Article Text

Abstract
Introduction Managing paediatric hydrocephalus with shunt placement is especially risky in resource-limited settings due to risks of infection and delayed life-threatening shunt obstruction. This study evaluated a new evidence-based treatment algorithm to reduce shunt-dependence in this context.
Methods A prospective cohort design was used. The CURE Protocol employs preoperative and intraoperative data to choose between endoscopic treatment and shunt placement. Data were prospectively collected for 730 children in Uganda (managed by local neurosurgeons highly experienced in the protocol) and, for external validation, 96 children in Nigeria (managed by a local neurosurgeon trained in the protocol).
Results The age distribution was similar between Uganda and Nigeria, but there were more cases of postinfectious hydrocephalus in Uganda (64.2% vs 26.0%, p<0.001). Initial treatment of hydrocephalus was similar at both centres and included either a shunt at first operation or endoscopic management without a shunt. The Nigerian cohort had a higher failure rate for endoscopic cases (adjusted HR 2.5 (95% CI 1.6 to 4.0), p<0.001), but not for shunt cases (adjusted HR 1.3 (0.5 to 3.0), p=0.6). Despite the difference in endoscopic failure rates, a similar proportion of the entire cohort was successfully treated without need for shunt at 6 months (55.2% in Nigeria vs 53.4% in Uganda, p=0.74).
Conclusion Use of the CURE Protocol in two centres with different populations and surgeon experience yielded similar 6-month results, with over half of all children remaining shunt-free. Where feasible, this could represent a better public health strategy in low-resource settings than primary shunt placement.
- child health
- meningitis
- cohort study
- health education and promotion
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Hydrocephalus is a significant cause of childhood morbidity and mortality in low-income and middle-income countries.
Ventriculoperitoneal shunt placement has been the standard of care, but the high long-term failure risk makes shunt-dependence more dangerous in settings where emergency access to neurosurgical care is limited.
What are the new findings?
We validated a novel treatment protocol for childhood hydrocephalus in sub-Saharan Africa, demonstrating similar results in two sub-Saharan African countries, with disparate patient populations.
Using the CURE Protocol, with its emphasis on primary use of endoscopic treatment, more than half of all children with newly diagnosed hydrocephalus were successfully treated without a shunt at both centres.
What do the new findings imply?
Half of all children presenting for treatment of hydrocephalus, regardless of aetiology, can be treated without shunt placement.
Such outcomes can be achieved at smaller volume, less experienced centres, after an appropriate period of training.
Endoscopic management of hydrocephalus could represent a better public health strategy in low-resource settings than one in which shunt placement is the standard primary treatment.
Introduction
The most recent estimate of the global burden of hydrocephalus worldwide reports close to 400 000 new cases each year, with approximately 82% of those cases occurring in low-income and middle-income countries and 47% occurring in sub-Saharan Africa alone.1 Although these cases are readily treatable with a ventriculoperitoneal shunt (VPS), the main challenges inhibiting adequate treatment in sub-Saharan Africa include: a paucity of neurosurgeons, equipment and infrastructure deficiencies, and significant economic and geographic obstacles to accessing both initial treatment and, in particular, emergency treatment for shunt failure. These circumstances drove the development of an alternative treatment algorithm for paediatric hydrocephalus at CURE Children’s Hospital of Uganda (CCHU), in Mbale, Uganda.
The CURE Protocol presented here is based on our ongoing experience in this dedicated paediatric neurosurgery hospital in East Africa that, since its inception in 2001, has treated upwards of 10 000 children for hydrocephalus. The protocol employs endoscopic treatment, rather than shunt placement, as the primary approach in the majority, with the over-arching goal of optimally treating hydrocephalus while avoiding long-term shunt dependence whenever possible. Endoscopic treatment involves performing endoscopic third ventriculostomy (ETV), usually combined with endoscopic choroid plexus cauterisation (ETV/CPC). The long-term failure rate for shunts is much higher than for endoscopic treatment. Unlike shunts, which can, and typically do, fail and require emergency revision over the course of the patient’s life, the majority of endoscopic treatment failures occur within 6 months of surgery, in a manner that is obvious to the family, and usually sub-acutely or chronically, allowing time for the family to return for evaluation. Our previous research, including a recent randomised trial,2 has shown either superior or similar outcomes between endoscopic treatment and VPS with respect to infection, seizure incidence, morbidity, and mortality as well as no difference in early developmental outcome and brain growth.3–8 We have also demonstrated equivalence of the initial cost between the two treatments, with significantly increased cost of treatment by VPS with each required revision.9
In Uganda, since 2005, the CURE Neuro programme has trained neurosurgeons from other low-resource countries and provided the necessary equipment to implement the CURE Protocol in the context of their own centres.10 In this report we provide details of the protocol and the outcome of its implementation among all children presenting to CCHU for hydrocephalus treatment. We also provide an external validation of the protocol’s effectiveness when implemented in Lagos, Nigeria, after the provision of training and equipment through the CURE Neuro programme.
Methods
Study design
Using the Strengthening the Reporting of Observational Studies in Epidemiology criteria, a prospective cohort design was used to compare outcomes of surgical management for paediatric hydrocephalus between the two sub-Saharan African centres during a defined time period with minimum of 6 months of follow-up.
Initial patient assessment
Our management protocol involves a systematic approach to initial patient evaluation as follows. Patients are evaluated clinically and with cranial CT or ultrasound, since MRI is not available. Symptomatic hydrocephalus in children is defined as ventriculomegaly in conjunction with at least one of the following: abnormally increasing head circumference crossing percentile lines, sunsetting of eyes, abnormal irritability/vomiting, decreased level of consciousness, poor feeding, bulging fontanel with child upright and quiet, distended scalp veins or symptomatic type 2 Chiari malformation following closure of myelomeningocele (eg, stridor, swallowing difficulties, etc). Isolated ventriculomegaly and macrocephaly alone are insufficient criteria for intervention; such patients are subsequently followed to look for progressive ventriculomegaly, abnormal rate of head growth, or the development of symptoms.
The diagnosis of postinfectious hydrocephalus is determined, according to previously published criteria, when there is no evidence of hydrocephalus at birth, and either a history of febrile illness preceding development of macrocephaly or endoscopic or imaging evidence of prior ventriculitis (or both).2 All other causes of hydrocephalus are categorised as either non-postinfectious or related to myelomeningocele.8
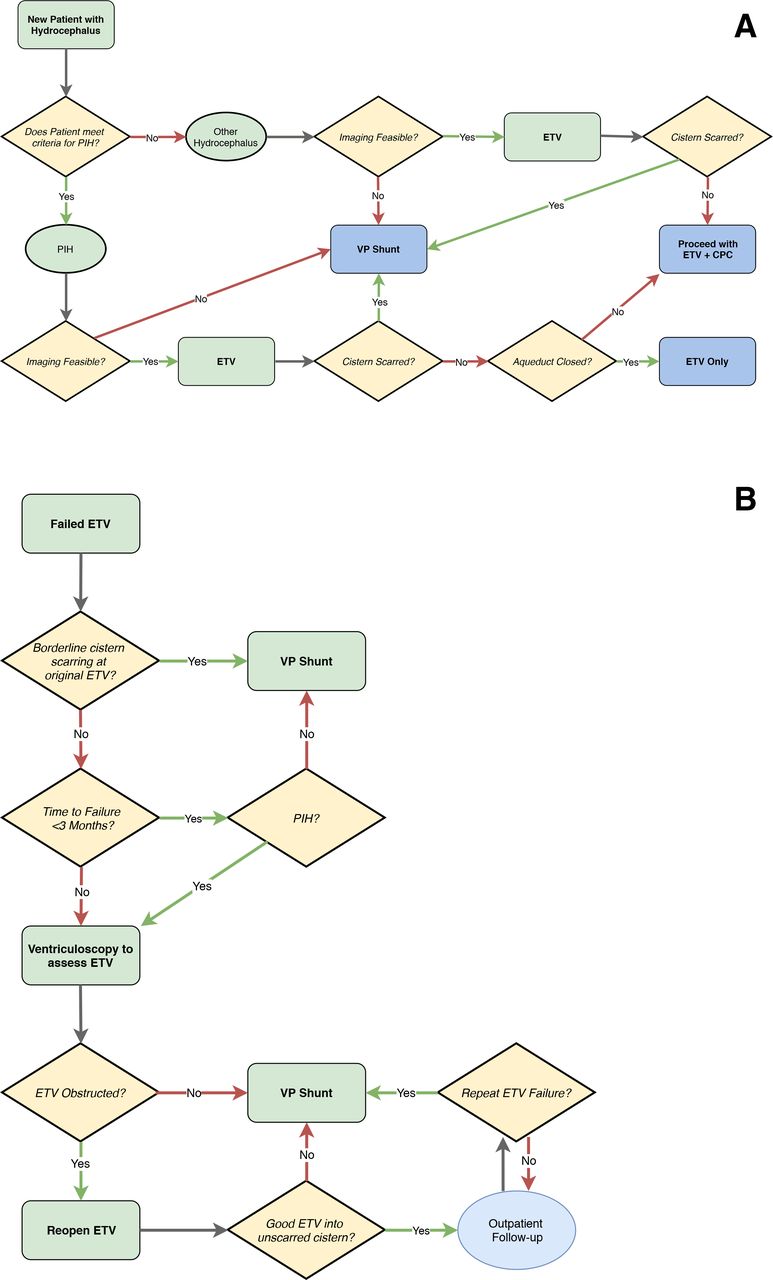
Prior to surgery, patients undergo a ventricular tap for cerebrospinal fluid (CSF) assessment to ensure sterility and sufficient clarity of the CSF. Bloody, murky or infected CSF prompts placement of a ventricular reservoir for serial tapping until the CSF has cleared. After initial assessment, all children <2 years of age requiring intervention are treated according to the CURE Protocol (figure 1A). Older children presenting for treatment are managed similarly except that CPC is not employed in conjunction with ETV.
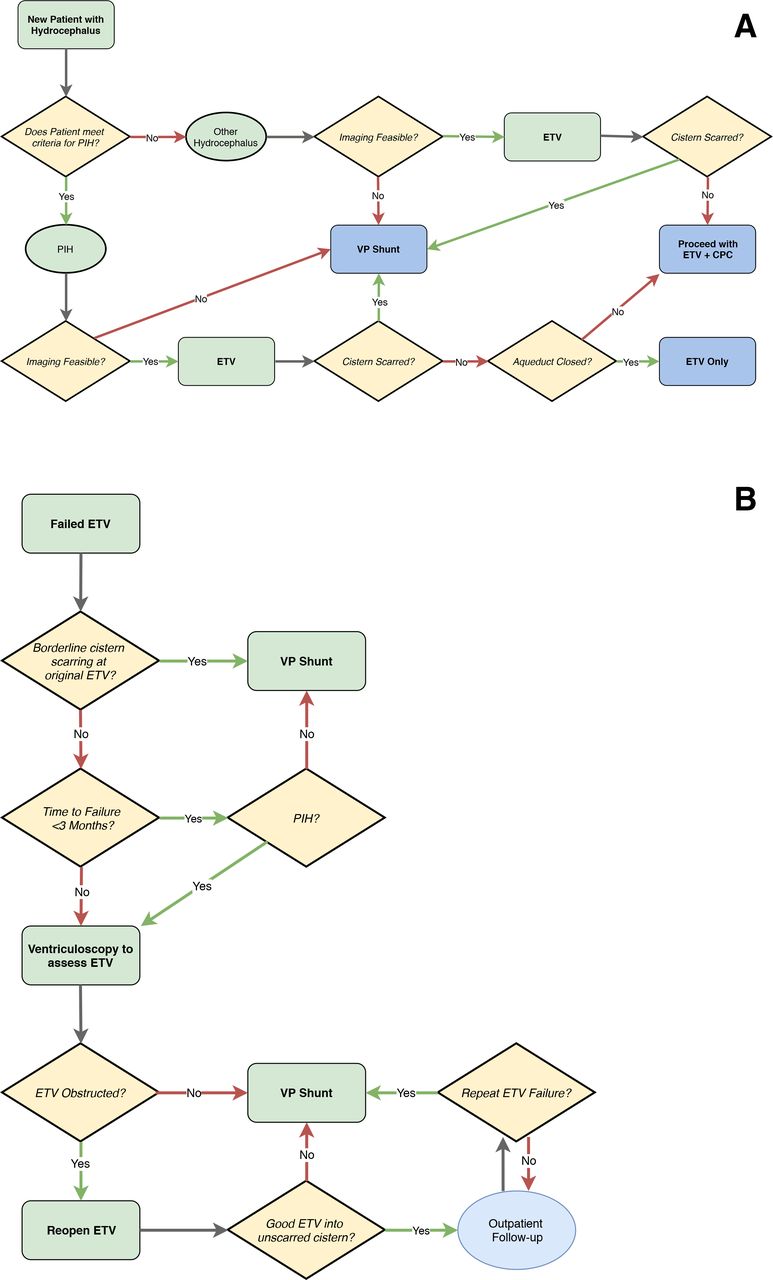
The CURE Protocol algorithm for (A) initial treatment and (B) treatment failure of paediatric hydrocephalus. Imaging feasible=anatomic feasibility of safely performing the ETV±CPC, as demonstrated by preoperative imaging study. CPC, choroid plexus cauterisation; ETV, endoscopic third ventriculostomy.

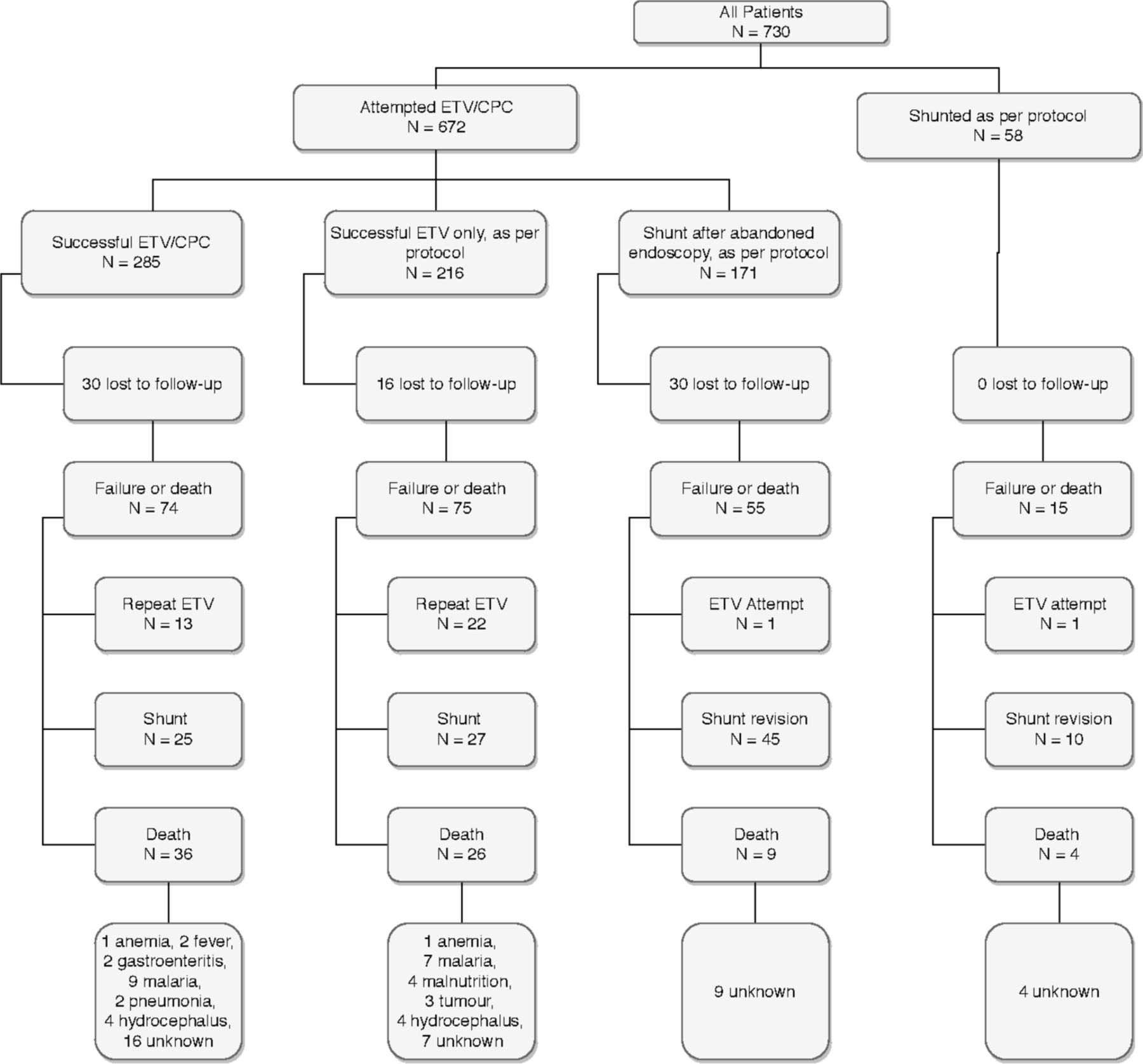
Treatment pathway for all 730 children presenting to Mbale, Uganda with newly diagnosed hydrocephalus. CPC, choroid plexus cauterisation; ETV, endoscopic third ventriculostomy.
The CURE Protocol
Algorithms for initial surgical treatment and management of treatment failure are presented in figures 1 and 2, respectively. The CURE Protocol is based on previously published analyses of outcomes data from CCHU, including a validated ETV/CPC success prediction score, which quantifies the prognostic effects of age, aetiology and degree of CPC; the latter was found to be the most heavily weighted factor predicting success.11 12 We have shown that ETV/CPC is effective in most types of hydrocephalus,8 13–17 and that initial endoscopic treatment does not subsequently affect long-term shunt outcomes in those for whom endoscopic treatment was abandoned or failed.18 A recent randomised trial has confirmed that treatment outcomes with respect to neurocognitive developmental, brain growth and most complications (aside from a higher infection rate for shunts) are similar for ETV/CPC and VPS in patients aged <6 months with postinfectious hydrocephalus.2 A post hoc analysis also demonstrated no difference in seizure incidence between the treatment groups.7
The CURE Protocol, therefore, emphasises a primary attempt at endoscopic treatment, unless the preoperative imaging suggests this is not technically feasible. No patients underwent surgery at either location without undergoing cranial imaging—either CT or cranial ultrasound. Findings at the time of endoscopy then dictate when ETV should be supplemented with CPC or abandoned in favour of shunt, according to the evidence-based algorithm. For example, if there is a diagnosis of postinfectious hydrocephalus and obstruction of the aqueduct of Sylvius is observed at endoscopy, then ETV alone is performed without CPC.8 As well, if, after completing the ETV, scarring of the prepontine cistern is discovered, then a shunt is placed under the same anaesthesia because the chance of ETV or ETV/CPC success is low in those patients.19 If the original imaging shows such anatomic distortion due to infectious loculations, intraventricular scarring or other congenital causes, such that endoscopic access to the floor of the third ventricle appears untenable or unsafe, a shunt is primarily placed, although this may be in concert with endoscopic fenestration of ventricular loculations, if necessary.
The technique for ETV/CPC developed at CCHU has been described in detail elsewhere.8 Briefly, a flexible ventriculoscope is passed into the right lateral ventricle and the floor of the third ventricle is fenestrated, thus completing the ETV. The majority of the choroid plexus (typically >90%) in the right lateral ventricle is then cauterised. If the septum pellucidum separating the two lateral ventricles is intact, it is endoscopically fenestrated before directing the endoscope into the left lateral ventricle where the majority of the choroid plexus is similarly thoroughly cauterised. When shunt placement is necessary (either as the primary procedure or when the ETV has been abandoned), a standard right frontal ventriculoperitoneal shunt is placed using the inexpensive Chhabra shunt (Surgiwear, India).5 6 20
Postoperatively, the patients are routinely monitored for 1–2 days prior to discharge.
Treatment failure is determined when hydrocephalus recurs (according to the initial diagnostic criteria) and requires a repeat operation. Operative infections, wound failures and all deaths (unless known to be unrelated to hydrocephalus or surgery) are also considered treatment failures. The CURE Protocol for management of endoscopic treatment failure is shown in figure 1B. For cases in which ETV (±CPC) fails 3 months or more after surgery, it is presumed that the ETV stoma has closed, so repeat endoscopic exploration is performed to reopen the ETV.21 Children in whom ETV (±CPC) failure occurs after <3 months undergo shunt placement. Shunt failures are treated by VPS revision, with infections requiring VPS removal followed by replacement after antibiotic treatment. A more detailed version of the CURE Protocol can be found at https://cure.org/neuro.
Study sites
Mbale, Uganda
CCHU is a dedicated paediatric neurosurgical hospital established and operated in Eastern Uganda by CURE International, a Christian non-profit organisation. It currently has a 10-bed intensive care unit and a 30-bed ward and, since 2006, is staffed only by Ugandan doctors and nurses. The facility accomplishes approximately 1500 paediatric neurosurgical cases per year with the majority relating to the treatment of hydrocephalus or spina bifida.10 All neurosurgical operations in this study were performed by one of the two Ugandan neurosurgeon coauthors (PS and JM). For this study, demographic, clinical and outcome data were prospectively collected for all patients presenting for hydrocephalus treatment between October 2009 and December 2011. Patients were seen in Mbale or in one of several regional outreach clinics at approximately 1, 3, 6 and 12 months following surgery, with the goal of annual follow-up thereafter.
Lagos, Nigeria
Lagos University Teaching Hospital (LUTH) in Lagos, Nigeria, is a 740-bed public teaching hospital with a general neurosurgery service, 42-bed neurosurgical ward and 6-bed general intensive care unit. The operating room has a video-endoscopy system identical to that at CCHU, as well as a dedicated neurosurgical operative team. All neurosurgical decision making and operations were completed by the Nigerian neurosurgeon coauthor (FB) after having undergone 3 months of training at CCHU and having subsequently employed the protocol into his practice.10 Postoperative care was performed by general nursing staff under the supervision of neurosurgical trainees and faculty. Data were collected prospectively for all children with newly diagnosed hydrocephalus presenting in Lagos between December 2009 and December 2012. A minimum follow-up of 6 months was accomplished. Criteria for initial treatment, determination and management of failure and prospective follow-up were the same at both sites as described under the CURE Protocol.
Statistical analysis
We used Kaplan-Meier method for time-to-treatment failure to construct survival curves. Baseline characteristics and outcomes were compared between the cohorts using χ2 or Fisher’s exact test. Cox proportional hazards regression was performed to compare time-to-failure for VPS and endoscopic cases, separately, by centre, adjusting for age and aetiology. Proportional hazards assumption was confirmed by plotting of residuals as a function of time. All analyses were performed on SPSS V.22.0 (IBM).
Patient and public involvement
Patients or the public were not involved in the design, conduct, reporting or dissemination of our research.
Results
Uganda cohort
During the study period, 730 consecutive children were newly diagnosed with hydrocephalus in Mbale and treated according to the protocol. The median age was 4 months, with a range of 0.1 to 180 months. Over 500 patients (557/730, 76.3%) were ≤6 months at the time of surgery. The most common aetiology was postinfectious hydrocephalus, seen in 469 out of 730 patients (64.2%), which was consistent with our previously reported experience (table 1).22 Mean and median follow-up times were 10.7 and 6.2 months, respectively. A total of 672 (92.1%) patients underwent an attempted endoscopic intervention. Of these, 501 received successful ETV or ETV/CPC, while the remaining 171 attempts were aborted for VPS due to significant scarring in the prepontine cistern. Fifty-eight patients received shunts as the initial, intended procedure. The treatment pathway for patients during the study period is shown in figure 2.
Comparison of demographic and clinical variables between the Ugandan and Nigerian cohorts with χ2 analysis
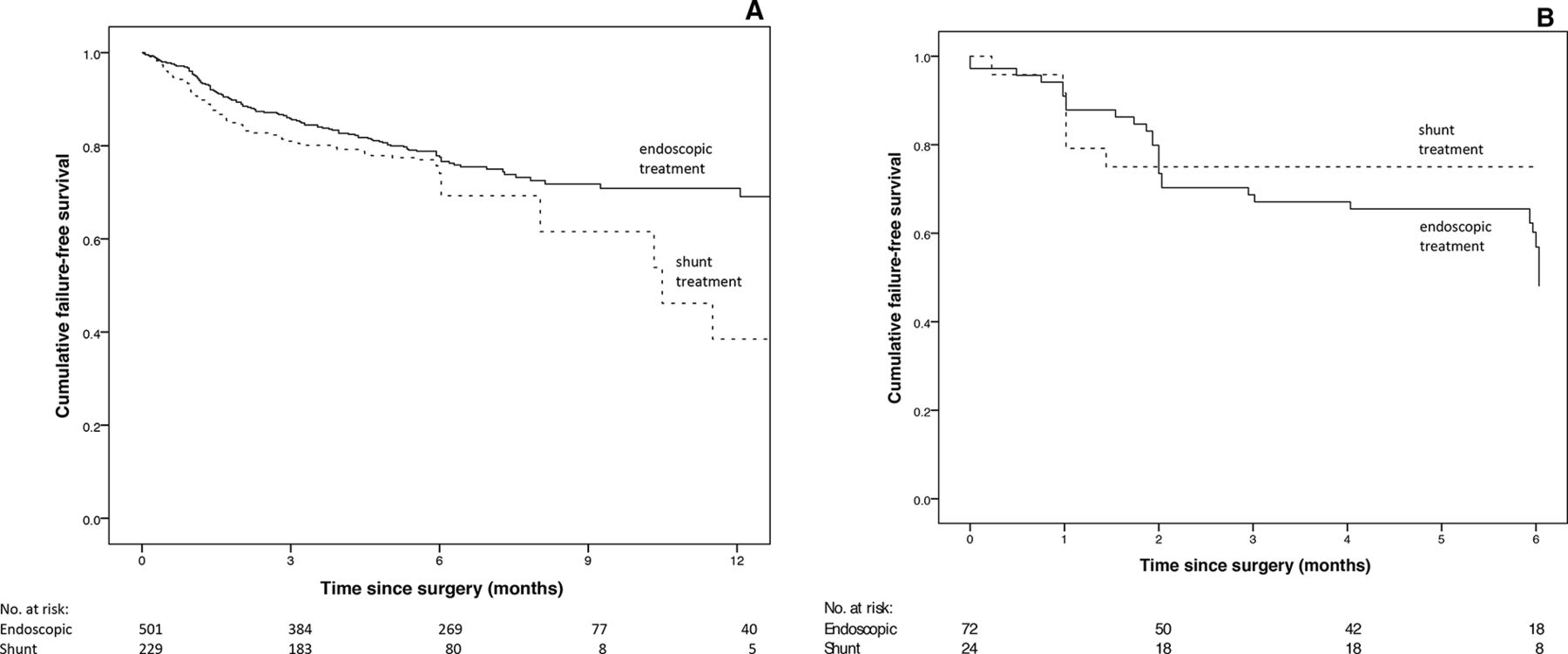
The survival curves for the Uganda cohort, stratified by initial treatment received, are shown in figure 3A. At last follow-up, 74.6% (374/501) of patients that underwent successful ETV or ETV/CPC remained shunt-free. In total, for all children presenting to CCHU with newly diagnosed hydrocephalus and being treated under the CURE Protocol, including those shunted at the first operation, 51.0% (372/730) were shunt-free at last follow-up.

Kaplan-Meier curves demonstrating comparison of time-to-treatment failure with stratification by initial treatment type for (A) the Mbale, Uganda cohort and (B) the Lagos, Nigeria cohort.
The all-cause mortality rate was 10.3% (75/730). The mortality rate directly related to hydrocephalus or unknown causes was 6.0% (44/730). There were 8 deaths related to hydrocephalus or hydrocephalus treatment and 36 deaths from unknown causes, which we included as treatment failures. There were an additional 31 deaths definitively unrelated to hydrocephalus (3 tumour, 16 malaria, 4 malnutrition, 8 other).
Nigeria cohort
There were 96 new consecutive cases of paediatric hydrocephalus presenting to LUTH during the study period. The median age was 4 months, with a range of 0.5–156 months. Sixty-seven (69.7%) patients were aged ≤6 months at the time of surgery. The most common aetiology was the ‘other’ category (49%), which includes all non-infectious causes of hydrocephalus, except myelomeningocele (table 1). Endoscopic treatment was initially attempted in 78 (81.3%) patients and 18 (18.8%) received a VPS per protocol. Six of the attempted endoscopic cases were aborted for VPS due to cisternal scarring or anatomic distortion, as per protocol. The treatment pathway is shown in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment pathway for all 96 children presenting to Lagos, Nigeria with newly diagnosed hydrocephalus. CPC, choroid plexus cauterisation; ETV, endoscopic third ventriculostomy.
This cohort was followed for 6 months and survival curves, stratified by initial treatment received, are shown in figure 3B. At last follow-up, 73.6% (53/72) of the patients treated by ETV (±CPC) remained shunt-free. The total shunt-free rate for all children presenting with hydrocephalus and being treated according to the protocol was 55.2% (53/96). The all-cause mortality rate for the cohort was 8.3% (8/96). The mortality rate directly related to hydrocephalus (2) or unknown causes (4) was 6.3% (6/96). There were two deaths that were definitely unrelated to hydrocephalus or treatment (one sepsis, one gastroenteritis).
Comparison of the two cohorts
Table 1 summarises the comparison between cohorts in regard to age, aetiology, initial treatment and outcomes at 6 months. The majority of patients were <6 months of age in both cohorts (76.3% Uganda, 69.7% Nigeria, p=0.16). There were significantly more patients with postinfectious hydrocephalus in the Uganda cohort (64.2% vs 26.0%, p<0.001) and significantly more with an unknown aetiology and with myelomeningocele in the Nigeria cohort (p<0.001).
Overall, a similar proportion of both cohorts received a shunt at the first operation (31.4% in Uganda vs 25.0% in Nigeria, p=0.2); but, more in the Nigeria cohort were selected for up-front VPS placement (18.8% vs 7.9%, p<0.001) while fewer had an ETV attempt abandoned for shunt placement (6.3% vs 23.4%, p<0.001) compared with the Uganda cohort. This was likely a reflection of the higher proportion of postinfectious hydrocephalus in the Ugandan cohort, with abandonment of ETV for cisternal scarring. The higher rate of initial shunt placement in Nigeria might have been anticipated at a lower-volume site with less experience.
The degree of cistern scarring was recorded intraoperatively for 477 of the 501 Ugandan patients (95.2%) and 71 of the 72 Nigerian patients (98.6%) undergoing endoscopic management.23 In the Ugandan cohort, 19.1% (91/477) of these were categorised as ‘scarred’ but given a chance of endoscopic success due to borderline scarring. Similarly, 14 of the 71 (19.7%) Nigerian patients were noted to have borderline scarred cisterns. The proportions of these patients with borderline scarring were not significantly different between the two cohorts of endoscopically managed patients (p=0.89). Additionally, the failure rate of this subset of patients was not significantly different between the two centres, with 39.6% (36/91) in Uganda and 35.7% (5/14) in Nigeria (p=0.78).
Excluding death and losses to follow-up, direct comparison of 6-month outcomes for the two groups showed a higher initial failure rate for endoscopic treatment in the Nigerian cohort (54.2% vs 27.9%, p<0.001), but the shunt failure rate was similar between the two cohorts (25% in Nigeria vs 26.2% in Uganda, p=0.9). This was confirmed with Cox regression, adjusting for age and aetiology: the Nigerian cohort had a higher failure rate for endoscopic cases (adjusted HR 2.5 (95% CI 1.6 to 4.0), p<0.001), but not for VPS cases (adjusted HR 1.3 (0.5 to 3.0), p=0.6). Interestingly, more patients with ETV failure were treated by redo ETV in Nigeria than in Uganda (81.8% vs 40.2%, p=0.001). Overall, there was no significant difference at 6 months in the proportion of shunt-free patients between treatment sites (55.2% in Nigeria and 53.4% in Uganda, p=0.74).
Discussion
Our study has shown the feasibility and success of the CURE Protocol for primary endoscopic treatment of paediatric hydrocephalus when implemented by local neurosurgeons in low-resource settings. Outcomes were comparable in an experienced, high-volume centre and a less experienced, lower volume centre with a different patient population. The early results in both cohorts demonstrate that just over half of the patients were treated successfully without shunt implantation, which had previously been the only option.
Structured training and support of neurosurgeons in the CURE Protocol has the potential to significantly reduce the burden of chronic shunt-dependent hydrocephalus and its associated morbidity and mortality in low-income and middle-income countries. This could be a better public health strategy in a low-income and middle-income country population, as compared with the historical default of shunt placement as the primary treatment in every child. The majority of endoscopic treatment failures in children occur in a ‘safe zone’ before cranial compliance abates significantly, which lessens the acuity of treatment failure while making the diagnosis visibly obvious (eg, rapid head growth and a full fontanel).14 17 Shunt failure later in life is less easily recognised and requires more urgent intervention in order to avert serious morbidity or mortality.
The CURE Neuro programme was developed to train and equip neurosurgeons from low-resource countries in the endoscopic techniques, as well as in proper application of the CURE Protocol. Neurosurgeons who graduate from the programme return to their home institution, which becomes a ‘Partner Treatment Locations’ (PTL), with which CURE Neuro maintains a supportive relationship. Even with this training, we acknowledge that the use of endoscopic surgery in this context is new and its adoption should be done judiciously. However, the concept of gradually attaining proficiency is clearly demonstrated throughout the general surgical,24 neurosurgical25 26 and other surgical specialty literatures.27 28 As long as newly trained surgeons have received proper instruction and demonstrated competence in both technique and judgement, it is reasonable for them to proceed in appropriate clinical circumstances when they are comfortable. Reductions in shunt burden may not initially be as apparent for newly trained surgeons, but would be expected to improve over time with increasing technical expertise and confidence. Although early results in independent retrospective studies from PTLs in Zambia and in Nigeria were encouraging,29 30 it is not surprising that the same Nigerian centre in this prospective study showed a higher initial failure rate for endoscopic cases compared with the higher-volume centre in Uganda. This was not the case for the technically simpler shunt operations. Possible explanations for this difference in early endoscopic outcomes include surgical technique, differences in decision making regarding patient selection and intraoperative conversion from endoscopy to VP shunt, aetiology of hydrocephalus or a lower threshold to diagnose failure of ETV and undergo ETV revision. The proportion of patients with borderline cisternal scarring still undergoing endoscopic management was similar between the two groups, and so is unlikely to be a contributing aetiology.
Despite this, however, the overall outcome of the cohorts with respect to attaining the ultimate goal of shunt freedom was similar. This is likely attributable in part to the relatively higher rate of redo ETV as well as a higher proportion of favourable aetiology for ETV in Nigeria. Regardless, the similarities in achievable rates of shunt freedom suggest that the Nigeria cohort was receiving appropriate and acceptable care. This indicates that the results of the CURE Protocol are reproducible among centres that differ in geography, patient mix and surgeon experience. Similar investigations are planned at PTLs elsewhere in Africa as well as in Southeast Asia.
Limitations
Although the rate of loss to follow-up in our study (6.6% in Uganda and 7.3% in Nigeria) was similar to previously published series in resource-limited settings,14 31 the loss of these patients could have biassed our results. Long-term follow-up of both cohorts is needed; however, we have previously shown that in the Ugandan experience those who remain shunt-free at 6 months are very likely to remain so without further need for surgery, confirming the durability of endoscopic treatment.32 This is, again, confirmed in our current study with 53.4% of Ugandan infants being successfully treated without shunting at 6 months and 51% at 24 months. This suggests that beyond 6 months from initial treatment there are very few endoscopically treated failures in comparison to the more numerous shunt failures. Long-term follow-up of the Nigerian validation cohort was limited in this study due to the unavailability of local research assistance but is needed to further demonstrate continued effect of endoscopic treatment. However, the early results are very promising with regard to the potential public health implications of radical reduction in shunt-dependence in resource-limited settings.
Both centres were located in sub-Saharan Africa and, therefore, our results might not be generalisable to paediatric populations in other regions. The results from Nigeria, specifically, represent the outcome after a dedicated period of focused training followed by several years of independent experience. Centres just beginning implementation of this protocol after the training period might not achieve similar results initially. Additionally, imaging characteristics were not recorded in the prospective database and it is possible that variations between sites in the interpretation of imaging studies as to whether ETV was anatomically feasible may have occurred. Lastly, while both sites attested to following the CURE Protocol, it is possible there were unaccounted for instances of protocol deviation based on clinical judgement. As such, however, our study represents the pragmatic outcomes of protocol implementation in a real-world setting.
Conclusions
Implementation of an evidenced-based protocol for the management of paediatric hydrocephalus in two centres in sub-Saharan Africa, with disparate patient populations and treated by local neurosurgeons in different countries, were very similar. Our study suggests that half of all children presenting for treatment of hydrocephalus, regardless of age or aetiology, can be treated without shunt placement using this strategy. With adequate training and judicious implementation, this could represent a better public health strategy in low-resource settings than one in which shunt placement is the standard primary treatment.
Acknowledgments
This study was completed while Jacob Lepard was a Wilson Family Clinical Scholar through the Department of Neurological Surgery at the University of Alabama at Birmingham. This work was supported in part by Benjamin Warf's MacArthur Fellowship.
References
Footnotes
Handling editor Seye Abimbola
Twitter @LepardJacob
Contributors The CURE Protocol was originally developed by BW. Additionally, BW was responsible for the conception and design of this study as well as study oversight. The Ugandan cohort was treated by JM and PS and they contributed to data collection. The Nigerian cohort was treated and data were collected by OB. The final data from both centres were assimilated and combined by MD and SC. The statistical analysis and critical revision of the manuscript was done by AK. The final steps of data management, manuscript drafting, data visualisation and publication coordination were accomplished by JL. All authors critically revised and approved the manuscript prior to publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval All data collection and research activity was approved by the CURE Children’s Hospital of Uganda and Lagos University Teaching Hospital ethical review boards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on request. The data collected and analysed for this study are available on request via contact with corresponding author.