Article Text

Abstract
Introduction We assessed whether the Women for Women International (WfWI) economic and social empowerment programme could reduce women’s experiences of intimate partner violence (IPV) and depression in Afghanistan.
Methods We conducted a two-arm individually randomised controlled trial in six urban and peri-urban communities. Communities were selected by WfWI for being conflict affected and showing signs of economic vulnerability (eg, little or no education, living in extreme poverty). Individual eligibility were female, aged 18–49, able to consent to participate and one woman per household. At 22 months, three primary outcomes were assessed: past year physical IPV experience; past year severe IPV experience; depressive symptoms. There was no blinding to arms. We conducted an intention-to-treat analysis, controlling for age. We also conducted qualitative interviews at endline, analysed using thematic analysis.
Results 1461 women (n=933 married) were recruited and randomised. Retention at endline was n=1210 (82%). Primary outcomes were in the hypothesised direction, but showed no significant impacts: physical IPV (adjusted OR (aOR) 0.88 (0.62 to 1.23)), severe IPV (aOR 0.75 (0.50 to 1.11)) and depressive symptoms (β −0.35 (−1.19 to 0.48)). Women reported reduced food insecurity (β −0.48 (−0.85 to –0.12)), higher earnings (β 3.79 (0.96 to 6.61)) and savings (β 11.79 (9.95 to 13.64)). Women reported less gender-inequitable attitudes (β −0.89 (−1.15 to –0.62)), more household decision-making (β 0.35 (−0.04 to 0.74)) and increased mobility (aOR 1.78 (1.27 to 2.50)). Twenty-eight in-depth interviews were conducted.
Conclusion The intervention did not impact IPV or depression. The intervention did improve livelihoods, create more gender-equitable relationships and increase women’s mobility. Translating these gains into IPV and depression reduction is critical.
Trial registration number NCT03236948, registered 2 August 2017.
- trial
- Afghanistan
- mixed-methods
- women
- violence against women
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Conflict-affected communities have high levels of violence, even following cessation of formal violence.
This includes high levels of intimate partner violence (IPV), perpetuated by gender inequality and poverty, exacerbated by the conflict.
The overwhelming majority of evaluations in conflict-affected communities to prevent IPV have been conducted in Africa, with limited impact on preventing IPV.
Key questions
What are the new findings?
At endline, the combined economic and social empowerment intervention had no impact on reducing married women’s experiences of IPV or depression, but a subgroup of women who experienced moderate food insecurity at baseline did see a significant reduction in IPV.
Women in the intervention reported significantly improved earnings, and savings, improved mobility, greater household decision-making power and more gender-equitable attitudes.
Qualitatively, poverty, overall limited authority in households, and few economic opportunities undermined greater change.
What do the new findings imply?
The combined economic and social empowerment intervention, while impacting known risk factors for IPV, did not impact women’s overall risk.
Further research and intervention development is required to understand how to enable these positive gains to translate into reductions in IPV.
Introduction
Conflict escalates the perpetration of interpersonal violence. Although rape in war has received considerable and much deserved attention,1 the most common form of violence women experience in conflict and post-conflict settings remains intimate partner violence (IPV).1 2 Driven by gender inequality and exacerbated by the destruction of social and community systems, long-lasting conflict-related trauma, deepened poverty and normalisation of violence, IPV is an enduring form of violence that continues throughout, and far beyond, the end of formal hostilities.1 3 4 Changing attitudes and social norms related to gender and the use of violence across communities is essential for peace-building in conflict and post-conflict settings. In addition, these need to also tackle the high levels of poverty that are lasting effects of conflict. Introducing interventions to start this work by elevating the status of women and reduce the violence they experience is crucial.
Very few interventions and trials have assessed whether, and what types of, interventions can prevent IPV in conflict-affected settings. A situational review of interventions targeting IPV in South Asian and Middle Eastern countries found that the majority of interventions focused on responses to IPV, such as providing legal and psychosocial support to survivors of violence, as opposed to prevention.5 As such, there is an urgent need to undertake high-quality prevention-oriented trials in these settings.
A major approach to intervening to reduce women’s experiences of IPV has been to combine economic strengthening interventions with social empowerment interventions.6 Theoretically, these two components are logically combined, as a wealth of research has highlighted how women’s experiences of IPV emerge in contexts of poverty and high levels of food insecurity, where households are under stress, and physiological impacts also lead to more arguments and greater conflict.7 Furthermore, economists also highlight how women’s lack of economic power places them at risk of IPV, as they have less bargaining power in relationships and less ability to exit violent relationships.8 In addition, patriarchal attitudes, most clearly seen in gender inequitable norms, particularly the acceptability of violence, are also key drivers of IPV, as violence is a more acceptable way of resolving conflict. As such, combining economic empowerment with social empowerment interventions has the potential to reduce women’s experiences of IPV. Indeed, a number of well-designed studies in Africa have demonstrated such approaches can reduce women’s experiences of IPV by up to 55%.9 10
In conflict and post-conflict settings, the primary intervention approach to reducing IPV has been focused on economic strengthening, sometimes combined with gender-transformative interventions. In rural Côte d’Ivoire, a savings group intervention for women affected by conflict added ‘gender dialogue’ sessions, targeting women and their male partners. There was little impact on physical or sexual IPV but a significant reduction in women’s experience of economic IPV.11 However, in a per-protocol analysis, women attending ≥75% of sessions showed reduced experiences of physical IPV.11 In Northern Uganda, a micro-enterprise assistance intervention had no impact on reported experiences of IPV. When a short male engagement component was added to the micro-enterprise initiative, women reported improved the quality of relationships with their husbands, but no reduction of IPV.12 In the Democratic Republic of Congo (DRC), a livestock asset transfer programme showed positive impacts on mental health and a non-significant reduction in emotional IPV experienced by women.13 Another set of studies evaluated the Creating Opportunities through Mentorship, Parental Involvement, and Safe Spaces (COMPASS) programme, which combines support for caregivers with provision of life skills training for adolescent girls in displaced populations in Ethiopia and Eastern DRC, and found no reduction in girls’ reported experiences of sexual violence.14 15 Many of these evaluations and interventions have had challenges in their design, including limited sample sizes, or incredibly short social empowerment interventions.
The small evidence base on economic and gender-transformative interventions in conflict-affected populations reinforces the need for further research, which builds on long-term interventions that have been implemented over many years. The limited impact of these types of intervention on IPV in conflict-affected populations is also reflective of the wider body of research on economic and gender-transformative interventions that finds better outcomes among women who are in more stable situations, often in rural settings and those not affected by conflict.6 This literature further highlights the importance of integrating gender-transformative components into economic programming to improve outcomes, with some studies showing that economic interventions alone can increase women’s experiences of IPV.6
Depression is also an outcome of high levels of exposure to conflict-related trauma, intimate partner violence and poverty.16 17 While short-term interventions such as cognitive-behavioural therapies and problem management approaches show promise in reducing symptoms of depression and poor mental health, including in conflict and humanitarian settings,18 19 in settings of abject poverty, and where IPV is common, interventions seeking to strengthen women’s livelihoods and reduce IPV experience may also impact on women’s depressive symptoms. Indeed, in conflict-affected DRC, a livelihoods asset transfer programme (Pigs for Peace) showed strengthened economic position and reduced depressive symptoms for women.13
Afghanistan has experienced over four decades of ongoing conflict. In recent years, insecurity has intensified with more attacks on the Afghan government and civilian population.20 High levels of trauma and poor mental health due to conflict, a highly patriarchal social structure that places restrictions on women’s mobility, women’s limited agency and power, and exceedingly high levels of poverty all come together to increase women’s risk of experiencing IPV.21 22 The 2015 Afghanistan Demographic and Health Survey (DHS) shows that IPV is widespread in the country, with 53% of ever married women aged 15–49 reporting lifetime experience of physical IPV and 46% reporting physical IPV in the past year.23 There is also wide variation by province, with past year physical IPV ranging from 4.7% in Helmand to 83.6% in Wardak.23 In 2018, the International Men and Gender Equality Survey (IMAGES), implemented in 14 provinces of Afghanistan, found that half (49.6%) of married women had experienced physical IPV in the past year, and two-thirds (69.7%) had been stopped from working outside the home in the past year.24 In addition, the DHS also showed low levels of work participation by women, with only 13% of currently married women reporting working outside their household in the past year, and only two-thirds of these women reported earning cash for this work.23
Women for Women International (WfWI) has been delivering a combined economic and social empowerment intervention in Afghanistan since 2002. The intervention is targeted at the most marginalised women in conflict-affected communities: those with low levels of literacy and numeracy, little or no formal education and high levels of poverty. The primary objective of the trial was to determine whether exposure to the WfWI intervention reduced married women’s experiences of IPV and improved the mental health of all women in the programme. Secondary objectives were to determine whether exposure to the programme improved gender attitudes and practices, strengthened livelihoods and improved life satisfaction.
Methods
Trial design
We conducted a two-arm individually randomised controlled trial of the intervention, with 1:1 randomisation, with an endline qualitative evaluation. More details on study rationale, setting, methods and intervention are available in a methods paper.25
Setting
The study was conducted in Kabul and Nangarhar provinces in Afghanistan in communities where WfWI had already planned to undertake recruitment in 2016 and 2017. WfWI undertook community assessments and coordinated with district governments to identify communities with sufficient populations that met eligibility criteria, leadership support for the programme and accessibility for the research and programming teams.
Participants’ eligibility
Community selection was based on WfWI’s programmatic focus, including (1) experience with war/conflict (eg, surviving violence, being displaced), (2) social vulnerability (eg, signs of malnutrition, poorer-than-average living conditions, facing restrictive traditional practices, forced or early marriage, or no or limited education) and (3) economic vulnerability (eg, extreme poverty, unemployment or limited to high-risk or unsafe occupations). These broad eligibility criteria were implemented in the initial community selection process, and then at the individual level through consultation with community and religious leaders to identify potentially interested women. Those incapacitated because of poor mental health or very severe disability were ineligible as they could not fully benefit from the intervention (though neither of these were objectively measured, but implemented by WfWI staff through the identification process). It was suggested women secure family support for their participation, which the vast majority did.
At the point of recruitment into the study, as a research team, we screened for the following criteria: (1) women should be aged 18 to 45, so that they could provide informed consent for the research; (2) women should not come from the same household. These two criteria sought to reduce the chances that a mother-in-law/daughter-in-law dyad would be enrolled because of concerns about privacy during the study, and any potential spill-over effects; (3) women had to agree to participate in the full programme. In addition, there was overemphasis on enrolling married women into the study during recruitment, as only currently married women could be asked about intimate partner relations in this context; however, this was not an inclusion criteria.
Intervention
WfWI’s 12-month economic and social empowerment programme aims to improve women’s economic stability, health and well-being, family and community participation and decision-making, and social networks (see online supplementary file 1). The rights-based programme features 90 to 180 min of programming per week, delivered to groups of 25 women in community-based training centres. Participants receive classroom training on numeracy, business skills and social empowerment topics, and hands-on training in a chosen vocational skill. In addition, participants receive a monthly cash stipend of US$10, an introduction to formal and informal mechanisms to save money (eg, self-help groups, microfinance institutions), referrals to health, legal and financial services, and connections to other women. The programme version tested in this trial was not specifically designed to prevent IPV. However, theoretical frameworks of root causes of IPV posit that combined programming strengthening women’s economic status in the household, and improving women’s social empowerment, could reduce women’s experiences of IPV. The control arm received a US$10 equivalent for each quantitative interview they completed.
Supplemental material
Outcomes
Table 1 describes the outcomes. The primary and secondary outcomes were pre-specified for the endline, 22 months post-baseline. To enhance learning, we also collected data at midline (12 months post-baseline). Outcomes and time periods were pre-specified in the trial protocol.13
Primary and secondary outcomes for the trial
Reflecting the uncertainty in how best to assess IPV in trial settings and the multiple objectives of the trial, the trial had three primary outcomes, two of which related to women’s experience of physical IPV.
Past year physical IPV was assessed with a modified version of the WHO Violence Against Women Scale.26 Five questions asked about physical IPV experienced in the past year from their husband and a range of different forms of physical violence (eg, slapped, beaten, threatened with a gun). Response options were never, once, few or many. A response of once or more frequently to any item led to a participant being classed as having experienced physical IPV in the past year.
Past year severe IPV used the same items as past year physical IPV, but coded responses differently. Women were classified as having experienced severe IPV if they responded positively to two or more items, or else responded few or many to any single item from the five questions. The classification of severity of IPV is derived from previous studies suggesting significantly greater health impacts for those experiencing two or more IPV experiences.27
Past week depressive symptoms were assessed through 20 items comprising the Center for Epidemiological Studies Depression scale (CES-D). An example was: “During the past week I had crying spells”, with possible responses being rarely or none of the time, some or little of the time, moderate amount of time or most or all of the time. The scale was summed and higher scores indicated more depressive symptoms.
Secondary outcomes are described in table 1.
Sample size
The sample size was estimated from our pilot study that showed that among 100 women who were already part of WfWI programming, past year physical IPV was 32% for married women. We estimated an effect size of 0.3 difference in prevalence of physical IPV between intervention and control arms at endline, and calculated at 80% power and at significance level (alpha) of 5%. This gave us an estimate of 337 per arm. We also took into account the proportion of currently married women to be recruited into the study and the proportion of women likely to be lost to follow-up, and had a final sample size of 1477.25
Statistical analysis
Our main analysis was an intention-to-treat analysis; this includes all participants no matter whether or not they attended the intervention (if in the intervention arm), or if they did attend the intervention (if in the control arm), and analyses participants based on whether they were randomised to receive the intervention or not. This is the most appropriate way to analyse interventions, as it accounts for the fact that not everyone attends interventions, even if they say they will.28 Our primary and secondary outcomes were committed to, as was our statistical approach before endline data were collected,25 ensuring we did not change our outcomes and statistical modelling approach in ways that would unfairly benefit the intervention. The statistical analysis approach took into account the study design, which randomised individuals (rather than communities) and followed up the same individuals over time, and the analysis accounted for these issues. All statistical analyses were conducted in Stata V.15.
Prior to assessing intervention effect on trial outcomes, we performed descriptive analysis on loss to follow-up (participants not available at 22 months), assessing whether loss to follow-up (LTFU) was associated with outcomes at baseline or with baseline predictors of the primary outcomes such as age of participant. There was no association between LFTU and outcome at baseline, or between LFTU and baseline predictors of the primary outcome (IPV).
Generalised linear models (GLMs) were used to compare outcomes at endline between control and intervention arms. For binary outcomes such as physical or emotional IPV, GLM with logit link was used to compare IPV experienced at endline between the two arms. GLM with Gaussian link function was used to compare mean scores at endline for continuous outcomes such as depression. Log transformation was used for past-month savings and earnings, and both were analysed using the tobit model due to the high clustering seen around zero in the data.
Adjustment was done for the baseline outcome variable of interest and age of the participant only, as no meaningful differences in the standardised mean differences of other predictor variables were found at baseline (table 2). We report percentages or means, unadjusted and adjusted estimates for GLM models with their 95% Confidence Intervals (CIs) and p values for all outcomes.
Sociodemographic and outcomes of the intervention and control arm, comparing standardised mean differences
Ancillary analysis
We also conducted a post hoc ancillary analysis of the three primary outcomes, stratified by participant’s level of food insecurity at baseline. In baseline analyses, food insecurity was associated with IPV,22 and in addition, there are sociological and economic theories which outline why poverty may be associated with IPV,7 29 described above. We hypothesised that because the intervention sought to impact on women’s food security, it may have differentially impacted on their experiences of IPV, depending on their food insecurity levels at baseline. Food insecurity was assessed through three items comprising the Household Hunger Scale, asking about household food insecurity in the past month. Scores were summed (range 3–12) and categorised into three levels (none, mild and severe) using the following cut offs: score of 3 was classified as no insecurity, score greater than 3 but less than 8 was classified as mild insecurity and score greater than 7 was classified as severe insecurity. The models adjusted for the outcome and age at baseline.
Procedures and randomisation
A local data collection firm was responsible for conducting the research activities, working closely with WfWI staff. Once appropriate communities were identified, WfWI staff engaged local community and religious leaders to secure access. This included getting religious leaders to speak about WfWI at Friday prayers. On an agreed day, WfWI staff and the research team went into communities to screen and enrol participants at women’s centres and other central points in a village. Local community leaders had pre-identified those they considered would meet the criteria around poverty.
Women who wanted to join the intervention were first briefed about it in small groups. Eligibility was then determined, though this proved challenging, particularly around age as many women did not know their age and few had official government identity cards with a date of birth. WfWI staff and enumerators made visual assessments and asked questions about life histories to best assess participant ages. A small proportion of those who were found ineligible came back masquerading as other people to try enrolling again, adding difficulty to this process.25
All participants were then given an explanation of the study and were told what participation would entail. They were told they could decline participation or withdraw from the study at any time. Due to low levels of literacy, participants provided informed consent by putting a thumb print on a form, witnessed by staff. If participants reported distress during research activities at any point in the trial, the enumerators referred them to support services.
Randomisation took place at the same time as eligibility screening and enrolment, prior to baseline data collection. Women were randomised in a public setting, using an opaque cloth bag filled with coloured balls that signalled study arm assignment. Women were told how the randomisation was to occur and they themselves pulled a ball out of the bag, which allocated them to the intervention or control arm one at a time. In some instances, women attempted to change the colour of the ball they pulled out to change their treatment arm assignment, but they were asked to redraw a new ball without looking. There was no blinding of arm allocation once the randomisation had occurred.
Once women had been randomised into each arm, women were invited to a scheduled baseline interview in the following 2 weeks. Quantitative interviews were done by the local data collection firm. All enumerators were female and received training from key research staff on survey content and interviewing techniques. Enumerators conducted face-to-face interviews with women in locations where auditory privacy could be assured. Interviews were done in either Dari or Pashto. Participants also provided information about where they lived, their father’s name, husband’s name (if currently married) and any other contact information they could provide. At midline and endline, enumerators used this information to locate and identify the participants and they completed interviews in the same way.
Data were double entered into an electronic database (SPSS at baseline, Epi-Info Endline) designed for this study. Discrepancies between data inputed were resolved through manual checking of the questionnaires.
Qualitative interviews
We conducted semi-structured in-depth interviews with intervention participants at endline. Due to security restrictions, the interviews were limited to participants in three communities in Kabul province. In total, 28 intervention participants were randomly selected for inclusion in this study by the research staff from the list of those who were randomised into the intervention. Women were approached by WfWI staff and asked to attend the interview. The interviews were conducted by a female consultant hired to undertake this component of the study. At the start of the interview, the interviewer detailed the research activity and participants provided informed consent for the qualitative study. Interviews were conducted in women’s centres or other spaces where auditory privacy could be assured for the interview. Interviews were conducted in Dari and audio recorded, then transcribed and translated into English by the consultant. Interviews lasted between 20 and 30 min. The topic guide covered women’s lives before and after programme participation, relationships with spouses and family members, reflections on violence/hardship in their own marriages and marriages in their community, experiences and learnings from the intervention, and a discussion about putting learnings from the intervention into practice.
Qualitative data were analysed using Attride-Stirling’s thematic analysis,30 using an inductive approach. Small sections of text were identified as basic codes,31 and these basic codes were grouped into themes and then clustered together into meaningful networks.
Patient and public involvement
Patients and the public were not involved in the design, implementation, analysis or dissemination of the study.
Findings
Recruitment and data collection
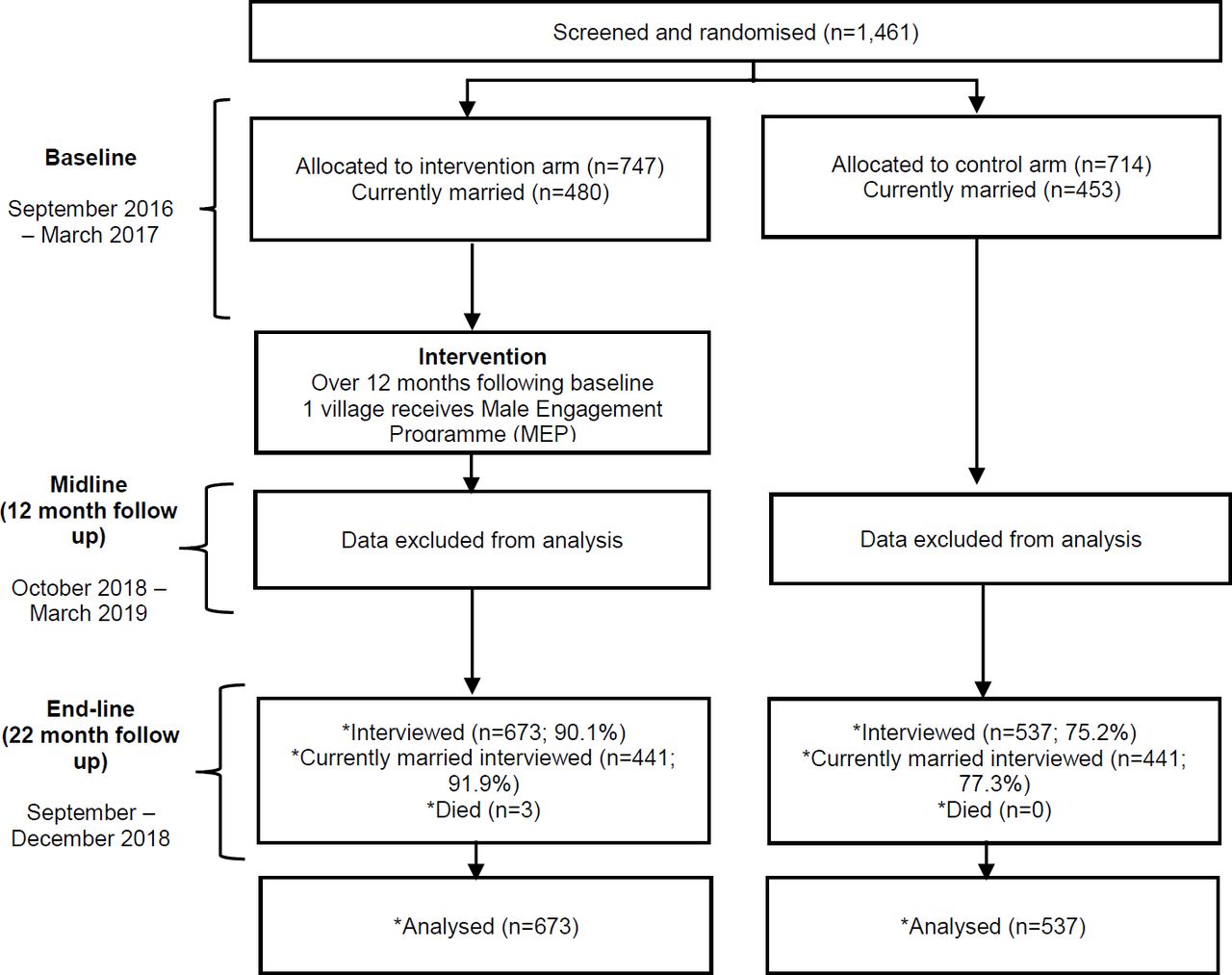
Figure 1 shows the trial flow diagram. Seven villages were approached to be part of the study. One village refused to participate because of the randomisation process. In total, four communities in Kabul and two communities in Nangarhar agreed to participate. Baseline (0 months) data collection took place between September 2016 and March 2017, with the intervention beginning shortly after surveys were completed in each village.

{kind=link}
Flow diagram of participants in the trial. MEP, Male Engagement Programme.
Midline data (12 months post-baseline), essentially constituting an immediate post-test assessment, were collected between October 2017 and March 2018. During the cleaning of the midline data, there were concerns that many respondents’ data (such as age, number of children etc) did not match logically with data from baseline. We did not identify the problem, unfortunately, until the end of the midline data collection.
In response to the problem during the midline data collection, and to prevent it reoccurring, we instituted additional screening and verification processes for the endline data collection. This included requesting additional information from participants for confirming their identity, hiring independent monitors to check the screening processes were being adhered to by the research field staff, and re-contacting participants seeking clarification if social or demographic characteristics provided seemed incongruent with earlier information. After reviewing data collected during endline, including discussion with participants about mismatches in what had occurred at the midline interviews, we decided to exclude the midline data from the analysis.
Endline data were at 22 months after the baseline data were collected and 10 months after participants completed the WfWI intervention. Data were collected between September and December 2018. The security situation deteriorated and data collection had to be halted early in one village at endline: the majority of missing data in this village was from the control arm.
Baseline data
At baseline, 1461 women were recruited into the trial comprising 98.9% of the target sample (n=1477). In a number of communities, we closed recruitment slightly early before reaching the full sample because of security concerns increasing the longer we worked in communities during the recruitment period. Overall, 63.9% (n=933) were married. Table 2 shows participants’ baseline characteristics, and there was no difference between arms (>0.2 for standardised mean differences).
At baseline, levels of each primary and secondary outcome were similar across groups (table 2). Past year IPV was common among married women, with a quarter (23.2%) reporting physical IPV, 15.6% reporting severe physical IPV and 25.6% reporting emotional IPV. There were no differences in mean scores for depression.
Numbers analysed
Follow-up rates at endline were 82% overall, and 84.8% among married women (figure 1). In one community, a sudden increase in insecurity prohibited the research team from locating and surveying many of the participants, specifically in the control arm, which led to a differential follow-up rate between the intervention arm (90.1%) and the control arm (75.2%).
Three participants died during the trial. All deaths were investigated and reported to the ethics committee for review; none were linked to study participation.
Outcomes and estimations
Table 3 shows the primary outcomes at endline. There were no statistically significant differences between arms for past-year physical IPV (adjusted OR (aOR) 0.88 (0.62 to 1.23), p=0.447), severe physical IPV (aOR 0.75 (0.50 to 1.11), p=0.15) or depressive symptoms (β −0.35 (−1.19 to 0.48), p=0.406), although all measures changed in the hypothesised directions.
Primary and secondary trial outcomes, unadjusted and adjusted outcomes
There was evidence of greater gender equality and decision-making power among women in the intervention (table 3). Women reported significantly less gender-inequitable attitudes (β −0.89 (–1.15 to –0.62), p<0.001), and married women’s decision-making in households was improved (β 0.35 (−0.04 to 0.74), p=0.078). In addition, among all women, those in the intervention reported greater mobility in the past year (aOR 1.78 (1.27 to 2.50), p=0.001). There were no other suggestions of changes in other forms of violence women experienced (emotional or from others in the household) or perceptions of cruelty in relationships.
At endline, women in the intervention reported significantly improved livelihoods. Household food insecurity was significantly reduced in the intervention (β −0.48 (−0.85 to –0.12), p=0.01), and both earnings in the past month (β 3.79 (0.96 to 6.61), p=0.009) and women’s mean overall savings (β 11.79 (9.95 to 13.64), p<0.001) were significantly higher in the intervention group.
Ancillary analyses
Among women at baseline reporting moderate levels of food insecurity, there were consistent patterns in changes in primary outcomes for IPV, indicating the intervention had greater effect on these women (table 4). Specifically, women with moderate food insecurity at baseline reported reduced past year physical IPV (aOR 0.47 (0.22 to 1.01), p=0.052) and severe physical IPV (aOR 0.38 (0.16 to 0.93), p=0.034). In this subgroup, there was no impact on depressive symptoms (−0.70 (−2.32 to 0.93), p=0.400). There were no differences with those reporting no food insecurity or severe food insecurity in terms of outcomes at endline.
Ancillary analyses of primary outcomes by food insecurity levels at baseline
Qualitative analysis
Table 5 provides information on the 28 women involved in the qualitative study. In two of the communities, the majority of women had migrated to Kabul province. Many of the women reported first being displaced to Pakistan (and in one case Iran) during conflict before coming to Kabul province, while the rest reported migrating because of poverty. In the third community, six of nine women reported having to leave the community during the period when the State was controlled by the Taliban, and were in Pakistan as refugees before returning to the same community after the fall of the Taliban. Few women knew their specific age, but we reconstructed likely ages based on the age of their children and age at marriage.
Summary of participant information from qualitative data
The thematic inductive analysis identified four themes around the intervention: the importance of social networks, how livelihoods training was received and acted on, savings and the role of the cash transfer, and women’s rights and decision-making. These are described and illustrated before being integrated in the discussion.
Social networks
Almost all women reported enjoying attending the intervention and women described multiple benefits of the sessions they attended including a greater sense of well-being and making new connections. In contexts where women were not able to easily move outside the home and make new friends, the intervention provided an opportunity for women to do this:
Interviewer: After the course, what has changed in your life, your relationships with others?
Community 2, Woman 5: My life has improved. The year that I was in this course, when we came here once a week, we met other women and made friends, it was a good change for me.
Another woman similarly reported how the intervention was important in building new relationships:
Community 3, Woman 7: It was good. I used to meet with the women. It was good recreation for me.
Basic education
Many women reported that the intervention supported them to learn the alphabet and basic numeracy:
Community 2, Woman 2: When I joined I could not read even Aliph (first letter of the alphabet). It was very difficult (laughs). I learned 1, 2, 3, up to 100.
Interviewer: What else did you learn?
Community 1, Woman 10: There were also the other things we learned that were very useful, like numbers. Before that we didn’t know the numbers to dial on the phone. Now I do…
In contexts where education opportunities had been removed from many women over the past 20 years, this provided women with both basic skills and knowledge, and also an increased sense of confidence.
Livelihoods
Almost all the women described learning about livelihoods during the intervention. The range of livelihoods women learnt about varied based on community and the specific training group women were in (table 5), but included animal husbandry, growing mushrooms, sewing/embroidery and knitting. One woman described how she had learnt knitting and used to it knit clothes for her baby, as well as selling knitted clothes:
Interviewer: How did you find the course?
Community 1, Woman 4: It was very good. We would come once a week, until lunch, and the teachers would come and teach us things. They told us to do business and taught us to knit, and said take it to the market and sell it.
Interviewer: Did you learn to knit?
Community 1, Woman 4: Yes, I did. I made some things for my baby… (and) I knit jackets for money.
Some women, particularly those taught sewing and embroidery, found their vocational skills training did not lead directly to income generation but allowed for important financial savings for them and their families:
Interviewer: Among everything you learned, what was most important to you? How have you used it? How did it help?
Community 2, Woman 7: The sewing. I now sew my own and my girls’ clothes. That is also a saving. If I go to a tailor, he will charge at least AFS100 or AFS50. Now I can sew their clothes myself.
Other women said they had struggled to translate the knowledge they had gained during the intervention into a livelihood, often citing a lack of money as hindering this:
Interviewer: You learned about keeping cows and about poultry?
Community 3, Woman 10: Yes. We learned about them.
Interviewer: Then what did you do with what you learned?
Community 3, Woman 10: Nothing. I don’t have anything with which to buy something. But, I have interest, I am very interested in having a cow.
Similarly, a woman from the same community who also learnt about animal husbandry described how while she was interested in this, she could not apply it to her life: “I don’t have space” (Community 3, Woman 7). In some other cases, women tried to implement the livelihood skills they had been taught, but when this failed to generate money, they stopped the activities.
Interviewer: And what did you learn?
Community 1, Woman 1: Yes, lots of things. They taught us many good things. It was good.
Interviewer: Can you remember any of the things they taught?
Community 1, Woman 1: They taught us to grow mushrooms, and gave us spores. I tried but didn’t get much produce and then there were no spores. I don’t have a proper place to grow them. You need a separate room… Very little was produced.
Some women described how unresolved health challenges affected their abilities to make sewing and embroidery their livelihoods:
Community 2, Woman 2: I used to do embroidery but now my eyes have become weak.
While many women described learning numeracy and literacy, some women suggested that a major challenge in embedding learnings was their overall lack of literacy, and how this impacted negatively on general learning. As one woman described:
Community 1, Woman 1: (laugh) Yes. I forget what I learned. I’m a non-literate person. I learn something and then after a few hours I forget everything.
The struggles that many women reported in translating their knowledge about livelihoods learnt in the intervention into meaningful actions and changes in their own lives highlights the overall challenge of livelihoods strengthening approaches in Afghanistan.
Savings
A key component of the intervention was the development of savings groups. In two of the communities, many women described how the savings groups, which were established during the intervention, continued after the WfWI staff finished working with them:
Community 3, Woman 6: …We would save AFS50 a month (during the intervention). We continue to save AFS50 a month. It is more than a year now. I think each of us has AFS1100 saved so far.
Another woman described how she had developed a habit around saving that she continued today:
Community 2, Woman 7: I learned that saving money is important. In the past if I had AFS100, I spent AFS100, and if I had more, I spent all of it. I learned to save some for when I need it. Now I save a little all the time from my expenses.
However, in many communities, savings groups were not implemented fully during the intervention, and even in communities where they were, some women struggled to participate in savings groups. Not all intervention groups established savings groups as this was discretionary: “We didn’t have a savings group. We didn’t have extra money to save” (Community 1, Woman 5).
Other women described not having enough money to be part of the savings groups:
Interviewer: Are you in a saving group?
Community 3, Woman 10: No. When they started the groups, I didn’t have money, so I couldn’t join. Later, when I wanted to join a group, they said you can’t join in the middle.
Cash transfer
The logic of the cash transfer was that it would provide an incentive to support women’s attendance and provide a level of cash to deal with basic needs and a platform for starting livelihood activities. All the women described the importance of receiving the US$10 per month for intervention attendance. Women were clear that the cash did make attendance much easier, with men actively supporting women to attend to ensure they received the cash, and a number of women describing the cash transfer as a “payment”.
Women additionally described using the cash in three main ways. First, all women described its importance in being able to take care of themselves and their family, without having to ask their husband for money. However, this often stopped them investing in livelihoods:
Community 3, Woman 1: I have used it well myself. For example, if my child falls ill I take him to the nearest healthcare centre quickly. Regarding business, the money they gave me, I couldn’t do any business. I spent it to buy clothes, or school bag or other things the children needed. Because my husband’s salary was not enough to satisfy their needs.
Second, a few women described saving a portion of this cash for future emergencies. This was never the full amount, but was a small portion and enabled them to start savings groups.
Community 3, Woman 8: We started saving money. We would save AFS50 each month from what we got. We still save AFS50 each month. Sometimes we borrow from it when we need it. It is not a lot; it may be around AFS1500 now, but that is the benefit.
Third, some of the women described how they invested their cash in paying for school fees for their children, which they clearly saw as a long-term investment:
Community 2, Woman 1: For some months, it helped pay the fees for the English language course my son attended.
Community 3, Woman 2: It was money. I used to take the US$10 and give it to my son to use it to pay for his course. I did not spend it at home.
The cash that women received during the intervention was incredibly important for them but, given the high levels of poverty women experienced, cash was often spent on short-term immediate needs rather than invested in long-term productive livelihoods, although some women did use it for their children’s education. As such, cash did not provide a springboard for stronger livelihoods.
Women’s rights and decision-making
A key aim of the intervention was to strengthen women’s decision-making power in relationships with their husband and, in addition, to strengthen women’s knowledge of laws related to women’s rights, including divorce and violence against women. A few women described how after the intervention they had greater ability to discuss issues with their husband, as one woman explained when asked how things had changed after participating in the intervention:
Community 1, Woman 1: My life has changed in that I can do things myself. If my husband says something, I can explain my idea about it.
Another woman emphasised how she learnt to express herself and felt empowered after the intervention:
Community 2, Woman 1: This group, the course itself, made me feel empowered in a special way. It made me feel I could make something of myself, and be self-dependent. Before that I was very timid; I couldn’t even talk properly to express myself.
There were limits, however, to women’s ability to impact decision-making processes within the household. One woman described how she was now confident to suggest something to her husband, but would back down quickly if he disagreed with her:
Interviewer: Do you ever have disagreement about anything? What happens when you disagree about something?
Community 2, Woman 8: Well one has to be careful not to do anything that would make a man angry. I might suggest something, but if he does not agree, I do as he wants.
Interviewer: What would happen if you disagreed? What would he do?
Community 2, Woman 8: It is up to the man. I listen to what he wants and do it.
Similarly, another woman also described how she would always concede in any discussion if there was disagreements between her and her husband:
Interviewer: What happens when you and your husband have a disagreement?
Community 1, Woman 6: No, I try to make sure it doesn’t happen.
Interviewer: So nothing makes him angry?
Community 1, Woman 6: It can happen that I think one thing should happen, and he thinks it another thing should happen. Then he disagrees and I accept his decision.
Women also could not contemplate the option of leaving their husband. In Afghanistan where woman-initiated divorce is incredibly rare and all divorce is highly stigmatising for women, many women described how women should try and tolerate abuse and violence and make a relationship work:
Interviewer: Are there people who are unhappy in their marriage? Why would someone be unhappy with their husband? Wife? What happens when women are unhappy with their husband?
Community 2, Woman 3: Of course people can be unhappy in marriage. Maybe because of money matters, or the husband is very strict or something.
Interviewer: What can the woman do if she is unhappy with her husband? Can she leave him? What could happen if she left him?
Community 2, Woman 3: She has no choice but to tolerate it. What can she do? She has nowhere to go. She must put up with it.
Some participants did acknowledge that a few women did get divorced. One mentioned she had heard it happening “among people who went abroad, it has happened among my relations. But not here”. Another woman, while recognising divorce was a potential option for women in Afghanistan, framed any woman who took that as being a bad woman: “Some women who are not from good families may leave their husband” (Community 3, Woman 9).
Broadly, the intervention supported women to understand their rights under the law, which given the context was incredibly important, and also strengthened women’s ability to raise issues in the home. However, women could not effectively contest their husband’s dominance, nor could they contemplate leaving violent relationships as the wider context did not allow this.
Discussion
Overall, women participating in the WfWI economic and social empowerment intervention did not see a reduction in their experience of IPV or depressive symptoms after exposure to the intervention. However, for a sub-group of women, those with medium levels of food insecurity at baseline, there is evidence that it did reduce their experiences of past year physical IPV and severe physical IPV by endline. Overall, women did show significant benefit in their livelihoods from participation in the intervention, although the proportion of earning and saving at endline was still low. Compared with the control group, women in the intervention reported mean earnings 39% higher, and total savings were over six times greater. Food insecurity was also significantly reduced. In addition, women in the intervention reported more gender-equitable attitudes, and there was a suggestion of greater decision-making by endline and increased mobility outside of their community.
Interpretation
Overall, there is strong quantitative and qualitative evidence that participation in the WfWI economic and social empowerment intervention incrementally strengthened women’s livelihoods and economic well-being. This is one of the few rigorous evaluations of an economic and social empowerment intervention in a conflict-affected setting and the evidence of value from the intervention for women is important.
The stronger economic well-being for women is an important outcome in and of itself, and women’s improved economic status is associated with improvements more widely for women’s health and well-being.32 33 In contrast to research that suggests that some women’s economic empowerment programming can increase women’s experiences of IPV,6 there was no suggestion that this occurred. The qualitative and quantitative results indicate that there is potential for more progress on economic empowerment and the lessons from the qualitative research provide important pointers for future strengthening of the intervention. In very conservative Islamic contexts, such as in neighbouring Tajikistan, a pilot study showed strong benefit in economic empowerment and changing gender relations from a family-centred intervention that included young married women, their husband and in-laws in the intervention, and this may also be a useful model for Afghanistan.34
There was evidence that among intervention participants, gender attitudes had become more equitable, and women had greater decision-making power in households and also more mobility. Women’s lack of decision-making power within the home has been associated with worse health outcomes for their children in a systematic review.33 And greater mobility for these women in contexts where mobility was often highly constrained is very important. Qualitative data, however, showed that the improvements in women’s decision-making power within the household were likely incremental, rather than very substantial.35 The qualitative data suggested that while the intervention supported women to raise their concerns, or make suggestions to their husbands, they felt unable to challenge their husband if he disagreed. An ongoing debate remains about the extent to which these small actions constituted significant changes for the women given the overarching context of extreme gender inequality.36 As such, while these changes did not lead to reductions in women’s experiences of IPV, it may be that these are important changes for the women in their own lives.35
For a subgroup of women who reported moderate levels of food insecurity at baseline, their experiences of physical IPV were significantly reduced through participation in the intervention by endline. Studies have highlighted how food insecurity and quarrelling about lack of food can be a driver of IPV.7 22 One possible explanation for the positive finding that was seen is that households who were moderately food insecure at baseline could benefit the most from strengthened livelihoods seen at endline compared with those with no food insecurity (and therefore where limited change was possible) and those with severe food insecurity where change was harder to establish. If this is the case, it is suggestive that the intervention’s impact on reducing this group of women’s experience of IPV was through reducing the stress of food insecurity within the household. Additional research on whether the reduction in food insecurity was the pathway through which IPV was reduced in this group is required.
Economic theories of IPV at the household level posit that strengthening women’s economic position, particularly when combined with working on women’s social empowerment, should reduce women’s experiences of IPV.29 Given that women’s economic position improved and there were indications of greater gender equity and women’s enhanced power within households, a key question remains as to why this did not reduce IPV overall. We suggest three potential reasons this may not have happened. First, women’s options for negotiating their relationship were highly constrained. A key component of economic theories of IPV is that with resources women can be independent, that is, women’s bottom line in negotiating violent relationships is her exit, but this was not a viable option for the women in the study. In Afghanistan, while divorce is legal, it remains highly stigmatised, more so if woman initiated, and leads to women losing access to their children and family support.37 38 There are very few shelters available and these are located only in major urban centres. Further, women who go to shelters face major challenges leaving and reintegrating into communities.38 This was clearly seen with the qualitative data, where divorce remained something that women could not even consider, and women who did divorce were considered morally ‘wrong’.
Second, while there were significant improvements in measures of livelihoods, they were small. Qualitative data highlighted the multiple challenges women faced in implementing the livelihood strategies that they had been taught such as lack of start-up capital, limited space for activities, failure to sustain harvests and health challenges. It also pointed to the very substantial difficulties faced by women who have never been to school and who, as we know from the research, had so often experienced trauma with enduring impact on their mental health.4 While a year seems long for a programme, it was very short for the very substantial body of ideas, attitudes and knowledge that women were expected to absorb and be able to act on, particularly for women who had limited or no prior experience of a classroom learning environment.
In total, only 9.7% of women in the intervention at endline reporting earnings in the past month (compared with 5.6% in the control), highlighting the limited economic opportunities for women. Similarly, while saving was something women in the qualitative data reported commonly in two of the communities, overall only a third (29.1%) reported household savings in the intervention arm (compared with 3.7% in the control), and this was primarily driven by two communities reporting very high rates of saving. This also reflected household poverty and difficulty in making savings. As such, while earnings or savings may have translated into important improvements for women who were able to attain them, the overall lack of uptake of these earnings and savings may have limited the potential for strengthened economic position to impact on IPV experience more widely. Additional research is needed to further understand whether modifications to the cash component of the intervention may lead to higher and sustained economic gains, increased participation in savings and larger business investments.
The third potential reason that there was no overall impact on IPV may be because of the way that gender power operates in Afghanistan. Gender inequality is deeply entrenched and incremental advances may not amount to a tangible increase in women’s power, especially for young women. Women’s mobility is also highly limited, and their access to education, livelihoods and healthcare are usually mediated by husbands, other male family members and/or older women.39 In this context, working individually with women may not be enough to effect change, as individual women may have relatively little ability to renegotiate power in a household or implement new livelihood strategies. As such, it is important to consider working with whole households, recognising that household dynamics need to change and that livelihoods strategies may operate more effectively with household involvement.34
The limited impact on depressive symptoms in the intervention group is likely due to two reasons. First, studies have emphasised the lingering effects of conflict and trauma on people’s poor mental health, even many years after formal conflict had ended.4 In addition, in Afghanistan there remained high and increasing insecurity in the communities we worked in.20 Second, significant drivers of depression include IPV, poverty and generalised disempowerment.16 The overall lack of effect is unsurprising given many of these outcomes did not change significantly for the intervention recipients.
Limitations of the study
This study has a number of limitations. The study was conducted in a very fragile setting and this constrained staff mobility and the study design. We were not able to conduct ongoing qualitative research during the study due to access and security issues, although this would have been desirable to assess and record changes as they happened. Randomisation occurred before baseline data collection was undertaken, although after recruitment into the study. Women may have answered questions differently expecting they would receive additional benefits depending on arm allocation, but it is unclear how this would affect bias. Randomisation was done at the individual level and there is risk of contamination between arms. Given the intensive nature of the intervention (twice a week for 12 months), and restrictions on women’s mobility and social interactions outside the home, it is unlikely women could share significant learnings. We recognise that studies of this design are often undertaken as cluster randomised controlled trials to better avoid contamination, but we were unable to do this due to limitations in number of villages accessible due to security concerns. We sought to ensure only one woman from a household was recruited into the study, and while we think we successfully achieved this, we cannot be sure. Questionnaires were completed through face-to-face interviews by trained research staff given the overall levels of literacy, and this could have changed participants’ responses, though studies from the Asian continent have shown face-to-face interviews are acceptable.40 We collected data at 12 months (shortly after intervention completion) but did not include it in the analysis because of concerns that we had not correctly tracked and identified some participants. As such, we cannot look at whether changes occurred immediately following intervention completion. For a number of measures (earnings and savings), the baseline measures did not make conceptual sense, and both intervention and control arms changed significantly over time. Reviewing the data implied that baseline measures captured household rather than individual measures, and for these outcomes in the adjusted analysis we only adjust for age. Last, due to increased insecurity in one community visited by the research team, the research activities had to be cut short and many control arm participants were not surveyed. As such, we have differential attrition between arms and this may have affected outcomes, although it is unclear in what direction. We do not have information on intervention attendance and fidelity to the intended model, as while this was collected by the NGO during its ongoing work, we did not have the funding to extract this and link this to trial documentation. A per-protocol analysis would have allowed us to assess the effectiveness of the intervention among those who attended more sessions. The trial structure does not allow for assessing if the intervention in its full package was most beneficial for women or whether it could have been shortened or should have had particular aspects enhanced. In the discussion, we emphasised the benefits of the economic component, but we do not know if it was the vocational training, cash transfer given during training or both that benefited women economically. Our hypothesis is that both were important but we have not tested this.
Conclusions
This evaluation of the WfWI economic and social empowerment intervention is one of the few large-scale trial evaluations in conflict/post-conflict settings looking at whether such interventions can have impacts on women’s experiences of IPV and depression. This study shows that long-term economic and social empowerment interventions can lead to significant improvements in livelihoods for women and more gender-equitable attitudes, greater decision-making in the household and greater mobility, even in a context as challenging for women as Afghanistan. However, this did not translate into overall reductions in IPV or depressive symptoms, although there were suggestions of reduced IPV for a subgroup of women with moderate food insecurity at baseline. Previous smaller-scale evaluations in conflict-affected populations have also showed limited impact on IPV outcomes, suggesting that economic strengthening and gender-transformative interventions that are successful in more stable contexts and populations may have challenges in translating to conflict-affected settings.
There are a series of important future research questions that emerge from this trial. First, there is an urgent need for more large evaluations to see what modifications are needed for combined economic and social empowerment interventions to reduce IPV in conflict and post-conflict settings around the globe. Second, further research is required to understand how to translate the positive findings on gender attitudes, decision-making and livelihoods in the trial into sustained reductions of IPV for Afghan women. Third, future trials should be adequately powered to assess the hypothesised pathways through which changes in livelihoods, gender attitudes and relationships can potentially impact on IPV outcomes, and not just on the primary outcome. Fourth, future trials should assess whether such interventions are more effective when delivered to individual women or to households in contexts such as these, where women’s power is constrained by her husband and other family members. Combined economic and social empowerment interventions such as WfWIs show promise and need to be optimised to effectively reduce women’s experiences of IPV.
Acknowledgments
We would like to thank the participants who gave up their time and provided us with the information for this study. We also acknowledge all of the enumerators and data collection team leads at Sayara International and Eureka Research who conducted this research across difficult terrains. Last, we would like to thank all of the WfWI staff who worked to implement the intervention and support the research activities.
References
Footnotes
Handling editor Seye Abimbola
Contributors RJ, AG, EC, JC, CM, FK and SM designed the study. CM-J and JC collected the data and oversaw data quality and processing. FK, EN, SM and AM oversaw the intervention implementation. EC, JC, RJ and AG did the data analysis. All authors contributed to the interpretation of the analysis. AG wrote the first draft of the paper. All authors reviewed and contributed to the draft paper. All authors approved the final submission.
Funding The research for this study is funded through the What Works to Prevent Violence Against Women and Girls? Global Programme, by the UK Department for International Development (DfID), and managed by the South African Medical Research Council.
Disclaimer The funders had no involvement in the study design, data collection, analysis or interpretation of the study.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Ethical approval for the randomised controlled trial was given by the South African Medical Research Council (EC034-11-2015) and the Afghan Ministry of Public Health (399302), and separately for the qualitative research study (EC031-10/2016). All women provided thumb prints (because of low levels of literacy) and these were witnessed by study staff.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. De-identified data sets for the project are available from http://medat.samrc.ac.za/index.php/catalog/WW managed by the South African Medical Research Council.