Article Text

Abstract
The International Health Regulations 2005 (IHR) is a legally binding framework which requires 196 WHO Member States to take actions to prevent, protect against, control and provide public health response to the international spread of disease. Improving IHR compliance provides grounds for better health system strengthening, which is key to moving countries closer towards Universal Health Coverage. Multisectoral, collaborative working within and across sectors is fundamental to improving IHR (2005) compliance, and for that, governance is the best lever of the health system. This paper highlights the importance of the relationship between governance and IHR in the context of Sustainable Development Goals (SDGs) which follow the fundamental principle of interdependence; SDGs interlink with one another. We consider governance (SDG 16) and how it influences the IHR capacity of SDG 3 (health and well-being for all at all ages). This paper considers the successes of the Myanmar Ministry of Health and Sports thus far in improving IHR compliance and highlights that an even greater focus on health system governance would lead to more sustainable outcomes. Nurturing an institutional culture with enforced rules, which are conducive for improved accountability through inclusive participation would further improve Myanmar IHR strengthening efforts. Without those principles of good governance, the developed IHR capacities cannot be sustained or owned by Myanmar people. This has now become even more urgent given the current COVID-19 pandemic.
- health policy
- health systems
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Prevention and control of public health risks are a collective responsibility of individual citizens, government and civil society organisations.
Myanmar has worked hard but its International Health Regulations (IHR) strengthening efforts can further be improved by promoting an environment which is conducive for better health system governance.
Accountability of key stakeholders in Myanmar should promote health system strengthening, not their own agenda.
The Myanmar health system should promote systematic inclusive cross-sector participation to ensure better compliance from key stakeholders.
The IHR-related rules and legislations need to be enforced and transformed into actions.
The COVID-19 pandemic underscores that governance and IHR are indivisible in that key governance principles are paramount to achieving multisectoral, collaborative working in a country.
Introduction and background
The International Health Regulations 2005, (IHR) as a multilateral legal instrument,1 underpins Global Health Security activity. The IHR provides a framework to WHO Member States as to how they should build and maintain their national capacities to prevent, protect against, control and provide public health response to the international spread of disease.1 By promoting IHR compliance, health systems become more resilient and in turn, contribute to achieving universal health coverage (UHC). There is increasing evidence that a resilient health system is the key to moving towards UHC.2 Without UHC, there is an increasing likelihood of cross borders health-seeking behaviour, which can threaten global health security.3 Furthermore, UHC could help to build trust between the government and populations, leading to better community compliance with state-led interventions during public health emergencies.4 5 Myanmar (formerly known as Burma) is one of the 196 WHO’s Member States and has committed to achieving IHR compliance. Like other low-and-middle-income countries, Myanmar has many challenges in strengthening IHR compliance due to limited resources and infrastructure in public health among competing demands.
To our knowledge, no studies have been published on IHR implementation or IHR strengthening from the perspectives of health systems governance in Myanmar. This paper provides an overview of the status of IHR compliance in Myanmar, highlighting the good work undertaken by the Myanmar Ministry of Health and Sports (MOHS) towards IHR compliance in recent years. We also show the importance of governance and its role in promoting multisectoral, collaborative working to achieve IHR compliance.
The International Health Regulations
In 1951, WHO member states adopted the International Sanitary Regulations (ISR), providing a single set of rules to help member states control the spread of ‘quarantinable diseases’.6 The ISR were then renamed as the IHR in 1969 and later modified in 1973, 1981 and 2005.6 The 2003 SARS outbreak reinforced the need for a more effective legal international framework to cover ‘all events potentially constituting a public health emergency of international concern (PHEIC)’, not only for infectious diseases. The SARS outbreak accelerated the revision of,7 IHR 2005 which came into effect in June 2007.7 IHR 2005 were transformative in these aspects, bringing in a shift in emphasis from (1) disease-specific approach that focused on three diseases to including all public health threats (2) passive to proactive use of real-time surveillance and (3) control at borders to detection and containment at the source.7
The IHR recognise the interconnected nature of the world and how prone it is to rapid spread of diseases.8 The IHR further recognises an increasing number of potential public health challenges beyond infectious disease, including environmental changes, chemical hazards and radio nuclear threats.1 The IHR has several salient features. First, the IHR prescribe a set of ‘core capacities’, those required for the Member States to effectively detect, assess, notify and report events and respond to public health risks and emergencies of national and international concern. Core capacities exist for diverse technical areas including legislation, surveillance, laboratory capacity and chemical and radio nuclear safety. Second, the IHR promote proactive risk management through the early detection of potential international threats (with notification and other reporting requirements under IHR).7 The regulations also mandate national IHR focal points in each Member States’ and WHO country offices to facilitate the communication and reporting processes.7 This is particularly important in the mobile world as information (both accurate and not) can be spread within seconds.8 Finally, the IHR attempt to prevent unjustified closing of borders or unnecessary interference with international trade and travel to avoid economic loss.9
The IHR have been tested in many real-world situations since 2005.10 Six events have involved the declaration of a PHEIC. The first was in 2009 when the WHO declared H1N1 influenza pandemic a PHEIC following consultation with Mexico and the USA.11 In 2014, there were two PHEICs-polio and the West Africa Ebola epidemic. The fourth PHEIC was declared in 2016 in response to the Zika virus epidemic. The last PHEIC on COVID-19 was declared on 31 January 2020 and is the largest pandemic in the 21st century. Due to the COVID-19 pandemic, there is a renewed focus on revisiting the IHR framework. COVID-19 once again underscores the importance of investing in national capacity building and preparedness, and the IHR is one instrument enabling this. At present, it has guided the global response to COVID-19. The IHR remains a valuable global framework for national and international health systems through coordination, collaboration and capacity building for global health security.11Figure 1 illustrates a brief overview of IHR history.
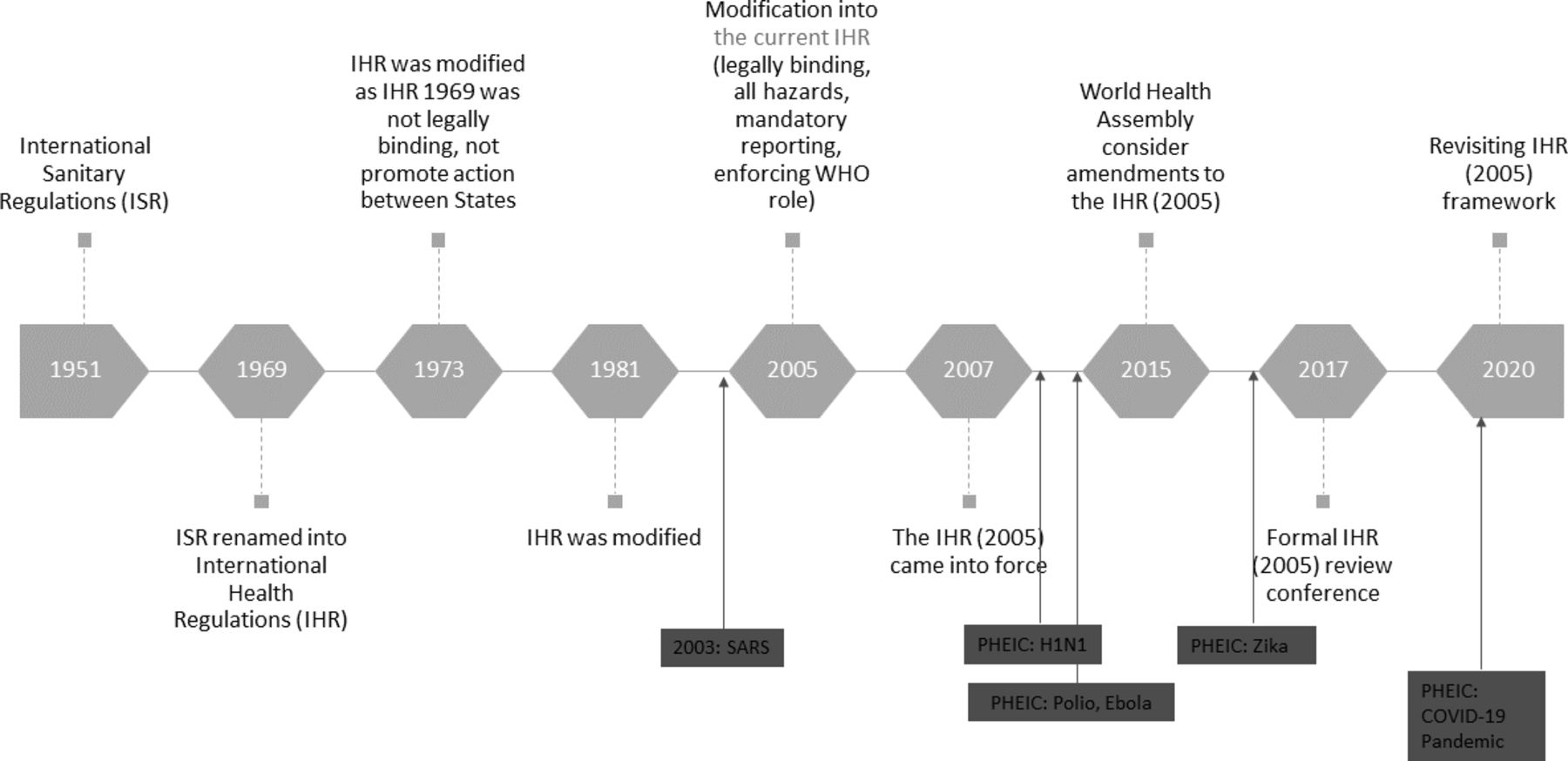
Historical overview of the IHR. IHR, International Health Regulations.
Status of IHR (2005) implementation in Myanmar
The post West Africa Ebola IHR Review Committee in 2017 recommended establishing a monitoring and evaluation framework comprised one mandatory (States Parties Annual Reporting) and three voluntary components (Joint External Evaluation/ JEE), after-action review and simulation exercises).11 Among them, the JEE helps countries identify the most critical gaps within their human and animal health systems to prioritise opportunities for enhanced preparedness and response.12 JEEs are needed to evaluate country capacity to prevent, detect and rapidly respond to public health threats independently of whether they are naturally occurring, deliberate or accidental.12 The first JEE serves as a baseline to assess the progress of a country’s capacities and capabilities and help ensure that improvements in capacity are sustainable.12 Myanmar was the third country in South-East Asia to undergo a JEE.
The Myanmar Union Minister MOHS, HE Dr Myint Htwe, initiated the process in May 2017. The JEE mission led by Myanmar MOHS consisted of a multidisciplinary team of national and international experts. The 2017-JEE demonstrated reasonable capacity in the Myanmar health sector for IHR compliance. However, numerous key technical areas were identified as requiring improvement, some with immediate actions (table 1).12 13 Given these findings, Myanmar MOHS has taken actions and prioritised the building of IHR core capacities in these areas. In 2018, the MOHS developed a costed 5-year National Action Plan for Health Security (NAPHS), the first in South East Asia, to realise the recommendations from the JEE findings.13 Myanmar may undertake another JEE, in 2022, as part of the recommended 5-year cycle for this.
Summary of Myanmar JEE scoring12
As in other low-and middle-income countries, Myanmar has many IHR compliance challenges, not least because IHR compliance is one of many priorities competing for constrained health system resources. Nevertheless, Myanmar must be commended for having strong political leadership to strengthen IHR compliance since its JEE.
The role of governance in promoting IHR implementation
WHO defines governance alongside leadership as ‘ensuring strategic policy frameworks exist and are combined with effective oversight, coalition building, attention to system design and accountability’.14 Governance is also defined as ‘developing and setting effective rules in the institutional arenas for policies, programmes and activities relevant to fulfil public health functions to achieve the objectives of the health sector’.15 Health systems governance is the ‘mortar’ which holds five other building blocks of health system: human resources, financing, health systems information, medicines, vaccines and technologies and effective health service deliveries.1 16 There is increasing evidence that governance is a critical building block for improving health system performance to achieve UHC.17 For instance, Ciccone et al18 showed how improved governance mechanisms have been associated with positive health outcomes. Lazarova highlighted that improved quality of regulatory capacity, rule of law and corruption control had reduced infant mortality rates.19 Other studies in sub-Saharan Africa have highlighted that, with good health systems governance, spending in health was twice as effective in reducing under-5 mortality and increased life expectancy.20 21 The importance of good governance is also reflected in the United Nations Sustainable Development Goals as Goal 16 comprises of the rule of law, accountability, participation and transparency.22
Evidence suggests that governance is the best lever to achieve IHR compliance as it is a cross-cutting framework.23 24 There are an increasing number of studies highlighting a positive association between good health system governance and health system outcomes/performance.17 25 For instance, good governance of public health agencies with a clear line of accountability, strong leadership and command system are critical for the effective performance of public health emergency operating centres (HEOC).26 Therefore, leveraging governance efforts can help achieve collaborative working within and across sectors. Collaboration and multisectoral working are vital to achieving IHR compliance as the prevention and control of public health risks are no longer the responsibility of a single ministry or department.7 Without coordination and engagement with other sectors such as animal health, transport, communication, education, foreign affairs, border and trade, IHR strengthening cannot be achieved. The Myanmar JEE explicitly highlighted that ‘the effective implementation of the IHR requires multisectoral/ multidisciplinary approaches through national partnerships for efficient and alert response systems. Coordination of nationwide resources, including the designation of a national IHR focal point, which is a national centre for IHR communications, is a key requisite for IHR implementation’.12
The Myanmar NAPHS includes intersectoral and multidisciplinary collaboration as a guiding principle and calls for a ‘One Health’ approach for collaborative working within and across different ministries. This includes partnership working with civil society organisations (CSO) and bilateral and multilateral organisations due to the ‘changing nature in increasing emergence and re-emergence of infectious, non-infectious and other PHEIC across the world’.13 Furthermore, fostering a culture of internal coherence and joint working between different departments of the MOHS as well as outside the ministry is recognised as vital. In this context, good governance is critical as without it collaboration and multisectoral working cannot be effectively achieved. However, governance is an abstract and diffuse concept.27 28 To promote governance in one single sector itself is challenging. Hence, promoting governance to strengthen IHR compliance where multisector collaboration is key to its success, is even more challenging. Among different principles of governance, three governance principles—accountability; inclusive participation; and enforcement of rules—are essential to strengthen IHR compliance in Myanmar (figure 2).

{kind=link}
{kind=link}
Key governance principles essential in strengthening IHR compliance. IHR, International Health Regulations.
First, ‘accountability’ of key stakeholders for national capacity building is an important initial step to help strengthen IHR core capacities in Myanmar. These include relevant policymakers and implementers from the government, including central, state/region departments as well as bilateral and multilateral organisations such as WHO and non-state actors (CSOs, ethnic health organisations/EHOs). Accountability of policy-makers and implementers will promote ownership and sustainability of the IHR strengthening efforts through regular evaluation and assessment of core public health capacities to improve the identified gaps. Accountability includes both internal (within health system hierarchy) and external (to populations they serve). Indeed, promoting stakeholders’ accountability will enforce and change values in strengthening IHR compliance. For instance, Myanmar has drafted a National Public Health Emergency Preparedness and Response Plan (multihazards) and an HEOC plan. In 2019, Myanmar tested this HEOC plan through a functional simulation exercise at three HEOC facilities in Nay Pyi Taw with the assistance of WHO and Public Health England (PHE). The exercise was conducted as part of the capacity building of staff at both national and subnational level, focusing on familiarising the roles and responsibilities of a HEOC and an incident management structure. The exercise focused on testing the communication aspect of the HEOC plan to promote accountability as clear lines of communication, and an understanding of roles and responsibilities are essential building blocks to improve accountability. Furthermore, a surveillance system review was conducted in October 2019, composed of a stakeholders’ workshop with representatives from 17 state and regions. The workshop aimed to improve the collection and use of surveillance information and to develop simple integrated communicable disease control and laboratory testing guidelines for basic health staff. These examples illustrate different efforts of the MOHS to improve accountability within its public health system, which can further be promoted through development of relevant accountability mechanisms and associated action plans.
While promoting accountability, care should be taken to avoid ‘accountability overload’, resulting from multiple demands for accountability with competing interests and conflicting expectations.29 Furthermore, ensuring the accountability of non-state actors is critical. This includes CSOs, EHOs, bilateral and multilateral organisations, charities and corporations whose accountability is often unclear. Clarity is needed on who these organisations are accountable to, the Myanmar people, their universal rights and health system, the funders or their own agenda.30 Ultimately, accountability of those organisations should promote health system strengthening, not the interests of the organisations.30 Accountability of key stakeholders is highly influenced by health systems software factors such as stakeholders’ attitudes and perceptions, clear roles and responsibilities, and values and the culture of the health system in addition to health system hardware (ie, resources).31 Therefore, stakeholders could be convinced of the benefits of IHR strengthening by focusing on safety and well-being of health staff and their workplaces, which can be witnessed during the COVID-19 pandemic. Delegation of authority to mid-level managers and a widening of their decision-making space can also promote accountability, efficiency and build their creative thinking and initiatives.
Second, Myanmar IHR strengthening efforts will benefit from ‘inclusive participation’ of different stakeholders (public, private, non-state actors). The NAPHS highlights ‘participation and engaging community’ as one of the guiding principles.13 In addition to communities, engaging policy implementers from different states and regions will be instrumental as they are the key frontline workers realising the NAPHS into action. Furthermore, enhancing inclusive participation of key implementers and non-state actors at different health system levels will ultimately promote their accountability. With lessons learnt from the Ebola epidemics in Africa, the importance of communities and civil societies for strengthening IHR compliance cannot be stressed enough.3 4 As an example, PHEs ongoing work in Myanmar to strengthen IHR compliance with respect to chemical poisoning is engaging all levels of the health system.32 In the ongoing COVID-19 pandemic, the Myanmar MOHS also proposed a bill to update the 1995 Prevention and Control of Communicable Diseases law. The bill was published in state-owned newspapers in February 2020 to enable the public to comment and send suggestions to the Union Parliament office further demonstrating inclusive participation in policy-making.
The Myanmar health system could further benefit from systematic inclusive participation. All levels of the health system, including those from states and regions’ basic health staff should be considered, and collaborative working and data sharing between relevant departments should be facilitated. This was highlighted in the JEE as engaging clinicians (both public and private) in public health surveillance will improve the national surveillance system. Engaging other public sectors to enhance the culture of multisector working is an important step to be considered. Furthermore, identifying ways to integrate the private sector into the national health system will be important as 70%–80% of ambulatory care in Myanmar is provided by the private sector.33
Additionally, Myanmar’s health system should continue to leverage the country’s socially ingrained volunteer spirit through existing CSO. The most significant example of such leverage was during cyclone Nargis in 2008 as emergency relief efforts were mainly carried out and supported by individual well-wishers and CSOs across the country. EHOs should not be neglected as the second Annual Operational Plan of the National Health Plan (2017–2021) delineates roles and responsibilities of EHOs for the first time in an official document.34 Hence, Myanmar cannot neglect the ‘mesolevel bottom-up’ approach because it can help to ensure stronger response and better compliance from key stakeholders and communities during the time of crisis.24 Myanmar needs to think globally but act locally by listening to key implementers and communities and engaging them in the work of the IHR strengthening work. This can ensure effective embedding of IHR core capacities into the national health system.
Third, strengthening the ‘rule of law’ or ‘enforcement of formal rules’ and legislations relevant to the IHR is another important governance principle which can help improve IHR compliance. The Myanmar regulatory system should provide a legal basis for prevention and response to public health emergencies,7 through promoting the institutionalisation and enforcement of laws, legislations and regulations. Myanmar has several laws, regulations, guidelines and standard operating procedures underpinning key aspects of health preparedness and response.12 However, they are not formally described in the existing draft laws that are being prepared for parliament as most are in the draft stage, requiring finalisation and endorsement followed by implementation.12 For instance, Myanmar has developed the National One Health Strategic Framework and Action Plan, involving three key ministries in 2019. Myanmar also is the first Association of Southeast Asian Nations (ASEAN) country to draft a national Chemical, biological, radiological and nuclear action plan. These are important milestones, illustrating attempts for multisectoral collaboration. But they need to be enforced and transformed into actions through endorsement from Parliament. As Gustafsson denoted ‘institutions without enforcement are not institutions at all’, the outcomes of the IHR strengthening efforts will depend on how these rules are enforced within the system.35 Myanmar should also have independent regulatory organisations which are assigned to enact the prescribed law or policy. It will be essential to separate regulatory and public health functions within government departments to avoid ‘regulatory capture’.36
Conclusion
Focusing on IHR technical capacities alone will not lead to the sustainable development of IHR strengthening in Myanmar. Myanmar health system should promote a culture which is conducive for better health system governance as multidisciplinary, multisectoral and multistakeholder working is paramount for IHR improvement. Without the principles of good governance, developed IHR capacities cannot be sustained or owned by the people of Myanmar. This paper highlights the importance of the relationship between governance and IHR in the context of the sustainable development goals (SDGs). As SDGs interlink with one another, persuing one SDG can effect (positively or negatively) other SDGs.37 This paper highlights how governance (SDG 16: peace, justice and strong institutions) influences indicator 3.d.1 (IHR capacity and health emergency preparedness) of SDG 3 (health and well-being for all at all ages).
The COVID-19 pandemic is a litmus test for Myanmar health system as it highlights whether the country is able to detect, assess, report and respond to a public health emergency at all levels of Government. The pandemic highlights the importance of governance more than ever as it has to move beyond the Government and public institutions with collective actions from responsible citizens. Myanmar like all countries should learn from the COVID-19 experience as the pandemic underscores that governance and IHR are indivisible as key governance principles and are paramount to achieving multisectoral, collaborative working in the country. Myanmar should continue to build on its unique socio-demographics, geopolitical conditions with resources they have, focusing on what is feasible, acceptable and sustainable for its own health system. Myanmar has demonstrated that the role of the Government in stewardship in health and its relation to other stakeholders whose activities impact on health is the key enabling factor in progressing IHR compliance. Sustaining this high-level political commitment and achieving multisectorality are essential to achieving improved health security through better IHR compliance.
References
Footnotes
Handling editor Seye Abimbola
Twitter @Thidar_Pyone, @DrSamColl
Contributors TP and AW conceived the idea for the paper. TP made the first draft of the manuscript. All authors contributed to drafting the manuscript. All authors approved the final version of the manuscript.
Funding This study was funded with the UK Aid grant for Official Development Assistance on IHR strengthening project through the Department of Health and Social Care UK.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All relevant data sources have been referenced in the paper.