Article Text

Statistics from Altmetric.com
Summary box
The past 20 years have witnessed an exponential growth in the global engagement of academic medical centres (AMCs) in the United States (US). In contrast to their global activity, US AMCs often do not adopt locally many of the evidence-based policies and practices adopted by the health systems of low-income and middle-income countries (LMICs).
Some of the best AMCs in the US (and arguably, in the world) are surrounded by communities where life expectancy and healthcare access are considerably worse than the national average and comparable to (if not worse than) those of many LMICs. Much like what happens when they engage globally, there are steps that the centres could take to maximise their impact locally.
These steps include: (1) include community health among the metrics by which the success of US AMCs is measured and alter financial incentives accordingly (2) establish/support public/community health departments/divisions; (3) establish multidisciplinary and multisectoral strategic partnerships; (4) prioritise capacity strengthening of local health stakeholders and sustainability; (5) increase diversity in composition of governance bodies and (6) establish hubs of innovation in health service delivery within surrounding communities.
Academic medical centres in the United States and global health
The past 20 years have witnessed an exponential growth in the global engagement of academic medical centres (AMCs) in the United States (US). According to the Consortium of Universities for Global Health, the number of US academic institutions (including AMCs) with global heath partnerships grew from 6 in 2001 to over 80 in 2018.1 Global health funding from the US government (primarily through the US President’s Emergency Plan for AIDS Relief) and from the Bill & Melinda Gates Foundation exceeded US$16 billion in 20182 3; US universities and AMCs were major recipients of this funding.
US AMCs engage globally primarily by devoting resources (funding and technology) and deploying expertise (faculty and students) to support research, training, and health service delivery in other countries, many of which are low- and middle-income countries (LMICs).
When abroad, US AMCs often accept policies and practices adopted by their partners in country (such as ministries of health and non-governmental organisations) and endorsed by WHO and other international organisations as the gold standard in global health. Among them are the integration of care between health facilities and communities, the pursuit of a multidisciplinary and multisectoral approach to complex health issues, and the establishment of strategic partnerships among different organisations. Together with their local colleagues, scholars and clinicians from US AMCs feature in several of the publications and reports that built the evidence base and consensus for these policies and practices.4–6
When abroad, US AMCs also opt to be accountable to the same health targets that their partners in country are accountable to. These targets are specific and concrete. Among them are the Joint United Nation’s Programme on HIV/AIDS (UNAIDS)’s targets for HIV, the 13 targets within the third of the Sustainable Development Goals (SDG3), and (at the country level) the targets established by local ministries of health.7 The accuracy of reporting for these targets is often compromised by the political and financial pressure that LMICs and their partners feel to show-case success. Additionally, even when the reporting is accurate, it might be difficult to determine whether and the extent to which a single organisation contributed to the targets. Despite these limitations, by being accountable to shared health targets, US AMCs send the important signal to their partners in country that they do not engage globally solely or primarily to gain organisational benefits, but to pursue a country’s health priorities and honour their organisational commitment to the greater good.
Increasing accountability and improving health locally: a missed opportunity
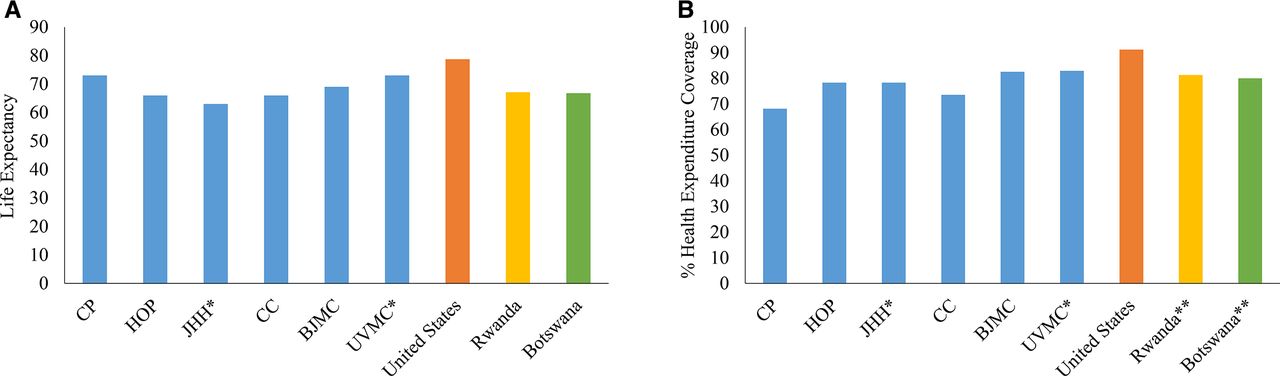
In contrast to their global activity, US AMCs often do not adopt locally many of the evidence-based policies and practices they accept in their LMIC work. This is a lost opportunity because LMICs have important lessons to teach to the US about maximising the impact of the available resources and expertise, delivering health services to the largest possible number of individuals and improving health outcomes for entire populations. Indeed, at the national level, the US lags behind many LMICs in the achievement of UNAIDS’s HIV targets and is currently not on track to achieve many SDG targets.8 9 Some of the best AMCs in the US (and arguably, in the world) are surrounded by communities where life expectancy and healthcare access are considerably worse than the national average and comparable to (if not worse than) those of many LMICs (figure 1).10 11 However, US AMCs rarely hold themselves accountable to shared health targets within their catchment areas.
{kind=link}
Lowest life expectancy (A) and health expenditure coverage (B) by census tract within the ZIP code area of major academic medical centres in the United States (US) vs national averages for the US, Rwanda, and Botswana.##Methodology: the academic medical centres (AMCs) listed in figure 1A,B were selected because they are located in major urban areas and had the most significant findings for life expectancy and health expenditure (insurance) coverage. The data for life expectancy and health insurance coverage were obtained from ‘500 cities: local data for better health’ (https://www.cdc.gov/500cities/). The values shown in figure 1A,B represent the lowest value by census tract within the ZIP code of the AMCs (each ZIP code contains several census tracts). The values related to health insurance coverage were determined by subtracting from 100%, the percent number for lack of health insurance in the census tract of interest. Lack of health insurance was presented as a percent interval between two values (ie, 24%–28.9%) in the original data source. We used the average between the higher and lower value for our calculations.*When the ZIP code area included only the premises of an AMC, data from bordering census tracts were also included.**Data for Rwanda and Botswana include only health expenditure coverage provided by government, not by private carriers. Rwanda offers a community-based health insurance to its citizens that covers a basic health package. In Botswana, reproductive health and antiretroviral treatment services are free to all citizens, while there is a small nominal fee for consultations for other services.BJMC, Barnes Jewish Medical Center, St Louis; CC, Cleveland Clinic, Cleveland; CP, Columbia Presbyterian Hospital, New York City; HOP, Hospital of University of Pennsylvania, Philadelphia; JHH, Johns Hopkins Hospital, Baltimore; UVMC, University of Virginia Medical Center, Charlottesville.
US AMCs can offer state of the art care to those who are admitted or have regular and reliable access to care, are drivers of innovation in biomedical research and technology, and are training hubs for outstanding physicians, and other health professionals. Why don’t the benefits accrued by patients and trainees alike extend to surrounding communities? Why aren’t the counties, cities and neighbourhoods where these centres are located, among the healthiest in the US and in the world?
The answer to these questions is, of course, complex. Current financial models do not incentivise US AMCs to invest adequately in the health of local communities. There is a lack of clarity on the respective roles of individual stakeholders, including AMCs, in advancing community health.12 Quality of care accounts for only 20% of health outcomes. Reliable and regular access to care is often limited for many of those living in the catchment areas of US AMCs. Many health outcomes depend on factors (such as physical environment, social and economic circumstances, and health behaviours) over which US AMCs have less control.
However, US AMCs could opt to be accountable not only for the health of individuals admitted to their wards or visiting their clinics but also for the health outcomes of the communities they are meant to serve. This accountability could be central to the centres’ mission. Much like what happens when they engage globally, there are steps that the centres could take to maximise their impact locally (box 1).
Adopting locally the lessons learnt globally: practical steps for academic medical centres (AMCs) in the United States (US)
Include community health among the metrics by which the success of US AMCs is measured and alter financial incentives accordingly.
Establish new or increase support for existing public health or community health departments and divisions.
Establish multidisciplinary and multisectoral strategic partnerships with local stakeholders to address complex health issues.
Prioritise capacity strengthening of local health stakeholders and sustainability.
Increase diversity in composition of governance bodies to reconcile financial responsibility and higher service aspirations.
Establish hubs of innovation in health service delivery and ‘model’ health systems within surrounding communities.
Adopting locally the lessons learnt globally: a few practical steps
First, a commitment to improving the health outcomes of surrounding communities should be included in the mission statement of US AMCs and should be one of the measures by which the success of the centres is measured. Additional financial incentives, like the receipt of special fees or multipliers when US AMCs achieve specific health targets in surrounding communities might also play an important role towards greater community engagement. Currently, the success of US AMCs is measured by metrics such as quality of care, the amount of revenue generated by clinical services, the amount of research funding secured, and the number/calibre of articles published by the faculty. Very rarely is community health a priority for US AMCs. As a result, surrounding communities have often felt neglected and disregarded by the centres rather than engaged in a meaningful and productive relationship. Changing this unhealthy and at times adversarial dynamic should be the first step taken by US AMCs seeking to advance community health.
Second, US AMCs could establish new or increase support for existing public health or community health departments. These departments would be tasked with securing and sustaining the ties between health services delivered within the centres’ facilities and those delivered within the centres’ catchment areas so that the benefits accrued by individual patients lead to broader improvements in the health outcomes of surrounding communities. They would also be tasked with breaking down the artificial separation between clinical care, public health, and social determinants of health that is often entrenched in many US AMCs.
Third, US AMCs could establish strategic partnerships with local health stakeholders with complementary and synergistic mandates, resources and expertise. These stakeholders do not differ significantly from those engaged by US AMCs abroad and include governmental organisations (such us city health departments), non-profit and faith-based organisations that focus on health issues, patient advocacy groups and other civil society organisations. When the complexity of the health issues requires it, local stakeholders in sectors outside of health (such as social protection, housing, education, food security, transport, urban planning and law enforcement) could be involved as well. To be effective, these partnerships would need a governance structure that favours collective action, a way to mobilise resources to initiate and sustain projects and activities, and a common set of policies, practices and targets that all partners agree on and are accountable to.
Fourth, US AMCs could adopt a framework for local health partnerships that prioritises capacity strengthening and sustainability. Establishing strategic partnerships can be challenging, especially when there are significant mismatches in the resources, capacity and expertise that each partner has. In global health, when certain partners are unable to fully contribute to a joint effort, other partners are expected to assist them in performing some of their duties early on and help them strengthen their capacity to function independently and sustain projects and activities over time. A similar approach to partnerships could be adopted by US AMCs locally. As likely the most resourced, capacitated and expert partner, US AMCs might have to play, at least initially, a leading role in these partnerships and step out of the traditional confines of their responsibilities.
Fifth, US AMCs could further increase the diversity in the composition of their boards of directors and governance bodies and include representatives from community-based organisations, civil society, and patient advocacy groups. Bringing together diverse voices and perspectives would help ensure that US AMCs operate in a financially sustainable way, live up to their higher service aspirations and address the health issues of patients with vastly different social and economic circumstances.
Finally, US AMCs could turn the neighbourhoods where they are located into hubs of innovation in health service delivery. Much like what happens in many global health initiatives and partnerships established abroad,13 14 US AMCs could seek to establish ‘model’ health systems that integrate care between health facilities and communities (eg, by relying on community health workers) and where implementation science can inform evidence-based, multisectoral and multidisciplinary health interventions.
Building on positive developments to further pursue health equity
Some US AMCs have already moved towards a greater engagement of surrounding communities and begun establishing innovative initiatives and partnerships within their catchment areas that prioritise community participation, integration between facility-based and community-based care, and multidisciplinary and multisectoral approaches to health service delivery.12 15–17 However, despite these positive developments, more needs to be done. Greater engagement of surrounding communities would allow US AMCs to maximise their impact in the neighbourhoods where they are located. It would also ensure that the centres honour the ongoing contribution of US taxpayers, who subsidise the costs of many of the centre’s operations. Lastly, it would save money by integrating disease treatment and prevention and biomedical interventions with actions that address social determinants of health and affect the most vulnerable patients (US AMCs deliver a disproportionate amount of health services to uninsured patients or patients covered by Medicaid, often at a significant financial loss).18
To be clear, we are not arguing that US AMCs should stop engaging in global health and turn inward. We are proposing quite the opposite: that the fight to improve the health of those who are most vulnerable is in fact a global fight, one to be undertaken overseas and in our own backyards. The lessons learnt in the pursuit of health equity abroad can renew the US AMCs’ commitment, infuse new energy and generate innovative ideas for the pursuit of the same goal locally. Our domestically underserved communities deserve nothing less.
Footnotes
Handling editor Seye Abimbola
Contributors This article is based on the collective experience of the authors. CC conceived the outline of the article with inputs from LVA and WP. CC wrote the first draft. All authors contributed intellectual content, edited the article and approved the final version for submission
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article.