Article Text

Abstract
Introduction Prolonged obstructed labour often results from lack of access to timely obstetrical care and affects millions of women. Current burden of disease estimates do not include all the physical and psychosocial sequelae from prolonged obstructed labour. This study aimed to estimate the prevalence of the full spectrum of maternal and newborn comorbidities, and create a more comprehensive burden of disease model.
Methods This is a cross-sectional survey of clinicians and epidemiological modelling of the burden of disease. A survey to estimate prevalence of prolonged obstructed labour comorbidities was developed for prevalence estimates of 27 comorbidities across seven categories associated with prolonged obstructed labour. The survey was electronically distributed to clinicians caring for women who have suffered from prolonged obstructed labour in Asia and Africa. Prevalence estimates of the sequelae were used to calculate years lost to disability for reproductive age women (15 to 49 years) in 54 low- and middle-income countries that report any prevalence of obstetric fistula.
Results Prevalence estimates were obtained from 132 participants. The median prevalence of reported sequelae within each category were: fistula (6.67% to 23.98%), pelvic floor (6.53% to 8.60%), genitourinary (5.74% to 9.57%), musculoskeletal (6.04% to 11.28%), infectious/inflammatory (5.33% to 9.62%), psychological (7.25% to 24.10%), neonatal (13.63% to 66.41%) and social (38.54% to 59.88%). The expanded methodology calculated a burden of morbidity associated with prolonged obstructed labour among women of reproductive age (15 to 49 years old) in 2017 that is 38% more than the previous estimates.
Conclusions This analysis provides estimates on the prevalence of physical and psychosocial consequences of prolonged obstructed labour. Our study suggests that the burden of disease resulting from prolonged obstructed labour is currently underestimated. Notably, women who suffer from prolonged obstructed labour have a high prevalence of psychosocial sequelae but these are often not included in burden of disease estimates. In addition to preventative and public health measures, high quality surgical and anaesthesia care are urgently needed to prevent prolonged obstructed labour and its sequelae.
- maternal health
- obstetrics
- surgery
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Prolonged obstructed labour often results from lack of timely access to obstetrical care, particularly caesarean sections.
Prolonged obstructed labour results in significant mortality and morbidity in women, particularly fistula.
What are the new findings?
Women who suffered from prolonged obstructed labour have a high prevalence of a wide range of physical and psychosocial sequelae.
The burden of disease resulting from prolonged obstructed labour is 38% more than previous estimates.
What do the new findings imply?
The current burden of disease associated with prolonged obstructed labour likely remains an underestimate of disability, particularly related to psychosocial sequelae.
High quality surgical and anaesthesia care are urgently needed to prevent prolonged obstructed labour and its sequelae
Introduction
Obstructed labour (OL) occurs when fetal descent is blocked by an insurmountable barrier despite forceful uterine contractions, requiring early and appropriate treatment.1 Advances in obstetrical care have eradicated most complications of OL in high-income countries through access to timely and safe caesarean section (CS) and instrumental delivery.2–4 Analyses have consistently demonstrated the cost-effectiveness of these interventions, even in resource-limited settings.5–8 However, in areas where women’s need for comprehensive obstetrical care has been neglected, the result is prolonged obstructed labour (POL). While there is a lack of consensus on the definition of prolonged labour generally, and POL specifically,9 10 there is global recognition of the impact of POL on maternal and newborn health, predominantly in sub-Saharan Africa and Asia.11 12
The lack of access to appropriate care, including surgical care, among women with POL has resulted in this condition accounting for 2.1% to 12% of maternal mortality,13 and for 29% to 44% of stillbirths.14 15 Even when deaths are prevented, mothers and infants may suffer from one or more lifelong disabilities. For infants, intrapartum asphyxia may cause neurological damage and developmental issues.16 17 Women contend with a varied array of physical and psychosocial sequelae that are originally referred as the OL injury complex: fistula between the urinary and gastrointestinal and genital tracts, urinary and faecal incontinence, vaginal fibrosis, cervical and vaginal stenosis, infertility, dyspareunia, sepsis, diastasis pubis, osteomyelitis, foot drop and chronic pelvic pain.18–20 POL-related mental health issues include depression and anxiety and social consequences such as experiencing stigma, divorce, abandonment, income loss and property loss; however, much of the literature documenting these issues comes from investigations of the experiences of women with fistula.18 19 21 22 Despite the broad range of sequelae, health programmes and research around treatment of POL have predominantly focussed on fistula repair alone.23 24
Current epidemiological analyses of the impact of POL have a limited scope. The Global Burden of Diseases, Injury and Risk Factors Study 2017 (GBD) to estimate the burden of disease (BOD) resulting from OL and uterine rupture, only takes into account maternal mortality, rectovaginal fistula (inclusive of faecal incontinence) and vesicovaginal fistula (inclusive of depression and urinary incontinence).25 This narrow focus fails to include many sequelae and underestimates the true impact of POL.
The objective of this study was to estimate the BOD associate with POL by surveying health practitioners to estimate the prevalence of the full spectrum of POL sequelae. These estimates were used to inform a BOD model with a more comprehensive set of sequelae than is currently reported by the 2017 GBD.
Methods
Study population
Inclusion criteria for survey participation were health practitioners from any field, working for at least 6 months in centres where women with POL are treated in Asia and Africa. The survey was distributed in English and limited to those with an understanding of written English. Given the near-complete absence of POL in health systems that provide timely access to safe CS, non-zero fistula estimates are only provided for 54 countries in the GBD study and our analysis is limited to these same countries.
Survey development and distribution
A literature search to identify existing validated questionnaires was conducted but none were found that comprehensively assessed physical and psychosocial sequelae from POL. We developed a survey questionnaire after an extensive literature review of the sequelae of POL followed by expert consensus of a multidisciplinary team of fistula surgeons, researchers and clinicians. Careful designing of the survey questionnaire took into consideration wording, form and order of the questions. In total, 27 unique sequelae previously associated with POL were chosen and grouped into eight different categories. The survey questionnaire included questions on demographics, practice type, practice location and prevalence estimates of the 27 sequelae for all women who experience POL (online supplementary appendix S1). Recognising the lack of a global consensus definition of POL, we did not provide a specific definition to respondents. Three of the survey questions addressed fistula while the remainder inquired about pelvic floor disorders, sexual and reproductive health, musculoskeletal issues, infectious diseases, mental health, neonatal outcomes and social impact.
Supplemental material
The questionnaire was distributed via email as an anonymous multiple-choice survey in November and December of 2018. Global networks of fistula care providers were approached to send the survey to their members. The target population was clinicians that work with patients who suffered POL. Snowball sampling was used to allow for further subject recruitment. Reminder emails were sent at 2-week intervals for 6 weeks following the original invitation to participate. Data were collected and managed using a REDCap (Research Electronic Data Capture) tool.26
Statistical analysis
Measures of central tendency (mean and median) and variance (SD and IQR) were calculated using frequency tables and formulae for grouped data. Inter-rater reliability was analysed using Kendall’s coefficient of concordance for ordinal data, with correction for ties. Landis and Koch criteria were then applied to the reliability estimate. Data analysis was performed using the R programming language through RStudio V.1.1.453.27 28
Estimating years lived with disability
To estimate years lived with disability (YLDs) for a more comprehensive set of morbidities than is currently reported by the 2017 GBD, we began by identifying which sequelae from our survey to include in an augmented YLD model. Given the desire to replicate GBD methodology for constructing YLDs to the degree feasible given our data, we began by associating each sequela with its assigned GBD disability; sequelae without disability weights were excluded from this analysis (eg, social impact due to loss of partnership or income). The final list of sequelae must account for comorbidities and be mutually exclusive and collectively exhaustive. Comorbidity sets are created by listing all possible permutations of individual sequela. Thus, the final list (box 1) of comorbidity sets avoids pairing sequelae that are inclusive of other sequelae (urinary incontinence and depression can be secondary to fistula and are both included as a factor in the fistula disability weights; urinary incontinence can be due to prolapse as well). We distinguish between acute sequelae (including the pain due to POL and sepsis) and chronic sequelae (which we further divide into chronic sequelae with fistula and chronic sequelae without fistula).
Prolonged obstructed labour comorbidity sets sequelae
Acute complications
Acute event without sepsis.
Acute event with sepsis.
Chronic complications with fistula (includes depression and incontinence)
Fistula with infertility, foot drop or chronic pelvic pain.
Fistula with infertility, without foot drop or chronic pelvic pain.
Fistula with infertility and foot drop, without chronic pelvic pain.
Fistula with infertility, foot drop and chronic pelvic pain.
Fistula without infertility, foot drop or chronic pelvic pain.
Fistula without infertility, with foot drop and chronic pelvic pain.
Fistula without infertility or foot drop, with chronic pelvic pain.
Fistula without infertility, with foot drop, and without chronic pelvic pain.
Chronic complications without fistula
Asymptomatic (no incontinence, infertility, foot drop or chronic pelvic pain).
With incontinence, infertility, foot drop and chronic pelvic pain.
With incontinence, without infertility, foot drop or chronic pelvic pain.
With incontinence and infertility, without foot drop or chronic pelvic pain.
Without incontinence, with infertility, foot drop and chronic pelvic pain.
Without incontinence and infertility, with foot drop and chronic pelvic pain.
Without incontinence, infertility and foot drop, with chronic pelvic pain.
With incontinence, without infertility, with foot drop and chronic pelvic pain.
With incontinence, without infertility or foot drop, with chronic pelvic pain.
With incontinence and infertility, without foot drop, with chronic pelvic pain.
With incontinence, without infertility, with foot drop, without chronic pelvic pain.
Without incontinence, with infertility, without foot drop and chronic pelvic pain.
Without incontinence, with infertility and foot drop, without chronic pelvic pain.
Without incontinence, with infertility, without foot drop, with chronic pelvic pain.
Without incontinence and infertility, with foot drop, without chronic pelvic pain.
Without incontinence, infertility and foot drop, with chronic pelvic pain.
When deriving disability weights (DW) for each set of comorbidities (c), we align with GBD methodology by calculating the multiplicative sum of the individual sequelae’s (s) disability weights, which is then subtracted from one:25

The next step was to derive an estimate of the incidence (I) of prolonged obstructed labour (Ipol) by country for ages 15 to 49. Age-specific and country-specific incidence and prevalence rate estimates are provided for OL by GBD, but these estimates include cases that receive appropriate treatment with CS. The GBD study also provides age-specific and country-specific incidence and prevalence estimates for obstetric fistula. Given that our survey (q) asked participants to estimate the proportion (prop) of POL cases that will develop obstetric fistula (f), we can use the following relationship to derive Ipol from GBD (g) and our survey data:

Equation two can be re-arranged as follows and solved for each country (l):

We then calculated the probability (prob) that each set of comorbidities (Probc) from box 1 will result from one case of POL, which we based on the median proportion estimate for each sequela for our baseline results. As with GBD, we assume that sequela events are independent. The country-specific incidence of each comorbidity set (Ic,l) in 2017 can then be estimated by multiplying Ipol,l and Probc.
The GBD study uses a prevalence-based approach for calculating YLDs. Thus, the basic equation for calculating YLDs in 1 year is:

where p=prevalence. Therefore, to be able to compare our estimates of YLDs with GBD estimates, we need to estimate the prevalence of each comorbidity set (Pc). To accomplish this, we take advantage of the relationship of incidence rate, prevalence and average duration (D) for diseases by assuming a population in steady-state population:

We conservatively assume that the average duration for chronic sequelae is equal to average duration of fistula (country-specific, derived from GBD results) for our baseline results. The duration for sepsis and obstructed labour events are taken directly from GBD 2017. Therefore:

and YLDs for POL in each country is given by:

For each country we estimated total number of YLDs and YLDs per 100 000 women of reproductive age (15 to 49 years old). We perform a simple two-way sensitivity analysis by varying duration of disease (D) for chronic sequelae and the proportion of POL cases that develop a sequela (mean vs median survey result) (online supplementary appendix S2). In this publication we report using median prevalence estimates from the clinician survey and a duration for chronic sequelae equal to that of the duration of fistula in each country as determined by GBD.
Ethics approval
The protocol was developed adhering to appropriate ethical principles to conduct global health research. The survey questionnaire solicited clinical opinion anonymously from key professional respondents. Therefore, on review of the initial study submission, Harvard Medical School Human Research Protection Program exempted the study from further Institutional Review Board review.
Patient and public involvement
Patients were not involved in the research design.
Results
Survey respondent demographics
Survey responses were obtained from 132 participants, and two incomplete responses were excluded for a total sample size of 130. Since snowball sampling was used, it is not possible to estimate a survey response rate. Most responders have been providing clinical care for over 10 years (72.7%) and work primarily in sub-Saharan Africa (83.1%). The participants provide a wide range of services to patients with POL with the most common scope of practice being general obstetrics (75.2%), gynaecology (73.6%) and fistula care (69.8%) (table 1).
Survey respondents characteristics
Prevalence of comorbidities
Estimates for 27 sequelae from POL were obtained (table 2). The most common sequelae were in the social category with inability to maintain income (59.88%, IQR=59.73) and dissolution of partnership or marriage (45.63%, IQR=54.33) being the most prevalent conditions. Inter-rater reliability was determined to be ‘fair’ according to Landis and Koch criteria with a Kendall’s W of 0.38 among all prevalence responses. Inter-rater reliability among the sequelae that were chosen for inclusion in the BOD model had a Kendall’s W of 0.51, a ‘good’ level of reliability according to Landis and Koch criteria.
Estimates of select comorbidities of prolonged obstructed labour
Years lost to disability
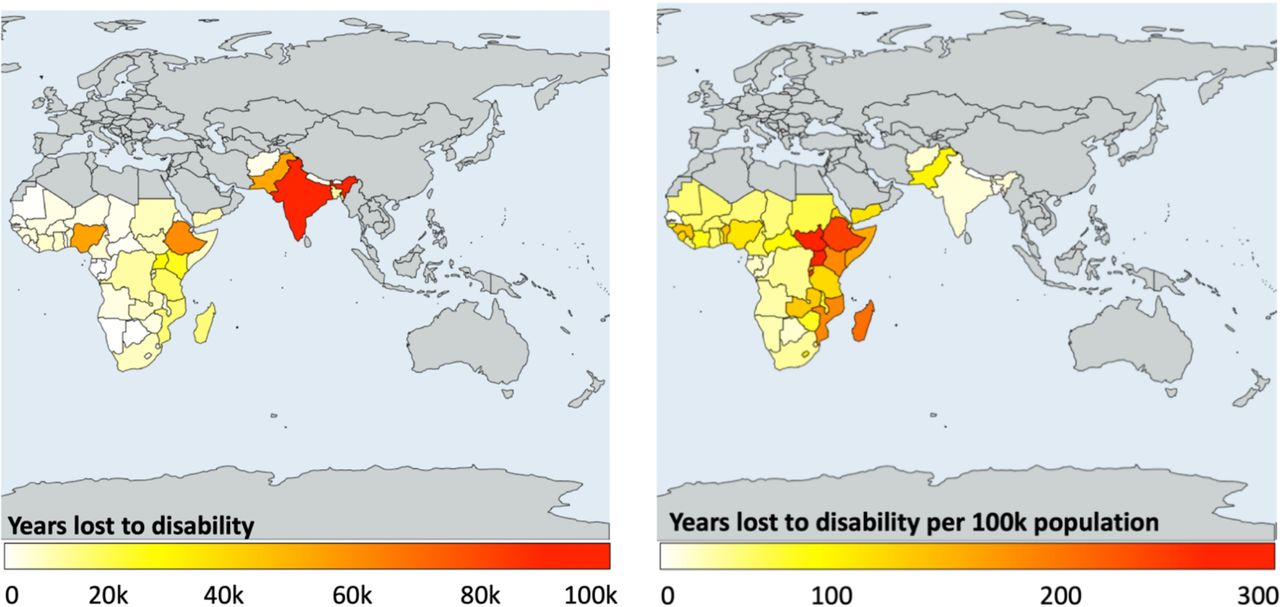
Using a comprehensive set of comorbidities, we estimated that during 2017 in 54 countries, the sequelae of POL resulted in a total of 485, 154.87 YLD, which is 37.9% more than the estimate using the GBD model. This estimate is 38% more than the previous GBD estimate. India has the largest absolute number of YLD, accounting for 21.1% of the global YLDs due to POL. When adjusting the total YLD by the population of women of reproductive age (15 to 49 years old), the country with the highest BOD per capita was South Sudan with 297.05 YLD per 100,000, which is 40.2% more than previously estimated. In Asia, Yemen has the highest per capita BOD with 108.18 YLD per 100 000. Nepal (17.55 YLD/100 000) and Senegal (19.32 YLD/100 000) have the lowest per capita BOD in Asia and Africa, respectively. Geographical variations of absolute YLDs and YLDs per 100 000 women are shown in figure 1. Burden of disease due to YLD for individual countries comparing the GBD model estimates and the estimates with the updated model with more comprehensive sequelae are on table 3.

{kind=link}
Geographical distribution of the total YLD and YLD per 100 000 women of reproductive age in 2017. YLD,years lived with disability.
Comparison of burden of disease (BOD) estimates by the Global Burden of Disease (GBD) study and our new model with a more comprehensive inclusion of sequela
Discussion
Main findings
Our study estimates the global prevalence of a comprehensive set of sequelae associated with POL, providing a more representative estimate of the burden of disease. The survey results suggest that the most prevalent sequelae is urinary tract fistula, affecting approximately 24% (IQR=54.8) of women. Obstetric fistula is often considered as the most devastating consequence of POL, and women often also suffer from incontinence (8.6%, IQR=15) and/or prolapse (6.5%, IQR=5.4). Our results suggest that 66.4% (IQR=69.7) of women with POL have a stillbirth and 13.6% (IQR=13.6) have an infant suffering sequelae of intrapartum hypoxia. Psychological and social sequelae were estimated to have a higher prevalence than most physical sequelae with grieving for stillborn, anxiety or depression symptoms estimated to be prevalent in approximately one-quarter of women. The most common social sequelae is loss of income, affecting approximately 59.9% (IQR=59.7) of women, followed by stigma in 43.6% (IQR=58.7) of patients. The estimates obtained for acute sequela such as fistula and sepsis and chronic sequelae such as incontinence, infertility, chronic pelvic pain and foot drop, were used to determine that the current estimates of the GBD study underestimate the disability from POL by at least 38%. Since we followed the GBD study methodology we were restricted on the sequela from POL that we could include, and this remains a conservative estimate.
Interpretation
Our survey results are consistent with literature estimates on the sequelae experienced by women with POL. For example, the percentage of stillbirths has been estimated to be 78% to 96% in women who develop obstetric fistula.29 30 The economic impact of POL disproportionately affects poor women who cannot access timely emergency obstetrical care, including caesarean delivery, for whom such services are too costly. POL sequelae further reduce income-earning activities, compounded by high out-of-pocket expenses that prevent access to fistula care.31–33 Consistent with our results, a longitudinal obstetric fistula study has shown that POL survivors’ psychosocial health and quality of life are greatly affected by high prevalence of stigma, disruption of social relations and depression symptoms.19 Evidence suggests that treatment of physical symptoms results in significant improvement of psychological health, but targeted reintegration services and psychosocial support is needed to support women after POL regardless of their physical comorbidities. It should be noted that much of this literature focusses on women with fistula, with limited exploration of the consequences to women who have experienced other sequelae of POL.
The significant detrimental impact of POL sequelae such as fistula, incontinence and psychosocial sequelae have been captured in qualitative studies.34 35 However, quantifying the disability experienced by these women remains a challenge. Global progress in maternal health has traditionally relied on maternal and neonatal mortality as metrics to track progress36–38 However, as mortality decreases, an increased focus on near-miss events, maternal severity index and preventable morbidity has emerged.39 Similarly, the estimates for the global burden of disease of POL, characterised in disability-adjusted life years, are evolving from being driven by years of life lost when women would often not survive complications of pregnancy, to being driven by YLD as more women survive POL and live with chronic disability.25 Measuring health loss from disability is complex, reflecting persistent failure to provide timely access to caesarean section to avert POL, as well as illustrating a failure to address all sequelae of POL.
Research, programmatic, funding and policy recommendations
Most of the outcome data on interventions to address POL sequelae focus on obstetric fistula and are sparse in elucidating other comorbidities and alleviation of barriers to timely care.40 Advancing research on the prevalence, management and outcomes of these sequelae in a similar fashion in which fistula repair has been studied could improve service delivery to these patients. POL is a rare event that is challenging to measure and as a result some countries have started including fistula indicators as part of their national health information systems or collecting data as part of their Demographic Health Survey.41 Developing health utility values for psychosocial factors would allow for inclusion of more sequelae, that are known to have a high prevalence, to be included in the estimates of BOD for POL. Robust data collection and research around POL will be necessary to strengthen service delivery and policy development.
Comprehensive clinical and public health programmes that address physical sequelae beyond fistula to include physical comorbidities, psychosocial sequelae, educational and vocational training for reintegration back into society and developmental screening for surviving infants are essential to holistically address the disability from POL. At the community level, education programmes on POL could decrease stigma and promote care seeking behaviour to prevent POL and to treat the entire maternal and newborn spectrum of sequelae from it. Despite an increase in antenatal care and institutional deliveries, access to timely high-quality obstetric surgical care remains challenging. As a result, even when women access healthcare facilities when in labour, lack of surgical capacity and quality results in preventable POL. For example, a study in Uganda showed that 50.9% of women acquired obstetric fistula in their first delivery despite 94.3% having received antenatal care.42 Furthermore, rises in iatrogenic fistula have been reported, therefore as surgical capacity is scaled up, a concurrent investment on quality of care is essential to prevent inflicting harm on women43
Treatment of obstetric fistula has received significant attention by the global community including the United Nations Population Fund’s (UNFPA) Campaign to End Fistula in 2003 and the United Nations Secretary-General 2018 call to action to end obstetric fistula by 2030.44 45 Despite large amounts of funding and programming for fistula treatment, many of the other comorbidities resulting from POL have been neglected. This illustrates how global funding efforts, guided by vertical interventions, may be poorly aligned with actual BOD.46 A more comprehensive understanding of the BOD associated with POL, as outlined by our results, could guide programmatic and funding allocation by informing policymakers, donors and other global stakeholders on the need to invest in comprehensive health services.
Several countries have national obstetric fistula policies that are undermined by gaps in programming and poor alignment with existing health and human rights policies.47 Most of these national fistula strategies are designed for fistula treatment without an equally effective strategy for POL prevention or treatment via safe and comprehensive emergency obstetric care, undermining the goal of a ‘fistula-free generation’.47 We recommend POL strategies that are well-integrated within national health strategies for maternal and surgical care to ensure funding, implementation and coordination with other services. Preventing and addressing the BOD elucidated by our study support the sustainable development goals-era mandate to end not only fistula, but preventable childbirth-related morbidity and mortality.44 48 49 While the public health approach to eradicate POL must include initiatives to delay the age of marriage, improve girls’ and women’s nutrition, assure girls’ education, reliable provision of family planning services, support for women’s economic empowerment and other gender-based transformations, all such efforts will not have their full desired impacts without concurrent strengthening of access to timely, affordable and high-quality obstetric interventions that include indicated, safe surgical care.48
Strengths and limitations
We obtained prevalence estimates from a multidisciplinary group of participants, working mostly in sub-Saharan Africa and South Asia, with extensive experience working with women affected by POL. As a result, we expect their assessments to provide an accurate estimate of patients’ sequelae. Although a multidisciplinary sample was targeted, the use of global networks of fistula care resulted in the majority of participants being surgical providers. Larger participation of other professions such as community health workers and midwives, may have revealed different results. Our results remain practitioner estimates, and facility level outcomes and patient-reported outcomes would further strengthen our results. Furthermore, this approach excludes the women who are not accessing health facilities. Future validation of the survey will be required to strengthen morbidity estimates of POL. The survey was distributed in English as most clinicians have higher education and speak the language due to the global nature of fistula provider networks. However, it is likely that English-speaking clinicians are more likely to work at large, regional centres while most women who suffer from POL are in more remote areas, therefore impacting our results. Estimation of the BOD due to POL was structured to match the Institute for Health Metrics and Evaluation robust GBD methodology, enabling meaningful comparisons to prior estimates. However, the list of sequelae included in the new BOD model was limited to those for which a disability weight exists, which restricted the inclusion of many comorbidities into the model, particularly psychosocial sequelae. All these limitations suggest that, despite providing a more comprehensive BOD model, our analysis still underestimates the true disability experienced by women and newborns as a result of POL.
Conclusion
POL is preventable, and when untreated, results in a wide range of debilitating physical and psychosocial sequelae. We estimated a more comprehensive BOD resulting from POL to better guide research and policy, but this likely remains an underestimate of disabilities women face, particularly from psychosocial sequelae. High-quality surgical and anaesthesia care are urgently needed as part of an essential component of maternal health systems. This will both prevent POL and treat all of the needs of the mothers and newborns who have survived POL, far too often into a lifetime of tragic suffering caused by preventable disability.
Acknowledgments
The authors thank Mary Ellen Stanton and Erin Mielke of USAID for their review of this manuscript.
References
Footnotes
LR and BCA are joint senior authors.
Handling editor Sanni Yaya
Twitter @LinaRoaS
Contributors LR, LC and BCA conceived the study. LR, GG, VT and LR developed the survey. LC, NH and GG collected data. LR, LC and BCA conducted the analysis. LR and BCA drafted the manuscript. All authors made significant contributions to the manuscript and meet authorship criteria.
Funding Lina Roa received support from the Ronda Stryker and William Johnston Global Surgery Fellowship Fund. This study was partly supported by the American people through the United States Agency for International Development (USAID) associate cooperative agreement AID-OAA-A14-00013. The opinions expressed are those of the authors and do not necessarily reflect the views of USAID or the United States Government.
Disclaimer Blake Alkire reports grants from Mercy Ships. No other disclosures were reported.
Competing interests BCA reports grants from Mercy Ships, these did not influence the submitted work.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data from the survey results are available upon request. Data used for burden of disease modelling is available at the Global Burden of Disease Study website from the Institute for Health Metrics and Evaluation and is available open access.