Article Text

Abstract
The German government’s response to the COVID-19 pandemic has been predominantly considered wellfounded. Still, the practice of mass quarantine in reception centres and asylum camps has been criticised for its discrimination of refugees and asylum seekers. Building on the concept of othering, this article argues that processes of othering are structurally anchored in German asylum regulations and they have further pervaded public health measures against COVID-19. The practice of mass quarantine made the negative consequences of exclusionary othering for public health particularly noticeable. In the light of recent data indicating this measure to be epidemiologically, legally and ethically insufficient, we apply the concept of othering to public health and discuss (1) exclusionary, (2) inclusionary and (3) diversity-sensitive approaches to public health. We finally conclude that a shift of perspective from exclusion to inclusion, from subordination to empowerment and from silencing to participation is urgently required.
- public health
- control strategies
- health policy
- prevention strategies
- SARS
Data availability statement
There are no data in this work.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
Efforts to control COVID-19 at German reception centres and asylum camps have been criticised for their discrimination of refugees and asylum seekers.
Recent analyses proved that mass quarantine in these settings is epidemiologically, legally and ethically insufficient and counterproductive in that it may increase the cumulative risk of infection.
By applying the concepts of exclusionary and inclusionary othering to the field of public health, we discuss (1) exclusionary, (2) inclusionary and (3) diversity-sensitive approaches to public health.
A shift of perspective from exclusion to inclusion, from subordination to empowerment, from silencing to communication and understanding and from non-participation to active involvement in public health practice is required. This implies a much-needed reflection on who is perceived as ‘mainstream’ or ‘different’, how power is used by dominant groups and how legal and normative commitments to human rights, health protection and well-being can be met sufficiently.
Introduction
Germany was struck by the COVID-19 pandemic in early 2020. Civil organisations and research communities soon and urgently pointed out that ‘viruses don’t discriminate’1 and that ‘COVID-19 will not leave behind refugees and migrants’.2 Efforts to control COVID-19 in Germany have, however, been characterised by the discrimination of persons living in reception centres and asylum camps (hereafter referred to as ‘collective accommodations’).3–5 Based on the concepts of exclusionary and inclusionary othering as introduced by Canales,6 this article discusses the traits and consequences of exclusionary othering that pervade the COVID-19 management in these settings. By using this example, we request a much-needed paradigm shift towards inclusionary and diversity-sensitive approaches to public health.
For this purpose, we first present an overview of the concepts of othering and categorisation, of refugees’ and asylum seekers’ situation in Germany and the previous pandemic management in German collective accommodations. We then continue by highlighting the traits of exclusionary othering in the response to COVID-19. Finally, we propose a paradigm shift towards inclusionary and diversity-sensitive public health that benefits the population as a whole, including those forced to flee their homes.
Othering
Processes of othering essentially concern the question of ‘how we engage with others, those perceived as different from self’.6 Two forms of othering can be distinguished. Exclusionary othering is a process in which dominant groups use their power to define subordinate groups as ‘other’ and ‘not belonging’. This is often done through a reductionist focus on problematic characteristics that are ascribed to subordinate groups, while disregarding their manifold backgrounds.6–9 Those who are marked as ‘outsiders’ from mainstream communities may, therefore, experience discrimination, disempowerment and marginalisation.7 Otherness can be maintained through keeping othered persons distant, unheard and unseen, so that little empathy and understanding of their complex situations can be developed.10
Inclusionary othering also implies the marking of certain groups as ‘other’. However, inter-relational power is used to promote mutual understanding, empowerment, participation and coalition building with the aim of transformation.6
While the following deliberations refer to exclusionary othering as represented in the response to COVID-19 in German collective accommodations, we will reflect on the potentials of inclusionary othering for public health at the end of this article.
Categorisation and the limitations of migration categories
Othering is a driver for categorisation, that is, the attribution of categories to the ‘other’ based on perceived differences.11 Categories help to structure the complex world through grouping, but they also contribute to constructing social contexts.12 In the field of migration, popular categories are ‘national’ versus ‘migrant’, ‘refugee’ and ‘asylum seeker’.12 According to the Refugee Convention 1951, refugees are those who are outside of their country of origin, who cannot return due to a ‘wellfounded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group or political opinion’13 and who have officially obtained refugee status by the receiving country. In order to obtain refugee protection, an often protracted asylum process needs to be completed.14 The term ‘asylum seeker’ officially refers to those whose claims for recognition as a refugee are still in process (ibid.). The status and entitlement granted in the asylum process has major implications for individual rights, living conditions and health.
Migration categories may seem helpful in certain contexts but they imply several problematic assumptions. First, they assume an unrealistic homogeneity of people despite their individual characteristics, experiences, resources, challenges and needs.12 15 Various authors and organisations have, for instance, pointed to a tendency towards portraying refugees and asylum seekers as passive, deserving, helpless, a drain on resources or even fraudulent.9 10 16 Vague references to ‘cultural differences’ are similarly prevalent, often leaving it unclear as to what is actually meant by ‘culture’.17–20 In addition, studies show that perspectives on the deservingness of international protection in receiving societies were skewed towards well-educated, ‘victimised’ and/or Christian refugees.21 This implies a preference towards those who have a ‘utility’ for the hosting society (well educated), share common characteristics (eg, religion or secularism) or have less power (victims).
Second, migration categories may be mistaken for neutral and fixed, while they are actually politically negotiated and, therefore, reflect political agendas and interests.12 15 Changes in the classification of countries of origin as ‘safe’ or ‘unsafe’ are a well-known example, which demonstrates how power is used to classify human beings as deserving international protection (or not).
Third, politically defined migration categories can influence public discourses and practices.12 Through reinforcing the perceptions of categorised persons as ‘outsiders’, they may hinder encounters and mutual understanding.6 7 A recent study among 215 people who crossed the Mediterranean to Greece in 2015 aptly concluded that ‘dominant (migration) categories fail to adequately capture the complex relationship between political, social and economic drivers of migration or their shifting significance for individuals over time and space’.12
Exclusionary othering and categorisation in public health
Migrants are neither generally sicker nor healthier than the non-migrant population.22–24 They might, however, have specific health-related resources and needs based on prior experiences and exposures that need to be taken into consideration.25 26 Despite the need for diversity-sensitive responses to individual health situations, refugees and asylum seekers are often depicted as a ‘burden’ and carriers of disease—as ‘a threat to a robust and healthy society, a threat of disease itself. They must be screened and quarantined to avoid the spread of disease’.9 Such narratives are closely linked to a notion of refugees and asylum seekers as a burden to social systems,27 which has found its way into German legislation: the German social welfare law for asylum seekers fundamentally restricts refugees’ and asylum seekers’ access to healthcare and other social services,28 which the UN Committee on Economic, Social and Cultural Rights has expressed serious concerns about.29 A recent study confirmed that the provision of illness benefits according to the prevailing ‘Act on Benefits for Asylum Seekers’ for persons in reception facilities was relatively low.30 This example clearly illustrates how legal and structural conditions may limit the opportunities of public health to pursue health equity and ‘health for all’.
A considerable body of literature highlights the consequences of exclusionary othering for public health, particularly with reference to limited access, use and provision of health services.7 9 25 31 32 These include inadequate health communication, late presentation of refugees to medical staff due to their fear of stigmatisation, misdiagnoses, underdiagnoses of mental diseases, inappropriate treatment and patients’ fear of retraumatisation.10 33
However, there is no individual or collective benefit from excluding refugees and asylum seekers from health services.9 32 34 Exclusionary othering is rather counterproductive in that it promotes ill health and stress among marginalised persons, which can lead to an even greater need for health services over time.7 10 The latter criticism becomes particularly urgent against the backdrop of the current spread of COVID-19, as will be further elaborated hereunder.
Accommodations and living conditions of asylum seekers and refugees in Germany
By the end of 2018, 411 211 persons were registered as asylum seekers in Germany.35 Persons who have claimed asylum in Germany must stay in allocated reception centres until the official approval of their protection and right of residence or, in the case of denial, until their departure.36 The maximum length of residence in reception centres is 18 months, but it may be prolonged in order to provide for the completion of the asylum process (ibid.). Asylum applicants are then further referred to collective or decentral accommodations run by administrative districts.36 37
In 2018, approximately 200 000 asylum seekers were located in collective accommodations.4 37 The housing conditions vary to a great extent and may include provisory solutions such as container-buildings, halls, trailer parks, former schools or refurbished offices.3 5 37 A publication of the Competence Network Public Health COVID-19 criticised the fact that many residents do not have any choice but to share their rooms, kitchens and bathrooms with other residents, partly under insufficient conditions in terms of hygiene, architecture and infrastructure.4 In addition to overcrowded and strictly regulated housing conditions, asylum seekers receive limited healthcare services and merely basic material and financial support.28 38 39
Consequences of exclusionary othering for the response to COVID-19 in German collective accommodations
The German government responded to the COVID-19 pandemic in line with most of the prevention guidelines that are targeted at the wider community, which were provided by the WHO and the Robert Koch Institute (RKI).40–42 Since the virus is primarily transmitted through droplet infection and contact routes, the recommended measures to control the spread included increased testing, hygiene routines, physical distancing (1·5–2 metres towards persons outside of own households), selected (self-)isolation and wearing cloth face masks (ibid.). Depending on the region and infection rate, public facilities were closed (ibid.). In spring 2020, the government complemented the existing laws on infection protection and social security by two new laws ‘on the protection of the population in epidemic situations with nationwide concern’.43 44 In addition, the National Pandemic Plan was updated.45–47
In May 2020, the German government’s overall management of the pandemic was described as ‘reasoned and sound’.3 At the same time, however, there is concerted critique that the response to COVID-19 did not consider marginalised groups, such as asylum seekers and refugees.1–3 48 49 These groups were hardly covered by the national pandemic plan, except for a general (and questionable) notion that there might be ‘non-compliance due to cultural differences’.45 No specific strategies or recommendations concerning the containment, outbreak management or disease prevention in collective accommodations had been provided at the national level by that time.3
The lack of tailored prevention measures for asylum seekers and refugees, particularly in collective accommodations, is highly problematic. The often overcrowded conditions in camps and camp-like settings facilitate the transmission of COVID-19 and hinder the implementation of prevention strategies, such as the maintenance of physical distance, increased hygiene routines or the isolation of infected persons.4 5 50 For this reason, advocacy groups urgently claimed that collective accommodations should be closed, individuals should be allowed to move into decentral facilities and access to health services must be guaranteed for everyone.51–54 These claims were seldom put into practice. Instead, as soon as the first cases of COVID-19 had been registered in collective accommodations, the district authorities quarantined entire accommodations. In some cases, residents were forced to stay in mass quarantine by means of fences, helicopters, police officers, security personnel and armed forces.4 5
The first scientific data are available on the epidemiological, legal and ethical implications of mass quarantine in collective accommodations. A study conducted by Bozorgmehr and colleagues estimated the risk of infecting further persons in quarantined refugee accommodations as soon as one case of COVID-19 had occurred (cumulative risk of infection).4 The authors referred to the cumulative risk of infection as ‘high’ (17%) and comparable to that on cruise ships.4 As such, overcrowding and missed opportunities to decongest collective accommodations has put inhabitants at higher risk of infection compared with a situation in which their right to individual protection (operationalised by possibilities to self-isolate and practice physical distancing) was fulfilled. It was found that mass quarantine showed no particular benefit in controlling the outbreaks in collective accommodations. In contrast, hundreds of residents who were in need of protection, including mothers, children and the elderly, have been exposed to a higher, although preventable risk of being infected irrespective of their individual health situations and conditions.52 At the same time, there is no evidence that mass quarantine would have any positive effects on the health of the population outside of collective accommodations (ibid.). It is rather possible that larger outbreaks in these settings might also put the wider population at risk.4 A recent guideline of the European Centre for Disease Control on COVID-19 prevention and management in collective accommodations also warns of high psychosocial stress associated with mass quarantine and recommends against this measure to manage outbreaks.55 From a public health perspective, the exclusion of individuals from infection protection, therefore, puts individuals and the broader community at risk.
In addition to the epidemiological shortcomings of mass quarantine in collective accommodations, various legal and ethical conflicts have been highlighted by a number of civil organisations and researchers.4 54 56 The measure contravenes the German Constitution,57 the German Law on non-discrimination,58 the German Infection Protection Act,59 the Charter of the United Nations,60 the UN 2030 Agenda for Sustainable Development,61 the UN International Covenant on Economic, Social and Cultural Rights62 and the WHO constitution.63 Detailed ethical and legal conflicts regard the wholesale definition of groups of persons as ‘potentially infected’ without the investigation of actual contacts with infected persons; deprivation of freedom of movement irrespective of the persons’ non-infection; the potential retraumatisation of persons and the enhancement of increased psychosocial stress.4 The Competence Network Public Health COVID-19 came to the conclusion, therefore, that mass quarantine in collective accommodations ‘is to be avoided without exception’.4
In the beginning of June 2020, unpublished guidelines by the RKI dated May 202064 gained the attention of various organisations and media outlets.65–67 The leaked draft stated that ‘the RKI standards for prevention and for the management of outbreaks apply to asylum seekers and refugees’.64 The institute shared the critique expressed before and summarised: ‘Through mass quarantine, an evitable high exposure as well as resulting risks for all residents are accepted, which contradicts the RKI recommendations on infection protection’.64
In summary, mass quarantine in collective accommodations as a response to the COVID-19 pandemic is legally, ethically and epidemiologically highly questionable, as:
The transmission of COVID-19 is generally promoted through overcrowded and insufficient housing conditions.
The response to the COVID-19 pandemic in collective accommodations may have further increased, rather than decreased, the risk of infection. The development of so-called COVID-19 hot spots has not been prevented.
Mass quarantine might have contributed to further psychosocial strain and possibly ill health among the residents.3
We argue that the processes of othering are structurally anchored in the German asylum regulations and they have remained in public health measures that are being implemented in the respective settings during the COVID-19 pandemic. The practice of mass quarantine in collective accommodations makes the consequences of exclusionary othering for public health particularly noticeable. The underlying logic of mass quarantine is a general perception of residents as potential carriers of infection who the mainstream population needs to be defended against and, if necessary, with the help of fences or even armed forces. Grove and Zwi have aptly described such practices as a perceived ‘protection of the general public’ through ‘an effort to keep forced migrants out’.10 In these cases, it becomes clear how power has been used to exclude individuals by legitimising restrictions to their fundamental human rights.
While approximately half of the refugees and asylum seekers in Germany have been located in collective accommodations, approximately 200 000 were not exposed to the risk of mass quarantine due to their decentralised location in apartments. This may be interpreted as a form of inclusionary othering as discussed hereunder. Such differences in the treatment of refugees and asylum seekers raise the question whether practices in the course of the asylum process may itself represent different forms of othering.
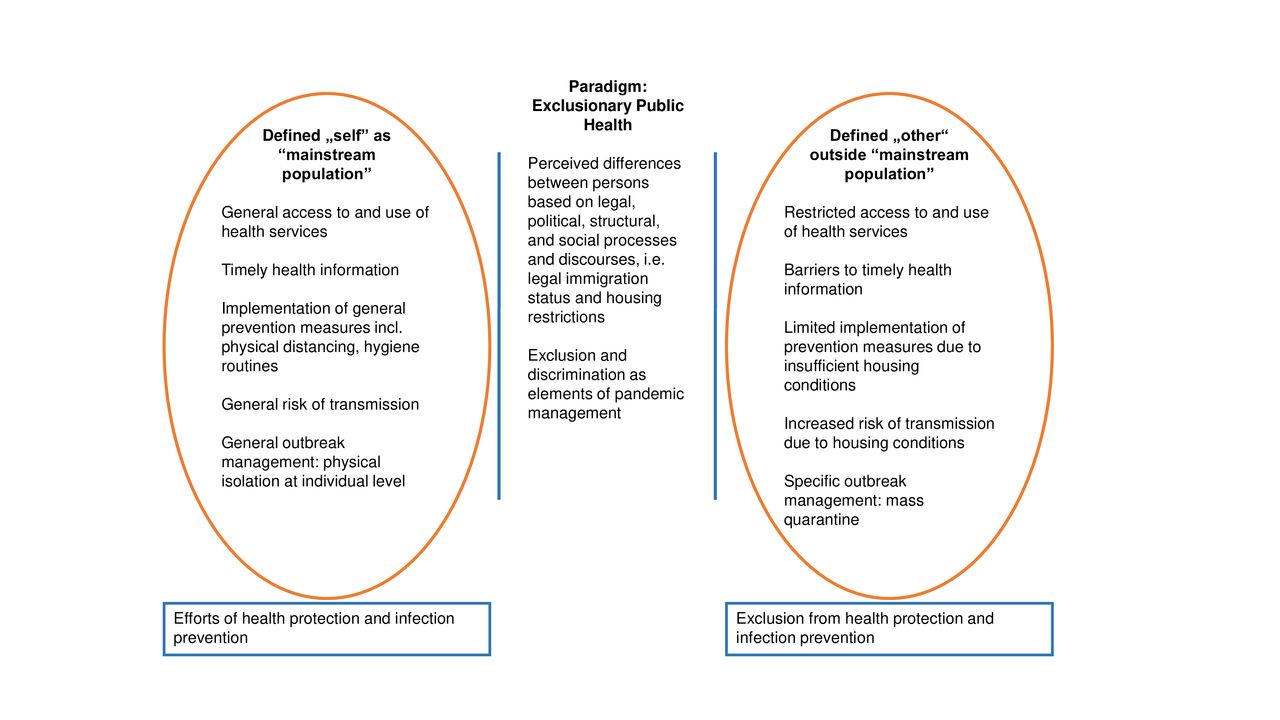
Still, civil organisations and researchers have warned against other aspects of exclusionary othering that might affect both groups of refugees and asylum seekers.1 3 5 49 68 Besides restrictions on health services, these include a lack of language-sensitive information, a lack of participation in the development of strategies against COVID-19, disempowerment through the provision of text-based information that cannot be accessed and read by all individuals and the ethnocentric culturalisation of individual behaviours through public discourses (ibid.). Figure 1 summarises the implications of exclusionary othering in public health using the example of COVID-19 management in collective accommodations.
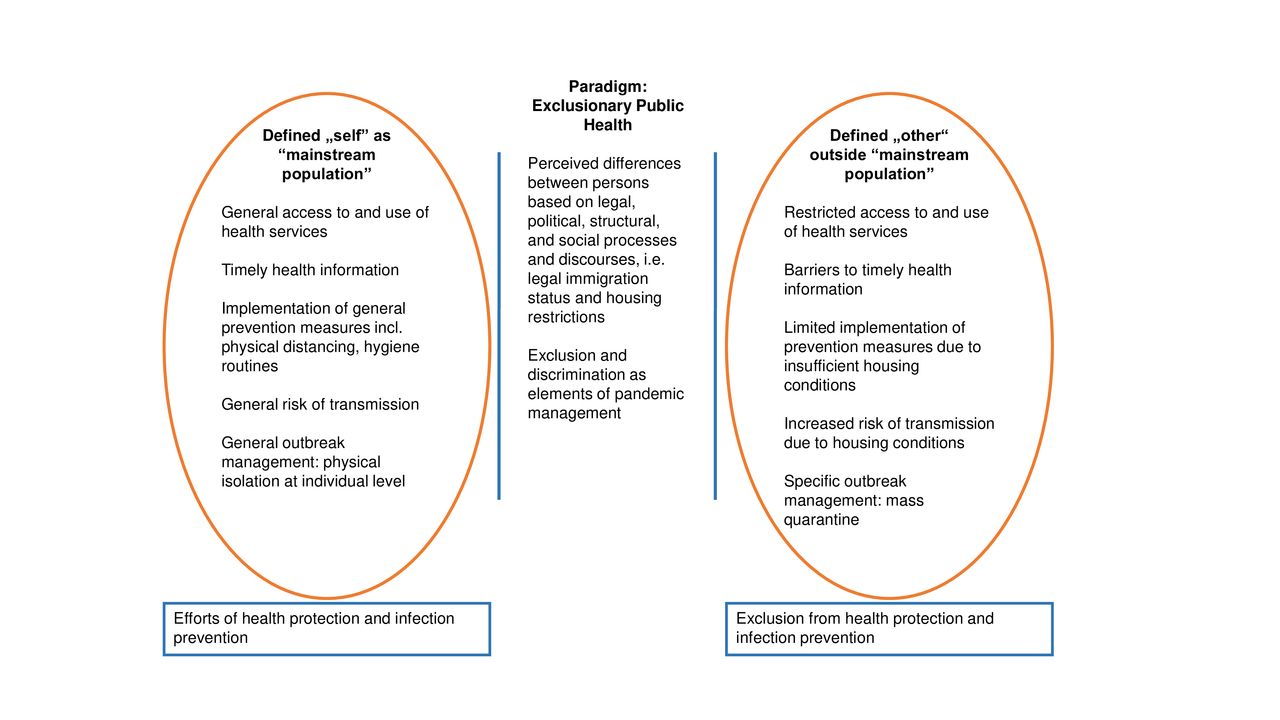
Exclusionary othering in public health using the example of COVID-19 management in German reception centres and asylum camps.
Towards inclusionary public health
The risk of infection concerns everyone. We, therefore, claim that public health needs to be reconsidered from an inclusionary and resource-oriented, rather than an exclusionary and risk-oriented, perspective. Persons forced to flee their countries and residing in Germany are part of the residential population and must be treated as such. Therefore, the measures taken for infection protection must not exclude specific individuals or groups. An inclusionary approach to infection protection benefits the general society and hinders the development of hazardous hot spots. We propose that an appropriate response to COVID-19 includes:
The reduction of risk of infection through improving the living and housing conditions of refugees and asylum seekers, including decentral housing and sufficient hygiene and sanitary facilities.
An epidemiologically, legally and ethically responsible reaction to cases of COVID-19 in collective accommodations in line with the outbreak measures in the general population in order to reduce the risk of infection for other residents.
There is broad consensus that successful public health depends on the promotion of health literacy, empowerment, participation and capacity building among the population and its communities.69 Public health, therefore, invariably comprises negotiations of power in order to enhance people’s control over their own lives (ibid.). It needs to shift its perspective from exclusion to inclusion, from subordination to empowerment, from silencing to communication and mutual understanding, from partition to encounter and from non-participation to active involvement.
It must be pragmatically assumed, however, that power imbalances and markings of difference, such as migration categories, will not be abandoned in the nearest future. Canales’ concept of inclusionary othering may provide a helpful basis for developing an understanding of inclusionary public health. According to Canales, inclusionary othering promotes shared power and coalition building among allies based on their connected experiences.6 This process depends on the will to develop informed empathy towards the ‘other’, and to appreciate the ‘others’ as equal and skilled partners with different qualifications.
Canales’ consideration can be translated into specific recommendations for a resource-oriented response to COVID-19 in collective accommodations. Central demands as published by advocacy organisations include:
The prevention of stigmatisation and marginalisation of refugees and asylum seekers based on reductionist and risk-oriented discourses.
The provision of free and equitable prevention, testing and healthcare for everyone.
The application of all the principles of infection prevention as applied in the wider community (eg, physical distancing, hand and respiratory hygiene).
The provision of sufficient housing conditions (decentralised housing in apartments or similar accommodations).
Early, clear, transparent, evidence-based and diversity-sensitive communication and information about the virus, its spread, the disease and protection measures.
The active participation and engagement of refugees and asylum seekers in the development of response plans, policies and strategies against COVID-19.
Multi-stakeholder collaborations through networks and organisations.1 49–52 55 66 68 70 71
Several examples of involvement and capacity building have been shared throughout the past months, highlighting the potentials of inclusionary public health. For instance, some regional medical boards have invited migrants with medical backgrounds to work as doctors despite their pending licenses to practice in Germany.72 The Berlin Senate supports the programme ‘Newcomers against Corona’, through which migrants have organised and contributed in various ways, including translating in medical situations, sewing masks, shopping for others and cooking.73 The WHO also supports the visibility of refugees’ contributions on its websites and also highlights the benefits of diverse backgrounds in order to mediate and disseminate health-related information to diverse groups of individuals.74
Figure 2 illustrates the implications of inclusionary othering for public health in the light of the COVID-19 pandemic.

Inclusionary othering in public health using the example of COVID-19 management in German reception centres and asylum camps.
Several theoretical links and intersections exist between inclusionary othering (and, therefore, inclusionary public health) and other concepts and theories. In addition to the concepts of empowerment and capacity building, Spivak’s concepts of agency and subalternity are highly relevant in the light of the presented matter.75 76 Subalternity refers to the oppression of ‘othered’ people through dominant groups (ibid.). At the same time, it engages the question of agency among the oppressed, that is, the ability to speak, present own views and needs within dominant discourses.75 While a discussion of subalternity and agency extends the scope of this article, it seems worthwhile to elaborate their scope and practical implications in the presented context.
Diversity-sensitive public health
A complete abandonment of othering and migration categories may be unlikely due to the current German policies and structures, including (continuously tightened) asylum regulations. However, in the fields of social science and reflexive migration research, there is an increasing understanding of the limitations of single differences, such as ethno-national categories or legal status.77–79 Rather, reductionist notions on difference have been opposed by a resource-oriented concept of diversity (ibid.). According to the concept, differences may be inherent, but they may also be acquired in the life course or constructed through social, legal and institutional practice.80 The aspects of diversity are manifold in that they may concern any social, biological, mental, cultural, spiritual, sexual, value-related or other facets of human beings. Appreciating diversity, therefore, means promoting equity and non-discrimination through respecting the complex realities of peoples’ lives. Its measures are targeted at the entire population, while taking diverse capacities, needs, social dimensions, knowledge sources, evidence and innovation into account.81 In the light of the COVID-19 pandemic, this implies that crucial pandemic regulations on health protection must apply to everybody, while implementation strategies need to be adapted to different settings. Discriminating and excluding statements about ‘non-compliance due to cultural differences’ among migrants should be avoided. At the same time, a diversity-sensitive approach requires adaption and adjustment processes among all of the recipients and actors in order to equally benefit from public health. Therefore, trust, empowerment, agency and participation are key to effective and innovative diversity-sensitive public health. Figure 3 outlines a diversity-sensitive public health approach that renounces institutional and legal othering in the context of COVID-19.

{kind=link}
{kind=link}
{kind=link}
Diversity-sensitive public health for everyone using the example of COVID-19 management in Germany.
Conclusion
Due to the structurally anchored processes of exclusionary othering, the health of refugees and asylum seekers in collective accommodations has not been sufficiently protected during the COVID-19 pandemic. The discriminatory practice of mass quarantine may increase, rather than decrease, the cumulative risk of infection. We argue that successful public health should strive for health equity and needs to shift its perspective from exclusion to inclusion, from subordination to empowerment, from silencing to communication and mutual understanding and from non-participation to active involvement. This requires a critical reflection on who is perceived as ‘mainstream’ or ‘different’, how power is used by dominant groups and how legal and normative commitments to human rights can be met sufficiently. This request is not ultimately limited to refugees and asylum seekers in times of COVID-19. Inclusionary and diversity-sensitive approaches to public health do not only serve human rights but also contribute to better health for everyone.
Data availability statement
There are no data in this work.
Ethics statements
Patient consent for publication
References
Footnotes
Handling editor Seye Abimbola
Contributors MT and JS developed the initial idea, searched for the literature and developed the conceptual models. MT wrote the first draft. KB contributed to the literature search and revised the manuscript. All of the authors contributed to the final draft.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.