Article Text

Abstract
Introduction Results-based financing (RBF) is being promoted to increase coverage and quality of maternal and perinatal healthcare in sub-Saharan Africa (SSA) countries. Evidence on the cost-effectiveness of RBF is limited. We assessed the cost-effectiveness within the context of an RBF intervention, including performance-based financing and conditional cash transfers, in rural Malawi.
Methods We used a decision tree model to estimate expected costs and effects of RBF compared with status quo care during single pregnancy episodes. RBF effects on maternal case fatality rates were modelled based on data from a maternal and perinatal programme evaluation in Zambia and Uganda. We obtained complementary epidemiological information from the published literature. Service utilisation rates for normal and complicated deliveries and associated costs of care were based on the RBF intervention in Malawi. Costs were estimated from a societal perspective. We estimated incremental cost-effectiveness ratios per disability adjusted life year (DALY) averted, death averted and life-year gained (LYG) and conducted sensitivity analyses to how robust results were to variations in key model parameters.
Results Relative to status quo, RBF implied incremental costs of US$1122, US$26 220 and US$987 per additional DALY averted, death averted and LYG, respectively. The share of non-RBF facilities that provide quality care, life expectancy of mothers at time of delivery and the share of births in non-RBF facilities strongly influenced cost-effectiveness values. At a willingness to pay of US$1485 (3 times Malawi gross domestic product per capita) per DALY averted, RBF has a 77% probability of being cost-effective.
Conclusions At high thresholds of wiliness-to-pay, RBF is a cost-effective intervention to improve quality of maternal and perinatal healthcare and outcomes, compared with the non-RBF based approach. More RBF cost-effectiveness analyses are needed in the SSA region to complement the few published studies and narrow the uncertainties surrounding cost-effectiveness estimates.
- maternal health
- child health
- health economics
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
There is increasing evidence that results-based financing (RBF) can promote service use and quality of maternal and neonatal care.
Little evidence exists ascertaining whether RBF interventions provide value for money in low-income and middle-income countries.
What are the new findings?
Introduction of RBF with some infrastructural support is likely to cost about US$1122 per disability adjusted life year averted.
What do the new findings imply?
At high thresholds of willingness to pay, RBF is likely to be a cost-effective intervention to promote maternal and neonatal health in Malawi.
More evaluations are merited to explore cost-effectiveness of different RBF schemes and to reduce uncertainties around cost-effectiveness estimates.
Introduction
Identification of policies and strategies that can increase coverage of pregnant women and newborns with priority maternal and newborn health (MNH) services is one of the main challenges on the global health agenda.1 Although sufficient evidence exists on MNH interventions that are effective and appropriate for implementation, population coverage remains suboptimal in low-income and middle-income countries (LMICs), especially among the poor.2 Consequently, for 2015 in sub-Saharan Africa (SSA) alone, 1 million babies were stillborn,2 approximately 0.8 million newborns died within 7 days of birth,3 4 while 201 000 women died from pregnancy-related complications.5 The majority of these deaths could have been prevented by improved coverage of mothers and newborns with existing effective MNH interventions.1 6
The SSA region has the highest maternal mortality ratio (546 per 100 000 live births) and perinatal mortality rate (56 per 1000 births) in the world.7 8 In order to increase population coverage, to narrow disparities between income groups and to reduce maternal and perinatal mortality, many countries in the region are investing in innovative strategies to enhance health system performance.9 Strategies such as results-based financing (RBF), including both performance-based financing (PBF) and conditional cash transfers (CCTs), are currently being rolled out.10
RBF consists of monetary or non-monetary transfers made to national or subnational governments, managers, providers or consumers of health services contingent on verified attainment of predefined results.11 Within the context of MNH, RBF encompasses both supply and demand side mechanisms. On the supply side, PBF is designed to act by motivating providers to increase quantity and quality of provided care.12 On the demand side, CCTs are designed to lower financial barriers to access and modify consumers’ behaviours.13
There is growing evidence that under favourable conditions, RBF schemes can increase service use and quality of MNH care in the SSA region.14–16 However, little information exists on cost-effectiveness of RBF schemes,17 18 even though the assessment of the comparative efficiency of RBF schemes has been identified as a priority research area.19–21 Costing studies have reported high RBF operational costs raising doubts about the cost-effectiveness of these interventions.22 Given limited resources, RBF schemes compete for scarce funds with alternative strategies within the healthcare sector. It is therefore essential to assess their value for money. Cost-effectiveness information on RBF is important to support policy makers when making healthcare priority setting decisions.23 24
The objective of this study was to contribute towards filling this knowledge gap by assessing the cost-effectiveness of an RBF scheme compared with status quo care in reducing maternal and perinatal mortality. This study was conducted within the framework of a larger impact evaluation related to the implementation of Results Based Financing for Maternal and Neonatal Health (RBF4MNH) Initiative in Malawi.25
Methods
Study setting
Malawi is 1 of 30 countries in SSA implementing RBF.26 In 2013, the Malawi Ministry of Health (MoH), with financial support from the Norwegian Ministry of Foreign Affairs and the German Federal Ministry for Economic Cooperation and Development, initiated a 5-year RBF programme designed to improve coverage and quality of MNH services. Selection of facilities was based on capacity to offer emergency obstetric care (EmOC), make referrals and provide 24/7 delivery care in four districts: Balaka, Dedza, Mchinji and Ntcheu. Performance indicators focused on delivery care,27 Box 1. Implementation started in 18 out of a total of 33 EmOC facilities in April 2013 to October 2014 and then expanded to 28 facilities until 2017.28
Results-based financing core performance indicators
Number of facility-based deliveries.
Number of referrals due to complications at the time of delivery.
Maternal and newborn deaths properly audited according to national guidelines.
Pregnant women who arrive at the facility for delivery with unknown HIV status who are tested and treated for PMTCT.
Accurately and completely filled HMIS reports submitted on time to the district health office.
Up to date and complete stock cards of essential MNH medicines and commodities on the date of verification.
Accurate and complete RBF Initiative specific reports submitted to district health offices on time.
HMIS, health management information system; MNH, maternal neonatal health; PMTCT, prevention of mother to child transmission; RBF, results-based financing.
Maternal and neonatal care
MNH care in Malawi is provided at EmOC facilities and includes antenatal, delivery and postnatal care. Basic EmOC (BEmOC) facilities are expected to consistently provide a set of seven key interventions known as ‘signal functions’, while two additional signal functions are to be provided by Comprehensive EmOC (CEmOC) facilities.29 Health centres providing BEmOC are supposed to be capable of managing obstetric complications and to refer emergency cases requiring more comprehensive care to CEmOC facilities. MNH and EmOC services are provided free in public health facilities and private not for profit facilities contracted by the MoH through Service Level Agreements.
The intervention
The Malawi RBF Initiative, designed and implemented by the MoH, aimed to improve service quality of EmOC facilities using performance-based payments to health facilities and providers based on achievements of predefined quantity and quality targets (box 1), implying that RBF facilities had additional funding on top of centralised allocations (budgets, supplies). The RBF Initiative also used CCT to incentivise pregnant women to deliver at EmOC facilities instead of non-EmOC facilities or at home. To ensure that the providers at EmOC facilities operated within environments with the required capacity to provide quality MNH care, the RBF implementation was preceded by a one-off investment in infrastructural upgrades and equipment supplies. More details of the Malawi RBF Initiative are provided elsewhere.25 28
The comparator
In contrast to RBF-supported EmOC facilities, non-RBF EmOC facilities (comparator) neither received funding beyond centrally allocated budgets nor any explicit infrastructural upgrades.
Analytic overview
We used a decision tree model to calculate the expected health effects and expected costs of the RBF4MNH Initiative from a societal perspective.30 The model simulates maternal and perinatal outcomes from 28 weeks gestation until 7 days after delivery. This period is consistent with the definition of perinatal outcomes in developing settings.31 32 Importantly, it captures the majority of maternal deaths, which occur during the third trimester and the first week after birth.33 We considered two alternatives: the RBF4MNH Initiative and status quo care (comparator). We used the model to estimate deaths averted, life-years gained (LYG) and disability adjusted life years (DALYs) averted from perinatal and maternal complications, as well as the additional (incremental) costs incurred by the RBF programme. The model was populated with information on population coverage with facility-based delivery (FD), the incidence of maternal complications, cause-specific maternal case fatality rates (CFRs), time to seek care for complications and effective coverage (parameter details are explained below).
Malawi-specific estimates for life expectancy at birth and life expectancy at the mean age of women of reproductive age were used to calculate LYG34 for each perinatal and maternal death averted, respectively. Future LYG and DALYs were discounted at 3%23 in the baseline scenario, while the influence of no discounting of future health was explored in sensitivity analysis.
Each alternative was simultaneously fitted with associated treatment costs, including RBF costs for the intervention arm. The costs are presented in 2013 US$. We calculated incremental cost-effectiveness ratios (ICERs)35 in terms of cost per DALY and death averted and per LYG. The ICER is the difference in costs between two interventions divided by the difference in their effects.36 An intervention is considered cost-effective if its ICER in US$ per DALY averted is less than three times gross domestic product (GDP) per capita and considered ‘very cost-effective’ if its ICER is less than the per capita GDP.37 Applied to the Malawian context, the RBF intervention would be considered cost-effective as long as it costs less than US$1485 per DALY averted and very cost-effective if it costs less than US$495 per DALY averted.38
Finally, deterministic and probabilistic sensitivity analyses were conducted to assess important drivers impacting the ICERs and the robustness of the model to variations in key parameter and model assumptions.
The decision model
Reflecting the options decision makers face, the decision model included two arms: RBF and non-RBF (comparator). Policy makers decided which facilities received RBF while mothers decided whether to deliver in an RBF health facility, a non-RBF health facility or at home. In the model, mothers’ decisions/service use parameters were based on primary trial data. Mothers who delivered in RBF facilities benefited from the intervention (combination of PBF+CCT) while those who delivered in non-RBF facilities only received status quo care.
For each delivery, we accounted for both perinatal and maternal deaths. We defined each delivery as normal or uncomplicated (not associated with any maternal complication) or complicated (associated with any maternal complication). Maternal complications included direct causes (haemorrhage, sepsis, obstruction, eclampsia) and/or any indirect causes. Each complication could lead to a maternal death or recovery. The model allowed for the fact that mothers experiencing normal deliveries may die from incidental causes.
Because some maternal complications can negatively affect perinatal outcomes, perinatal survival is linked to maternal survival.33 39 After a delivery event, the model therefore considered perinatal outcomes based on mothers’ status, that is, whether the mother was alive or dead. The outcome of the newborn (ie, stillbirth, early neonatal death, alive) was then assigned conditional on the status of their mothers. Figure 1A,B gives an overview of the decision model. The full model (available on request) was constructed using TreeAgePro 2016 software.
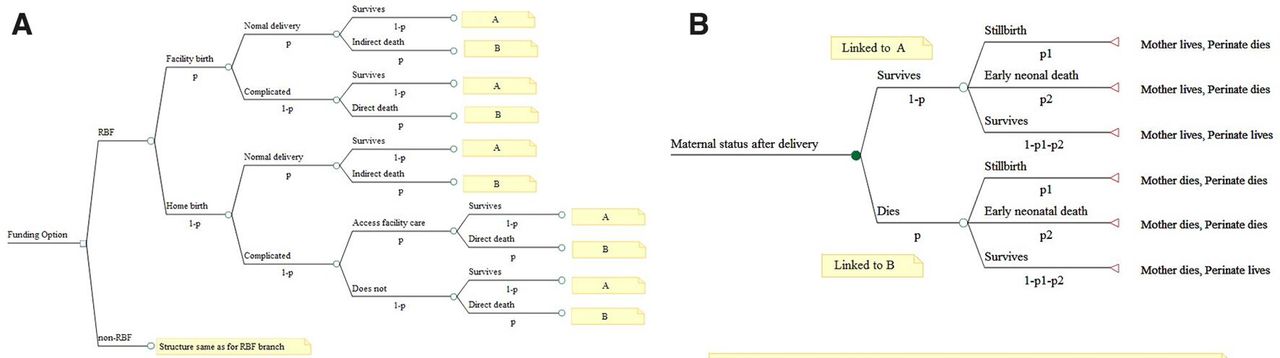
(A) Pathways of maternal events, demonstrating maternal status after delivery. (A) is linked to perinatal outcomes for live mothers. (B) is linked to perinatal outcomes for dead mothers as shown in (B). (B) Pathways of perinatal events, demonstrating conditional relationships between perinatal outcomes and maternal status after a delivery event. RBF, results-based financing.
Epidemiological data
The Malawi RBF trial25 28 was not designed to collect health outcomes data including case fatality or mortality rates. This lack of health outcomes data necessitated modelling. We therefore obtained epidemiological estimates of perinatal mortality, maternal complications and CFRs from the published literature to populate the corresponding probabilities in the model, assumed to be similar for both arms at baseline.
RBF effects on service use, quality and subsequent mortality reductions
At population level, maternal/perinatal survival depends on both coverage of pregnant women with FD services and timely access to quality obstetric emergency care.40 An impact evaluation of the RBF4MNH on service use did not demonstrate any significant differences in utilisation with facility delivery rates of 82.8% and 79.8% between RBF and comparison non-RBF facilities, respectively.41 Furthermore, obstetric care utilisation rates among women who developed complications outside health facilities were 78% and 75%, respectively.42 However, RBF was associated with significantly reduced mean time to care for women experiencing complications,42 which may translate into better survival. Importantly, the RBF impact evaluation detected significant improvements in effective coverage (ie, provision of higher quality care in respect to structural and process quality indicators, such as routine use of partographs, uterotonics for active management of third stage of labour and infection control).28 41
Similar efforts to improve the quality of obstetric care were associated with 25%–30% reductions in CFRs and 19%–20% reductions in stillbirth rates in Zambia and Uganda.43 Given similarity in MNH settings across these countries,44 we adopted the mean figures of 27.5% and 19.5% reductions in CFRs and stillbirth rates with RBF, respectively. Consistent with the Zambia and Uganda studies, we assumed that RBF had no significant effect on early neonatal mortality. Details of parameters used in the model and their sources are shown in table 1.
List of parameters used in results based financing compared with non-results based financing decision tree model.
Incidence of maternal complications
Information on incidence of maternal complications and respective CFRs is needed to calculate maternal deaths. There is wide variation in reported incidences of maternal complications even though countries by principle adhere to the same version of the International Classification of Diseases.45 A WHO multicountry survey estimated that 7.3% of FDs in developing countries are associated with maternal complications.46 This is probably the most representative estimate; thus, we used it for the baseline scenario. For home births, we assumed that the percentage of complicated deliveries was 50% higher, given that most home deliveries are not assisted by skilled birth attendants in developing countries.47
There is lack of reliable data on case-specific incidences for sepsis, haemorrhage, eclampsia and obstruction.48 49 However, data on relative frequencies of these conditions among women with complications exist. In Malawi’s rural facilities, sepsis, haemorrhage, eclampsia and obstruction account for 32%, 32%, 20% and 11% of obstetric complications, respectively, while other direct/indirect causes account for the remaining 5%50 (table 1). We thus estimated cause-specific incidences indirectly, by multiplying the relative frequency of each condition with the overall incidence of maternal complications. Overall incidence of other direct/indirect causes was estimated in a similar way.
Maternal mortality
Regarding maternal CFRs, wide variations exist in data for the SSA region. A review of recent estimates (year 2000 onwards)49 reported that facility based CFRs range from 3.6% to 18.0% for sepsis;51 52 2.8% to 12.3% for haemorrhage;52 53 3.4% to 18.0% for eclampsia51 52 and 2.0% to 12.7% for obstruction.51 54 We used the mean estimates as baseline estimates of CFR and tested the whole ranges in sensitivity analyses to reflect this diversity of CFRs across SSA settings. As no corresponding data exist for women experiencing indirect complications and among home births, we adopted the mean CFR (0.09%) to identify deaths due to complications from other/indirect causes and during home births (table 1).
Though rare, women can have comorbidities or experience more than one complication, raising the problem of competing mortality risks.55 The model applies cause-specific incidences concurrently, on the assumption that the risk of each maternal complication is independent from the risk of other complications. Mortality risk for non-maternal causes was approximated by subtracting annualised life time risk for maternal death (0.0008) for women of reproductive age (15–49 years)56 from annualised all-cause mortality risk (0.0048) for women aged 25–29 years.34
Perinatal mortality
We calculated perinatal deaths by combining the risk of stillbirth and early neonatal mortality with information about the status (live or dead) of the mother after delivery. The international literature estimates stillbirth and early neonatal mortality rates at 28.4/1000 births and 19.3/1000 live births, respectively, among a population-based cohort of mothers that survive births in LMIC.39 For mothers that die soon after births, the estimated stillbirth and neonatal mortality rates are 318.8/1000 births and 89.9/1000 live births, respectively.39 As perinatal mortality risks following incidental maternal deaths are not linked to maternal complications, we assumed they are the same as for normal deliveries. We transformed these rates into corresponding probabilities57 (table 1).
Adjusting perinatal risks by place of delivery
Individual studies in SSA report mixed results on risk of perinatal mortality by place of delivery; some studies find that the risk is lower for FDs58–60 while others report lower risks for non-facility based deliveries.61 62 We based our perinatal risk adjustment on a meta-analysis that pooled results from population-based cohort studies in SSA.63 The study reported an OR of 1.21 in perinatal deaths for non-facility based compared with facility-based births. This was transformed into corresponding relative risk.64
Disability adjusted life years estimation
DALYs are the sum of years of life lost (YLL) due to premature mortality and the years lived with a disability (YLD),65 DALY=YLL + YLD. Maternal YLL were estimated as the number of maternal deaths multiplied by the life expectancy at 25 years using Malawi life tables.34 Similarly, perinatal YLL were estimated as the product of perinatal deaths and the life expectancy at birth. Maternal YLD were estimated by multiplying prevalence of maternal complications by their corresponding disability weights65 (table 1). Since disability weights for eclampsia and other maternal conditions are not available,66 we adopted the mean disability weight of haemorrhage, sepsis and obstruction (0.260) for eclampsia and 0.133 for other maternal conditions66 assuming that most of them would be related to infections given the high infectious disease prevalence in the SSA region.67 Perinatal YLD were not estimated due to lack of data.
Cost data
We collected health systems and RBF4MNH programme costs from four health centres. We randomly selected two districts, and within each district, randomly selected an intervention and a comparison health centre. From these, we collected cost data twice, in 2014 and in 2015, to cover two separate fiscal years. Given some differences in actual timing of RBF implementation between intervention health centres, the periods of data collection were not identical.
We used the World Bank RBF toolkit to guide cost data collection.68 We defined costs as variable (changing with service volume) or fixed (not changing with service volume). For variable costs, we used an ingredient approach to estimate unit costs.23 At the health facilities, we identified and recorded quantities of resources used for maternal and new-born care. We used pharmacy and inventory records to quantify drugs and other supplies. Unit prices were obtained from Malawi Central Medical Stores catalogue or local retailers as appropriate.69 Information on utilities, building maintenance were either collected at the health facilities or respective district offices, depending on where complete records were available. RBF data on incentives, training, information and communication materials, equipment supplies, upgrades and supervision were collected from both RBF desk officers at the health facility and/or the main RBF office at the MoH Reproductive Health Unit. We used the consumer price index to convert prices into 2013 constant prices before discounting them at 3%.23
For fixed costs (building and equipment), information on useful life years and replacements costs was obtained from MoH Planning and Policy Directorate and from the National Health Accounts.70 We annualised and discounted the fixed costs at 3% rate and used a top-down approach to allocate joint or shared costs using allocation proxies.23 For instance, we used the proportion of maternity unit area relative to the area of all hospital units to allocate building costs to the maternity unit, while we used the share of maternity unit clients among all visits to allocate health worker salaries. An implicit assumption of the latter is that resource requirements of the maternity unit are equal to the average resource requirement of all facility activities.
We used facility registers and human resource records to find information on births, staffing levels and cadres. Costs related to administrative support from the district offices were not collected, on the assumption that they would not substantially differ between health centres. We estimated RBF personnel costs, office rentals and other overhead costs from the central office by inflating all RBF costs by 38.8%. In this way, the overall RBF administrative costs account for 28% of total implementation costs, which is consistent with a pay for performance programme in Tanzania.22 Household costs, including direct and indirect costs, associated with care seeking were based on our earlier analyses.42 Local currency values were converted to US$ equivalents using the 2013 midyear exchange rate (US$1=MK 330).
Sensitivity analyses and parameter uncertainty
We first explored the impact of each model parameter on ICERs through one-way sensitivity analyses.71 We varied the mean of each parameter over appropriate reported ranges. We used normal approximation methods to estimate ranges for binomial parameters in cases where corresponding CIs were not provided.72 In the absence of empirical estimates, parameters were varied ±20% (table 1). The 10 parameters that influenced the ICERs most were further assessed through probabilistic sensitivity analyses after assignment of appropriate distributions. Gamma distributions were specified for costs, normal distribution for LYG, lognormal distributions for probabilities and Beta distributions for service use.30 Bounds for the parameters were derived using methods of moments.30 We conducted parametric bootstrapping based on 5000 iterations to propagate parameter uncertainty through the model and presented the results as cost–effectiveness scatter plot and acceptability curves. At any given value of willingness to pay, acceptability curves show the probability of an intervention being cost-effective relative to the comparator.
Model validation
We validated the model by comparing baseline perinatal mortality rates with estimates from the published literature (internal validity) and by inspecting that all parameters influence the model according to expectations (face validity).
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting, or dissemination plans of our research.
Results
Costs of RBF
The estimated economic cost per delivery at an RBF facility was US$44 or about five times the cost for a comparison non-RBF facility. Most of the extra costs were RBF related, driven by new medical equipment investments, financial rewards and programme monitoring. RBF facilities tended to be larger with higher staffing levels. RBF facilities also had higher non-RBF related budget lines. A health worker in an RBF facility received US$420 annually as individual rewards. This amount varied by health worker cadre, with more qualified health workers (eg, nurse-midwives) receiving almost three times the reward amount compared with lower qualified health staff (eg, community health workers). Eligible mothers received US$6 on average in CCTs, of which more than 50% was used for reimbursing costs directly linked to institutional delivery (table 2 and online supplementary table 1).
Supplemental material
Facility characteristics and provider economic costs (US$)
Cost-effectiveness of RBF relative to non-RBF
The model estimated that RBF would avert one additional DALY (maternal and perinatal), one additional death (maternal and perinatal) and gain one additional life year (maternal and perinatal) at an incremental cost of US$1122, US$26 220 and US$987, respectively. Averted perinatal DALYs, deaths and LYG contributed most to the total effects (table 3).
Incremental cost-effectiveness ratios of RBF compared with non-RBF by outcomes
One-way sensitivity analysis
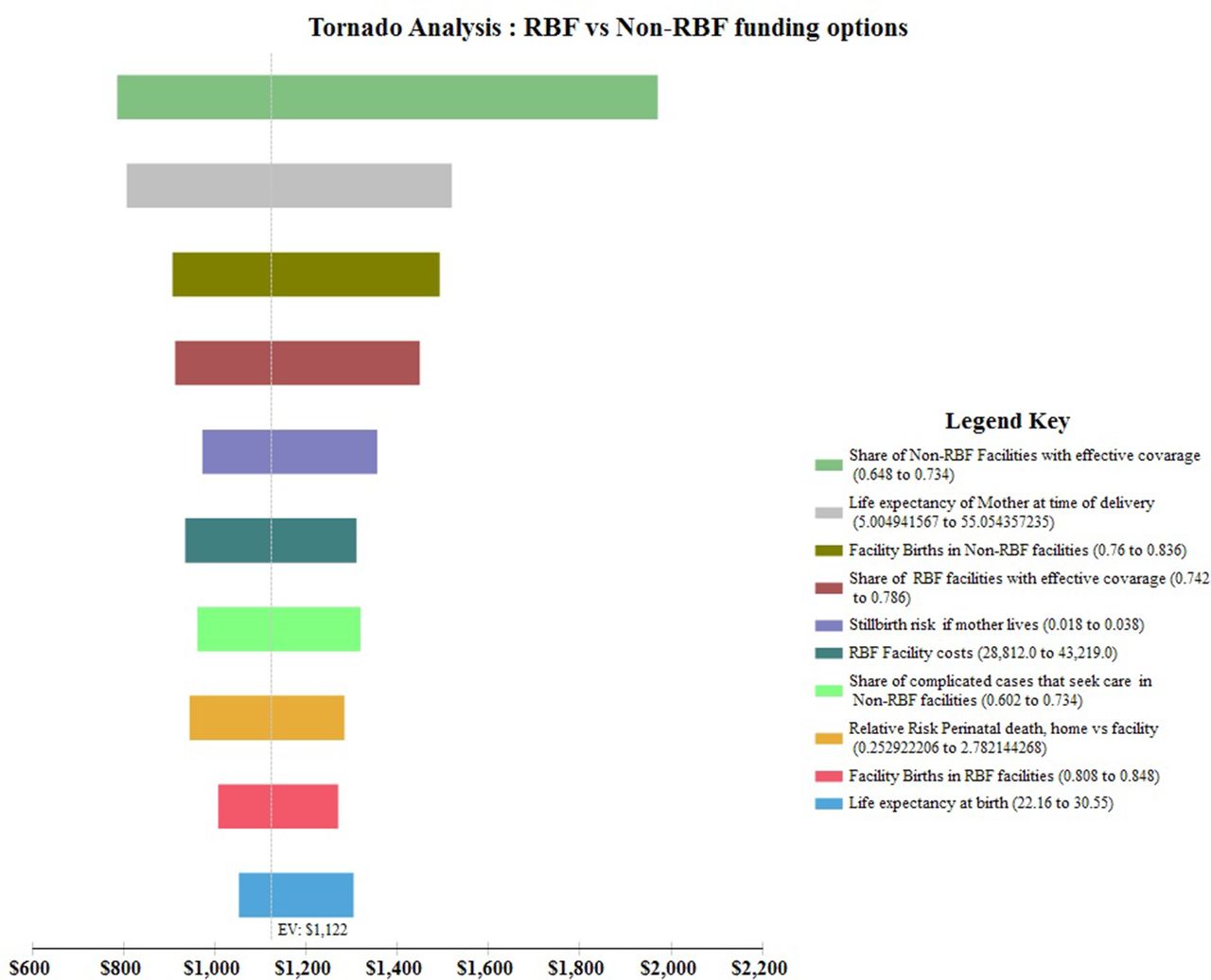
The share of non-RBF facilities providing quality care, the life expectancy of mothers at time of delivery and the share of births in non-RBF facilities had the strongest impact on ICERs for any DALY averted (figure 2). Relative to baseline, increases/decreases in the share of non-RBF facilities providing quality care would lead to more favourable/unfavourable ICERs while high/low life expectancies of mothers at time of delivery would be associated with unfavourable/favourable ICERs. The 10 parameters with most influence on RBF cost-effectiveness are shown in figure 2.
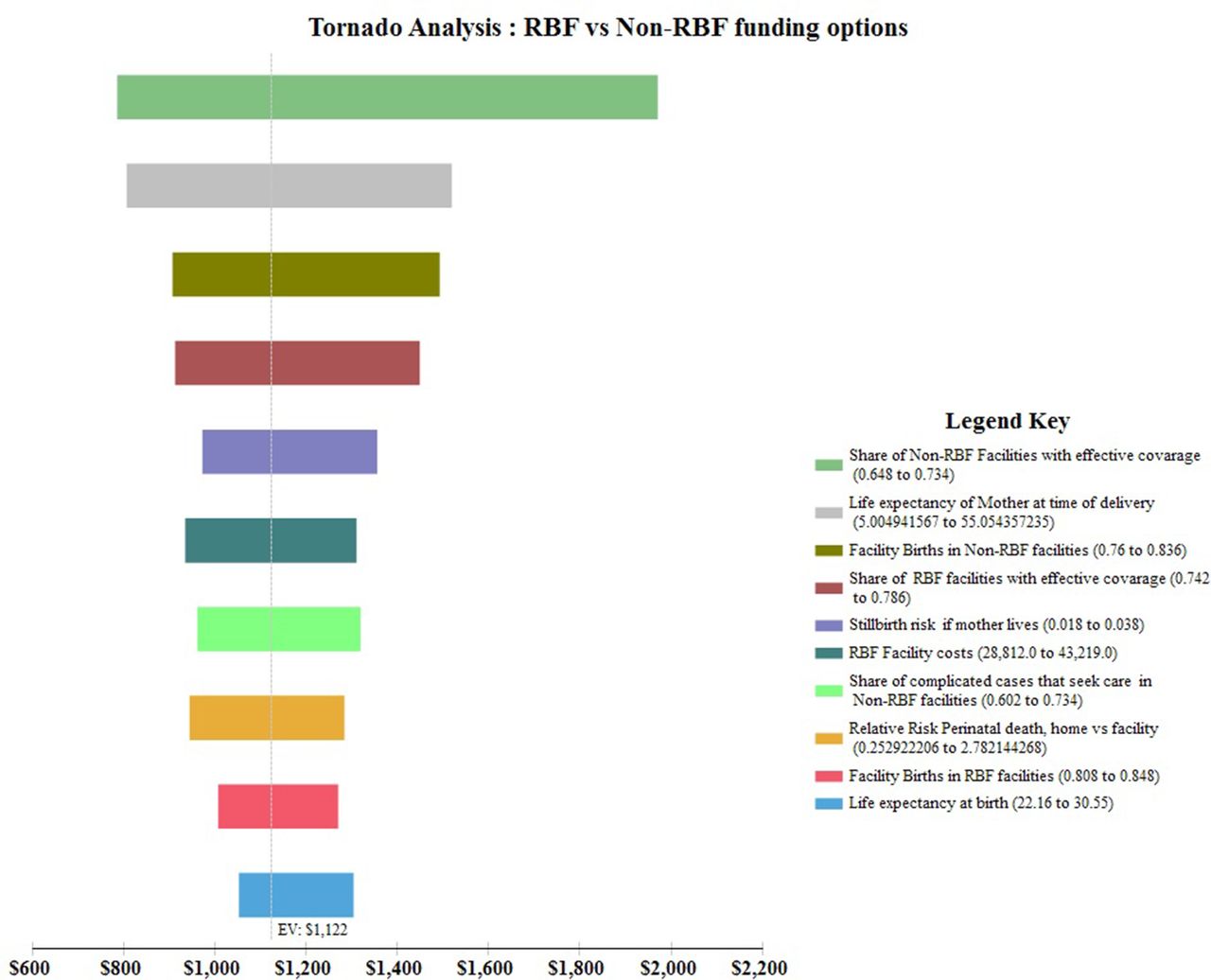
One-way sensitivity analysis showing variations in incremental cost-effectiveness ratios per disability adjusted life year averted. RBF, results-based financing.
Probabilistic sensitivity analyses
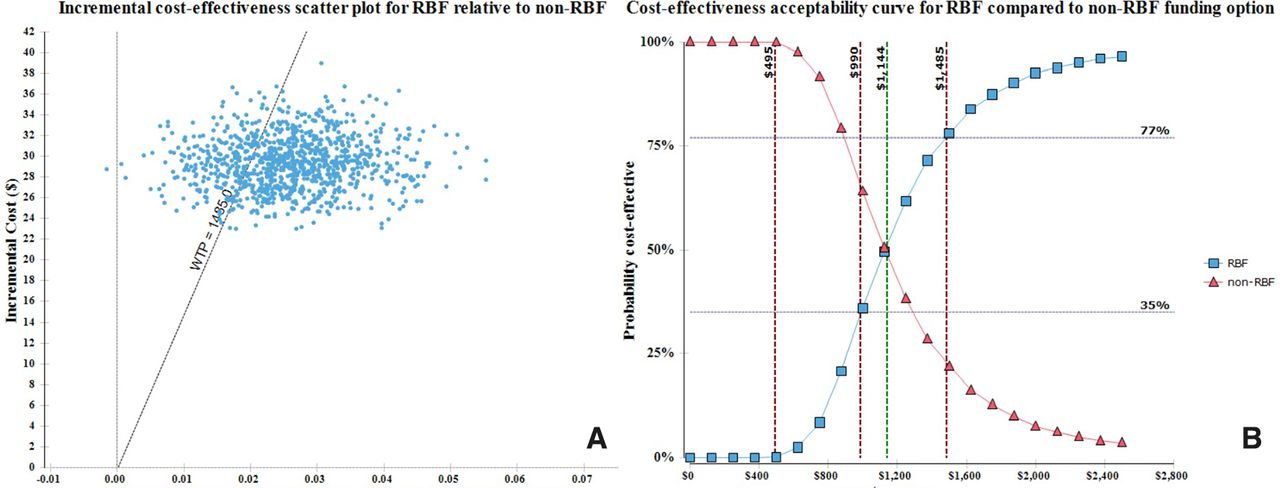
The ICER scatter plot illustrates that all iterations of DALYs for RBF relative to non-RBF consistently have positive costs, reflecting higher RBF costs with certainty. However, some have less (negative) DALYs relative to non-RBF, reflecting that the probability of overall lower health effects in the RBF arm relative to non-RBF cannot be completely ruled out (figure 3A). The probabilities that RBF is cost-effective compared with non-RBF at different levels of willingness to pay are shown in figure 3B. At a willingness to pay of US$495, US$990 and US$1485, (1X, 2X and 3X Malawi GDP per capita, respectively), RBF has a 0%, 35% and 77% probability of being cost-effective. At a willingness to pay of US$1144 per DALY averted, RBF and non-RBF have equal probabilities of being cost-effective. Thus, with a lower willingness to pay for health (<US$1144), non-RBF is most likely to be optimal, while at higher levels of willingness to pay RBF represents the more optimal policy.

{kind=link}
{kind=link}
{kind=link}
(A) Incremental cost-effectiveness scatter plot for RBF relative to non-RBF. (B) Cost-effectiveness acceptability curves for RBF compared with non-RBF funding option. RBF, results-based financing.
When deaths averted (maternal and perinatal) are used as a measure of health benefit, the threshold is at a willingness to pay of US$26 500 per death averted. For a lower willingness to pay, non-RBF remains optimal, while RBF is the policy choice with highest probability of being optimal when the willingness to pay for a life is higher than this threshold (online supplementary figure 1).
Supplemental material
Model validation
The model structure was informed by data availability and consensus view that it reasonably represents the situation on the ground. It estimates perinatal mortality rate of 47/1000 births in the baseline scenario, which is comparable to 56/1000 live births reported for the SSA region8 and 40/1000 live births estimate for Malawi.73
Discussion
This study demonstrates that an RBF intervention with a strong quality improvement component is probably cost-effective compared with status quo care. These results were produced in a context characterised by high levels of FDs and in the absence of significant changes in service use. Most of the health benefits resulted from averted perinatal deaths due to improvements in quality of care, underscoring the potential gains for newborn survival if RBF is rolled out.
This is the first full economic evaluation of an RBF (combining PBF and CCT components) intervention for MNH in a low-income country. We therefore have no relevant previous studies against which our results may be compared. When maternal or perinatal outcomes are considered separately, our ICER results are larger compared with findings by Alfonso et al17 for a voucher programme in Uganda, which reported an ICER per maternal death averted of US$20 756, which is 1/3 of the US$61 260 per maternal death averted in this study. This estimate however ignores the benefits in terms of perinatal health. Our ICER results are also larger than those published by Hounton et al74 assessing a health worker surgery training aimed at increasing access to EmOC in Burkina Faso, which reported an ICER per perinatal death averted of US$11 757. We estimated an ICER of US$45 841 per perinatal death averted, although this estimate ignores maternal health benefits. In Zambia, Zeng et al75 have reported an ICER of US$809 per Quality adjusted life year gained for a PBF scheme, but this estimate only considers financial costs. Compared with some specific MNH interventions including quality improvements efforts76 and new-born care,77 RBF has higher ICERs per DALY averted. However, RBF is a broader and more complex intervention, where capturing all effects is challenging. We find substantially lower ICERs when we combine both maternal and perinatal outcomes, confirming assertions that the cost-effectiveness of MNH interventions is underestimated if benefits are assessed separately, rather than jointly, for mothers and perinates.20
Because the RBF4MNH intervention appears more effective and also more costly than providing MNH care under status quo conditions, decisions to adopt it would depend on policy makers’ willingness to pay. At a willingness to pay of US$1485 per DALY averted, policy makers can be 77% certain that RBF is more cost-effective compared with status quo care. This confidence is reduced to 50% if we consider a willingness to pay of US$1144 and further reduces to 35% at willingness to pay of US$990 per DALY averted.
The choice of a new intervention is not based on cost effectiveness analysis (CEA) results alone but also on the capacity of resource-constrained governments to sustain its routine use.78 The implications for low-income countries like Malawi, where coverage gaps in other vital MNH interventions still remain, is that implementing new costly interventions based on the WHO threshold can only occur at the expense of displacing other interventions, thus risking lowering overall population health attainment and increasing health inequalities.79 Going forward, an important line of inquiry is therefore to conduct a budget impact analysis of the RBF4MNH. Besides ascertaining the affordability of RBF and potential dividends from economies of scale in case of scale up, such analysis may also offer needed insight regarding broader impact of RBF on other interventions.
Our model is sensitive to estimates of non-RBF facilities with effective coverage and share of births in non-RBF facilities (both directly influenced by quality of care) and life expectancy of mothers at time of delivery. Quality of care is important in RBF programmes and there are ongoing efforts to improve its measurement and reporting.80 The observed sensitivity underscores the importance of quality as it relates to health outcomes and that better data are needed to improve our model accuracy. The sensitivity to RBF costs is not surprising, given the financial outlays associated with RBF.81 It does nonetheless highlight the imperative to contain operational costs and improve programme efficiencies. Though the model is sensitive to the share of births in both RBF and non-RBF facilities, it is not as sensitive to the percentage of complications among facility deliveries (FD), which depends on FD coverage since women with complication self-select into care, especially when FD rates are less than 40%.82 As FD rates are variable in SSA, ranging from as low as 12% in Ethiopia83 to as high as 91% in Malawi,84 we postulate that cost-effectiveness of RBF may be strongly influenced by the share of obstetric complications at much lower FD rates than those obtained in Malawi. In this regard, CEA studies in different setting are required to contextualise findings.
We did not consider benefits from potential reductions in perinatal morbidity due to lack of quality data. Studies on MNH report a heavier morbidity burden due to disabilities than to mortality per se.85 Inclusion of averted perinatal morbidity would thus increase effectiveness and improve cost-effectiveness of RBF. Future CEA studies should account for the potential of RBF to reduce all disabilities.20
We observed large differences in rewards based on cadre. The size of financial rewards is assumed to positively influence performance86 while perceived unfairness in distribution of rewards may demotivate staff, undermining RBF objectives. Assessment of adequacy of rewards, perceived fairness in how rewards are shared and their impact on health system performance should inform future lines of inquiries.87
This study has limitations. First, estimates of RBF effects on stillbirths and CFRs were based on programme evaluations in Zambia and Uganda due to lack of randomised trial data. Intense monitoring and supervision under programme settings may have improved programme effectiveness, biasing our results downwards. We attempted to minimise this by using mean effectiveness estimates in the baseline scenario. Second, we were not able to account for maternal deaths that occurred before 28 weeks of gestation due to lack of data. The share of maternal deaths before 28 weeks is small and as early maternal deaths are not explicitly targeted by RBF, they may be assumed to be a constant that does not affect our estimation. Thus, we believe that this omission is less likely to substantially bias the effectiveness estimates. Third, the model considered diverse events and use of incidence in DALY estimation would have been more appropriate. We cannot ascertain how use of prevalence based approach affected our results but given use of similar approach by recent global burden of disease estimates,65 we believe our results can be trusted. Fourth, RBF was preceded by one-off infrastructural/equipment support. Disentangling the effects of such investments from the quality effects of RBF is problematic. Our results therefore represent the costs and effects of the combination of infrastructural improvements and RBF rather than RBF alone. Fifth, not all central level start-up costs were captured. This might have led to underestimating RBF costs. We attempted to characterise these uncertainties by using wide ranges (±20%) in probabilistic sensitivity analysis and found that the main results were stable across these ranges. Finally, GDP-based thresholds have been shown to be easily attainable and unconnected to local budget constraints;88 the reader should note this caveat when considering our results.
Conclusion
The RBF4MNH Initiative is a potentially cost-effective way to fund health facilities to improve quality of maternal and perinatal health, and to increase pregnant women’s access to EmOC, compared with the current non-RBF based funding in Malawi.
Although delivery services at RBF supported facilities are about five times as expensive per delivery compared with services offered at non-RBF facilities, we estimate that the intervention will avert 1.5% of perinatal and 12.1% of maternal deaths that occur with status quo MNH care in Malawi. The cost of US$1122 per DALY averted is lower than Malawi’s three times GDP per capita, which is one of the decision rules towards implementation.
More RBF CEAs are merited to explore cost-effectiveness of different intervention types, different health systems settings and health services and to reduce uncertainties around RBF CEA estimates related to modelling. Researchers in SSA should take advantage of the numerous RBF studies being implemented in the region to generate needed economic information to support policy decisions. Further, RBF studies should particularly prioritise generating more health outcomes data, while future economic evaluations should focus on identifying optimal RBF designs and implementation models that have lower transactional costs. This would allow to better assess the adequacy of different reward options and aspects of fairness in the allocation mechanisms to maximise individual health worker and team efforts.
Acknowledgments
The authors would like to thank Professor Don Mathanga and Dr Jacob Mazalale for their support during data collection. The authors are also grateful to Dr Matthias Arnold and the two anonymous reviewers for their helpful comments.
References
Footnotes
Handling editor Lei Si
Contributors JC and BR made substantial contributions to the development and design of the model. SB, MDA and AM provided substantial input to ensure model structure reflects situation on the ground. SB, AM and MDA made substantial contributions to acquisition of some of the data for the study. JC drafted the initial manuscript. All authors contributed substantially to the manuscript and interpretation of the data. All authors approved the final version of the manuscript to be published. The corresponding author attests that all listed authors meet the authorship criteria and that no one meeting the criteria has been omitted.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval for the study was obtained from University of Malawi, College of Medicine Research and Ethics Committee (COMREC) protocol P.02/13/1353.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.