Article Text

Abstract
Background Cash transfer (CT) programmes are implemented widely to alleviate poverty and provide safety nets to vulnerable households with children. However, evidence on the effects of CTs on child health and nutrition outcomes has been mixed. We systematically reviewed evidence of the impact of CTs on child nutritional status and selected proximate determinants.
Methods We searched articles published between January 1997 and September 2018 using Agris, Econlit, Eldis, IBSS, IDEAS, IFPRI, Google Scholar, PubMed and World Bank databases. We included studies using quantitative impact evaluation methods of CTs with sample sizes over 300, targeted to households with children under 5 years old conducted in countries with gross domestic product per capita below US$10 000 at baseline. We conducted meta-analysis using random-effects models to assess the impact of CT programmes on selected child nutrition outcomes and meta-regression analysis to examine the association of programme characteristics with effect sizes.
Results Out of 2862 articles identified, 74 articles were eligible for inclusion. We find that CTs have significant effects of 0.03±0.03 on height-for-age z-scores (p<0.03) and a decrease of 2.1% in stunting (95% CI −3.5% to −0.7%); consumption of animal-source foods (4.5%, 95% CI 2.9% to 6.0%); dietary diversity (0.73, 95% CI 0.28 to 1.19) and diarrhoea incidence (−2.7%, 95% CI −5.4% to −0.0%; p<0.05). The effects of CTs on weight-for-age z-scores and wasting were not significant (0.02, 95% CI −0.03 to 0.08; p<0.42) and (1.2%, 95% CI: −0.1% to 2.5%; p<0.07), respectively. We found that specific programme characteristics differentially modified the effect on the nutrition outcomes studied.
Conclusion We found that CT programmes targeted to households with young children improved linear growth and contributed to reduced stunting. We found that the likely pathways were through increased dietary diversity, including through the increased consumption of animal-source foods and reduced incidence of diarrhoea. With heightened interest in nutrition-responsive social protection programmes to improve child nutrition, we make recommendations to inform the design and implementation of future programmes.
- child health
- health policy
- systematic review
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Previous systematic reviews and meta-analyses on the impact of social protection programmes generally, and cash transfers (CTs) specifically, on nutrition outcomes find mixed results.
In their 2013 systematic review and meta-analysis, Manley et al find that the average effect of 17 CT programmes, mainly from Latin America, on child height-for-age z-scores was 0.025 SDs (95% CI −0.03 to 0.08, p<0.38), a statistically insignificant finding.
We are unaware of any meta-analysis that also has included proximate determinants of undernutrition, or used meta-regression to examine the associations of effect sizes on child nutrition outcomes.
What are the new findings?
This updated systematic review and meta-analysis builds on previous work and includes more recent evaluations of CT programmes conducted in Africa and Asia.
In addition, it estimates the effect of CTs on multiple nutritional outcomes, including height-for-age, weight-for-age, stunting and wasting, as well as more proximate determinants including the quality of children’s diets (consumption of animal-source foods and dietary diversity) and child morbidity (illness and diarrhoea).
By conducting meta-regression analyses evaluating more characteristics than any prior study, this paper systematically examines how programme characteristics modify the effect of CTs on nutrition outcomes.
Key questions
What do the new findings imply?
Based on a new sample of 74 studies this analysis provides robust estimates of the impact of CTs on nutritional outcomes, finding significant effects on HAZ and stunting, and clarifying the role of determinants along the pathway to impact.
Findings from meta-regression analysis reveal CT programme characteristics that influence programme effectiveness that may be useful for the design of future CT programmes.
This study provides evidence to support the future design, monitoring and evaluation of nutrition-responsive cash transfer programmes, findings ever more important given the impact of the COVID-19 pandemic on nutrition and the push for social protection measures to mitigate its short-term and long-term consequences.
Introduction
Globally, the burden of child malnutrition continues to be high: in 2019, an estimated 144 million children (~21%) under 5 were stunted, 47 million children (~7%) were wasted and 38 million children (~6%) were overweight.1 Despite progress, current trends indicate that we are off-course to reach the nutrition-related Sustainable Development Goal targets for the reduction of child stunting, wasting and overweight.2
Most children suffering from stunting and wasting live in low-income and lower middle-income countries,1 3 with children from the poorest households most afflicted. These forms of undernutrition are inextricably linked with food systems and poverty, limiting access to nutritious, safe, affordable diets and services to support healthy growth.3
Social protection policies and programmes can provide a crucial safety net to children and caregivers from vulnerable households by alleviating poverty and addressing the underlying determinants of malnutrition. An increasingly common modality for delivering social protection are cash transfer (CT) programmes, which provide real income to vulnerable households: estimates of the number of recipients range from at least 350 million to 1.1 billion as of 2020.4–6
Despite strong conceptual links between CTs and improving child nutrition, the evidence to support this approach is limited. To date, only one meta-analysis of 17 CT programmes from 1995 to 2010 has been conducted which found a positive, yet insignificant effect on height-for-age.7
More recent systematic reviews8–11 evaluate the impact of CTs on child nutrition. Collectively, the findings have been inconclusive. Of note, much of the early literature focused on CT programmes in Latin America. Given the expansion of CT programmes globally, especially in sub-Saharan Africa and Asia, and the global push to improve the quality of children’s diets,12 this systematic review and meta-analysis seeks to update the earlier meta-analysis. The findings are perhaps more relevant given the impact of the COVID-19 pandemic on nutrition, and the push for social protection measures to mitigate the short-term and long-term consequences of the pandemic.13
Methods
Search strategy and study selection
In this systematic review and meta-analysis, we used the following criteria for study inclusion: (1) quantitative estimates of the effect of a CT programme (including national and subnational, government and non-government, in both development and humanitarian contexts) on child health or nutrition outcomes for children, with data sufficient to identify not only average programme effects but also marginal effects with SEs. (2) We followed standards commonly applied in systematic reviews and meta-analysis, including only studies meeting high standards for rigour, including only studies based on clear counterfactuals (ie, control groups). (3) We only included studies with sample sizes of at least 300.14 (4) Last, we limited our scope to countries with gross domestic product (GDP) per capita below US$10 000. We exclude programmes providing cash for work, and eliminate programmes that provided recipients only one or two disbursements in total (see the online supplemental appendix 3 for a full list of programmes.) Finally, for our analysis of primary outcomes and illness, we limit our sample to those studies examining children under the age of 60 months. For (secondary) dietary outcomes, we use estimates of impact at the household level.
Supplemental material
We searched Google Scholar, Agris, Econlit, Eldis, IBSS, IDEAS, IFPRI, PubMed and World Bank using two broad terms: “cash transfer” and either “child health” or “child nutrition.” In addition, a “snowballing” method was used to identify references from key sources.8–11 Searches were limited to articles published from 1 Jan 1997 to 30 Sept 2018 in peer-reviewed or grey literature. Searches were carried out in English, though the snowball ended up including three Spanish studies in our final set.
Patient and public involvement
Patients and members of the public were not involved in the research. Experts from a variety of fields including nutrition and social protection were consulted as the direction of the project was decided, and representatives of many organisations continued to guide the work throughout the data collection, research and analysis process.
Data collection and analysis
The title and abstract searches were each carried out by the first author and one of several hired researchers in September 2018. Full article search results were compiled and categorised separately and differences were reconciled through discussion. Two researchers independently extracted data from included studies. Matched values were accepted, and any unmatched values were discussed and then finalised to form the database for this study.
Data extraction tables included the following information: year of study, whether the document was published, transfer amount, programme characteristics including conditionality as well as provision of health services or clinic access, nutritional supplements and BCC (behaviour change communication). Measured household characteristics include baseline income, mean child age, age and education of household head, age and education of child’s mother, household size, share of the sample in urban areas, baseline stunting rates, as well as study location. GDP was collected from the World Development Indicators.15 The primary and secondary outcome measures for this study were guided by a conceptual framework of how CTs lead to improved child nutrition,10 which draws on UNICEF’s conceptual framework describing the immediate, underlying and basic determinants of malnutrition.16
The primary outcome measures were anthropometric markers of nutritional status: height-for-age z-score (HAZ) and weight-for-age z-score (WAZ), as well as stunting and wasting for children under 60 months of age. We included only outcomes from studies directly or indirectly reporting SEs (ie, via t statistics).
The secondary outcome measures were markers of immediate and underlying determinants of malnutrition. Animal-source food was defined as the probability of a household consuming animal-source foods on a given day or household budget share spent on animal-source foods. (Results were combined since both reflect increased consumption, but separate results are also below.) Dietary diversity was based on the number of defined food groups based on a 24-hour recall period: while the majority of our studies operationalise this outcome using the Household Dietary Diversity Score (HDDS) based on 12 food groups,17 some studies used indices with fewer groups.
Childhood illness was constructed as a composite indicator reflecting how child morbidity was measured in different studies: either the percentage of children with fevers (3/10 studies), acute respiratory infections (3/10 studies) or the probability that a child was ill in the past month (4/10 studies). Finally, the incidence of child diarrhoea was defined as three or more watery stools in a 24-hour period.
We estimated the pooled effect sizes via the metan command in Stata V.15.1. Homogeneity in programme effect was rejected at the 5% level for all full sample forest plots except childhood illness, where it was rejected at the 6% level; thus random effects (DerSimonian-Laird methodology) were used in all forest plots to take into account differences between studies.18 The I2 was also generated for each group of studies; every pooled estimate of heterogeneity was above the 40% threshold given in the Cochrane handbook.19 We first analysed primary outcomes of nutritional status, then the secondary outcomes related to diet quality and child morbidity. For each outcome, we generated forest plots using random-effects models. We then used meta-regression analysis to systematically examine associated programme characteristics: given the small sample sizes for certain variables, we restricted such meta-regression analyses to those where N≥10.
Several sensitivity analyses were conducted for all outcome measures. First, to test whether CTs targeted to children under the age of 2 had differential effects, we conducted subgroup analyses separately considering children under 24 months and children aged 24–60 months, noting the programmatic emphasis of targeting interventions to the first 1000 days, between conception and the first 2 years of life, where interventions to prevent undernutrition can have greatest impact. Second, to test the robustness of the results, a sensitivity analysis removing studies from Mexico, many of which are early studies that may introduce bias for the overall effect estimates. Finally, we also conducted a funnel plot to assess whether significant impacts are more likely in published works.
Results
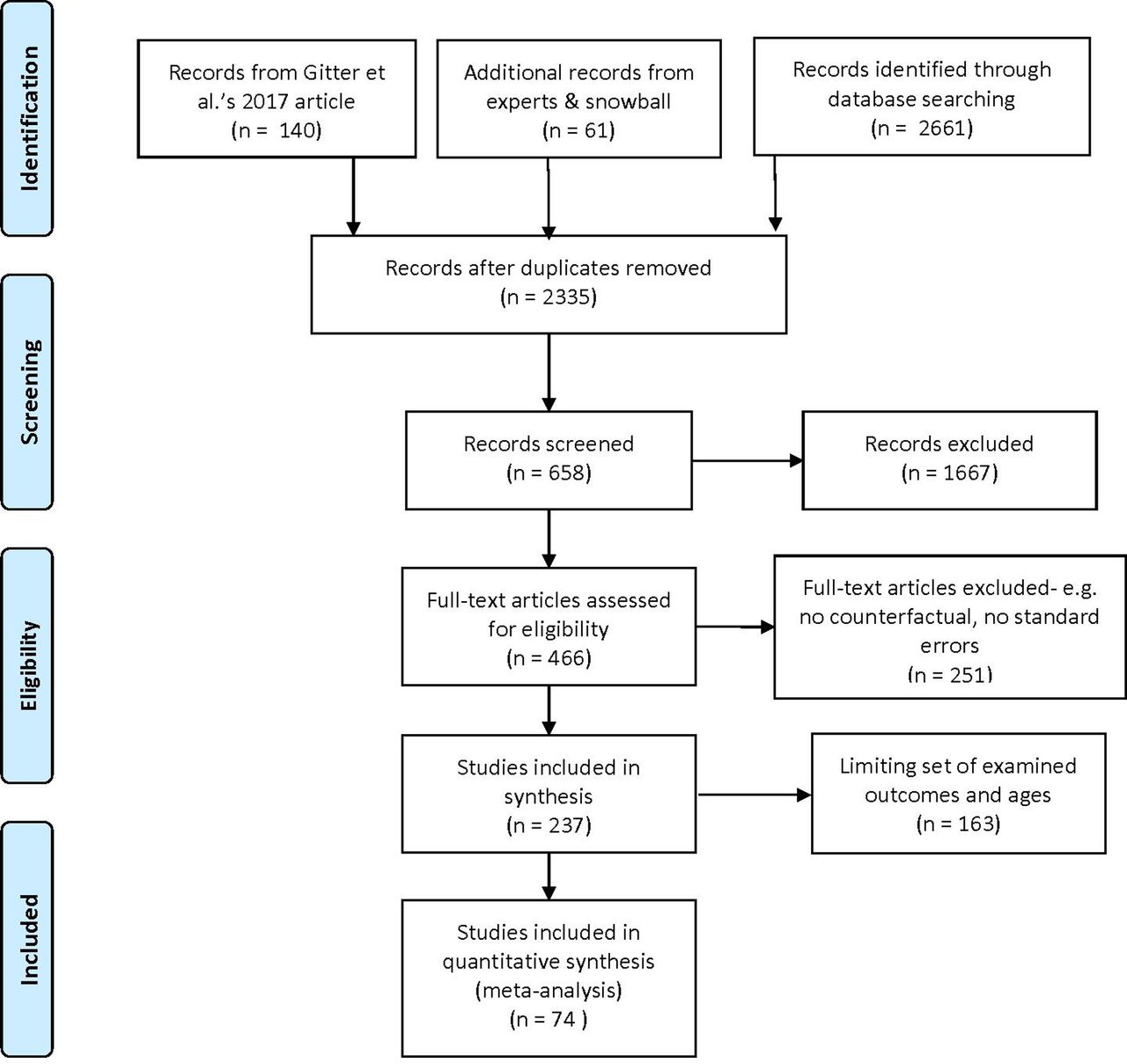
From the search strategy, we identified 2325 studies; of those, 658 titles and abstracts were articles that were considered relevant and screened. The full text of 466 studies were examined for eligibility and after applying inclusion and exclusion criteria, 74 studies from 40 CT programmes were deemed eligible for inclusion in this systematic review and meta-analysis (figure 1). Of the 74 studies included, 60 are double differences including randomised controlled trials (31) and quasi-experimental studies. The remainder include propensity score matching (6), regression discontinuity (4) and other strategies (4). The final list of included studies and their details are presented in online supplemental appendices 1–3.

Search process.
Table 1 shows the summary statistics of the studies included in the meta-analysis. Sample sizes ranged from 322 to 20 000, with a mean of 2881 and median of 2078. The median study took place in 2011, and median study duration was 2 years. Half of the studies (38 of 74) were peer reviewed. The majority of studies were conducted in Latin America and Africa (81%), with the remainder from Asia. The median GDP of countries in the year the study took place was US$1641 (mean $3505).
Characteristics of studies included in the meta-analysis
Programme participants received transfers worth US$121 on average, an increase of 20% of their income. Over half, 53%, of programmes set conditions on recipients: among programmes setting conditions, 95% of CTs required households to send children to school and 90% required health services. (Enforcement of conditions was variable and was not tracked.) Approximately 50% of programmes provided health services and BCC interventions.
At the time of measurement, the average child was 30 months old and the majority (85%) lived in a rural area. Thirty-nine of 74 studies (46%) included baseline stunting rates; the average stunting rate in these studies was 34%. The mean recipient household lived in a country with a GDP of US$3505 but the median of the sample is $1641.
Meta-analysis results
Table 2 shows unweighted means of the dependent variables, and table 3 summarises the results of the meta-analyses. Forest plots for all outcomes are in (online supplemental appendix 7). For HAZ, data were available from 46 studies. On average, the pooled effect size associated with CT programmes on HAZ scores was 0.03 (95% CI 0.00 to 0.05; p<0.03). Twenty-seven studies found effects on stunting, and on average, CT programmes decreased stunting relative to baseline by 2.1% (95% CI 0.7% to 3.5%; p<0.01). For WAZ, data were available from 19 studies. On average, the pooled effect size associated with CT programmes on WAZ scores was 0.02 (95% CI −0.03 to 0.08; p<0.42). From 17 studies, CT programmes were found to decrease wasting by 1.2% (95% CI: −0.1% to 2.5%; p<0.07).
Supplemental material
Unweighted sample statistics of dependent variables
Random-effects meta-analysis: the effect of cash transfer programmes on child nutrition outcomes
Consumption of animal-source foods increased by an average of 4.5% (95% CI 2.9% to 6.0%; p<0.01). Separately considering studies examining the share of household food budgets, we see a pooled effect size increase of 2.2% (95% CI 0.7% to 3.7%; p<0.01) while studies reporting changes in the probability of consumption found an increase of 12.7% (95% CI 7.3% to 18.0%; p<0.01).
Of 13 studies with data on the diversity of diets, children enrolled in CT programmes had increased diet diversity with the number of food groups consumed increasing by 0.73 (95% CI 0.28 to 1.19; p<0.01). Considering only the eight papers using the HDDS 12 group measure, the pooled effect is 0.65 (95% CI 0.03 to 1.28; p<0.05).
CT programmes on average decreased child illness by 2.8% (95% CI −0.3% to 5.9%; p<0.09) among the 10 studies with data. From the nine studies which estimated programme effects on the incidence of diarrhoeal disease, an average decrease of 2.7% (95% CI 0.0% to 5.4%; p<0.05) was found among CT programme participants.
Univariate meta-regression results
Table 4 shows the compiled results of the meta-regressions of covariates (programme characteristics) of CTs on outcomes. Each cell represents the result of a single meta-regression.
Meta-regression analysis: the effect of cash transfer programmes on child nutrition outcomes, by selected covariates
We find that mother’s age modified the effect of CTs on HAZ scores (0.018, p<0.05). While CTs were found to have no association with WAZ in the meta-analysis, the meta-regression showed that the year data were collected, programme conditionality and health service access were factors found to modify the effect of CT on WAZ. We find baseline stunting rates modified the effect of CTs on consumption of animal-source foods, while the transfer size (as a percent of income) modified the effect of CTs on diet diversity.
We break down impacts by region in table 5. No region on its own has a significant overall effect on HAZ or stunting. Only sub-Saharan Africa shows significant impacts on WAZ. One study of three reporting effects on wasting in Latin America finds that the programme increased wasting, a result strong enough to influence the overall point estimate. All regions saw increases in consumption of animal-source foods. Finally, dietary diversity is most examined and most improved in sub-Saharan Africa.
Sensitivity analyses: regional analysis
Next, we consider separately studies investigating programme effects on children in the first 1000 days of life (table 6). The effect sizes of CTs on HAZ (0.05, 95% CI 0.02 to 0.09, p<0.005) are higher and statistically significant for children over 2 years old; neither HAZ nor WAZ is significant for children under 2.
Sensitivity analyses: child age and excluding Mexico
Because Mexico is over-represented in the data, we separately analyse the data excluding studies in Mexico (table 6, third column). The estimated impact on HAZ of CTs has dropped (0.02, 95% CI −0.00 to 0.05, p<0.14). Although programme effects on animal-source food intake are higher in this sample, the results are otherwise similar.
Table 7 shows the effect of CTs by conditionality, though we should note first that the type of intervention is strongly linked with the region. Eighty-one per cent of programmes in Latin America are conditional, while just 4% of programmes in sub-Saharan Africa are. (Exactly half of the 14 studies in Asia examined conditional programmes.) Unconditional programmes seem somewhat more successful in reducing child illness and they are much better at improving child weight as shown in WAZ and the food consumption variables.
Sensitivity analyses: conditionality
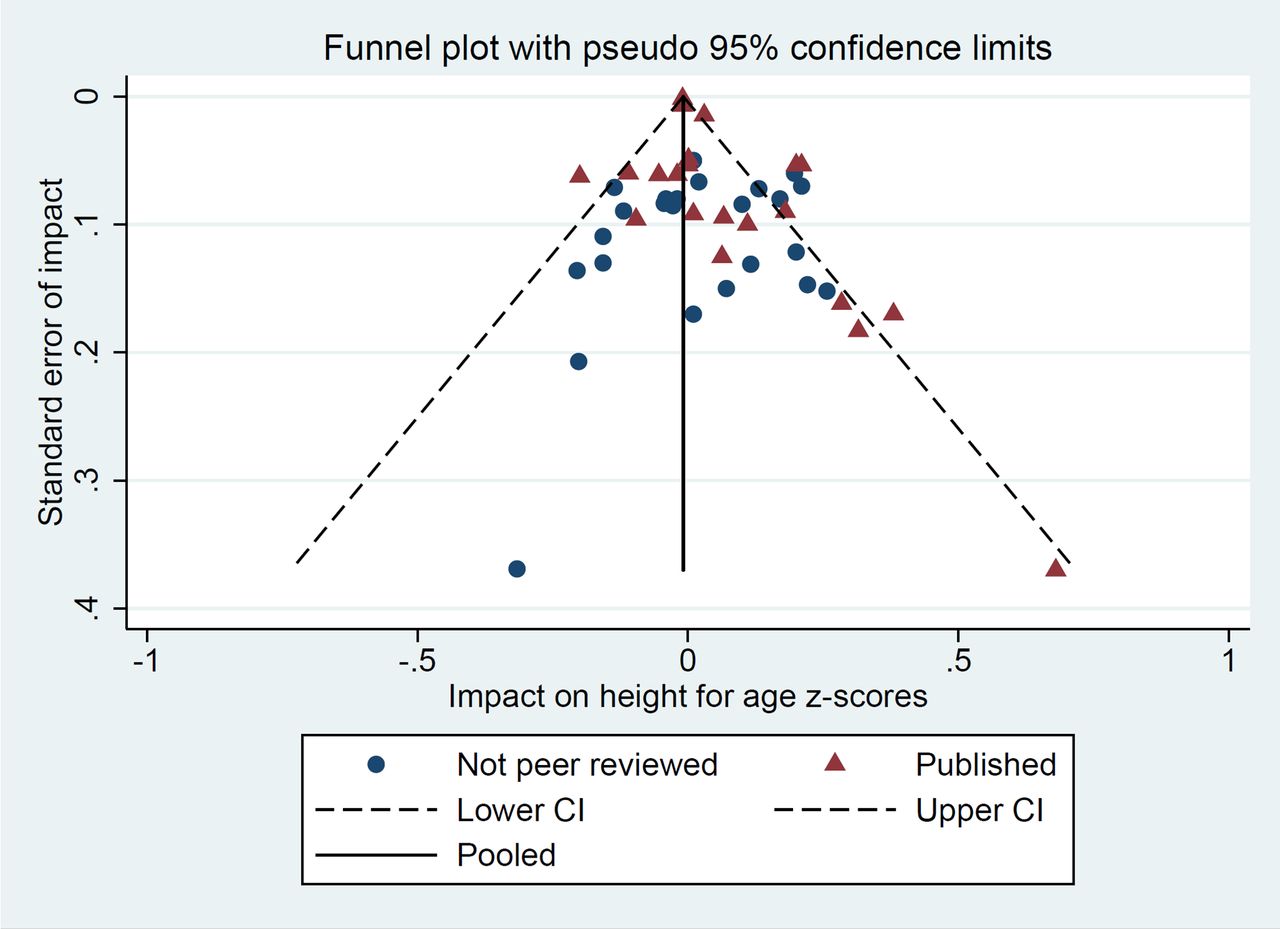
Further, we conducted several subanalyses to investigate: (1) publication bias, (2) methodological choices and (3) programme characteristics. We find that there was no publication bias when comparing peer-reviewed versus non-peer-reviewed programmes, with the possible exception of programmes reporting an impact on stunting (online supplemental appendix 5). In addition, we find that methodological choices do not play a significant role in our findings (online supplemental appendix 5) and that the type of conditionality (online supplemental appendix 6) has limited differential effects.
Finally, we produce a meta-funnel plot to investigate publication bias as regards height for age (figure 2). Unlike the earlier review7 we find no evidence of bias.
{kind=link}
{kind=link}
Publication bias in papers reporting impacts on height-for-age z-score.
Discussion
In this systematic review and meta-analysis of evaluated CT programmes carried out in several low-income and middle-income countries, we found that CT programmes targeted to households with young children under 5 years had a small, yet significant effect on improving linear growth and reducing stunting. Our findings confirm likely pathways are through consumption of animal-source foods, increased diet diversity and reduced incidence of diarrhoea.
A previous meta-analysis of the effects of CTs on child nutrition carried out in 2010, based on 17 programmes, mainly from Latin America, found a non-significant pooled effect on HAZ of 0.025 (95% CI −0.03 to 0.08).7 The present study, which includes 11 more studies from Africa and 5 more studies from Asia, shows a significant effect on HAZ of 0.026 from 46 studies. Our findings are therefore consistent with previous analyses, providing a more robust case to support nutrition-responsive social protection programmes globally.
We further add to the literature in several ways. First, to our knowledge, this is the first meta-analysis to examine the pathways to improved child nutrition through its determinants. Although only a few studies measured indicators relating to children’s diets and morbidity, we find evidence that CTs likely act through these determinants to improve child nutrition. Indeed, with increased household purchasing power provided by CT programmes, caregivers are able to boost the quality of young children’s diets: by increasing access to nutrient-dense animal-source foods, such as dairy, eggs, fish and meat; and by increasing the diversity of food groups. In addition, we find a similar pattern of these programmes reducing child morbidity, likely through increased access to health and nutrition services. Despite the small number of studies, the finding of a significant effect of CT programmes on reduced diarrhoea incidence supports this being an important pathway for breaking the well-documented cycle of poverty, disease and malnutrition.20
Second, we explore the characteristics of CTs associated with effect size for the nutrition outcomes. Notwithstanding the fact that we had few data points and that these results are observational, this analysis is useful to inform the design of programmes. Programme factors (transfer amount, conditionality and health services access) and participant factors (baseline stunting and maternal age) seem to have differential effects on different child nutrition outcomes, demanding consideration when designing such programmes.
Third, we explore whether targeting CTs to households with children under 24 months have differential impact on primary and secondary outcomes, finding that the effect of CTs on stunting reduction is much greater among children aged 24–60 months. A possible reason for this is that the first 2 years coincides with the period of growth faltering that has been observed across several settings,21 which coincides with the period after of introduction of complementary foods at 6 months. CTs may be mitigating such growth faltering but this is not clear. We note however that in these studies CTs increased household animal-source food consumption and dietary diversity as well as (weakly) decreasing illness among children under 2.
Our study has a number of limitations. First, by analysing pooled data rather than individual-level data from these studies, we lose much of the granularity especially as it relates to understanding how the design and quality of implementation of CT programmes may differentially affect child nutritional status in different households. Second, few studies included data on secondary outcomes (children’s diets and morbidity), limiting our ability to examine the likely pathways through which CTs can improve children’s nutritional status. Third, many studies included household-level measurement of variables such as dietary diversity which may reflect household purchasing power rather that the nutritional quality of children’s diet; this is likely to increase measurement error. Fourth, the relatively short duration of many studies may be insufficient to see changes in linear growth. Fifth, regarding conditionality in particular, we do not track enforcement of conditions, so their effectiveness is unclear. Sixth, a variety of issues remain unaddressed here, including intrahousehold dynamics and gender issues. Finally, there is substantial heterogeneity of study contexts and designs in our data. Although we correct for some differences statistically, some likely remains.
There are several implications of this work for both research and programming. We see the value of conducting an in-depth qualitative review of existing CT programmes that seek to improve child nutrition. There are several design choices or typologies of nutrition-responsive CT programmes and greater understanding of these typologies and their programme impact, across humanitarian-development contexts, will be useful to inform current and future programmes. This is relevant given the growth of such programmes, especially in sub-Saharan Africa and Asia. Future studies of similar CT programmes should more systematically collect data on nutrition outcomes and those along the pathway to impact, especially at the individual level (rather than household level) to better quantify and understand the differential impacts for participants. Such studies could also consider collecting more data on caregiver characteristics (including maternal nutritional status), as well as considering long-run effects.22
There is considerable interest and need to strengthen social protection systems to protect, promote and support food security, diets, services and practices that prevent malnutrition among vulnerable children.23 Thus, it is critical to continue building a robust evidence base to improve our understanding of how best to design and leverage CT programmes to most effectively ensure that children’s rights to nutrition are protected in different contexts. Latest available data from UNICEF’s NutriDash database show that 56 countries were implementing CT programmes designed to improve nutrition in 2018, an increase from 49 countries in 2017.24 The number of CT programmes is expected to rise and the need is more acute than ever: with the estimated 90–117 million children falling into poverty due to COVID-19, the pandemic and its socioeconomic consequences represent a crisis to the survival and well-being of children, particularly vulnerable children living in poverty,3 11 25 26 and those already suffering from hunger and malnutrition. Rapidly expanding nutrition-responsive social protection programmes and strengthening social protection systems for nutrition will be critical to mitigating the pandemic’s impact on food security and nutrition.27
Acknowledgments
This study was commissioned by UNICEF as part of a series of analytical work to contribute to strengthening the evidence base to inform programming on nutrition-responsive social protection systems to improve child nutrition, building on existing efforts.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @KHURSHIDATIF
Contributors JM conducted the review and developed the protocol with input from AK, LH, DS, JO, SMurthy and NEW-R. JM did the systematic search, selected studies for inclusion and extracted the data. YB, SMalm and JM substantially revised the paper and sharpened the analysis. JM did the analysis, generated figures and wrote the manuscript with input from all other authors. All authors critically engaged with the manuscript and approved the final submitted version.
Funding Funding for JM was provided by UNICEF grant 43254067.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request. Data available once published and/ or as needed by reviewers in the reviewing process.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.