Article Text

Abstract
Background Noma, a rapidly progressing infection of the oral cavity, mainly affects children. The true burden is unknown. This study reports estimated noma prevalence in children in northwest Nigeria.
Methods Oral screening was performed on all ≤15 year olds, with caretaker consent, in selected households during this cross-sectional survey. Noma stages were classified using WHO criteria and caretakers answered survey questions. The prevalence of noma was estimated stratified by age group (0–5 and 6–15 years). Factors associated with noma were estimated using logistic regression.
Results A total of 177 clusters, 3499 households and 7122 children were included. In this sample, 4239 (59.8%) were 0–5 years and 3692 (52.1%) were female. Simple gingivitis was identified in 3.1% (n=181; 95% CI 2.6 to 3.8), acute necrotising gingivitis in 0.1% (n=10; CI 0.1 to 0.3) and oedema in 0.05% (n=3; CI 0.02 to 0.2). No cases of late-stage noma were detected. Multivariable analysis in the group aged 0–5 years showed having a well as the drinking water source (adjusted odds ratio (aOR) 2.1; CI 1.2 to 3.6) and being aged 3–5 years (aOR 3.9; CI 2.1 to 7.8) was associated with being a noma case. In 6–15 year olds, being male (aOR 1.5; CI 1.0 to 2.2) was associated with being a noma case and preparing pap once or more per week (aOR 0.4; CI 0.2 to 0.8) was associated with not having noma. We estimated that 129120 (CI 105294 to 1 52 947) individuals <15 years of age would have any stage of noma at the time of the survey within the two states. Most of these cases (93%; n=120 082) would be children with simple gingivitis.
Conclusions Our study identified a high prevalence of children at risk of developing advanced noma. This disease is important but neglected and therefore merits inclusion in the WHO neglected tropical diseases list.
- epidemiology
- public health
- other infection, disease, disorder, or injury
- cross-sectional survey
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Our understanding of the current disease burden and epidemiology is limited; the WHO estimates 770 000 people are currently living with noma globally.
Three Nigerian studies estimated the burden of disease ranging from 7 cases per 1000 children aged between 1 and 16 years (2003) to 6.4 per 1000 children (2003) to 1.6 per 100 000 population at risk (2010–2018).
What are the new findings?
The prevalence of any stage of noma was identified in 3.3% of sampled children.
Having a well as a drinking water source, being aged between 3 and 5 years and preparing pap less than once a week were associated with higher noma prevalence.
What do the new findings imply?
Noma is a disease with considerable burden in northwest Nigeria.
Resource allocation to improve health systems to prevent, detect and treat noma is required and this could be enhanced if noma were added to WHO’s list of neglected tropical diseases.
Introduction
Noma, also known as cancrum oris, is a poorly understood, rapidly progressing infection of the oral cavity, with a reported 90% mortality rate.1 If untreated, death usually occurs within 2 weeks after the onset of acute necrotising ulcerative gingivitis (stage 1 noma).1 2 Treatment with antibiotics, wound debridement and nutritional support in the early reversible stages of the disease greatly reduce mortality and morbidity.2 Noma mostly affects children aged 2–5 years, and those who survive have severe facial disfigurements and multiple functional impairments including difficulties eating, seeing and breathing, contributing towards stigmatisation.2 Noma starts as an inflammation of the gums leading to the rapid destruction of the hard and soft tissues of the face usually within 1 week.3 The WHO has classified noma into stages1: stage 0, simple gingivitis; stage 1, acute necrotising ulcerative gingivitis; stage 2, oedema; stage 3, gangrene; stage 4, scarring; stage 5, sequelae. It is unknown what proportion of simple gingivitis cases progress to the later stages of noma, but it is thought to be a small fraction.1 In the majority of cases, infection causes the destruction of the cheek, while destruction of the jaw, lip, nose and eye have also been reported.4 Noma can become inactive with, and sometimes without, treatment. Once this occurs, patients can survive into adulthood but often require extensive reconstructive surgery and physiotherapy to correct the resulting defects and improve function.1 The aetiology of noma is unknown but thought to be multifactorial.2 Noma typifies the complex interactions between extreme poverty, malnutrition, poor oral hygiene, poor access to routine childhood vaccinations, limited access to quality healthcare and immunosuppression resulting from comorbidities such as HIV.2
In the 1800s, noma was widely reported in Europe5 but is currently thought to be most prevalent in low-resource settings in Africa and Asia.6 Based on expert opinion, the WHO estimates that 770000 people are currently living with noma globally; however, it is unclear what stages of noma are included in this estimate.7 The oldest estimate of the burden of this disease that we could locate was from Edinburgh, UK, which indicated that noma was diagnosed once out of every 5000 cases of children with an illness between 1860 and 1871.8 Two recent Nigerian studies estimated the burden of disease ranged from 7 cases per 1000 children aged between 1 and 16 years (2003)9 to 6.4 per 1000 children (2003).10 A study from 2019 estimated the period prevalence of noma from 2010 to 2018 was 1.6 per 100 000 population at risk in Nigeria.11 These estimates are based on expert opinion, number of hospital admissions and retrospectively collected data, and it is unclear which stages of noma were included.12 Our understanding of the current disease burden and epidemiology thus remain limited. There are few studies not only on the burden of disease but also on the pathogenesis and mortality rate. Although these aspects highlight the neglected nature of the disease, noma is not currently on the WHO neglected tropical diseases list.
Noma cases are frequently reported in Nigeria.9 13–15 The Nigerian Centre for Disease Control recorded 37 646 noma cases from 2011 to 2017.16 However, these records may underestimate the true burden of cases, given limited surveillance data and the potential for under-reporting (low rates of diagnosis, patients not accessing healthcare, reported high and rapid mortality).16 The majority of noma cases are reported from the northwest and northeast of the country.17 At the 2018 National Noma Day Workshop, the Nigerian Ministry of Health confirmed that noma was a national public health priority, and highlighted the urgent need to generate robust evidence on the country’s disease burden for programmatic planning.18 This study contributes towards this need by estimating the prevalence of noma in northwest Nigeria.
Methods
Study design and setting
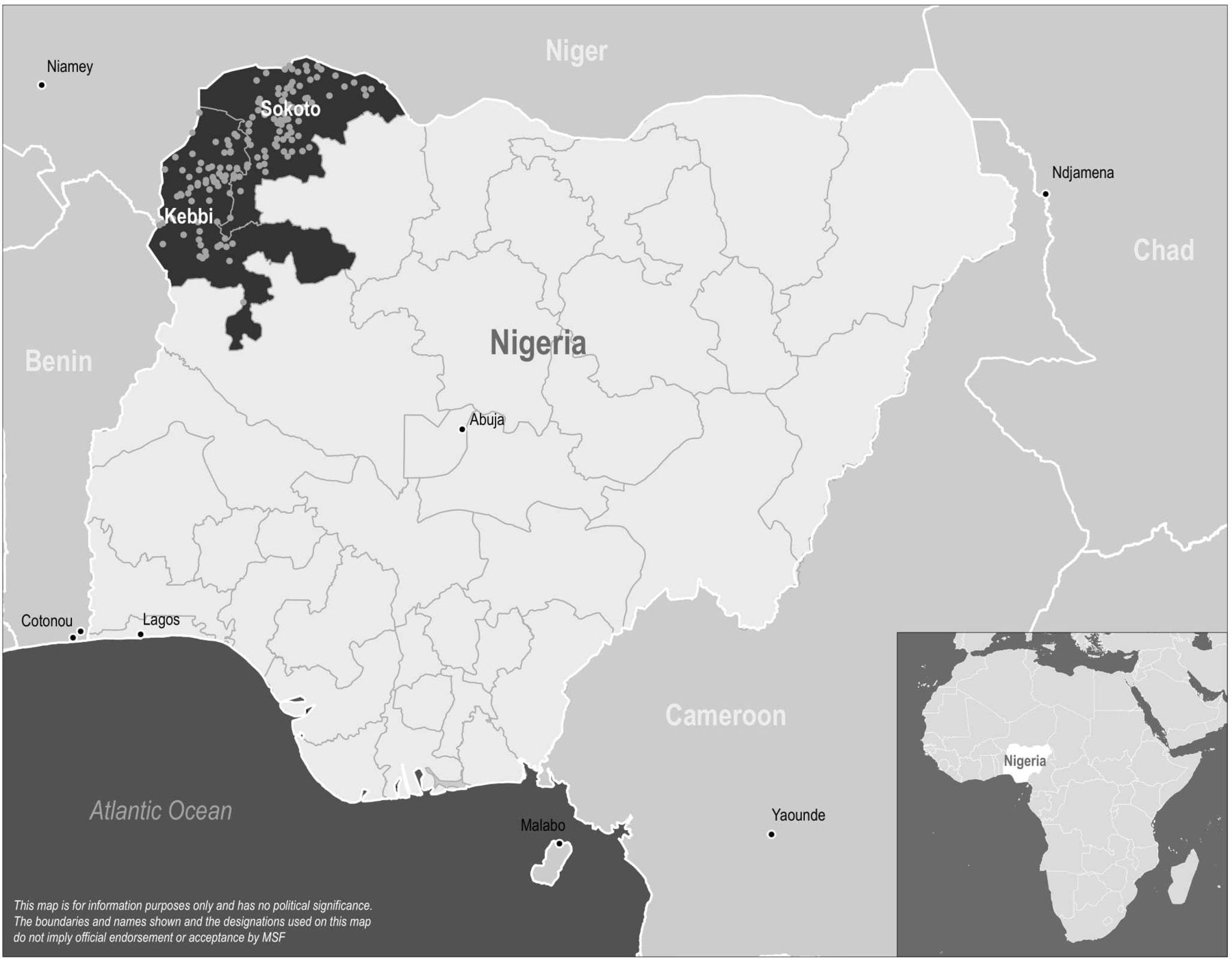
A two-stage cluster-based cross-sectional survey was conducted in Sokoto and Kebbi States in northwest Nigeria (figure 1).

{kind=link}
Map of Africa (inset) and Nigeria (main panel). Main panel, grey lines represent state boundaries. Sokoto and Kebbi states, locations for this study, are shaded dark. Pale grey dots within Sokoto and Kebbi states indicate the clusters where data collection occurred during the survey.
Sampling
Sokoto and Kebbi States have estimated populations of 4 798 979 and 4 203 978, respectively.19 Sample size calculations indicated the need for inclusion of 3615 households across 181 clusters with 20 households per cluster in order to estimate noma prevalence with precision of 0.4%. This calculation was based on the following assumptions: prior prevalence estimate, 1%10; design effect, 2; 1.98 children per household in the group aged 0 to 4 years20; average household size, 621; and a 10% non-response rate.
The number of villages (clusters) per ward was selected proportional to the population size of each administrative ward. A sampling frame of villages was created by ward in Sokoto and Kebbi using geosampling remote sensing methods. The OpenStreetMap database was compared against freely available satellite imagery to identify and verify village geolocations and add new village geolocations to the list. Villages were each assigned a number and a random selection was conducted.
Study participants
All children aged ≤15 years who lived in a selected household in sampled clusters were included in the study.
Data collection
Five research teams, each with five team members, of whom one was a nurse or doctor, and one the team leader, carried out data collection. Teams were trained for 1 week prior to the commencement of data collection. Teams followed directions to selected clusters using a mobile mapping application (OsmAnd) on data collection tablets (electronic mobile devices). Random household selection at cluster level was done using the adapted WHO Expanded Programme on Immunisation method.22
In selected households, consenting caretakers answered a structured questionnaire, collected on tablets using KoBoCollect (KoboToolBox), which covered sociodemographic characteristics, living conditions, child’s vaccination status, oral hygiene practices, food preparation, feeding practices and access to healthcare in the 12 months preceding the interview. For the questions around feeding practices, pap was defined in this context as a type of porridge staple made from maize, sorghum or millet. Interviews were conducted in Hausa, and answers were coded automatically on the KoBoCollect tool into English.
In the sampled households, all eligible children underwent oral screening, which involved visual examination by a medical team member for any noma stage, based on the WHO classification.1 The caretakers of children with simple gingivitis were advised to follow a strict oral health regimen (gargle with salt water or use water to clean mouth twice or more a day) as were acute necrotising gingivitis cases who were also referred to the closest health centre. If children were identified as having any later stage of noma, they were referred directly to the Noma Children’s Hospital for care.
To assess the malnutrition status in children aged 6 months to 5 years, mid-upper arm circumference (MUAC) measurements were conducted using a flexible MUAC device with a precision of 1 mm.
Medical data (oral screening and MUAC) were collected on paper and later entered into a password-protected database by the study team.
Collected data were screened daily by the research team supervisors to identify inconsistencies and missing items, and immediate feedback was given to the data collection teams.
Statistical analysis
We performed descriptive analyses of household characteristics in the study sample. Categorical variables are reported as frequencies and percentages. Continuous variables are summarised using medians and IQR. Missing data numbers are recorded in each table.
Wealth scores were calculated by assigning a value of one to each of the following items owned by the family: a mobile phone, motorbike, tractor and camel (these items were chosen based on consultation with local researchers, knowledgeable about the context). The minimum wealth score was zero and the maximum was four.
Weighted prevalence and 95% CI for all WHO noma stages were estimated and stratified by age group (0–5 years and 6–15 years). The number of individuals with noma in Sokoto and Kebbi States was calculated by extrapolating the percentage prevalence from our study results to the total population in the group aged 0–15 years for these states. This calculation took into consideration the cluster survey design and population age distribution of the two states. Using MUAC measurements, we estimated the weighted prevalence of severe acute malnutrition (SAM, MUAC <115 mm), moderate acute malnutrition (MAM, between MUAC ≥115 and <125 mm) and global acute malnutrition (GAM, MUAC <125 mm) in children aged 6 months to 5 years. The SEs of the estimates were adjusted using the linearisation method (syvset suite of Stata commands) to reflect the two-stage clustered design of the survey.23 The estimates and SEs were weighted to account for the actual population distribution of the two states, as our survey sample was observed to have under-represented participants aged 6–15 years, when we compared our sample’s age distribution with the population age distribution. The design effect (DEFF) was calculated to assess the ratio of variance under the sampling method used, in comparison to the variance of a simple random sample. This reflects the impact of the cluster sampling strategy. DEFF is reported for each prevalence and malnutrition estimate.
Univariable analysis with logistic regression was conducted to identify factors associated with noma stages 1 and 2 in the total study sample, where the number of noma cases were too small to allow for multivariable analysis.
Univariable and multivariable analyses were conducted using logistic regression to estimate factors associated with any noma stage (stage 0–2); stratified by age group (0–5 and 6–15 years). Variables chosen for inclusion in the multivariable analysis were those with 10 or more cases24 and a univariable strength of association equivalent to a p<0.2, after assessing collinearity among variables. To further understand the association with age, an age covariate with finer age categories (0–2 years, and 3–5 years, in the younger age group model; and 6–10 years, and 11–15 years, in the older age group model, respectively) were included in the univariable analyses for both age group models, and in the 0–5 year old multivariable model.
All data analysis was conducted with Stata V.15 (StataCorp LP, College Station, Texas, USA).
Patient and public involvement
Patients and the public were involved in the framing of the study questionnaire and data collection. Dissemination of results to patients and the public will take place through outreach activities from the NCH.
Ethical considerations
Written informed consent was obtained from all literate caretakers; caretakers with insufficient literacy provided a thumbprint and a signature from a literate witness. For individuals aged 8–17 years, the child provided assent and a caretaker provided written consent.
Results
The survey was conducted from 17 September to 5 November 2018, and included 3499 households in 177 clusters, 92 clusters from Sokoto and 85 from Kebbi (four clusters were not accessible because of security issues), with 7164 children aged <15 years. As 42 children did not have oral examinations, they were excluded from the analysis and the remaining 7122 were included. The median caretaker age was 30 years (IQR 25–35); 3423 caretakers (97.8%) were female; 2194 (30.8%) were employed or self-employed, and the median household size was five people (IQR 4–7). Most children (n=4239; 59.5%) were aged 0–5 years, 3692 (52.1%) were female, 5875 (83.0%) had no education, and 6686 (94.4%) had a primary caretaker that was the mother (table 1).
Demographic characteristics of households and children in the noma prevalence survey population
Prevalence
Table 2 reports the prevalence of all stages of noma in the study population overall and by age group. Any stage of noma was identified in 3.3% of sampled children (n=194; CI 2.7 to 4.0). Stage 0 noma was identified in 3.1% (n=181; CI 2.6 to 3.8), stage 1 in 0.1% (n=10; CI 0.1 to 0.3) and stage 2 in 0.05% (n=3; CI 0.02 to 0.2). No children with stages 3–5 noma were detected in our study population (table 2). Based on these results, 3300 out of every 100 000 children in the group aged 0–15 years would have any stage of noma and 150 out of every 100 000 children would have stage 1 or 2 noma in the study area.
Noma stage and malnutrition prevalence (overall and by age group)
The prevalence of SAM in children aged 6 months to 5 years (n=3993) was 3.7% (n=149; CI 3.2 to 4.4) and MAM 7.7% (n=309; CI 6.7 to 8.7) (table 2).
Factors associated with noma
Table 3 describes univariable analysis of risk factors for stage 1 and 2 noma regardless of age category. This analysis showed that having eaten pap in the last 24 hours (OR 0.2; CI 0.1 to 0.9); the child eating pap once or more per week (OR 0.4; CI 0.1 to 0.9) and the caretaker preparing pap once or more per week compared with less frequent preparation of pap (OR 0.3; CI 0.1 to 0.8) were associated with not having stage 1 and 2 noma. The child experiencing an illness in the 12 months prior to the interview was associated with being a stage 1 or 2 noma case (OR 8.8; CI 1.1 to 69.5) (table 3).
Univariable analysis for stage 1 and 2 noma
The risk factors associated with any stage of noma for the group aged 0–5 years are shown in table 4. The multivariable analysis shows that two factors remained associated with being a noma case in the group aged 0–5 years, namely, having a well as the source of drinking water (adjusted odds ratio (aOR) 2.09; CI 1.22 to 3.60) and being aged 3–5 years (aOR 3.90; CI 2.04 to 7.47) (table 4).
Univariable and multivariable analyses of associations with any noma cases (stage 0 to 5), 0–5 years
In the group aged 6–15 years, the risk factors associated with any stage of noma are shown in table 5. Multivariable analysis showed that males were more likely to be noma cases (aOR 1.52; CI 1.04 to 2.22), and that the caretaker preparing pap once or more per week was associated with not having noma (aOR 0.36; CI 0.16 to 0.82) in the group aged 6–15 years (table 5).
Univariable and multivariable analyses of associations with any noma cases (stage 0 to 5), 6–15 years
Vaccination coverage rates in both age groups were low (21% of 0–5 year olds and 12% of 6–15 year olds had any immunisations noted on the vaccination card seen by the interviewer). No association between vaccination status and noma was seen in our study.
Discussion
We have shown that the prevalence of any stage of noma in Kebbi and Sokoto States is 3.3%. Based on the study results, we therefore estimate that 129 120 (CI 105 294 to 152 947) individuals <15 years of age would have any stage of noma at the time of the survey within the two states. Most of these cases (n=120 082, 94% of all cases) would be children with simple gingivitis (ie, stage 0) and approximately 7101 (4% of all cases) and 1937 (2% of all cases) of children would have stage 1 and 2 noma, respectively. Our estimates exceeded those from Bello et al 2010–2018 period prevalence estimates (1.6 per 100 000)11 and Fieger et al. in 2003 (6.4 per 1000 children).10 Differences between the estimates could be due to geographical differences (Bello et al is north central Nigeria vs our northwest Nigeria), or due to methodological differences (Bello et al used patient record review of patients presenting at hospital and Fieger et al based their estimates on the number of clefts and mathematical modelling vs our community-based cross-sectional survey). It was unclear which stages of noma were included in these estimates.
Despite only covering two states of one country, our prevalence estimates would account for 17% of the current global WHO prevalence estimates.7 Even though direct comparisons between the WHO and current study estimates are difficult as the stages included in the WHO estimates were not reported, our findings do suggest that the true burden of noma worldwide may be higher than previously thought.
Results from this study highlight the under-reported and overlooked nature of noma. Even though oral diseases, such as noma, are largely preventable, they impact over 3.5 billion people worldwide (untreated dental caries are the most prevalent of these oral health issues), disproportionally affecting marginalised groups.25 Oral diseases are frequently more neglected than other diseases in low-income and middle-income countries, which may be linked to the fact that modern dentistry focuses on high-technology solutions, which are unaffordable and not currently feasible in low-resource settings.26 This overarching neglect of oral diseases is magnified in the case of noma, as patients live in underserved, often rural locations.27 Many cases will never seek care, and, even if they do, noma is unknown to many healthcare workers in endemic areas.28 The condition may thus go undiagnosed, and rapid detection with opportunities for early treatment through improved oral hygiene, nutritional support and antibiotics, may be missed.
Strong surveillance systems have been the cornerstone of many successful neglected tropical disease control programmes.29 30 The WHO has stated that robust surveillance helps to better understand the burden and distribution of disease, and to identify high-risk populations so that evidence-based decision-making can be used to target interventions in resource-constrained contexts.31 A further benefit of robust surveillance is an increase in the number of cases identified, diagnosed and treated.32 Due to the neglected nature of noma, surveillance activities for active noma cases are hampered and it is unlikely that current surveillance mechanisms adequately identify deaths from noma at a community level. The mortality rate associated with noma is unknown, but estimated to be as high as 90% if the disease is left untreated.1 Deaths may be primarily due to starvation, aspiration pneumonia, respiratory insufficiency or sepsis,33 34 and not be attributed to noma, further reducing the potential for accurate reporting of disease burden. Our findings suggest that improved efforts to enumerate the burden of disease are necessary.
This study highlights the need for a single classification system for the differential diagnosis of each stage of noma, which would be beneficial in standardising reporting of noma globally by the clinical and research noma community. In published work, noma is often classified into two stages (acute and chronic noma35 36) or with the Montandon system (classifies noma according to the location of the defect).37 The lack of standardisation complicates comparison between different studies. The WHO noma staging system1 is the most comprehensive to date and includes an early-stage noma definition which is useful as it identifies those at risk of progressing to later stage noma. However, it lacks specificity as it overlaps with commonly seen ailments such as simple gingivitis and acute necrotising gingivitis and therefore may overestimate the burden of disease. It is currently unknown what the risk factors are for progression of noma, nor the proportion of patients who progress to the later stages of disease. Explicit reference to which WHO stages of noma are included in prevalence and incidence estimates as well as improved detail of the method employed in these estimations would greatly improve our ability to compare findings across studies. The lack of consistency of approach to assessing the incidence and prevalence of noma in the literature and the lack of real investment in assessing the true incidence and prevalence of this condition particularly in regions that bear the highest global burden contribute to the ongoing neglect of this disease and the populations it affects.
Study findings indicate that children aged between 3 and 5 years had a higher prevalence of noma in comparison to those aged 2 years or less, a finding corroborated by other studies.38–41 We hypothesise that this finding is likely due to the relationship between child feeding practices in Nigeria and malnutrition as a risk factor for noma. Our study did not identify an association between acute malnutrition and having noma. However, other studies have shown that rural Nigerian children typically breastfeed until 24 months of age42 and then transition to a limited diet.43 This has shown to result in higher levels of malnutrition and stunting43 and therefore, a potentially higher risk of developing noma. This discrepancy in our findings in comparison to other studies could be due to the fact that our population had early stage noma, whereas other studies could have identified the association between malnutrition and late stage noma. It is also possible that late stage noma could cause malnutrition if the child was having difficulties eating due to the noma infection.
Our findings showed that older (aged 6–15 years) male children were more likely to have noma in comparison to older female children. We do not know what would explain this finding as we would not expect an inherent difference in gender in noma development. This finding warrants further research.
We showed that various factors relating to pap preparation and consumption were linked to not having stage 1 and 2 noma among the whole study sample and of any stage noma in the group aged 6–15 years old. It is difficult to explain this finding as it could be due to a lack of access to food or that pap made more frequently has less chance of becoming contaminated (thus causing less disease) as it is stored for shorter periods of time. A Nigerian study showed that when mothers prepared food far in advance, contamination was more likely to occur.44 A further Nigerian study in Kebbi State showed that pap was contaminated with high levels of Salmonella in comparison to other commonly eaten foods.45 This finding affected children in the older age group which may be because they are more reliant on this food source in comparison to the younger children.
This study further indicated that having a well as the main water source in comparison to other water sources such as a borehole, river or tap, was associated with having noma in the group aged 0–5 years. Well water has a high risk of contamination from nearby pit latrines or livestock,46 and the consumption of contaminated well water is a risk factor for diarrhoea,47 which in turn is an identified comorbidity for children with noma.48
Vaccination coverage in all eligible children included in the study was low. Even though this result prevented us from exploring whether vaccination is associated with noma prevention, it does confirm findings from other studies in rural Sokoto State, where up to 70% of children were not vaccinated against measles and other common childhood diseases.35 Low immunisation coverage is an important indicator of struggling societal systems in need of multisectoral improvements, including access to quality timely healthcare, access to safe drinking water, improved nutrition and security. Prevention efforts should also include early detection training with healthcare workers, and setting up effective referral pathways. These initiatives are resource-intensive and require large-scale investment of time, money and human resources.
This study had a large sample size and robust approach to sampling and analysis, and we are confident that prevalence estimates are broadly representative of the study area. However, a few limitations should be considered. This cross-sectional study was conducted on a disease with an extremely rapid clinical progression with onset to death taking as little as 2 weeks.1 Thus, it is possible that Neyman bias was present and we only identified a fraction of noma cases that occur. The research team did come across stage five noma patients in study villages, but not in households included in the study. These patients were referred to the NCH for care. It is possible that a study with a larger sample size could have identified children with the later stages of disease. Some of the answers were self-reported by caretakers, which could have introduced social desirability bias that either inflated or deflated the risk factor associations found in the study. This aspect was mitigated by anonymising the survey and trying to phrase questions in contextually acceptable ways. Data on some risk factors, such as comorbidities, water quality and malnutrition in older children were not collected, limiting our ability to identify associations with these factors. It is difficult to interpret the results of questions asking about consumption of any food and specific foodstuffs in the 24 hours prior to the interview and associations with noma as respondents with noma could have difficulty eating in general and would thus have been less likely to report eating at all. Finally, the challenging security situation limited the areas the research teams could access. This may have introduced selection bias, and an underestimation of noma and malnutrition prevalence, as we did not visit the hardest to reach communities who were likely most vulnerable to noma infection. Future research on the burden of noma should be combined with existing surveillance systems for other disease and research activities such as malnutrition and vaccination surveys.
Noma meets the criteria of a neglected tropical disease as defined by the WHO: it is a preventable disease that affects children in low-resource contexts; children that survive will have life-long physical and mental health sequelae; and there is poor understanding of the disease, its pathogenesis and global burden.49 This study has shown that the prevalence of any stage of noma is higher than previous estimates. While we did not find any later stages of the disease, the high rates of simple gingivitis and the presence of known risk factors for noma (low vaccination rates, malnutrition and poor access to healthcare) suggest the need for improved coverage of preventative interventions and access to care in northwest Nigeria. Our prevalence estimates are greater than those for snakebite in Nigeria (497 per 100 000 people), which the WHO recently recognised as a neglected tropical disease.50 Noma prevention and control will require a concerted health systems approach. Adding noma to WHO’s list of neglected tropical diseases will facilitate global attention for noma and the allocation of much-needed resources to those countries where noma continues to be a public health problem.
Acknowledgments
The authors are grateful to the caretakers and children who agreed to be a part of this study, the study team, the staff at the Nigerian MSF Mission and the Noma Children’s Hospital, the Missing Maps volunteers and the Sokoto and Kebbi Ministries of Health. Emma Veitch, freelance medical editor for MSF, UK, provided editorial assistance and her work was funded by MSF UK. Thank you to Mary-Ann Davies for her substantial contribution to the interpretation of data and critical review of the manuscript
References
Footnotes
Handling editor Alberto L Garcia-Basteiro
Contributors EF, AL, KB, SvdK, DBM, UM and CA were responsible for the study concept and design, and interpretation of data. EF, OMJ and JS collected the data. FS, ASA, SI, CI, BO and AF provided support for the data collection. JV and RB conducted the geo-sampling and created the figure. EF, AL and CA did the statistical analysis. EF and AL, drafted the manuscript. All authors critically reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Map disclaimer The depiction of boundaries on the map(s) in this article do not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. The map(s) are provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient and public involvement Patients and/or the public were involved in the design, or conduct, or reporting or dissemination plans of this research. Refer to the Methods section for further details.
Patient consent for publication Not required.
Ethics approval Ethical approval was obtained from the Médecins Sans Frontières (1848), Usman Danfodiyo University Teaching Hospital (729) and the Sokoto (SKHREC/070/018) and Kebbi (104:4/2018) States Ministry of Health ERB’s.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on request. MSF has a managed access system for data sharing that respects MSF’s legal and ethical obligations to its patients to collect, manage and protect their data responsibility. Ethical risks include, but are not limited to the nature of MSF operations and target populations being such that data collected often involves highly sensitive data. The dataset supporting the conclusions of this article is available are available on request in accordance with MSF’s data sharing policy (available at: http://fieldresearch.msf.org/msf/handle/10144/306501). Requests for access to data should be made to data.sharing@msf.org.