Article Text

Abstract
Background Risks for condomless sex among transgender women and cisgender men who have sex with men (trans-WSM and cis-MSM, respectively) in the Philippines, where HIV recently became a national public health crisis, are shaped and exacerbated by various risk factors across multiple levels.
Methods Between June 2018 and August 2019, we conducted a cross-sectional online study with 318 trans-WSM and cis-MSM respondents from Manila and Cebu cities. Structural equational modelling procedures were performed to determine direct, indirect and overall effects between condom use and latent variables across multiple socioecological levels: personal (ie, condom self-efficacy), social (ie, social capital), environmental (ie, barriers to condom and HIV services) and structural (ie, structural violence, antidiscrimination policies).
Results Adjusted for gender, age, location and income, our model showed that: (1) all latent variables at the structural and environmental levels were significantly positively associated with each other (all ps<0.05); (2) barriers to condom and HIV services were significantly negatively associated with social capital (p<0.001) as well as condom self-efficacy (p<0.001); and (3) there were significantly positive associations between social capital and condom self-efficacy (p<0.001), and between condom self-efficacy and condom use (p<0.001). Moreover, social capital and condom self-efficacy fully mediated and buffered the negative effects between environmental and structural barriers and condom use.
Conclusion This is the first known study pointing to multiple relationships and pathways across multiple socioecological levels that can potentially be leveraged for future interventions aimed at improving condom use among Filipinx trans-WSM and cis-MSM. Such interventions should be multicomponent and build and/or strengthen social capital and condom self-efficacy, as well as intentionally target prominent structural and environmental barriers to condom use.
- HIV
- cross-sectional survey
- epidemiology
- prevention strategies
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
The Philippines is currently experiencing a national public health crisis that is concentrated among communities of transgender women and cisgender men who have sex with men (trans-WSM and cis-MSM, respectively), primarily due to condomless sex.
What are the new findings?
The findings of this study modelled, for the first time, the various multilevel relationships and pathways across the socioecological model that can potentially be leveraged and addressed for future HIV prevention interventions that aim to improve condom use among these populations.
Specifically, it highlighted the role of social capital and condom self-efficacy as key to increasing condom use while also acting as a buffer against the negative effects of structural and environmental barriers on condom use.
What do the new findings imply?
The new findings provide support for widespread multicomponent condom interventions among trans-WSM and cis-MSM populations in the Philippines and in other settings alike, including promotion of social capital and condom self-efficacy.
Background
Globally, communities of transgender women and cisgender men who have sex with men (trans-WSM and cis-MSM, respectively) are disproportionately impacted by the HIV epidemic.1–3 In the Philippines, where HIV is a national crisis, Filipinx (ie, gender and racially neutral term to describe citizens of the Philippines) trans-WSM and cis-MSM account for about four in five new HIV diagnoses annually since 2016.4 Moreover, the HIV prevalence is higher for trans-WSM and cis-MSM (1.7% and 4.9%, respectively), compared with the general population’s HIV prevalence of 0.1%.5 In the last decade, the country’s HIV epidemic has rapidly increased by more than fivefold, from 15 000 diagnosed cases in 2010 to 77 000 in 2018.5 Country surveillance reports have attributed trans-WSM and cis-MSM’s elevated risk for HIV infection primarily to condomless sex.5–8 According to UNAIDS, about 1 in 3 trans-WSM (out of the estimated population size of 122 800 trans-WSM) and about 1 in 2 cis-MSM (out of the estimated population size of 531 500 cis-MSM) have ever used condoms in the Philippines.5 Given the low uptake of condoms, it is important for the country’s public health efforts to understand factors that impact condom use among these two important communities.
Although condom use is often considered an individual-level behaviour, studies have shown that risks for condomless sex are shaped and exacerbated by social, environmental and structural factors and conditions.9–11 The socioecological model is a conceptual model developed to understand and organise multilevel predictors of a behavioural health outcome across individual, social, environmental and structural levels.9 In the literature of gender and sexual health, it has been hypothesised that trans-WSM and cis-MSM’s health inequities and behaviours arise from multiple, intersecting personal, social and structural stressors due their marginalised gender and sexual identities.10 In the context of the Philippines, the HIV literature among trans-WSM and cis-MSM communities remains scant,12 and no studies to date have applied the socioecological model to understand condom use behaviour in these two Filipinx communities.
Socioecological factors that contribute to condomless sex among trans-WSM and cis-MSM communities in other settings have been previously described.11 Some individual-level factors include having low self-efficacy in using condoms with casual and primary partners, and low condom knowledge.13 14 Social-level indicators include not having social capital to access and use condoms and other HIV prevention services.13–15 Environmental-level factors include inaccessibility and unavailability of condoms, and avoiding health services due to issues such as cost, distance and lack of competent providers.16–18 Structural-level factors include widespread violence (eg, transphobia, homophobia) due to identifying as part of marginalised gender and sexual communities (eg, lesbian, gay, bisexual, transgender (LGBT) community) and HIV communities.17 19–21 Moreover, structural factors such as lack of protective antidiscrimination policies have also been linked to lower condom use.22 23 The lack of protective structural factors such as antidiscrimination policies may drive trans-WSM and cis-MSM members away from attaining HIV prevention services like condoms. Taken together, these findings underscore the need for multilevel, high-impact condom intervention tailored to trans-WSM and cis-MSM populations.24–28
However, the studies conducted to date have generally focused on predictors of condom use at a single level of analysis, often situated at the individual level such as understanding how to increase knowledge, skills and attitudes towards improving use of condom,29–31 rather than examining condom use predictors at multiple levels simultaneously. To our knowledge, there are no studies that have assessed these multilevel factors to predict condom use in a unified conceptual framework using structural equational modelling (SEM) approach to demonstrate associations within and across levels simultaneously.10 12 As noted, social capital and self-efficacy are key variables within the socioecological model due to their relevance for public health interventions. Both variables theoretically operate as mechanisms linking upstream variables (structural and environmental factors) with condom use. Investigation of these theorised relationships can provide empirical support for the design of interventions aiming to strengthen social capital and self-efficacy as pathways to increase condom use and reduce HIV transmission among trans-WSM and cis-MSM. However, if there are direct associations between upstream variables and condom use that are not explained by social capital and self-efficacy (ie, as mediating variables), then it is unlikely that interventions addressing these specific mid-level variables can influence condom use. In this case, interventions must more directly target structural and environmental factors or identify alternative mid-level variables that account for the influence of upstream variables on condom use.
There is a clear need to improve condom utilisation among Filipinx trans-WSM and cis-MSM communities to reduce the spread of HIV in the Philippines.12 17 Currently, condom distribution programmes in the country face barriers to implementation. For example, the country’s Department of Health strategy for public condom distribution and educational programmes are currently facing strong oppositions from the Catholic Church.32 The Philippines’ population is 93% Catholic,33 and religious institutions are concerned that distributing condoms may encourage promiscuity and are, therefore, restricting availability of condoms only to health clinics and convenience stores.32 However, our formative qualitative study on barriers to condom use among Filipinx trans-WSM and cis-MSM found that despite condom availability in these venues, issues such as cost, distance to and from healthcare clinics and convenience stores, lack of privacy and feeling stigmatised when purchasing condoms continue to be salient barriers to condom use, leading many to avoid these venues.17
To understand how these multilevel factors of condom use are linked among Filipinx trans-WSM and cis-MSM, it is essential to examine pathways that explore how these factors interplay across the multiple socioecological levels. Using SEM, the purpose of this analysis is to: (1) to test our hypothesised model, displayed in figure 1, that condom use behaviour among these two communities are reinforced and/or enabled by personal, social, environmental and structural factors; and (2) to assess the direct, indirect (ie, mediating) and overall effects of associations between structural-level and environmental-level barriers to condom use, social-level social capital, and personal-level factor condom self-efficacy, and the outcome, condom use. Specifically, we hypothesised that:
Hypothesis 1: Social capital mediates the relationship between condom use and structural-level and environmental-level barriers to condom use.
Hypothesis 2: Condom self-efficacy mediates the relationship between condom use and structural-level and environmental-level barriers to condom use.
Hypothesis 3: Condom self-efficacy mediates the relationship between social capital and condom use.
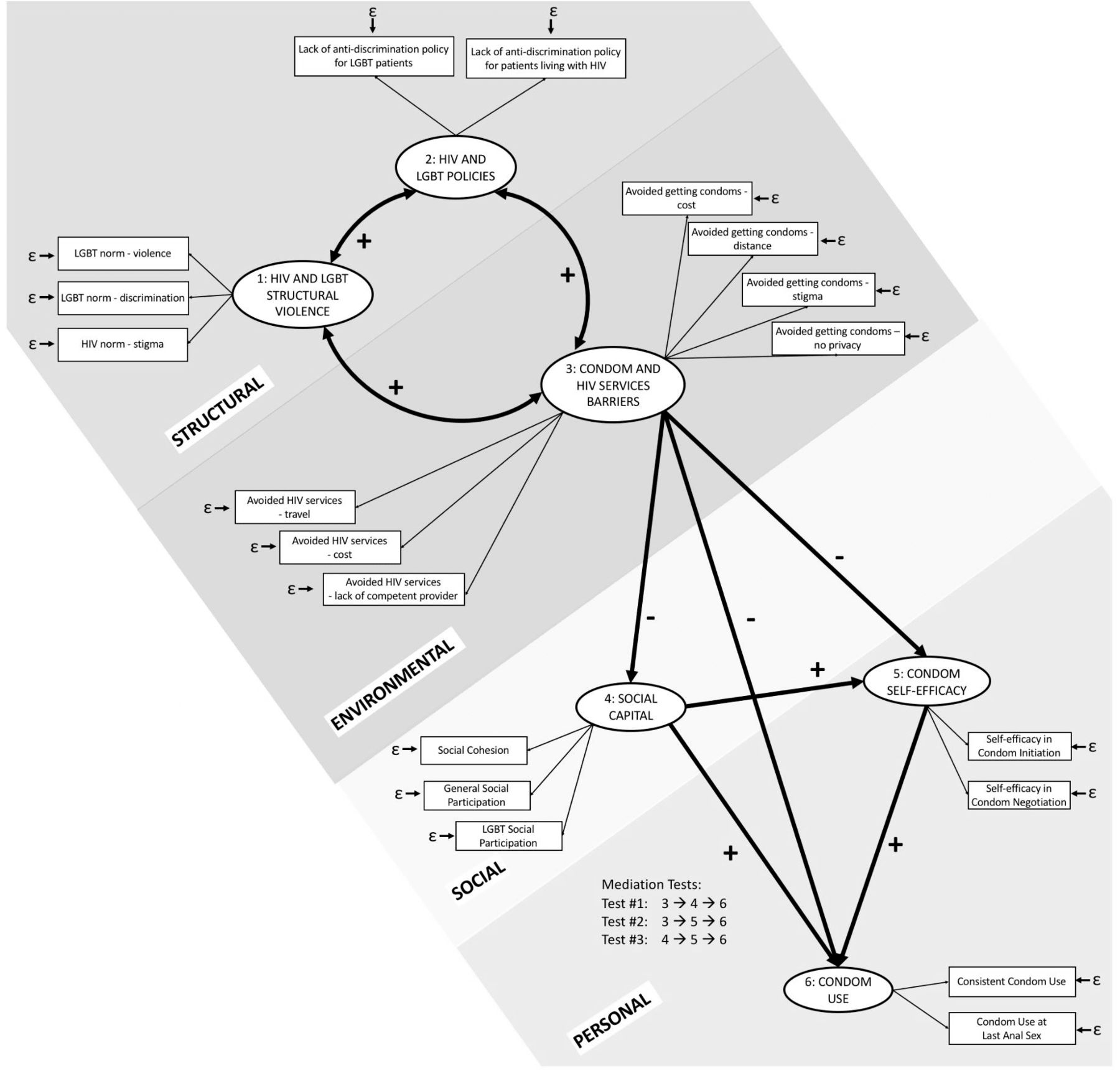
Hypothesised model. Notes: error variance terms for measured variables are shown as ε. Model is adjusted for gender, age, location and income. LGBT, lesbian, gay, bisexual, transgender.
Methods
Setting
Data for this study were collected through a web survey of trans-WSM and cis-MSM in Manila and Cebu cities, Philippines. Manila and Cebu are the top two metropolitan Philippine cities where HIV prevalence are observed to be highest,8 and where TW and cis-MSM are likely to congregate. The study was conducted between June 2018 and August 2019.
Sample
Participants were recruited via purposive sampling by posting the survey link at online venues where trans-WSM and cis-MSM are known to commune including: (1) private Facebook pages of local non-profit LGBT community-based organisations (CBOs); and (2) private member-only email listserv created by local CBOs.
To be eligible for this study, participants had to: (1) be at least 18 years old; (2) identify as either trans-WSM or cis-MSM; (3) self-report condomless anal sex in the past 12 months; (4) live in Manila or Cebu; (5) provide online written consent and (6) demonstrate English comprehension via a brief cognitive screening form. A brief cognitive screening form tested participants’ English comprehension via a series of true–false questions based on the consent form. Example questions include: ‘There is no cost for you to participate in this study’ (true/false), and ‘This study is voluntary’ (true/false). Moreover, we used the Flesch-Kincaid Reading Level Test to help ensure survey language was maintained a sixth grade level readability.34 In our formative qualitative work, conducting the study in English was not an impediment to recruiting, creating rapport and interviewing participants.
Procedures
Participants interested in the study were screened for eligibility. Following electronic informed consent, participants answered the survey using their own device (eg, laptop, smartphones or tablet computers). The range of time for participants to complete the survey was between 20 min to 25 min.
We implemented a series of best practices for conducting online surveys.35 First, to confirm that actual human participants were taking the survey, a ‘captcha box’ was programmed into the survey to rule out robots.36 Second, to ensure that each survey was unique and that there were no duplicates, we systematically implemented a cross-validation programme that flagged duplicated (Internet Protocol) IP addresses.37 38 Any IP address that were not unique were blocked from taking the survey.
All enrolled participants provided electronic written informed consent and received an online mobile load card worth P300 (approximately US$5.85) for their time spent completing the survey. The survey instrument was pilot tested by two trans-WSM and two cis-MSM community members to ensure its face validity.
Measures
Demographic variables
We asked about participants’ demographic characteristics, specifically about their gender (transgender woman/cisgender man), age (continuous), location (Manila/Cebu) and past year income (no income in the past year/less than ₱10 000/₱10 000–₱20 000/₱20 000–₱30 000/₱30 000 or more).
Structural-level variables
We operationalised the latent variable lack of HIV and LGBT clinic policies via two indicators of LGBT-related and HIV-related lack of antidiscrimination clinic policy for (1) LGBT patients and (2) for patients living with HIV. We asked participants whether their primary healthcare clinics lacked antidiscrimination policies based on sexual and gender identities or HIV status. Responses were dichotomised into either yes or no.
We operationalised the latent variable of HIV and LGBT structural violence using three indicators: (1) LGBT violence, (2) anti-LGBT discrimination and (3) HIV stigma. In this study, structural violence is defined an ‘avoidable impairment of fundamental human needs’.39 This includes multiple forms of violence based on one’s identities, including gender and sexual identities and HIV status.
To measure LGBT violence, we adapted Hill and colleagues’ Transphobia, Homophobia and Genderism Scale,40 which measures participant’s perception of society’s beliefs and attitudes about violence towards trans-WSM and cis-MSM. Example items include: ‘People around me have behaved violently towards a man because he was too feminine’, and ‘People around me have teased a transgender woman because of her masculine appearance or behavior’. This is a 7-item scale with a 5-point Likert response options from 1=strongly disagree to 5=strongly agree. Responses were summed and scored continuously (mean (M)=11.41, SD=9.89, Cronbach α=0.93).
We assessed anti-LGBT discrimination by adapting a subsection of Davidson’s Gender Inequality Scale that pertains to discrimination.41 This subsection measures participants’ experiences of facing discrimination based on their gender and sexual identities, including whether they have lost their job or have been denied a promotion at work, removed from direct contacts with classmates, workmates or patients, and have been denied healthcare services, all due to their LGBT identity. This is a 4-item measure with response options that were either 1=true or false=0, and scores were responses were summed and scored continuously (M=0.71, SD=1.32. Cronbach α=0.89).
To assess HIV stigma, we used Reinius et al’ HIV stigma scale,42 which measures public attitudes and stigma about people living with HIV. Example items include: ‘Most people believe a person who has HIV is dirty’, and ‘People who are suspected of having HIV/AIDS lose respect in the community’. This is a 13-item scale with a 5-point Likert response options from 1=strongly disagree to 5=strongly agree. Responses were summed and scored continuously (M=37.15, SD=9.52, Cronbach α=0.94).
Environmental-level variables
Condom and HIV services barriers as a latent variable was operationalised via a series of items that asked participants whether they have avoided getting either condom or HIV services due to barriers they experienced in the past year. These items were based on our formative qualitative work.17 Specifically, we asked participants about whether they have avoided getting condoms due to: distance of travel from/to at convenience stores or clinic (yes/no), cost of buying condoms (yes/no), feeling stigmatised by store or clinic workers (yes/no), or having no privacy when either purchasing or getting condoms(yes/no). Given that condoms are also freely available in clinics, and that some clinics in the Philippines were reported to require HIV testing prior to giving out condoms,17 we included barriers to HIV services together with condoms as one latent variable. We asked participants about whether they have avoided getting HIV services due to: distance of travel from/to clinics (yes/no), cost of services (yes/no) and lack of competent providers who are knowledgeable about health issues and needs specific to trans-WSM and cis-MSM (yes/no).
Social-level variables
We operationalised the latent variable of social capital using three indicators: (1) social cohesion, (2) general social participation and (3) LGBT social participation. In this study, social capital is defined as the resources that are available and accessed by trans-WSM and cis-MSM via involvement and participation within their social relationships and networks.43–45
To measure social cohesion, we adapted Lippman et al’ Social Cohesion Scale.28 Example items from scale included: ‘You can count on your trans-WSM and/or cis-MSM friends to help you access health services’, and ‘You can count on your trans-WSM and/or cis-MSM friends to support the use of condoms’. This is a 9-item scale with a 5-point Likert response options from 1=strongly agree to 5=strongly disagree. Responses were summed and scored continuously (M=32.51, SD=7.04, Cronbach α=0.91).
To measure general and LGBT social participation, we adapted Fonner et al’ Social Participation Scale.14 This scale asked participants four items on their involvement in general community activities (eg, going to church, participating in cultural events) as well as four items on their LGBT community activities (eg, joining HIV advocacy groups, and advocating for local LGBT organisations). Response options were either 1=no involvement, 2=member, 3=active member or 4=leader of the group. Responses were summed and scored continuously (M=6.55, SD=2.45, Cronbach α=0.78 for general social participation, and (M=8.42, SD=3.60, Cronbach α=0.85 for LGBT social participation, respectively)).
Personal-level variables
Condom self-efficacy was operationalised using two indicators: (1) self-efficacy in condom initiation, and (2) self-efficacy in condom negotiation.
Self-efficacy in condom initiation was measured using Misovich and Fisher’s Condom Self-Efficacy Scale,46 which asked participants to rate their self-efficacy in buying condoms from the store, getting condoms from clinics, using condoms while under influence of alcohol or illicit drugs, and initiating condoms use with sexual partners. Example items include: ‘How hard would it be for you to buy or get condoms’, and ‘If you were able to persuade your partner to begin using condoms with you, how hard would it be for you to continue using condoms every time you have sexual intercourse until both of you get an HIV test?’ This is an 8-item scale with a 5-point Likert response options from 1=very hard to 5=very easy. Responses were summed and scored continuously (M=26.04, SD=3.69, Cronbach α=0.92).
To measure self-efficacy of condom negotiation with partners, we used Rotheram-Borus and Murphy’s Condom Negotiation Efficacy Scale.47 Example items include: ‘I can ask a partner to use condoms’, and ‘I can get every partner to use condoms, even if they don’t want to’. This is a 5-item scale with a 10-point Likert response option from 1=cannot do at all to 10=certainly can do. Responses were summed and scored continuously (M=32.12, SD=12.85, Cronbach α=0.91).
Outcome variable
Condom use was operationalised using two indicators adapted from Fonner et al’ Condom Use Measurement48: (1) consistent condom use, and (2) condom use at last sex. For consistent condom use, we asked participants whether they have used condom all the time, occasionally, or never in the past year. We scored consistent condom use conservatively by dichotomising responses to all the time versus occasionally/never. For condom use at last sex, we asked participants whether they used condom during their last sexual anal intercourse (yes/no).
Analyses
The analysis was restricted to participants (n=318) with complete data on our latent outcome variable of interest (ie, condom use). This resulted in dropping two participants from the analysis. We performed descriptive (ie, mean, percentages) and bivariate analyses (ie, χ2 or t-test) to determine patterns of association between our outcome and independent variables (table 1). To determine internal reliability of our scale variables, we conducted sensitively analysis (table 2). All Cronbach alphas ranged from acceptable to excellent reliability (all alphas >0.70, range=0.78–0.94).
Sample characteristics by condom use outcomes (n=318)
Descriptive statistics and reliabilities of examined scales for model latent variables (N=318)
We tested our hypothesised model using SEM. Prior to running our SEM, we conducted a multicollinearity test using variance inflation factor (VIF), and determined that there were no multicollinearities between our measured variables (all VIFs<4.00).49 We then conducted SEM to test our hypothesised model (figure 1), including our three proposed mediational tests. Given the modest sample size, we used a non-parametric bootstrapping procedure with 100 iterations to resample and increase our confidence in statistical interpretation and inference.50 The final model was standardised and controlled for gender, age, location and income. Mediation analyses were adjusted for all demographic, environmental-level and structural variables. To determine overall model fit,51 52 we used the following standard cut-off points for SEM: (1) χ2 badness-of-fit index (p>0.05), (2) root mean square error approximation (RMSEA <0.08), (3) non-normed fit index (NNFI value >0.90), (4) comparative fit index (CFI >0.90) and (5) standardised root mean square residual (SRMS <0.08). All analyses were conducted using StataSE V.15.1, and two-tailed tests were used for determine significance (p<0.05).53
Results
Sample characteristics
A total of 318 participants were included in this analysis. Sample characteristics across personal, social, environmental and structural indicators by condom use outcomes are displayed in table 1.
Bivariate analysis
Bivariate test results are displayed in table 1. As shown, both condom use variables were significantly associated with structural, environmental, social and personal levels of the proposed model. Participants who did not report consistent condom use were significantly more likely to not use condoms during last sex (p<0.001).
Final adjusted structural equation model fit
The final standardised SEM model was adjusted for gender, age, location and income (figure 2). With exception to χ2 goodness-of-fit test (χ2 (174)=277.70, p<0.001), the overall fit of the final standardised SEM model was acceptable with RMSEA=0.04 (90% CI 0.03 to 0.05), CFI=0.93, NNFI=0.90 and SRMS=0.05.

{kind=link}
{kind=link}
Final standardised and adjusted parameter estimates model with mediational analyses. Notes: error variance terms for measured variables are shown as ε. Model is adjusted for gender, age, location and income. With exception to χ2 goodness-of-fit test, this model has acceptable fit (χ2 (174) = 277.70, p<0.001; root mean square error approximation = 0.04, 90% CI = 0.03 to 0.05; comparative fit index=0.93; non-normed fit index=0.90; standardised root mean square residual=0.05). *p<0.05, **p<0.01, ***p<0.001. LGBT, lesbian, gay, bisexual, transgender.
Overall effects
Latent variables at the structural and environmental levels were all positively associated with each other. Specifically, HIV and LGBT structural violence was significantly associated with lack of HIV and LGBT clinic policies (A: β=0.48, p<0.001), lack of HIV and LGBT clinic policies was significantly associated with condom and HIV services barriers (B: β=0.74, p<0.001), and condom and HIV services barriers were significantly associated with HIV and LGBT structural violence (C: β=0.39, p<0.001).
Experiencing barriers to accessing condoms and HIV services was significantly associated with decreased social capital (D: β=−0.18, p<0.001) and condom self-efficacy (E: β=−0.35, p<0.001). Experiencing barriers to condom and HIV services was not significantly associated with condom use (F: β=−0.01, p=0.99) due to mediation analysis.
Significantly positive associations were found between relationships of social capital and condom self-efficacy (G: β=0.29, p<0.001), and between condom self-efficacy and condom use (I: β=0.47, p<0.001). Social capital was positively associated with condom use (H: β=0.71, p=0.45); however, this relationship was not significant.
Direct and indirect (mediating) effects
Full mediations were observed across all three hypothesised mediational tests. Below we detailed the direct and indirect effects for each of the hypothesis test.
Hypothesis 1
Social capital fully mediated the relationship between barriers to condom and HIV services and condom use, given that the direct effect between barriers to condom and HIV services and condom use was no longer significant after social capital was added in the model (F.1.1: β=−0.20, p<0.05 (before mediation) vs F.1.2: β=−0.12, p=0.13 (after mediation)). The indirect effect between barriers to condom and HIV services and social capital (D.1: β=−0.17, p<0.01), as well as between social capital and condom use (H.1: β=0.47, p<0.001) remained statistically significant and provided further support for full mediation.
Hypothesis 2
Condom self-efficacy fully mediated the relationship between barriers to condom and HIV services and condom use, given that the direct effect between barriers to condom and HIV services and condom use was no longer significant after condom self-efficacy was added in the model (F.2.1: β=−0.20, p<0.05 (before mediation) vs F.2.2: β=−0.0003, p=0.99 (after mediation)). The indirect effect between barriers to condom and HIV services and condom self-efficacy (E.2: β=−0.39, p<0.001), and between condom self-efficacy and condom use (I.2: β=0.51, p<0.001) remained statistically significant and provided further support for full mediation.
Hypothesis 3
Lastly, condom self-efficacy fully mediated the relationship between social capital and condom use, given that the direct effect between social capital and condom use was no longer significant after condom self-efficacy was added in the model (H.3.1: β=0.19, p<0.05 (before mediation) vs H.3.2: β=0.06, p=0.53 (after mediation)). The indirect effect between social capital and condom self-efficacy (G.3: β=0.36, p<0.001), and between condom self-efficacy and condom use (I.3: β=0.47, p<0.001) remained statistically significant and provided further support for full mediation.
Discussion
To our knowledge, this is one of the first empirical studies that linked together multilevel theoretical predictors and mediating variables in a single social-ecological model to explain condom use among trans-WSM and cis-MSM populations. The sample was recruited in the Philippines, which is currently experiencing a rapidly growing HIV epidemic. Only a minority of our sample used condoms consistently in the past year (19.69%) and at last sexual anal intercourse (42.50%). The results suggest that social capital and condom self-efficacy are important mediators between environmental barriers to condoms and HIV services and our outcome, condom use. These findings corroborate national Philippines surveillance reports that document low condom use among these two communities,5 8 and underscore the importance of exploring and addressing multiple relationships and pathways that can potentially be leveraged to improve condom use.
This study highlighted a reinforcing feedback mechanism loop, such that variables at the structural and environmental levels are all positively associated with each other—and that environmental barriers to condom and HIV services contribute to lower condom use. Given how widespread these barriers are in the Philippines and the fact that they are likely to be salient in the lived experiences of Filipinx trans-WSM and cis-MSM,20 54–56 there is a need for future interventions to address multilevel, external factors that are simultaneously impacting condom use behaviours. Other studies among these populations have noted that risk factors for condom use are often predominantly situated at the individual level, particularly informational-related, attitude-related and knowledge-related factors.29–31 While interventions addressing individual-level factors could impact condom use, such change may unlikely be maintained over time in the absence of interventions that also address environmental and structural factors that can enable long-term behaviour change goals.57–59 Given the reinforcing feedback mechanism of this loop, future examination using systems thinking analysis approach may likely be beneficial in understanding this cycle.60 A systems thinking analysis approach applied in behavioural research could further explicate and visualise the interconnected ‘system of systems’ that are present in a particular environment that altogether work to sustain or limit a particular behaviour.60
In agreement with previous studies,15 16 28 61–65 this study highlights social capital and condom self-efficacy as vital protective factors that buffer against the negative effects of environmental barriers on condom use, which support our hypotheses. Based on our findings, these variables can be strategic targets for public health interventions aiming to improve condom use for populations that experience environmental barriers to HIV services. Previous research has noted that social capital could help prevent structural violence and lower environmental barriers via social networks’ collective participation and sharing of resources.14 15 A previous qualitative study characterising Filipinx trans-WSM and cis-MSM’s social networks has also noted that condoms are often distributed through peer-to-peer social connections, such that trans-WSM and cis-MSM peers or ‘clan members’ would often rely and ask each other for supplies of condoms.17 The current study characterises a nuanced mediating role for both social capital and condom self-efficacy in promoting actual condom use behaviours in the presence of environmental barriers. Future studies should examine the direct role of structural barriers on social capital, self-efficacy and condom use.
Additionally, our findings highlighted pathways that could potentially increase both social capital and condom self-efficacy in this setting. This study found that environmental barriers to condom and HIV services are inversely associated with social capital and condom self-efficacy. Increasing social capital and condom self-efficacy in this context, therefore, necessitates future research to examine mechanisms that can address upstream or distal factors that reduce environmental barriers to promoting social capital and condom self-efficacy. This is in line with Bordeau’s approach to social capital,66 which posits that health inequities in general can be addressed by facilitating greater capacity for members of social networks to participate in accessing and using health resources. The findings of this study suggest that addressing environmental barriers to condom and HIV services may potentially increase trans-WSM and cis-MSM community members’ social capital as doing so may provide greater capacity for members to participate in accessing and using condoms and other HIV prevention resources. Similarly, Bandura’s triadic reciprocal determinism theory has also described efficacy as a personal cognitive factor that is both influencing and influenced by behaviour and existing environmental resources.67 Future behavioural interventions aiming to promote condom utilisation among Filipinx trans-WSM and cis-MSM should be multicomponent,29 and should situationally examine and address the kinds of environmental barriers present both external and within trans-WSM and cis-MSM’ social networks.
In the current context of the Philippines, the lack of protective laws specifically for trans-WSM and cis-MSM communities in combination with the widespread structural violence like stigma and discrimination present as structural barriers.20 54–56 68 69 Such barriers can promote negative experiences and drive community members further away from accessing resources like condoms and other HIV services,70 71 and prevent community members from affiliating, identifying and interacting with other trans-WSM and cis-MSM. While there is currently a national antidiscrimination law (ie, Republica Act 11166) in the country,72 it only safeguards individuals based on HIV positive status; there are no existing national policies that provide protections explicitly based on gender and sexual identities.69 Moreover, the current national HIV strategy makes no mention of structural programmatic priorities,54 such as antidiscrimination clinic policies and cultural competency trainings, which could improve care delivery to trans-WSM and cis-MSM community members. There is emerging evidence showing positive effects of antidiscrimination structural interventions and professional trainings.73–75 The findings of this study, therefore, point to structural gaps in HIV prevention policy strategies and programmatic trainings that could potentially address environmental barriers to condom and HIV prevention services among trans-WSM and cis-MSM communities in the Philippines.
We also found that travel, cost and distance to/from clinics or convenience stores as barriers to condoms and other HIV services are linked to lower social capital, condom self-efficacy and condom use. One possible explanation for these linkages could be due to the opportunity cost in the context of poverty, since approximately two-fifths of the sample either earned less than ₱10 000 (approximately US$200) or did not have income in the past year. These barriers pose an opportunity cost—that is, the loss of a benefit when one person chooses one alternative option over another76—since most individuals who experience poverty are likely to focus their time on other priorities and not on activities that may be strenuous, time consuming and/or costly. Additionally, these barriers also act as constraints to condom self-efficacy given that the product (ie, condoms) is cost prohibitive; therefore, the recommended behaviour cannot be performed.67 While condoms are free in clinics, the findings point to the infrastructural and logistical issues in distributing condoms given the scarcity of HIV clinics in the Philippines. As of 2018, there were 14 HIV clinics, with only three community-based organisation clinics targeting cis-MSM and no clinics have been designed for trans-WSM.77 These findings, therefore, align with Philippine’s Health Department current condom distribution strategy to further expand availability of free condoms beyond clinics.32 Additionally, while condoms can be purchased in convenience stores, it could likely continue to pose as a financial barrier to community members from low-income background. Given that trans-WSM are often economically marginalised from attaining jobs and fair wages due to employment discrimination and stigma,21 78 it is possible that Filipinx trans-WSM community members may face greater financial barrier to purchasing condoms than their cis-MSM peers—a point for further research.
Limitations
There are some limitations to this study that are worth noting. First, the cross-sectional data do not allow inferences about causation between exposure and outcome variables.79 Future research exploring this phenomena should use data from longitudinal study design, which can provide temporality and can strengthen findings of the mediation analysis. Second, because the levels of socioecological model are defined in various ways in the literature,21 80 81 it is possible that some of the variables that are hypothesised in this study may reside in a different level according to different interpretations of the socioecological model. Third, the variables assessed in this study are based on perceived individual-level experiences across the social, environmental and structural levels. As such, this analysis could be strengthened by having multiple sources of data that do not rely on self-reported measures (eg, administrative data, biomarkers, surveillance, assessment of existing antidiscrimination policies, etc). Fourth, this study used a convenience sampling approach through purposively targeting social media and email platforms and implemented English comprehension language screening. As such, the study findings are not representative of and cannot be generalised to all Filipinx trans-WSM and cis-MSM, particularly those who may not have access to these platforms and/or may lack English language comprehension. Lastly, the data were collected in a self-reported manner. While self-reports are conventional methods in behavioural research, self-reports are often prone to under-reporting particularly when questions probe participants’ personal behaviours and experiences that may be stigmatising.
Conclusion
This study examined and linked together various multilevel predictors and mediators of condom use in Filipinx trans-WSM and cis-MSM communities. Taken together, the findings of this study call for multilevel interventions to improve condom use behaviours among Filpinx trans-WSM and cis-MSM. In particular, findings reveal that social capital and condom self-efficacy are important mediators to be considered for future interventions aiming to increase condom use and other HIV services among these communities. Such multicomponent interventions should involve building and/or strengthening community cohesiveness and participation and should carefully examine and intentionally target prominent barriers to social capital, condom self-efficacy and condom use.
Acknowledgments
The authors's foremost appreciation goes out to the participants of this study. They thank their research assistants who made this study possible: Patricia Rodarte, Savannah Gomes, Bianca Obiakor, Emily Yoshioka and Valerie Santos.
References
Footnotes
Handling editor Seye Abimbola
Contributors All authors were involved in the conceptualisation of this paper. AR, TS, ML, SC-U and DO designed the analysis for this paper and analysed the data. AR conducted the data analysis and wrote the paper. All authors reviewed the paper.
Funding This work was supported by the National Institute of Health-Fogarty International Centre under Grant D43TW010565; Providence/Boston Centre for AIDS Research under Grant P30AI042853; the National Institute on Drug Abuse under Grant R36DA048682. AR is a recipient of the Robert Wood Johnson Foundation Health Policy Research Scholars and a Public Policy Fellow at amFAR, the Foundation for AIDS Research. AO’s contribution is supported by the National Institute on Drug Abuse under Grant R36DA047216. TS’s contribution is supported by NIMH Centre under Grant P30MH43520.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee (Brown University Human Research Protection Programme Institutional Review Committee in Providence, Rhode Island) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Data cannot be shared publicly per IRB agreement on data sharing and to minimise participant risk and maximise privacy and confidentiality as much as possible. Data are available from the Brown University Institutional Data Access/Ethics Committee (contact via irb@brown.edu) for researchers who meet the criteria for access to confidential data.