Article Text

Abstract
Introduction Indigenous Peoples worldwide endure unacceptable health disparities with undernutrition and food insecurity often coexisting with obesity and chronic diseases. Policy-level actions are required to eliminate malnutrition in all its forms. However, there has been no systematic synthesis of the evidence of effectiveness of food and nutrition policies for Indigenous Peoples around the world. This review fills that gap.
Methods Eight databases were searched for peer-reviewed literature, published between 2000 and 2019. Relevant websites were searched for grey literature. Articles were included if they were original studies, published in English and included data from Indigenous Peoples from Western colonised countries, evaluated a food or nutrition policy (or intervention), and provided quantitative impact/outcome data. Study screening, data extraction and quality assessment were undertaken independently by two authors, at least one of whom was Indigenous. A narrative synthesis was undertaken with studies grouped according to the NOURISHING food policy framework.
Results We identified 78 studies from Canada, Australia, Aotearoa/New Zealand and the USA. Most studies evaluated targeted interventions, focused on rural or remote Indigenous communities. The most effective interventions combined educational strategies with policies targeting food price, composition and/or availability, particularly in retail and school environments. Interventions to reduce exposure to unhealthy food advertising was the only area of the NOURISHING framework not represented in the literature. Few studies examined the impact of universal food policies on Indigenous Peoples’ diets, health or well-being.
Conclusion Both targeted and universal policy action can be effective for Indigenous Peoples. Actions that modify the structures and systems governing food supply through improved availability, access and affordability of healthy foods should be prioritised. More high-quality evidence on the impact of universal food and nutrition policy actions for Indigenous Peoples is required, particularly in urban areas and in the area of food marketing.
- nutrition
- public health
- health policy
- prevention strategies
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Indigenous Peoples worldwide experience unacceptable health disparities. To improve food and nutrition-related health outcomes for Indigenous Peoples, both targeted (Indigenous-specific) and universal (population-wide) policy action is required.
What are the new findings?
This is the first international review of food and nutrition interventions among colonised Indigenous Peoples in Western nations. The most effective interventions combined strategies to promote food affordability, healthy food and beverage provision, healthy food retail systems and environments; and nutrition knowledge and skills. Targeted approaches were effective when community directed, participatory, multifaceted and culturally relevant. Universal approaches were effective when they addressed the structures and systems in which people access food.
What do the new findings imply?
Targeted approaches should combine strategies to improve food affordability, healthy food environments and nutrition knowledge and skills. The evidence for universal approaches is limited but promising approaches include:
Mandatory rather than voluntary food reformulation targets.
Interpretive food labelling systems applied across all products.
Food pricing policies that both incentivise healthy products and disincentivise unhealthy foods and beverages.
Robust intervention monitoring, evaluation and statistical analysis is required to determine the differential impact of population-wide policy actions on Indigenous Peoples, including in urban areas.
Introduction
The United Nations Declaration on the Rights of Indigenous Peoples affirms their right to the highest attainable standard of health.1 However, many Indigenous Peoples globally continue to experience unacceptable health and social inequities compared with their non-Indigenous counterparts.2 In high-income countries such as Canada, Australia, Aotearoa (New Zealand) and the USA, life expectancy at birth for Indigenous Peoples is 5–10 years lower than for other citizens.2 These inequities reflect the histories of colonisation, dispossession, marginalisation and disruption of cultures and kinship systems.2 3 These histories interact with and are amplified by contemporary socioeconomic disparities as well as interpersonal and institutional racism.3
Indigenous Peoples’ traditional food systems have protected human health and natural environments for millennia. Before their lands were colonised, Indigenous peoples worldwide maintained healthy and sustainable food systems, grounded in transgenerational knowledge of lands, waterways, seasonal food sources, sophisticated agricultural practices and food preparation methods.4 Traditional foods were derived from biodiverse plant and animal sources, high in protein, fibre and micronutrients and low in fat, sugar and salt.5 However, for many Indigenous peoples, food represents more than a source of nutrients; it is intimately connected to land, family, history and culture, as well as to social, emotional and spiritual well-being.5 Consequently, precolonial Indigenous food systems were self-determined, ecologically sustainable and provided healthy, varied diets which protected population health.4
European colonisation has severely disrupted Indigenous food systems in many countries. Dispossession of Indigenous Peoples from their homelands, introduction of industrial food production, processing and distribution has manifested in rapid Westernisation of food environments and dietary patterns.4–6 The transition from traditional to industrialised diets has increased the prevalence of obesity, type 2 diabetes and other diet-related chronic diseases globally, but especially for Indigenous populations.4 For many Indigenous peoples, food security is undermined by environmental degradation, loss of biodiversity and insufficient access to healthy food and other social and economic resources required for health, particularly in rural, remote and Arctic communities.5–8 As a result, nutrition-related health conditions disproportionately affect many Indigenous populations throughout the life course.2 7–9 Despite these inequities, Indigenous Peoples worldwide maintain valuable ecological knowledge and continue to advocate for greater control over their food systems.4 6
Malnutrition, including both undernutrition and obesity, is a leading contributor to the burden of disease worldwide.9 10 Additionally, unsustainable Western food systems are increasingly recognised as a key driver of environmental degradation and climate change.11 In response, the United Nations has declared a Decade of Action on Nutrition and expert panels have called for multilevel, multisectoral policy responses to improve food environments.12 Governments around the world are increasingly implementing food and nutrition policy actions to reduce the impact of the health, environmental and economic burden caused by unhealthy diets.
A range of different food and nutrition policy options exist. These include policies targeting individual behaviour change as well as the systems and environments framing dietary norms.13 14 The NOURISHING framework outlines 10 areas for policy action: nutrition labelling; offering healthy food in specific settings; using economic tools (eg, taxes/subsidies); restricting unhealthy food marketing; improving the quality of the food supply; supply chain interventions; healthier retail environments; information campaigns; nutrition advice and counselling; and giving education/skills.15 Policies may target specific groups (usually of higher risk) or take a universal approach and target whole populations and/or settings (indiscriminate of risk), both of which are necessary to reduce inequities. Targeted policies aim to improve the health of the most disadvantaged groups. Conversely, universal policies act across sociodemographic groups and have potential to improve population health but may be markedly less effective for individuals with limited social and economic resources.13
Indigenous Peoples have the right to be actively involved in policy decisions which affect them, including the development of health priorities and strategies.1 Therefore, Indigenous Peoples should be involved in the determination of policy actions (both targeted and universal) to improve population nutrition. There is an urgent need for evidence-based, equitable public health policies. However, there have been no systematic reviews of the impact of population food and nutrition policies on Indigenous peoples around the world. In this review, we synthesised the evidence on the effectiveness of food and nutrition policy interventions on Indigenous Peoples’ diets and nutrition-related health outcomes.
Methods
This review followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses Equity guidelines,16 and the protocol was registered with PROSPERO (#CDR42019142677).
Search strategy
We searched eight electronic databases for peer-reviewed articles published between January 2000 and December 2019: MEDLINE, Embase, PsycINFO, CINAHL, Informit, Scopus, Global Health and Econlit. The International Journal of Indigenous Health, the Journal of Indigenous Wellbeing, the Indigenous Policy Journal, the First Peoples’ Child & Family Review and the New Zealand Journal of Indigenous Scholarship were hand-searched for non-indexed articles. We searched for grey literature via Google Scholar (the first 300 hits), the Australian Indigenous HealthInfoNet, the Indigenous Studies Portal, the Indigenous Knowledge Network for Infant, Child and Family Health, the NOURISHING database and national government websites from Australia, Aotearoa/New Zealand, Canada and the USA. We contacted experts in the field of Indigenous health and nutrition research from Australasia and North America for unpublished evaluation reports. Reference lists of identified papers were scanned for additional resources.
We combined four sets of search terms, which described Indigenous populations, food policy interventions, nutrition-related outcomes and evaluation study designs. Where possible, relevant subject headings were included in each database search. Each set of search terms and subject headings was combined with the Boolean operator ‘OR’, then the results of each set were combined with the operator ‘AND’. The MEDLINE search strategy is available in online supplementary file 1.
Supplemental material
Study selection and inclusion criteria
Population—Indigenous peoples of Western colonised countries, including studies targeting only Indigenous participants and studies of mixed populations with analyses stratified by ethnicity.
Intervention—study examined a policy intervention, implemented by government or an organisation (eg, school, store) aimed at improving food consumption or nutrition.
Outcome—quantitative impact/outcome data on behaviour, food/nutrient intake, anthropometry, biochemical indicators or diet-related health outcomes were reported.
Study design—evaluations of intervention impact or effectiveness. Reviews, descriptive studies, protocols, modelling and cost-effectiveness analyses were excluded.
Study screening and selection was undertaken independently by two researchers, at least one of whom was Indigenous. Articles not meeting all of these criteria were excluded. Articles unavailable in English were also excluded. Disagreements regarding study inclusion were resolved through discussion with a third researcher until consensus was reached.
Data extraction and quality assessment
A data extraction template was developed to compare study settings, interventions and evaluation results. Data were extracted from included studies, including publication details, study setting, participant characteristics, intervention type, study design, setting, duration, sample size, intervention strategies, Indigenous involvement in intervention design/implementation and relevant outcomes, including the differential impact between Indigenous and non-Indigenous participants, where applicable. The template was piloted by three reviewers with two studies each. Data extraction was completed for all included studies by two reviewers, at least one of whom was Indigenous. Results were cross-checked and discrepancies were resolved through discussion.
Quality assessment was undertaken using the relevant Joanna Briggs Institute (JBI) critical appraisal tool.17 JBI has separate tools for appraising different study designs. Quality assessment was undertaken independently by two reviewers, and disagreements were resolved through discussion and/or consultation with a third researcher. Studies were classified as high quality if more than 80% of applicable appraisal characteristics were endorsed, moderate quality if 50%–80% of characteristics were met and low quality if less than 50% were achieved.
Data synthesis
A narrative data synthesis was undertaken due to the diverse range of interventions and study designs reviewed. The outcomes reported were heterogeneous, therefore, a meta-analysis was not possible. Instead, included studies were grouped and synthesised according to the relevant policy areas of the NOURISHING framework. Although the NOURISHING framework was not specifically designed for Indigenous contexts, it highlights different categories of population-wide food and nutrition policy action, and thus provided a useful framework for organising the findings of our review.
Patient and public involvement
This review was undertaken by a team of Indigenous and non-Indigenous health researchers and practitioners with expertise in public health, nutrition, Indigenous health and cultural safety. It was part of a larger research project designed in partnership with the Victorian Aboriginal Community Controlled Health Organisation (VACCHO). The findings of this review have been presented to VACCHO staff to inform future research, practice and advocacy.
Results
The literature search identified 5276 records after duplicates were removed. After initial screening, we assessed 158 publications for eligibility. Of these, 78 studies met the inclusion criteria and were included in this review (figure 1).
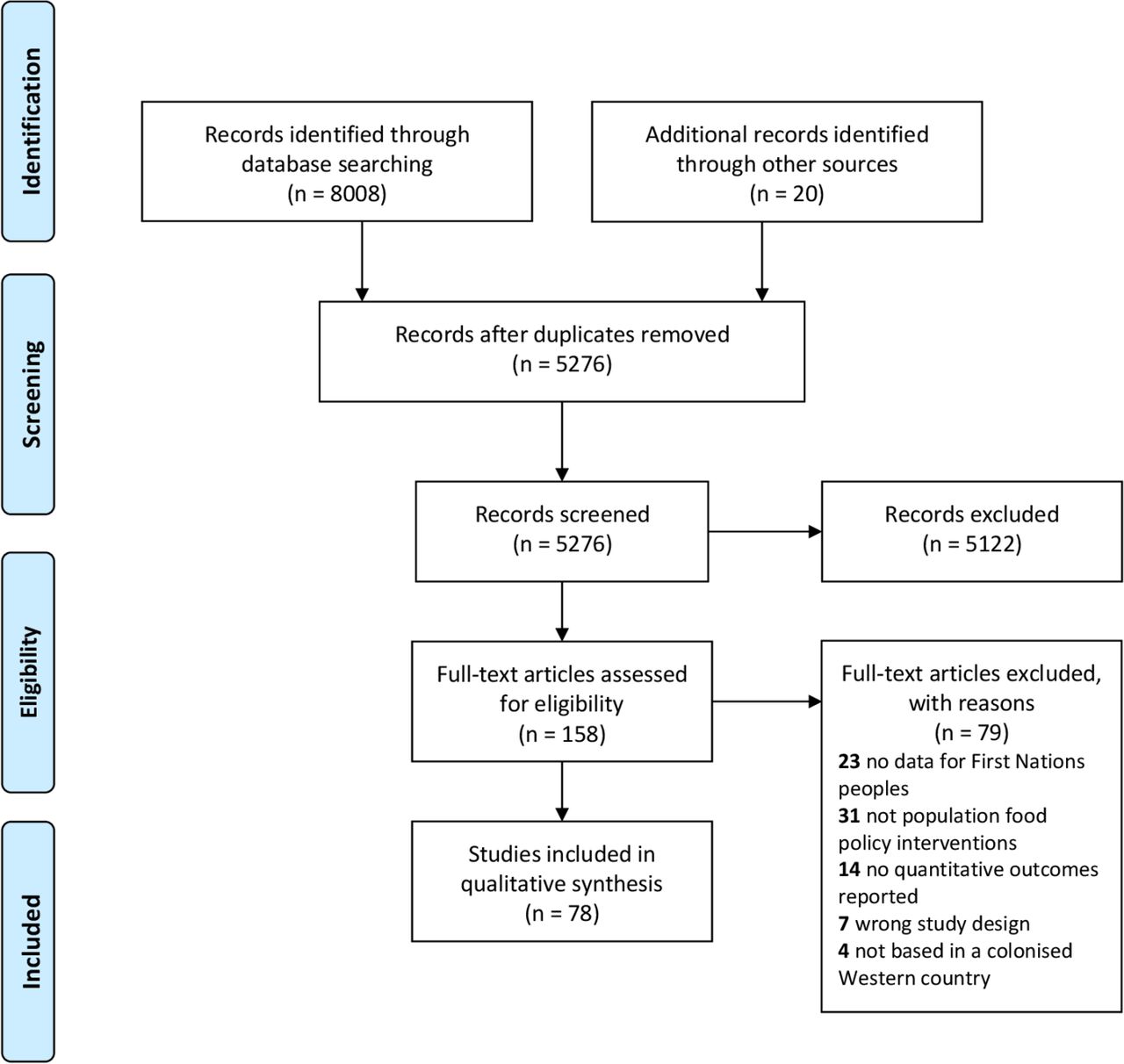
{kind=link}
PRISMA flow chart of included and excluded articles. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
These 78 studies have been summarised in online supplementary table 2 and grouped according to the policy areas of the NOURISHING framework (table 1). There were 5 articles examining food labelling,18–22 21 relating to healthy food provision (predominantly in schools),23–43 10 reporting economic interventions (predominantly subsidies/discounts),44–53 10 evaluating food composition strategies (mainly food fortification),54–63 10 food retail studies,64–73 6 food system/supply chain interventions,54–62 4 information/public awareness campaigns,74–77 4 nutrition counselling/advice evaluations78–81 and 8 education/skill development interventions.82–89 No studies evaluated the impact of unhealthy food marketing restrictions on Indigenous People. This was the only area of the NOURISHING framework not represented in this review.
Supplemental material
Summary of results according to areas of the NOURISHING framework
A diverse range of Indigenous Peoples were described in the literature. This included Aboriginal and Torres Strait Islander Australians; First Nations, Inuit and Inuvialuit Canadians; Native American and Alaskan Native tribes; and Aotearoa Māori. Most articles were from Australia (n=31), followed by Canada (n=22), the USA (n=15) and Aotearoa (n=10). Twenty-three studies included urban Indigenous People, the majority of studies (n=55), however, focused on rural or remote communities.
The review included 13 randomised controlled trials (RCTs), 42 non-randomised, quasi-experimental studies, 11 natural experiments, 11 cross-sectional surveys and 1 case–control study. Seven of the 78 studies were considered high quality. Most (n=42) were assessed as moderate quality and 29 were rated low quality. The quality assessment components most frequently lacking were blinding, a control group, follow-up, reliability of measures and statistical analysis (particularly power calculations to detect an impact in Indigenous populations).
Change in self-reported food or nutrient intake was the most common outcome measure, included in approximately half (n=39) of all studies. A further 17 studies evaluated dietary change via store turnover or sales. Twenty-seven studies included anthropometric outcomes, 16 included biochemical markers and 15 included health outcomes (eg, dental caries, diabetes prevalence, birth outcomes). Five studies evaluated behavioural responses to food labels.
Outcomes according to NOURISHING framework categories
Nutrition labels
Five articles evaluated behavioural responses to food labels.18–22 There were differences between Indigenous (Māori) and non-Indigenous (Pākehā) Peoples of Aotearoa (New Zealand) in the ability to use and interpret the Nutrition Information Panel and industry-led per cent dietary intake labels, with Māori participants less able to use these labels to determine whether a food was healthy. Interpretive labelling systems, such as traffic lights and health stars, were better understood for both Māori and Pākehā groups, although disparities remained.18 One RCT compared the Nutrition Information Panel, Traffic Light and Health Star rating systems among Māori and Pākehā and found no significant differences in food purchases between the labelling groups.22 Interestingly, among frequent label-users, interpretive systems led to more healthy food choices compared with when using the nutrition information panel, a result that did not vary between Māori and Pākehā.22 However, in a second post hoc analysis of the same trial, there was no significant difference (among Māori participants) in the nutritional value between foods/beverages purchased after viewing the interpretive label compared with products whose labels were viewed but not purchased.21 In an Australian study, four years after the front-of-pack Health Star Rating System was implemented, Indigenous participants were significantly more likely than non-Indigenous participants to indicate this labelling system influenced their purchasing decisions.20 The only study to compare generic and culturally tailored food labels found that while both labels significantly increased selection of the healthier food item, the culturally tailored label was more effective than the generic label and significantly increased the price Indigenous shoppers were willing to pay for a healthy item.19
Offer healthy food and set standards in public institutions
Twenty-one articles described the impact of offering healthy food in schools or childcare centres. The majority (n=13) of studies evaluating healthy food provision were undertaken in primary/elementary schools.26–38 Most of these were multicomponent interventions combining healthy food provision within school curriculum or other nutrition education activities. Ten studies measured anthropometric outcomes among Indigenous students, with most finding no significant difference in body mass index (BMI) postintervention,23 25 however, one RCT reported a 10% reduction in the prevalence of overweight among Indigenous children.29 Two studies undertaken in general school populations with mixed ethnicities reported favourable effects on obesity prevalence, including Indigenous children.32 37 Studies evaluating dietary outcomes for Indigenous children frequently reported reductions in consumption of high fat/high sugar foods and beverages,26–29 and/or improvements in food group and nutrient intake.24 39 40 A low-quality evaluation of a fruit provision programme for Indigenous children (n=12) observed improvements in vitamin C status and hearing tests following the intervention.33 34 Positive oral health outcomes were reported for Indigenous children attending childcare centres or schools with ‘water only’ policies.31 37 While another study demonstrated significant reductions in sugar-sweetened beverage consumption and plasma insulin levels among Indigenous high school students following the introduction of a nutrition policy, with insulin levels for males reaching parity with the non-Indigenous comparison group after three years.43
Use economic tools to address food affordability
Eight studies evaluated the impact of subsidising foods and beverages such as fruit, vegetables, bottled water and diet drinks,44–51 predominantly in rural/remote Australia. Findings suggests fruit and vegetable subsidies can improve fruit and vegetable intake48 51 and nutritional status44 45 in rural and remote communities. A high-quality RCT in remote Australian stores, where approximately 95% of the population was Indigenous, demonstrated that a 20% price discount on fruit and vegetables increased purchases by 12.7% during the discount period and by 19.8% after the discount was removed.48 The evidence for price discounts on water and diet drinks was less clear. Most evaluations did not demonstrate significant changes in beverage consumption.48 50 Key factors determining the success of subsidy programmes, according to these studies, were the magnitude and promotion of the discount.49 50 The only study undertaken in an urban (Indigenous and non-Indigenous) population was unable to demonstrate a beneficial effect of price discounts on healthy foods for Indigenous participants, with authors citing that this may have been due to high attrition.47 An adverse outcome observed in some studies of food subsidy programmes was a concurrent increase in overall calories purchased.48 51
Another economic intervention evaluated was compulsory income management. This Australian government intervention, which initially required suspension of the Racial Discrimination Act, quarantined 50% of Indigenous people’s social security payments for essential items including groceries. Two studies independently evaluated the impact of this government policy on store sales52 and birth outcomes.53 Both studies, which received ethical approval, were undertaken after the Racial Discrimination Act had been reinstated. The intervention had no beneficial effect on fruit, vegetable and soft drink purchasing,52 while exposure to the income management policy reduced birth weights by over 100 g and increased the probability of low birth weight by 30%.53
Improving the nutritional quality of the food supply
Nine studies evaluated the impact of food fortification.54–62 Australian evaluations demonstrated that voluntary folic acid fortification failed to improve folate status among Indigenous women and widened the gap in prevalence of neural tube defects (NTD) between Indigenous and non-Indigenous infants.55 56 58 Conversely, mandatory folic acid fortification was associated with significant reductions in folic acid deficiency among Indigenous women and marked reductions in NTD.57 59 62 The most comprehensive study reported a 74% fall in NTD among Indigenous infants following mandatory fortification, almost completely closing the gap between Indigenous and non-Indigenous infants.59 Evaluation of mandatory bread fortification with iodine in Australia and Aotearoa demonstrated improvements in iodine intake60 and urinary iodine concentration61 among Indigenous women; however, pregnant women remained at risk of iodine deficiency.60 61
Food reformulation is another intervention to improve the quality of the food supply. One study evaluated the impact of a 25% salt reduction in a top-selling bread in Indigenous stores in remote Australia.63 The intervention did not affect overall sales but resulted in a reduction in the sodium density of all foods purchased, which reached statistical significance when one control store was removed from the analysis.
Set incentives and rules to create a healthy retail and food service environment
Ten store-based interventions aimed to increase the availability and visibility of healthier options within Indigenous communities.64–73 Many of these also included health information/education activities within the store or in the broader Indigenous community. The Canadian Healthy Foods North study reported improvements in micronutrient intake,64 71 reduced energy intake71 and decreased consumption of targeted high fat and sugar products among Inuit and Inuvialuit communities.69 Other North American studies found more frequent exposure to store-based interventions was associated with increased healthy food acquisition among Indigenous Peoples,65 67 68 while another observed reduced unhealthy food acquisition among Indigenous overweight participants.70 The Australian studies reported a positive impact of store-based interventions on purchasing of fruit and vegetables and reductions in unhealthy foods and beverages, as a proportion of total energy purchased in Indigenous communities.66 73 No studies were able to demonstrate statistically significant changes in BMI,67 68 70 72 however, one observed a downward trend in BMI in favour of the store-based intervention and found higher intervention exposure was associated with significant reductions in BMI and improvements in overweight/obesity among Navajo Indigenous Peoples.67 Furthermore, an Australian study found improvements in biochemical markers of chronic disease risk, despite no changes in obesity prevalence for participants living in remote Indigenous communities.72 73
Harness the food supply chain and action across sectors to ensure coherence with health
Six studies evaluated multisectoral interventions aimed at improving food and/or beverage supply chains.90–95 Evidence from Australian remote Indigenous communities suggests community-driven and multisectoral collaboration to improve local food systems, supply chains and environments, can increase sales of fruit, vegetables and water and reduce sales of confectionary and sugar-sweetened beverages.91 92 94 95 Furthermore, the two North American studies demonstrated harnessing Indigenous and non-Indigenous food systems to deliver healthy food directly to community settings, such as schools or community centres, can increase intake of healthy foods (including traditional foods) and reduce food insecurity among Indigenous Peoples.90 93
Inform people about food and nutrition through public awareness
Providing nutrition information was a component of many interventions included in this review, however, four studies had public awareness campaigns as their primary intervention.74–77 These included community-wide, multicomponent health promotion campaigns, incorporating local media and community education, while encouraging food system/environmental change.75–77 One of these studies in a Māori community in Aotearoa, who were at high risk of diabetes, observed significant reductions in the prevalence of insulin resistance among Māori women75 while others reported improvements in breast feeding and reduced dental caries among Native American infants after a community educational intervention.76 77 Another study compared Indigenous Peoples’ responses to a universal and a culturally adapted and targeted media campaign, suggesting the targeted campaign was more effective than the universal campaign at reducing sugar-sweetened beverage consumption, although the results did not reach statistical significance.74
Nutrition advice and counselling
Four studies evaluated individual nutrition education and counselling services.78–81 Three focused on improving the health of pregnant women and infants through maternal education and counselling during the prenatal/postnatal period.78–80 All studies reported positive results for breast feeding, with the largest improvements from a programme employing Indigenous peer-counsellors to provide targeted breastfeeding advice and support.79 The universal Canadian Prenatal Nutrition Programme was also associated with improved breastfeeding duration and reduced risk of low birth weight among First Nations infants, however, excess weight gain during pregnancy and increased numbers of large for gestational age babies were noted as unintended consequences.80 The other intervention was a universally available telephone lifestyle coaching service that was culturally tailored to increase participation of Australian Indigenous People.81 The evaluation reported significant improvements in self-reported BMI, waist circumference and dietary indicators with no significant differences between improvements made by Indigenous and non-Indigenous participants.81
Give nutrition education and skills
Eight studies evaluated nutrition education programmes.82–89 Most (n=6) were of short duration, had small sample sizes and relied on self-reported dietary outcomes. A high quality evaluation of a school-based peer education programme in which older students mentored younger students about nutrition, physical activity and self-esteem found a reduction in waist circumference among Indigenous children that was almost double that of non-Indigenous children.88 Cultural tailoring of this programme for Indigenous schools resulted in significant reductions in zBMI and waist circumference among participants, while zBMI increased in the control group.87 Other studies reported short-term increases in fruit and vegetable intake among Indigenous children and adults following nutrition education,83 86 however, long-term evaluation of a school-based programme was not able to demonstrate significant improvements in children’s diets.84
Involvement of Indigenous Peoples
Sixty of the 78 publications described the involvement of Indigenous Peoples in intervention design or other cultural considerations in the research (see online supplementary table 2), while 18 studies did not provide any details about Indigenous engagement. Engagement was variously described through gaining permission from local Elders and organisations; involvement in programme initiation, design, implementation, staffing, evaluation; and, in some cases, translation of outcomes.
Discussion
This is the first multicountry systematic review to examine the impact of food and nutrition policy actions on Indigenous Peoples. We found 78 articles, published over the last 20 years in four Western colonised countries. We identified food policy actions across all but one of the areas (marketing) where governments need to take action to promote healthy diets according to the NOURISHING framework. Although the populations included in this review have different lands, ethnicity, culture, language and food practices, they all experience health disparities underpinned by social inequity and the ongoing impact of colonisation. Many of the policy actions included in this review have demonstrated significant improvements in a range of nutrition and health outcomes for Indigenous Peoples; however, many evidence gaps remain.
A salient finding of this review is population-wide policies, including mandatory food fortification, reformulation and interpretive front of pack labelling systems, have the potential to reduce health inequities between Indigenous and non-Indigenous Peoples: when universally applied. This is exemplified by mandatory folic acid fortification in Australia, which almost completely closed the gap in Neural Tube Defects between Indigenous and non-Indigenous infants,59 while voluntary fortification widened this gap.55 56 The studies in our synthesis, including one on sodium reduction,63 suggest policies to improve the nutritional quality of the food supply can be particularly beneficial for Indigenous Peoples; however, these are not consistently applied across countries. Australia, Canada and the USA all have mandatory folic acid fortification policies in place; however, in Aotearoa folic acid fortification remains voluntary. Similarly, Australia, Aotearoa and Canada mandate iodine fortification while the USA does not. None of the countries included in this review have implemented mandatory sodium reduction targets. With respect to sodium restriction, given the lack of food industry action when food reformulation targets are voluntary,96 97 mandatory food reformulation policies have greater potential to reduce health inequities.
We found that interpretive food labelling systems may be more effective at facilitating healthy food purchasing decisions compared with the mandatory nutrition information panel.18 22 While the Health Star Rating front-of-pack interpretive labelling system has been implemented in Australia and Aotearoa, it remains as a voluntary policy. Initial evaluation of this labelling system has yielded promising results for self-reported influence on purchasing decisions among Indigenous Peoples20; however, the study was narrowly focused (two survey questions on perceived influence), limiting the generalisability of the findings. Furthermore, the Health Star Rating system, in its current form, has been criticised for being reductionist and facilitating marketing of processed foods; and is currently under review.98 99 Thus, while our findings support interpretive front-of-pack labels per se, we do not seek to endorse the specific algorithms used for this labelling system.
Previous systematic reviews found school nutrition policies, combined with nutrition education and family engagement, are among the most promising obesity prevention interventions.100 101 Our findings confirm comprehensive school and child-care centre-based policies are also a promising approach for Indigenous children. Many of the studies reviewed reported improvements in nutrition-related outcomes, although methodological quality varied. Three interventions with a focus on reducing sugar-sweetened beverages in children’s settings demonstrated statistically significant improvements in health outcomes for Indigenous children, including dental health25 31 and insulin sensitivity,43 suggesting a pro-equity effect. Although most school-based interventions did not change BMI, those studies that evaluated BMI as an outcome were of relatively short duration. The one long-term evaluation of a population-wide school health promotion programme demonstrated statistically significant improvements in childhood obesity rates across Indigenous and non-Indigenous groups.37
Food retail and supply chain interventions to improve local food and beverage environments in rural and remote Indigenous communities were consistently effective across included studies. Consistent with the results of a recent review of retail food environment interventions,102 all studies targeting local food retail and supply chains within Indigenous communities were able to demonstrate improvements in at least one outcome including dietary quality, healthy food purchasing, food security, nutrition or chronic disease biomarkers, and one reported a downward trend in mean BMI.67
Furthermore, the use of store sales data to evaluate the impact of remote Indigenous community store interventions in Australia provided objective evidence for multi-sectoral food system interventions to increase purchasing of fruits and vegetables, and decrease purchasing of confectionary and sugar-sweetened beverages.66 91 92 94 Critically, all of these studies reported strong Indigenous involvement and ownership of local Indigenous communities in intervention development, implementation and/or evaluation. Conversely, interventions targeting Indigenous Peoples implemented without Indigenous leadership or consultation, such as income management, do not improve nutrition outcomes and may be harmful.52 53 It remains unclear as to whether the positive findings from remote communities can be translated to Indigenous Peoples living in urban areas. The only store-based intervention undertaken in urban and regional areas was not sufficiently powered to detect geographical subgroup differences.47
Food and beverage pricing policies are frequently proposed as an effective strategy to improve population diets and health equity.103–106 Our review indicates subsidies/price discounts, when of sufficient magnitude and adequately promoted, can be effective at improving fruit and vegetable consumption,48 51 nutritional status and children’s health outcomes44–46 in Aboriginal communities in rural and remote Australia. However, concurrent strategies are required to prevent the concomitant increase in purchasing of energy-dense foods and beverages observed in these studies.48 51 93 Further, while the evidence was strong for targeted fruit and vegetable subsidies, we did not identify any studies examining the impact of universal food or beverage taxes on Indigenous Peoples’ food purchases, health or well-being. Evaluation of the sugar-sweetened beverage tax in Mexico revealed reductions in sugar-sweetened beverage purchasing were greatest among lower socioeconomic households,107 108 but the impact on the Indigenous Peoples of Mexico has not been analysed. Policies that increase the price of sugar sweetened beverages are in place in some Indigenous community stores in remote Australia109 and the Navajo Nation (Native American territory) has introduced a 2% tax on unhealthy foods and beverages and removed a 5% sales tax on fruit, vegetables and water.110 It will be important to evaluate these policies for their impact on Indigenous Peoples.
There is convincing evidence that exposure to unhealthy food advertising influences children’s food intake.111 112 Mandatory restrictions on marketing of unhealthy foods and beverages are likely to be effective across socioeconomic groups.113 114 However, we found no evaluations of the impact of food advertising restrictions on Indigenous Peoples. This is particularly concerning as it has been estimated that Canadian First Nations children are exposed to one food advertisement every 5 min.28 Furthermore, there is evidence from Aotearoa suggesting Māori children have higher rates of exposure to food, alcohol and gambling marketing compared with non-Māori children.115–117 Policy action and evaluation in this area is another evidence gap that needs to be closed.
Public information campaigns, lifestyle advice and nutrition education are often not the preferred strategy of public health advocates as they target individual behaviour change rather than the structural determinants of food choice.13 118 The evidence in this review indicates a place for educational interventions, especially when implemented concurrently with approaches targeting food systems and environments. The best results were from studies of community-wide, culturally relevant nutrition information and education programmes with multiple components, which showed improvements in insulin sensitivity, BMI and dental health.75–77 81 87 88 One-to-one nutrition education and counselling, especially using an Indigenous peer education approach, effectively improved breastfeeding rates, BMI and waist circumference.79 87 88 Previous reviews have also found community nutrition education and health promotion campaigns can be effective when implemented alongside changes to the food environment and with high levels of community involvement.14 119–121
Most studies included in this review were of moderate methodological quality, with only 7 out of 78 were assessed as high quality. Although the JBI quality assessment tools were useful as they allowed different study designs, they are intended for clinically-based studies rather than complex population-based or ‘real-world’ interventions. The appropriateness of quality appraisal tools for multicomponent public health interventions is frequently questioned.120 122 Furthermore, the aspects of ‘quality’ included in existing tools are constructed through a Western ontological lens and are likely entirely different from what is considered high quality research from Indigenous Peoples’ perspectives.123
Many of the studies in this review reported the ways in which researchers engaged with Indigenous communities in intervention design and evaluation. Indigenous leadership; community engagement and involvement; participatory approaches; trust and relationships; incorporation of cultural knowledge; culturally safe approaches and translation of findings and benefits back to participating communities are among the features consistently identified as critical to the success of health promotion and public health research in Indigenous communities.124 125 However, despite the increasing volume of research conducted in the food and nutrition policy field (one-third of all studies were published in the last four years), there still exists no universally accepted tool for appraising public health and health promotion interventions for Indigenous Peoples. Indigenous Peoples have a long history of critiquing health research and several Indigenous-led research groups have piloted tools for appraising health promotion research in Indigenous contexts.123 126 There is clearly the need for further rigorous evaluation research into food and nutrition interventions in Indigenous populations, including the differential impact of population-wide policy actions. However, equally important is the development of research protocols and quality assessment tools that value both Indigenous and Western ways of knowing.
Strengths and limitations
This review makes an important contribution to the evidence for both population-wide and Indigenous-specific food and nutrition policy action. It included an extensive search strategy, incorporating international peer-reviewed and grey literature and broad inclusion criteria to ensure a diverse range of Indigenous populations, policy actions, outcomes and study designs. A further strength of this review is the inclusion of Indigenous researchers on the review team who were involved in every step of the process including protocol design, study screening, data extraction and quality assessment.
We also note some limitations. Like all systematic reviews, our synthesis may be limited by publication bias as unsuccessful interventions are less likely to appear in the literature. We attempted to reduce this risk by including grey literature and contacting experts in the field for unpublished reports. Our review only included studies published in English from Western colonised countries, thus policies implemented in Indigenous populations in non-English-speaking, low-income and middle-income countries have not been included. It is possible this systematically excluded potentially relevant studies from Latin America, a region with increasing implementation of regulatory food and nutrition policies.127 However, within the four countries included in the current review, the great diversity of the Indigenous populations represented means that generalisability is not possible. Furthermore, Indigenous peoples worldwide represent a much broader range of nations, language groups, cultures, gender identities and food system contexts than the populations included in this review. There is a need for further research to capture the full range of Indigenous experiences. Despite these limitations, we draw some high-level conclusions and implications for policy and practice.
Conclusion
Our findings suggest that to improve nutrition-related health outcomes for Indigenous Peoples, both targeted and universal policy actions are required. Targeted approaches should be community-directed, participatory, culturally relevant, multifaceted interventions combining strategies to improve food affordability, healthy food environments and nutrition knowledge and skills. To promote equity, universal approaches should change the structures and systems in which populations access food, which for Indigenous Peoples, have been severely disrupted by colonisation. Promising approaches include food pricing policies that incentivise healthy products and disincentive unhealthy products; mandatory rather than voluntary food reformulation targets and interpretive food labelling systems; and restrictions on junk food marketing to children, however, further research is required to confirm this. Rigorous designs with sufficient statistical power, careful monitoring and evaluation are required to determine the differential impact of population-wide policy actions on Indigenous Peoples, particularly in urban areas.
Acknowledgments
We respectfully acknowledge the Indigenous Peoples in the articles included in this review: Aboriginal and Torres Strait Islander (Australia), Māori (Aotearoa/New Zealand), First Nations, Inuit and Inuvialuit (Canada) and American Indian and Alaskan Native Peoples. This research took place on the lands of the Wurundjeri, Wathaurong, Yorta Yorta and Awabakal Peoples of Australia. ML is a Ngiyampaa man, TW is a Yorta Yorta man and ME is a Gunditjmara/Mutti Mutti woman.
References
Footnotes
Handling editor Stephanie M Topp
Contributors JB conceptualised the study and developed the protocol in consultation with KB and ME. JB, ML and TW screened and selected the studies, extracted and analysed data. JB drafted the initial manuscript, TW, ML, KB and ME provided feedback on initial drafts and further revised the manuscript. All authors read and approved the final manuscript.
Funding JB is supported by an Alfred Deakin Postdoctoral Research Fellowship. KB is supported by a Heart Foundation Future Leader Fellowship (102047). This study was funded by the Victorian Health Promotion Foundation (VicHealth).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplementary information. Details of included studies are included in online supplementary file 2.