Article Text

Abstract
Introduction Intimate partner violence (IPV) threatens women’s health and safety globally, yet services remain underdeveloped and inaccessible. Technology-based resources exist, however, few have been adapted and tested in low-resource settings. We evaluate the efficacy of a community-partnered technology solution: culturally and linguistically adapted version of the myPlan app, a tailored safety decision-making and planning intervention, administrated by trained lay professionals.
Methods This randomised, controlled, participant-blinded superiority trial compares safety-related outcomes at baseline, immediate post intervention and 3-month follow-up among women at risk of and experiencing IPV in Nairobi, Kenya. Women were randomised (1:1 ratio) to: (1) myPlan Kenya (intervention); or (2) standard IPV referrals (control). Primary outcomes were safety preparedness, safety behaviour and IPV; secondary outcomes include resilience, mental health, service utilisation and self-blame.
Results Between April 2018 and October 2018, 352 participants (n=177 intervention, n=175 control) were enrolled and randomly assigned; 312 (88.6%, n=157 intervention, n=155 control) were retained at 3 months. Intervention participants demonstrated immediate postintervention improvement in safety preparedness relative to control participants (p=0.001). At 3 months, intervention participants reported increased helpfulness of safety strategies used relative to control participants (p=0.004); IPV reduced in both groups. Among women reporting the highest level of IPV severity, intervention participants had significant increase in resilience (p<0.01) compared with controls, and significantly decreased risk for lethal violence (p<0.01).
Conclusions Facilitated delivery of a technology-based safety intervention appropriately adapted to the context demonstrates promise in improving women’s IPV-related health and safety in a low-resource, urban setting.
Trial registration number Pan African Clinical Trial Registry (PACTR201804003321122).
- public health
- randomised control trial
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Safety planning is a widely advocated intervention to respond to intimate partner violence (IPV).
An mHealth-based safety decision aid intervention for IPV survivors has demonstrated reductions in decisional conflict and increases in safety planning behaviours.
To date, all mHealth safety planning interventions have occurred in high-income settings.
What are the new findings?
This study is, to our knowledge, the first trial evaluating a technology-based intervention for IPV prevention and response with support of trained lay providers in a low-income or middle-income setting.
Survivors in the intervention group reported improvements in safety preparedness and increased helpfulness of safety strategies used.
Among women at the highest levels of violence severity, the intervention increased resilience (p<0.01) relative to control condition, and significantly decreased risk for lethal violence by 3-month follow-up (p<0.01).
What do the new findings imply?
Technology implemented by lay professionals can be used to appropriately deliver safety interventions for IPV survivors in low-resource settings.
Tailored, app-based IPV prevention and response tools may reduce the public health impact of IPV, when situated alongside meaningful community-based violence prevention and response efforts.
Introduction
Intimate partner violence (IPV) threatens the health and well-being of women and girls globally. Eliminating IPV and other forms of gender inequity are targets of the sustainable development goals.1 Intimate partners perpetrate over one-third of female homicides.2 Non-fatal IPV consequences include poor mental, physical and sexual health.3 Evidence-based prevention and response is urgently needed, particularly in low/middle-income countries (LMICs), where support resources can be scarce. In Kenya, an estimated 39% of ever-married women have experienced physical or sexual IPV.4 Enabling social norms include male-dominated decision-making and authority within relationships, as well as IPV tolerance that challenges women’s ability to seek help and identify abusive experiences.5–7
While a comprehensive approach to IPV requires addressing perpetration, sustained needs remain for supporting IPV survivors, particularly in high-prevalence settings. Safety planning for harm reduction is one of the most widely recommended interventions for IPV prevention and response. Disclosing abuse and obtaining support can reduce self-blame8 and revictimisation.9 Yet too few survivors receive formal support due to stigma, self-blame and gaps in logistics and infrastructure.10 11 In LMICs, limited available research shows that IPV survivors engage in active, intentional harm reduction and safety strategising, including engaging informal networks, removing stressors/avoidance, minimising damage to the self and family, and building personal resources.12 In Nairobi’s informal settlements, IPV survivors face a host of barriers to safety, yet often take action steps in securing financial resources and personal property.13
Women often face multiple, competing priorities such as privacy, children and financial security in considering how to respond to IPV. Thus, a cornerstone of safety planning is clarification of personal priorities. Decision science, which examines decision-making processes and decisional conflict resolution, is a novel and underutilised tool for the IPV response. Decision aids can provide information about healthcare options, and clarify personal priorities to reduce decision-related uncertainty and support decisions.
The first decision aid to address IPV and safety planning is myPlan, an interactive, personalised tool for survivors. Content is delivered via a secure app, developed by Johns Hopkins University (www.myplanapp.org). myPlan provides healthy relationship education, and solicits information about a current intimate relationship, including risk of severe and lethal violence, reproductive coercion and safety priorities to prompt risk recognition and generate safety strategies and referrals tailored to women’s priorities.14 Key features include the self-assessed ‘red flags’, or signs of an unhealthy intimate relationship, and Danger Assessment, a validated measure of risk factors for severe and lethal relationship violence15; scores are converted to visuals to convey danger levels. Subsequently users complete an interactive prioritisation of safety priorities (eg, well-being of child(ren), privacy, etc) via systematic pairwise comparison. Based on inputs, a personalised safety plan is generated with relevant referral information. Extensive electronic safety features include a four-digit security personal identification number (PIN), a ‘dummy’ PIN that redirects to alternate content, and access via web or downloadable app to maximise options. In addition to decision science, myPlan is rooted theoretically in social cognitive theory,16 empowerment17 and trauma-informed care,18 which emphasise safety and empowerment through agency in decision-making and healing. myPlan works to promote long-term support and safety by providing support for (1) defining healthy relationships; (2) safety behaviour, by helping women identify the severity of the violence and potential danger to self and family and providing a set of options; (3) decision-making, via clarifying safety priorities to reduce decisional conflict and enhancing safety preparedness; and (4) healing, via validating messages to counter the culture of victim blaming and stigma, bolster resilience and enable safety behaviour and connection to both formal services (eg, hotline, healthcare providers, advocates) and informal (family/friends, coworkers) networks. Reducing decisional conflict and self-blame, and enhancing resilience and safety behaviours are critical short-term outcomes on the pathway to safety and violence prevention. myPlan has been implemented with racially and ethnically diverse populations in high-resource settings (eg, USA, Canada, New Zealand and Australia). It has generated reductions in decisional conflict about safety,19 20 increases in use of helpful safety strategies,20 separation from abusive partners20 and in some cases, reductions in violence severity.21 The myPlan safety decision and planning intervention was adapted to the context of Nairobi, Kenya through an extensive community-partnered formative process.22 Specifically, key informant interviews and focus group discussions with violence support service providers and female IPV survivors were used to refine app content and format. Recommendations emphasised graphics and efficiency, and the resulting adapted app was piloted and further refined based on user feedback.22
To test the intervention’s efficacy on safety and health outcomes over 3 months, we conducted a longitudinal randomised controlled trial (RCT) comparing the intervention with a control condition of standard IPV-related referrals to community-based advocacy and support services. In-depth interviews (IDIs) contextualised results and clarified intervention mechanisms. We hypothesised that the intervention would increase safety preparedness, reduce decisional conflict, increase use and helpfulness of safety behaviours, and reduce IPV exposure (primary outcomes). In addition, we examined secondary outcomes that include resilience, depression, use of IPV support services, self-blame, recognition of IPV, self-efficacy, relationship quality and risk for severe/lethal violence. This RCT was conducted in Nairobi, Kenya to extend the limited knowledge base on mHealth in LMICs and advance the global priority of evidence-based interventions that prevent and respond to IPV.
Methods
Study design and participants
This community-based RCT with a one-to-one allocation ratio was conducted in three informal settlements in Nairobi, Kenya in collaboration with Ujamaa-Africa, a violence prevention and response non-governmental organisation. Ujamaa’s Mashinani Program provides economic empowerment to IPV survivors via support groups, coupled with microfinance loans, affording the team unique insight into local IPV dynamics. Study sites were Korogocho/Kariobangi, Dandora and Huruma/Mathare; these sites are densely populated, low-income informal settlement communities with a host of social and economic hazards for women, and a range of community-based services. For expedience and sensitivity in enrolling IPV survivors for this randomised trial, sites were selected based on the established presence of Mashinani, relative economic diversity and geographical proximity.
Community-based methods, including flyers, community presentations and word of mouth, recruited women who had experienced physical or sexual IPV, or reported being afraid of their partner in the previous 3 months, resided in target communities with no plans to move in the next 6 months and spoke English or Swahili. Age eligibility was restricted to 18–35 years; this population was identified in the formative phase as high risk for IPV and likely to have highest technological literacy. Eligibility confirmation, oral informed consent and all study procedures occurred in person in private, community-based, dedicated offices with skilled research assistants.
The intervention adaptation phase, study protocol and procedures are available elsewhere.22
Randomisation and masking
This randomised, controlled, participant-blinded superiority trial entailed two parallel groups. Participants were randomly assigned (1:1) to receive either myPlan Kenya intervention or a standard of care control condition, stratified by study site. Computerised blocked randomisation provided site-level stratification within the myPlan Kenya app.
All participants and staff were blinded to intervention status with the exception of team members administering the intervention. The randomisation sequence (concealed from study staff) was programmed into a secure tracking database, separate from the study website, by the study programmer, who had no participant contact.
Procedures
Participants completed the baseline survey with a trained research assistant in a private space in a community-based organisation in each of the three settlements. The tablet computer was used for consent documentation, survey data collection and analytics, such as time to completion. Following baseline survey, tablet-based randomisation directed participants to the control or the intervention conditions, which were also administered via the tablet.
Trained community health volunteer (CHVs), who worked with IPV survivors in the study communities and were technology literate, assisted in the use of the myPlan Kenya intervention app on the study tablet computer, based on formative phase recommendations to use CHVs to ease use and maximise comfort.22 The research team and CHVs underwent a month-long training focused on data collection procedures, app content, tablet use, survey measures and ethical training specific to research on gender-based violence.23
myPlan Kenya app intervention
The myPlan Kenya app sections included the following: the Healthy Relationships section is educational and helps women to define healthy and unhealthy relationships as they reflect on their own relationship. My Relationship asked the user to provide information on their relationship characteristics (eg, living together, married/partnered, children in home) to inform the tailoring of safety strategies. Red Flags assessed warning signs (eg, extreme jealousy, insults, threats, reproductive control). My Safety section provided an opportunity to self-assess risk for severe and lethal violence using the validated Danger Assessment scale.15 In the interactive My Priorities section, users made pairwise comparisons to weigh priorities such as dignity and respect, feelings for partner, health and children using a clickable ‘sliding bar’. The My Plan section provided the tailored safety plan that is populated based on data supplied by the user in the previous sections. The safety plan was followed by supplemental information About Violence, Harmful Beliefs, and relevant Resources.
Control condition
The control condition consisted of a standard ‘usual care’ set of referrals to IPV-related legal, health, safety, counselling and financial resources. For modality comparability, content was delivered in an app-like webpage with research staff available for assistance.
Immediate post intervention
Following completion of intervention or control app content, participants completed a brief tablet-based exit survey to examine immediate safety preparedness. Research assistants then issued a brief verbal screener to monitor for any emotional upset triggered by the survey, and offered participants a small grocery item and transport reimbursement. All participants were offered a facilitated referral for IPV-related medical, psychosocial or economic support. Participants in both groups had the option to return to the study centre to review their safety plan and referrals prior to 3-month follow-up visit, though no participants opted to do so.
Three-month follow-up data collection and retention
Participants were contacted for follow-up data collection beginning 1 week prior to the 3-month anniversary of their baseline study visit. Following informed consent, data collection procedures were identical to those at baseline. The myPlan Kenya app was offered to control participants following data collection.
In-depth interview
Intervention participants retained at follow-up were eligible to participate in an IDI. Purposive sampling (n=30) ensured approximately equal distribution of baseline severity of IPV, and study sites (n=10 IDIs per site). Interest and scheduling were assessed immediately after follow-up survey data collection, with all interviews occurring the following week with the same research team member. Semistructured interview guides focused on participant’s experiences with and recommendations for the intervention. Interviews were audio recorded, transcribed verbatim and translated to English language. Coding used inductive thematic analysis and focused on usefulness of the app and challenges/future recommendations; both presented herein. Emergent themes and subthemes detailed domains of helpfulness of strategies including referrals, and recommendations. Illustrative quotes that reflect overarching themes are presented. Quantitative results and qualitative themes were triangulated via convergence matrixes.
Outcomes
Primary a priori outcomes included safety preparedness, decisional conflict, use and helpfulness of safety strategies and IPV experience. We report psychometric properties for scales at baseline (n=352). Measures were vetted locally and piloted with CHVs prior to use, resulting in minor refinements to enhance readability.
The value of material provided with regard to safety preparedness, for example, how much the material reviewed assisted in decision-making and weighing risk/benefits, was assessed immediately following completion of intervention or control condition (exit survey) via 10-item Likert scale (responses: 0—not at all to 4—a great deal; range: 0–40; α=0.90).
With a 12-item adapted Decisional Conflict Scale,24 participants rated knowledge, clarity and confidence in safety options and risk/benefits of potential safety options on a Likert scale (responses: 0—not at all to 4—a great deal; range: 0–48; α=0.83).14 Decisional conflict subscales included: uninformed (α=0.74), unclear values (α=0.52), lack of support (α=0.60) and uncertainty (α=0.81).19
Metrics specific to safety strategy use and helpfulness centred on five safety strategies specific to the myPlan app content,9 14 for example, left the house temporarily to put space between you and your partner, developed an emergency signal to use with others when you felt you were in danger, put a plan into place for how to keep children safe. For each strategy, participants reported use (dichotomous), and, where applicable, helpfulness (responses: 1—not helpful to 5—very helpful). Responses generated two summary metrics: use of safety strategies reflecting number of strategies used (range: 0–5), and helpfulness of strategies used, reflecting both use and helpfulness by dividing summed helpfulness by number of strategies used (range: 0—never used to 5—used and found helpful).
Physical and sexual IPV were assessed with short forms of the Revised Conflicts and Tactics Scale (CTS-2; α=0.87).25 For each of 10 violent behaviours, women were asked frequency of occurrence in the past 3 months: never (0), 1–2 times (1), 3+ times (2) and scores summed across behaviours (range: 0–20). The 10-item Women’s Experiences of Abuse Scale26 captured emotional abuse (responses: 1—agree strongly to 6—disagree strongly; range: 10–60; α=0.89). Reproductive coercion was assessed via nine-item existing scale27 (α=0.86), summarised into a binary measure indicative of experience/no experience.
Secondary outcomes included resilience (10-item Connor-Davidson Scale; responses: 0—not true at all to 4—true nearly all the time; range: 0–40; α=0.82),28 depression (10-item Center for Epidemiologic Studies Depression Scale29; responses: 0—not at all/less than 1 day to 3—nearly every day; range: 0–30; α=0.82; modelled continuously and dichotomously with depression indicated at score≥10), self-blame (three-item adaptation of the characterological subscale of the Sexual Victimization Attributions Measure30; responses: 0—never to 4—almost always; range: 0–12; α=0.69), recognition of abuse (six-item adapted Abusive Behaviors Scale27; responses: 0—not abusive at all to 4—very abusive; range: 0–24; α=0.78), self-efficacy (six-item Generalized Self-Efficacy Scale31; responses: 1—not true at all to 4—exactly true; range: 6–24; α=0.80), safety-specific self-efficacy (four-item Self-Efficacy for Safety in Relationship Scale19; responses: 1—strongly disagree to 5—strongly agree; range: 4–20; α=0.70) and risk for severe/lethal violence (20-item Danger Assessment Scale15; range 0–20; α=0.84; intervention participants only). Relationship quality was added based on local input (four-item scale adapted from CTS-2 negotiation subscale; responses: 0—never to 3—almost always; range: 0–12; α=0.70).25 Support service consideration and use, respectively, were assessed for health, emergency, police/chief, legal, crisis hotline, counselling, housing and child services individually. Self-blame was the only measure from which items were dropped to improve psychometric properties (α improved from 0.58 to 0.69 after dropping from four to three items).
Analysis
This superiority trial aimed to evaluate myPlanKenya as compared with the standard of care control condition, and was designed with 80% power to detect differences in IPV between the two study groups, assuming 24% prevalence in the intervention compared with 39% in the control, 15% attrition and alpha at 0.05; 350 participants were required (175 per group).
Analyses were conducted from November 2018 to April 2019, using STATA V.14. The intent-to-treat, differences-in-differences approach used random effects logistic and linear regression models. Primary analysis used a group*time (pre/post) interaction term and accounted for within-person clustering and recruitment site. Main effects analyses stratified by intervention group explored effects underpinning the interaction term. Significance was set at 5%. Mean imputation handled small amounts of missing data (<2%) for the majority of outcomes and up to <6% for resilience, decisional conflict and exit-survey safety preparedness.
To explore effect modification, analyses were stratified based on IPV severity, resilience and previous (3 months prior to baseline) violence-related help-seeking, with resulting group by time interaction coefficients compared by strata.
Patient and public involvement
This community-engaged study sought public and end-user input at all phases. During the formative research stage, input from IPV survivors and stakeholders informed and finalised myPlan Kenya content, supported implementation and length of administration. CHV and end-user input informed the refinement of the logic model, and selection of survey constructs (eg, relationship quality), and ensured face validity and accurate translation of all survey measures. Intervention and surveys were piloted before implementation to assess time burden. All recruitment was conducted by CHVs who had worked with IPV survivors in the selected communities. Preliminary findings were disseminated at an event in November 2018 involving clinics, government representatives, elders/faith leaders, community-based organisations and CHVs from each of the study communities. Readiness assessment for further dissemination is underway.
Results
Quantitative findings
Participant recruitment occurred from April to August 2018, with 3-month follow-up from July 2018 to October 2018. Of the 407 participants screened for eligibility, 352 were consented and enrolled at baseline (86.48%; n=175 control, n=177 intervention; figure 1). A total of 312 participants were retained at 3-month follow-up and included in subsequent analyses (88.64%, n=155 control, n=157 intervention). Commonly cited reasons for loss to follow-up were inability to return (n=16), relocation (n=11) and inability to contact using safe contact information (n=10). Three participants asked to discontinue the study. One participant completed baseline data collection but did not complete the intervention; per intention to treat, she was included in the difference-in-difference analysis. Attrition was non-differential on baseline demographics and IPV severity; retained participants were significantly (p<0.05) more likely to report depressive symptoms consistently and report their abusive partner had concurrent partners.

Consolidated Standards of Reporting Trials.
Participants were predominantly married (84.94%; table 1) and cohabitating with their partner (85.90%), with a mean age of 26.52 years old (SD=4.70) and 2.06 children (SD=1.14). Slightly more than half (51.28%) had completed primary school or less and the vast majority (94.23%) were unemployed. Randomisation achieved equal distribution by group.
Participant characteristics at baseline by study arm (n=312 retained)
Immediately post intervention, safety preparedness was higher for intervention participants as compared with control (36.05 vs 34.52; b=1.42; p<0.05; table 2), controlling for baseline decisional conflict. For use of helpful safety strategies, a group by time interaction was identified (binteraction=0.43; p=0.004), reflecting increases in the intervention arm (bintervention=0.40; p<0.001). Results were null on decisional conflict overall, which decreased in both groups; an intervention effect was identified for the uninformed decisional conflict subscale (binteraction=−1.52; p=0.03). Intervention results were null for IPV including the CTS summary score, physical violence, sexual violence, both physical and sexual violence, and reproductive coercion, with both groups reporting decreases over time (p<0.05). Emotional abuse showed a group by time interaction effect (binteraction=3.33; p=0.01) favouring the control arm, prompted by decreases in the control arm (bcontrol=−4.78; p<0.001) and sustained emotional abuse in the intervention arm.
Difference-in-difference analysis for primary and secondary intervention outcomes (n=312)
In secondary outcomes, resilience demonstrated a non-significant trend favouring the intervention (binteraction=2.13; p=0.06). Intervention results were null for safety-specific self-efficacy, which increased for both groups, and depression scores, which decreased for both groups. No between-group changes were observed in considering or seeking services, self-blame, recognition of abuse or general self-efficacy. For relationship quality, an interaction effect was observed favouring the control group (binteraction=−0.8; p=0.05), reflecting a greater increase in relationship quality for the control group. Risk for severe/lethal violence, assessed for intervention participants only, reduced over the 3-month follow-up (11.58baseline; 10.78followup; bintervention=−0.80; p<0.01).
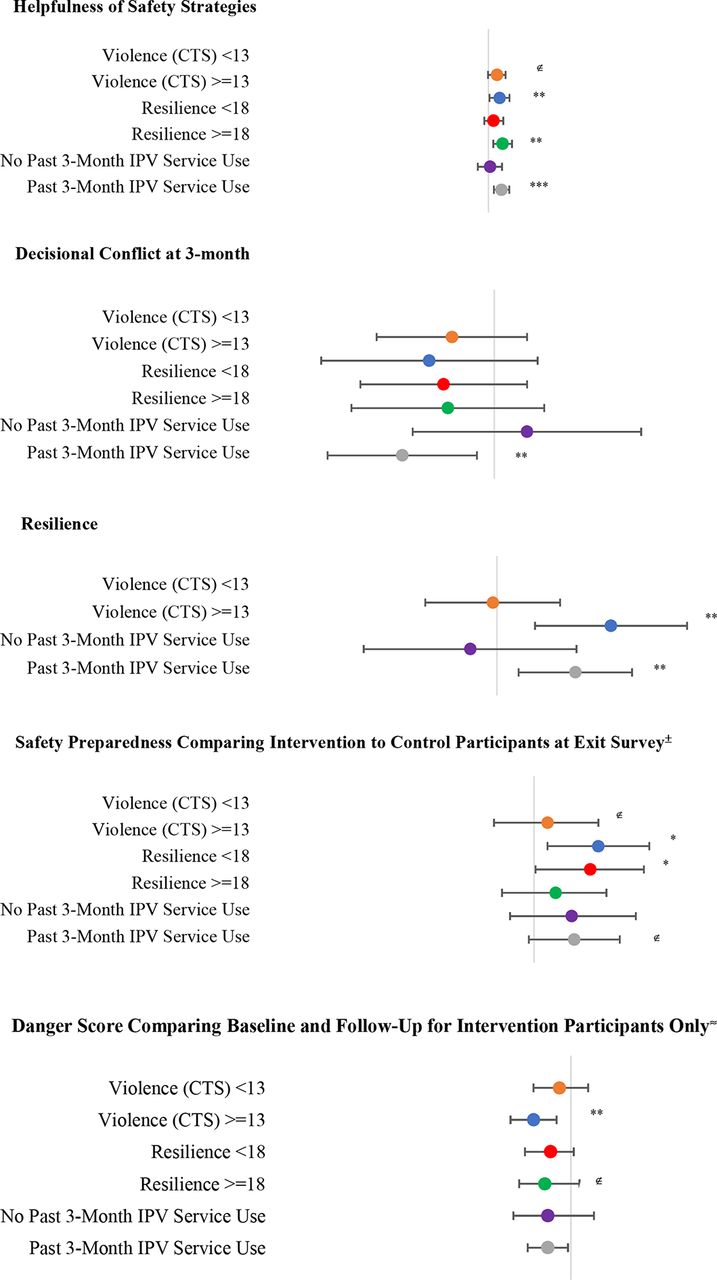
Among participants exposed to multiple forms of IPV (CTS >=13; figure 2), significant time by group interaction effects were identified for helpfulness of safety strategies used (p<0.01) and resilience (p<0.01); immediate post-intervention safety preparedness was significantly higher for intervention participants relative to controls (p<0.05), and risk for severe and lethal violence declined significantly from baseline to follow-up (p<0.01) in the intervention group. In results stratified by past 3-month service use at baseline, improvements in helpfulness of safety strategies used, decisional conflict and resilience were concentrated among participants who had previously sought IPV-related services (all p<0.05), with no significant time by group interaction effects identified among participants who were IPV-service naive.

{kind=link}
{kind=link}
Regression Coefficients and 95% CIs Stratified by Baseline Violence Severity, Resilience, and Past Three-month IPV-related Service Use Line indicates regression coefficient relative to line value of "1". Betas from interaction term in difference-in-difference linear regression unless noted; ∉=p<0.10; *=p<0.05; **=p<0.01; ***p<0.001. ±Linear regression comparing intervention to control group for exit survey safety preparedness, adjusting for baseline decisional conflict and site ≈Linear regression comparing baseline and follow-up for intervention participants only.
Qualitative findings
Participants described their impressions of the intervention, the usefulness of intervention safety strategies, intervention strengths and challenges-specific IPV resources and areas for intervention improvement.
myPlan impressions
App strengths
In considering intervention impressions, many women referenced strengths including its tailoring of their personal situation, and the availability of options that supported safety while staying in relationships, recognising the barriers to terminating relationships even in the presence of violence.
All that was being discussed in regard to myPlan app related to me. It was exactly my situation then. It was like hearing my own story. I was reading through and seeing just how it was resonating with my life and at the same time offering me guidelines and important information regarding my situation.
—21 years, Huruma
I am just happy about this study, it has helped me in big way. I have learnt how I can stay with him so that the violence and abuse is mitigated.
—32 years, Korogocho
Another strength was that working through the myPlan app with a CHV provided women an opportunity for relief from isolation and stress.
Here you are free to express yourself about your life. You cannot speak up when you are in the community but here you can and I can open up to you and you can assist me.
—35 years, Dandora
Post-intervention safety strategies
Children and safety
Women explained the most helpful strategies related to safety and well-being of their children.
I liked those ones involving children’s health. I understood that issue the way it was explained in the study. I thought back to the time I was going through a hard time. My kid got to a point where he developed ulcers. I felt that my child’s health was affected…[so] I felt that that strategy was important… if you only prevent physical harm, there may still be emotional harm.
—29 years, Huruma
Speaking up about abuse
Women explained that the intervention experience enhanced their ability to disclose violence to trusted friends and family. Though confidants were not always helpful, women gained confidence in reaching out for help.
When I came here, I got good at speaking up. I confide in my parents or even his or my friends because it will be beneficial.
—26 years, Dandora
There are times when you are stressed, you don’t have to keep it to yourself, you need to pay your friend a visit and have a casual conversation to eliminate that stress.
—24 years, Korogocho
De-escalation
Women explained that persevering in the face of IPV was common pre-myPlan Kenya. Post intervention, women described using de-escalation tactics, such as choosing not to engage with a drunk or upset partner, and temporarily leaving to provide physical space.
Now, when he comes home, I study his mood so that I know how to handle him in order to avoid the chaos. While talking to him, you can know from his reactions that it will lead [to] violence. You need to wait for him to cool down before talking to him. If I see he is unhappy when he comes home, I normally keep quiet until he starts a conversation.
—35 years, Dandora
In regards to my safety, when he seems like he is spoiling for a fight, I would stay away from him and come back when he has calmed down.
—34 years, Korogocho
Financial independence
Strategies related to supporting financial independence were described as useful in reducing monetary-driven arguments and provide peace-of-mind surrounding provision of basic needs for themselves and their children.
I decided to find some little money and start selling clothes. This has really helped me. I can buy food for my children, unlike when I used to just wait for my partner; at times he would come and say he did not have money for food and beat me up.
—25 years, Huruma
IPV support services and referrals: strengths and challenges
Women described important gains in knowledge about available services as a result of the intervention.
I did not know that there is a way for women who are in trouble. You can be directed to people who can assist you. I knew that once you are assaulted, that’s it, life ends there. After going through myPlan, I learnt that there are facilities and steps that can be taken in case you have a problem in your marriage.
—33 years, Korogocho
Simultaneously, women’s chief concerns with the intervention centred on the helpfulness of resource referrals, reflecting gaps in the underlying IPV response community. While most services were welcomed, participants cited past negative experiences with law enforcement in particular, and questioned the value of including law enforcement as an option for IPV response.
So when I went to the police. Since [my partner] has money, he was able to bribe them and was set free and the police did not pursue the case. When I took him to the chief, he bribed the chief…[I have gone to the police and chief] about four times now. I got tired and gave up.
—30 years, Korogocho
The security purpose where you’re being told have you visited government help like the chief? You’re not supposed to put that chief. They have no use. They don’t help women.
—27 years, Dandora
Several participants also suggested including churches as referral resources.
Additional challenges & recommendations: ensuring high-quality communication
Women’s recommendations for improvement centred on ensuring access for low literacy populations as well as those whose native language is neither Swahili nor English. They recommended audio or in-person assistance to support communication.
Triangulation of qualitative and quantitative results (table 3) identified areas of convergence as well as divergence. Results related to decisional conflict and safety strategies converged across quantitative and qualitative results, with qualitative findings adding nuance to quantitative evidence of improvements in aspects of decisional conflict and use of helpful safety strategies. Results diverged in domains of IPV experience and services. Specifically, IDIs described helpfulness of the app in mitigating abuse, yet quantitative results showed decreases in IPV in both arms. IDIs indicated relevance of IPV-related referrals and importance of confidence gained for garnering support; however, quantitative results were null with regard to IPV-related services.
Triangulation matrix of quantitative and qualitative results
Discussion
This study represents the first longitudinal trial of the adapted myPlan Kenya safety decision and planning intervention delivered via a secure app to survivors in Nairobi, Kenya. Women who used the myPlan Kenya app had significantly improved safety preparedness immediately post intervention compared with the control group. At 3-month follow-up, intervention women had a greater increase in use of helpful safety strategies and felt they had information needed to make safety decisions, both aligned with the intervention’s theory of change. There were no significant between-group differences in IPV or depression, likely reflecting the relatively short follow-up duration, which contrasts with the dynamic and lengthy process of decision-making, safety planning and achieving longer term safety for women in abusive relationships. Among women reporting more violent and abusive behaviours by the partner at baseline, women in the intervention group reported significantly greater resilience and helpfulness of the safety strategies they used relative to control participants. Among women who had previously sought services for IPV, intervention women reported improvements in resilience and helpfulness of safety strategies and a reduction in decision conflict about safety. These endpoints are important on women’s trajectories towards safety, and suggest that the intervention can be valuable for bolstering change in safety even for those already in touch with services. Results provide promising efficacy evidence for the myPlan safety decision and planning intervention with IPV survivors in an urban, low-resource settlements.
Findings affirm the value of human-centred design in appropriately adapting technology to context. Technology-based interventions are often falsely contrasted with people-powered interventions, with the implication that technology-based interventions can replace skilled advocates and providers. This intervention is distinct from a static webpage or app in that it is evidence-based, tailored, codesigned with survivors in local languages. Further, it contains extensive safety features and is delivered through technology appropriate to the context. Our human-centred design phase revealed that the most appropriate app delivery method was with support trained lay professional CHVs; this was found acceptable and appropriate for both parties. The resulting intervention achieved results comparable to those from trials in high-income settings.19–21 Our technology adaptation process and supported app implementation may be relevant for other lower resource settings where the rapid expansions in mobile accessibility have not yet been matched in technology literacy and comfort for some populations.
Results stratified by past IPV service use are particularly informative in understanding women’s processes of behavioural change. The intervention was effective in reducing decisional conflict and improving resilience for women who had previously sought IPV-related services. Prior service use may be a marker for readiness for change; alternately myPlan Kenya, tailored to the survivors’ situation, may have amplified, extended and/or reinforced the availability and value of IPV services and working closely with skilled advocates and providers. Results illustrate that app-based safety planning tools constitute a valuable element of comprehensive IPV prevention and support services, and function in part by enhancing connection to existing services, and extending the value of existing services. They are by no means a replacement and will function best when effectively integrated as one of many options.
Other IPV prevention trials have reported IPV decreases in both groups.20 The structured baseline assessments may have conferred benefits; however, there were no overtime changes in either group in self-blame, recognition of abuse, nor consideration nor uptake of IPV-related services. Qualitative results speak to intervention acceptability and its impact on recognition of services and reduced isolation. The divergence of qualitative and quantitative results for IPV and IPV-related services suggests that quantitative study measures may not have been sufficiently sensitive. Both groups improved modestly on safety-specific self-efficacy, which could contribute to enhanced safety. A longer follow-up period is warranted to clarify intervention effects on longer term outcomes of safety and mental health, as well as durability over time. This trial conducted in a controlled environment did not support questions related to dose viewed and dose–response as they relate to primary and secondary outcomes; both are important future research questions.
Strengths include successful randomisation, adherence to protocol with 88% retention, qualitative interviews with intervention participants and no reported adverse events. Study measures were refined by the community-partnered study team. Limitations include the 3-month follow-up duration and the limited generalisability with recruitment in a single city. Several important measures demonstrated limited performance, specifically subdomains of the decisional conflict scale, as well as the self-blame assessment; these results should be interpreted with caution and further work is needed to strengthen measurement in these areas. The community-based recruitment may have limited reach to the most vulnerable women, including those fearful of seeking help from CHVs.
Trial results are comparable to those in high-income countries19–21 in demonstrating improvements in safety preparedness, decreases in aspects of decisional conflict about safety, and increases in use of helpful safety strategies following this intervention. Further, among women reporting severe IPV, those in the intervention group reported increased resilience and reduction in risk for lethal violence. The innovation here is twofold. First, safety decision-making and planning interventions codesigned with IPV survivors in local languages, with extensive safety features, and delivered through technology appropriate to the context are similarly effective in this LMIC-based urban settlement as in high-resource settings. Second, myPlan Kenya app is acceptable and feasible for use by survivors with support from a trained lay professional, in a private location in a community-based organisation. Findings advance the evidence base on IPV prevention and response tools for diverse settings with high IPV prevalence and limited advocacy and support services.
Acknowledgments
The authors gratefully acknowledge the study participants and local stakeholders for their time and input in this endeavour.
References
Footnotes
Handling editor Seye Abimbola
Contributors MD and NG designed this study. MD, ZH and SW drafted the paper. NG, MD and AC designed the intervention content. NAP provided power calculations and analysis oversight. BA ran the project in the field, with CT, IA, IW and SRK responsible for recruitment, intervention adaptation, piloting and formative work. SW led analysis. ZH, SRK and AF led training, protocol development, data quality, technical support and structured community input. BO contributed to the conceptualisation of the trial and facilitated interaction between the teams on scientific issues. RO and MM identified and facilitated connection with field partners. JC conducted all study-related programming including the intervention app and randomisation. All authors contributed to the drafting and critical review of the manuscript, and reviewed the final draft.
Funding This study was funded by Ideas42 (PI Decker).
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting, or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval The Johns Hopkins Bloomberg School of Public Health Institutional Review Board and the Kenya National Commission for Science Technology and Innovation approved the protocol.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request. The authors will make data available to scientists planning specified and agreed further analyses; for access, contact the corresponding author.