presence of radiographic pneumonia, while the absence of the following features was associated with a lower likelihood of radiographic pneumonia: axillary/body temperature >38°C (−LR 0.77 (95%CI 0.74 to 0.80)), rales/crepitations (−LR 0.73 (95%CI 0.66 to 0.80)), and SpO2 <95% (−LR 0.83 (95%CI 0.78 to 0.88)).
Test characteristics of signs and symptoms of radiographic pneumonia
Age-specific RR thresholds were neither highly sensitive nor specific for the radiographic diagnosis of pneumonia in the overall cohort and among the subset of children without wheezing (table 3). Among children 2–11 months of age, those with RR >60 breaths per minute were more likely to have radiographic pneumonia (+LR 1.08 (95%CI 1.03 to 1.14)), while those with RR <60 were less likely to have radiographic pneumonia (−LR 0.91 (95%CI 0.86 to 0.97)).
Test characteristics of varying respiratory rates (RRs) by age group among all children and those without wheezing*
The test characteristics of SpO2 for radiographic pneumonia for all children and those without wheezing are shown in online supplementary table 1. Sensitivity decreased and specificity increased with increasing levels of hypoxaemia, although no single threshold had optimal test characteristics for the identification of radiographic pneumonia.
Supplemental material
The combinations of varying degrees of hypoxaemia, fever and tachypnoea are shown in tables 4–6. At each SpO2 category, specificity increased with increasing RR. Among children with SpO2 <90%, children with RRs ≥10 breaths per minute above the WHO threshold for age-defined tachypnoea were slightly more likely to have radiographic pneumonia (+LR 1.40 (95%CI 1.28 to 1.53)), while those without this degree of tachypnoea were less likely to have radiographic pneumonia (−LR 0.92 (95%CI 0.90 to 0.94)) (table 4). Among the subset of children with temperature >38°C, those with an RR ≥10 breaths per minute above the WHO threshold for age-defined tachypnoea were slightly more likely to have radiographic pneumonia (+LR 1.24 (95%CI 1.14 to 1.35)) (table 5). The combination of temperature >38°C and SpO2 <85% was highly specific for radiographic pneumonia (specificity 0.96, (95% CI 0.96 to 0.97)) while the sensitivity was quite low (sensitivity 0.07, (95% CI 0.06 to 0.08)) (table 6).
Test characteristics of varying respiratory rates (RRs) with SpO2 levels in children
Test characteristics of varying respiratory rates (RRs) with fever (temperature >38°C) in children
Test characteristics of varying oxygen saturations (SpO2) without and with fever (temperature >38°C) in children
Discussion
Our study of over 15 000 children from geographically diverse parts of the world is the largest to date assessing the test characteristics of clinical signs and symptoms for radiographic pneumonia among children 0–59 months of age. We observed that individual findings commonly used to identify pneumonia in resource-limited settings, including tachypnoea and chest indrawing, had poor specificity for the diagnosis of radiographic pneumonia. The test characteristics of all signs and symptoms did not materially differ based on the presence or absence of wheeze. Our study demonstrates that no individual symptom or physical examination finding was strongly associated with radiographic pneumonia in children. Extreme levels of hypoxaemia were highly specific for radiographic pneumonia, although sensitivity was low. Lower thresholds of hypoxaemia commonly used in clinical settings (ie, <95% and <90%)19 demonstrated moderate sensitivity and specificity for the identification of radiographic pneumonia.
The WHO guideline recommends oral amoxicillin treatment in children 2–59 months of age with chest indrawing.12 20 In our analysis, chest indrawing alone was not specific for the radiographic diagnosis of pneumonia. It has been suggested that children with chest indrawing and signs of severe respiratory distress, oxygen desaturations, moderate malnutrition, and unknown HIV-status in HIV-endemic areas be monitored daily or referred for inpatient management given their risk for decompensation.21 In a large prospective pneumonia aetiology study in low- and middle-income countries, tachypnoea, hypoxaemia, crackles, and fever were all independently associated with an abnormal chest radiograph.11 Oxygen desaturation was the most specific single sign for radiographic pneumonia in our study. In a small, retrospective study of 147 children in Rwanda, oxygen desaturation was significantly associated with radiographic pneumonia.22 In a larger prospective study of nearly 400 children in Norway, hypoxaemia (defined as SpO2 <92%) independently predicted radiographic pneumonia and was the only clinical feature that predicted radiographic pneumonia.23 If available, SpO2 should be measured in children evaluated for pneumonia as the presence of extreme levels of hypoxaemia is highly specific for the diagnosis of radiographic pneumonia.
Although tachypnoea is used to assess for pneumonia in many resource-limited settings, our data showed that commonly used, age-specific RR thresholds were neither sensitive nor specific for the identification of radiographic pneumonia in children. This finding adds further support to the body of evidence suggesting that tachypnoea should not be used as an isolated finding to diagnose pneumonia and subsequently determine which children would benefit from antibiotic treatment.9 10 24 25 Radiographic pneumonia, though often used as the reference standard for the diagnosis of pneumonia, should be interpreted in the context of its limitations including the potential delayed manifestations of radiographic findings, inability to reliably distinguish bacterial and viral infections, and variable inter-rater reliability among radiologists for certain findings suggestive of pneumonia.17 Our investigation used primary end point radiographic pneumonia, which was developed for vaccine trials to identify pneumonia that could be prevented by Streptococcus pneumoniae and Haemophilus influenzae B vaccines and it became a useful and a sensitive tool to evaluate vaccine outcomes.26 27 Primary end point radiographic pneumonia is a subset of all cases of clinical pneumonia.11 Our finding that tachypnoea is not strongly associated with radiographic pneumonia might partially explain the variable results from randomised trials comparing amoxicillin and placebo among children with fast breathing pneumonia.28–30 Furthermore, many children receiving a diagnosis of pneumonia in resource-limited settings may harbour other respiratory illnesses such as asthma or other viral infections as demonstrated by the Pneumonia Etiology Research for Child Health study group.31
Treatment decisions for children with suspected pneumonia in low-income and middle-income countries rely largely on clinical findings, including tachypnoea and chest indrawing.12 13 This allows community health workers and healthcare providers at primary level health facilities to make decisions around antibiotic administration and the need for referral in areas with scarce resources. However, other signs, such as hypoxaemia, are critical to identify as it has been shown to be associated with radiographic pneumonia,9 24 and carries up to a fivefold increased risk of mortality when compared with children without hypoxaemia in low- and middle-income countries.32–36 Our study identified extreme levels of hypoxaemia as highly specific for radiographic pneumonia. Though the WHO IMCI chart booklet recommends use of pulse oximetry when available,12 many low-resource settings lack this tool.37 38 However, the recent development of low-cost technologies for pulse oximetry,39 including hardware attached to mobile phones,40–42 may expand its use in resource-limited settings.
The major strength of our aggregated database containing individual patient-level data is our ability to evaluate the test characteristics of combinations of signs, symptoms, and physical examination findings for the radiographic diagnosis of pneumonia. Prior single-centre studies have not been powered to identify which combinations of clinical findings could be used to identify radiographic pneumonia.24 43–47 Additionally, prior meta-analyses investigating the test characteristics of clinical signs and symptoms for the prediction of radiographic pneumonia observed that no single sign or symptom was highly accurate for the identification of radiographic pneumonia,9 10 and discussed the impetus for future studies to allow for the assessment of a combination of signs and symptoms to improve the care of children with suspected pneumonia. In this study, by aggregating patient-level data from ten investigations, we observed that by combining certain signs and symptoms, including tachypnoea, oxygen desaturation, and fever, we were able to improve the discriminator ability to identify radiographic pneumonia. The diagnostic performance of a combination of signs and symptoms should be explored in a prospective fashion to allow for a judicious approach to antibiotic treatment in children with suspected pneumonia.
Limitations
The results of this analysis should be interpreted in the context of their limitations. First, as many studies used in this analysis used the WHO IMCI definition of tachypnoea and lower chest indrawing as an inclusion criterion, there may be overestimation of the true sensitivity and specificity of tachypnoea in the radiographic diagnosis of childhood pneumonia. Also, the inclusion criterion of tachypnoea as defined by WHO thresholds limited our ability to assess the test characteristics of RRs below the WHO thresholds in the radiographic diagnosis of pneumonia. Second, there was no common standardised approach to define radiographic pneumonia across all 10 studies, though most studies included in this analysis used primary endpoint pneumonia or lobar consolidation, which is part of end point pneumonia definition.16 The inclusion of both primary end point pneumonia and lobar consolidation as the reference standard may have introduced some heterogeneity to our findings but improves the generalisability of our findings to more practical clinical settings. Third, lack of uniformity of recording some signs and symptoms across included studies may have led to overestimation or underestimation of the test characteristics for the signs and symptoms evaluated in this analysis. Fourth, we did not conduct formal statistical analyses to account for heterogeneity in the included studies’ inclusion and exclusion criteria. Fifth, there was a high degree of heterogeneity with respect to study types, settings, type of clinician performing the evaluation, and patient population. Lastly, our findings may not be as applicable to extremely resource-limited settings in which chest radiography is not routinely available.
Conclusions
In this study, including >15 000 children 0–59 months of age, we observed that no individual symptom or physical examination finding was predictive of end point radiographic pneumonia. The presence of tachypnoea as an isolated finding was neither sensitive nor specific, while extreme levels of hypoxaemia was a specific finding among children with radiographic pneumonia. Combinations of commonly used vital signs including temperature, RR and SpO2 improved the specificity for the identification of radiographic pneumonia.
Acknowledgments
We acknowledge the World Health Organization PREPARE study group members including Rajiv Bahl, Wilson M. Were, Lulu M. Muhe, Valerie D’Acremont, Donald M. Thea, Abdullah Brooks, Romina Libster, Joseph Mathew, Tabish Hazir, and Sunil Sazawal.
References
Footnotes
Handling editor Alberto L Garcia-Basteiro
Twitter @lmartinezarroyo
Contributors CAR, MIN, YBN, and SQ conceptualised the study and designed the analysis. MIN, SB, AG, BDG, CBK, ML, LM, K-AFO, ROR, CT, HC, HN, JF, LJW, and MH curated the data. YBN, LJW, and MH conducted the data analysis. All authors contributed to the interpretation of the data. CAR and MIN drafted the original draft of the manuscript. All authors critically reviewed and revised the manuscript.
Funding The study was funded by the Bill & Melinda Gates Foundation (#OPP1106190) through a grant to the WHO.
Disclaimer The funders had no role in the study design or in the collection, analysis, or interpretation of the data. The funders did not write the report and had no role in the decision to submit the paper for publication.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval As this study used de-identified data from existing studies, ethical approval was obtained from each site. Included studies which were sponsored by the WHO additionally received ethical approval from the WHO ethics review committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be made available on reasonable request.