Article Text

Abstract
Introduction Despite the rapid growth of research on transgender (trans) health globally, the extent of research on trans men and other transmasculine persons assigned the female sex at birth remains unclear. We, therefore, conducted a scoping review on trans men’s health in low-income and middle-income countries (LMICs).
Methods The review included peer-reviewed articles and conference abstracts, and grey literature published from 1 January 1999 to 5 July 2019 in English, French, Hindi or Spanish and reporting original quantitative and/or qualitative data on the health of trans men or transmasculine persons living in LMIC. Studies were excluded if they did not disaggregate data for trans men or if they only described surgical techniques or laboratory values.
Results We included 53 studies (42 peer-reviewed and 11 grey literature) from 19 LMIC. Most were conducted in higher-middle-income countries (n=12) and in Latin America (n=16, 30.2%), the Middle East (n=14, 26.4%) or Sub-Saharan Africa (n=12, 22.6%) and published in 2014 or later (n=44, 83.0%). Approximately half of studies used quantitative methods (52.8%, n=28), of which 64.3% (n=18) had fewer than 50 participants and 14.2% (n=4) had over 150. Across study designs, social determinants of health and gender-affirming care were the most commonly represented domains (49.1% and 47.1% of studies respectively), with common themes including gender-based violence, coercion and discrimination as well as unprescribed hormone use. Other domains represented included mental health (32.1%), sexual and reproductive health (24.5%), general healthcare access (18.9%), physical health (9.4%) and substance use (9.4%).
Conclusion Greater inclusion and disaggregation of trans men and transmasculine persons in global health research is needed to support sex- and gender-based analyses of trans health. Community-based research approaches and theoretically driven research may help to increase the relevance and rigour of such research. Funders should invest in research on trans men’s health in LMIC.
- systematic review
- review
- public health
- mental health & psychiatry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
A 2016 systematic review identified only three quantitative studies from low-income and middle-income countries (LMIC) reporting disaggregated data on trans men.
What are the new findings?
We identified 42 peer-reviewed and 11 grey literature studies on trans men’s health in LMIC, predominantly from higher-middle-income countries.
Most studies had small samples of trans men and only nine studies were specific to trans men.
Social determinants of health and gender-affirming care were the health domains most commonly addressed, and measures of current mental or physical health status were limited.
There were regional differences in research production, foci, and methods, with the Middle East and North Africa being the only region in which clinical studies predominated.
What do the new findings imply?
Despite the rapid increase in global trans health research, data on trans men in LMIC remain scarce and limited in their ability to inform interventions.
Increased collection and disaggregation of data on trans men, in partnership with communities, is needed to advance the field of global trans health.
Introduction
Globally, transgender (trans) people face stigma, discrimination, and social exclusion.1 Within this context, available data indicate numerous health and healthcare inequities between trans and cisgender (non-trans) people. For example, trans populations experience a high burden of depression and suicidality,2 3 HIV infection4 5 and unmet healthcare needs.6 7 These health inequities were, until recently, made largely invisible by systemic exclusion or ‘erasure’ of trans people in health research and information systems.8 9 Since about 2013, there has been remarkable growth in health research on trans populations, but research remains concentrated in high-income countries. In a systematic review of peer-reviewed quantitative trans health articles from 2008 to 2014, under one-fifth (22 of 116) were from low-income or middle-income countries (LMICs).10
Trans people assigned the female sex at birth, including trans men and other transmasculine persons (collectively referred to as ‘trans men’ herein) in LMIC, are particularly understudied. Only three LMIC publications in the aforementioned systematic review included disaggregated data on trans men.10 This may be due to scientific and donor interest in the nexus of trans health and HIV, with a widely cited 2013 review estimating 18% HIV prevalence among trans women in LMIC. While HIV research often addresses comorbidities, social determinants of health and healthcare barriers that are relevant to trans health more broadly, such research has almost universally excluded trans men.11 Notably, the assumptions about sexuality and sexual behaviours underlying this exclusion are not empirically supported, with scant evidence from countries with generalised epidemics indicating high HIV risk among trans men.12
This apparent under-representation of trans men in global health research has both scientific and human rights implications. Trans populations, regardless of geographical location or birth-assigned sex, share in common a set of trans-specific social experiences (eg, stigma) and healthcare needs (eg, many trans people require hormone therapy).10 However, the health of trans people, like that of cisgender people, is also shaped by sex-linked biology, gendered socialisation and gendered social relations.13 A lack of data on trans men’s health may lead to inappropriate extrapolation from trans women and missed opportunities to enhance understanding of sex-based and gender-based health and disease processes through comparative analyses. Similarly, trans people’s health is impacted by the contexts in which they live. Clearly, there is much diversity across LMIC with respect to the policies, health systems and cultural norms that impact trans people.14 For instance, in some LMIC gender non-conformity is explicitly or de facto criminalised, while the world’s most progressive gender recognition laws have been implemented in Latin American LMIC.14 Yet, there are shared challenges that warrant a specific focus on LMIC, including a dire lack of gender-affirming health services; psychopathologisation and stigmatisation; and invisibility of trans men.1 The exclusion of trans men from research contributes to their invisibility and may therefore reinforce their exclusion from policy processes. In India, for example, a historical presence of communities with indigenous transfeminine identities15 has meant that in the public, policy-making and scientific spheres, the image of who a trans person might be is often limited to trans women. This perception is further reinforced by the invisibility of trans men in health research and policy, shaped by the central role of India’s state and donor-supported HIV programmes as vehicles for trans health and policy initiatives.16 As a result, trans men have been largely excluded from deliberations on trans rights legislation and its potential health impacts.17
Despite the continued rapid growth of trans health research since 2014, the extent of research on trans men’s health in LMIC is unclear. We, therefore, conducted a scoping review of original peer-reviewed and grey literature research on trans men’s health in LMIC published over a 20-year period from 1999 to 2019. The objectives of the review were to characterise the geographical and topical range of existing research, methodological and theoretical approaches employed, and health outcomes or processes identified among trans men. We aimed to inform future research and health services by identifying gaps and opportunities in the extant literature, and emergent health concerns.
Methods
We conducted a scoping review following Arksey and O’Malley’s framework18 and present the review following Preferred Reporting Items for Systematic Reviews and Meta-Analyses-Extension for Scoping Reviews guidelines.19 The review protocol was preregistered with the Open Science Framework on 2 December 2019 (osf.io/enqt2).
Study eligibility
Eligible publications were peer-reviewed articles, published conference abstracts or grey literature published from 1 January 1999 to 5 July 2019 and including original quantitative and/or qualitative data on the health of trans men living in LMIC. Based on the language capacity of team members, included publications had to be in English, French, Hindi or Spanish. Trans men were defined to include individuals assigned female at birth who self-identify as a different gender, including but not limited to as a man, transgender man or gender non-binary. As terminology and ascertainment approaches vary across time, place, and research field, reviewers sought explicit and implicit evidence that participants met this expansive definition of trans men. For example, studies describing participants only as ‘transgender’ were excluded unless female assigned sex at birth could be clearly inferred from reported data. Similarly, studies that mislabelled transgender women as ‘transgender men’ were identified and excluded based on other reported information (eg, HIV-related studies in which male sex at birth was an inclusion criterion). Health was defined broadly to include physical and mental health, access to care, and social determinants of health. LMICs were categorised based on World Bank classifications as of June 2019. Review articles, commentaries or editorials and clinical case reports were excluded. Studies were also excluded if they did not report any disaggregated data for trans men (quotes or themes attributed to trans men in the case of qualitative data) or if they described surgical techniques/results or laboratory values alone.
Search strategy and information sources
For peer-reviewed literature, we searched Medline, Embase, PsycINFO, CINAHL, Social Science Citation Index and Global Medicus Indicus using search terms related to the concepts of (1) trans men and (2) LMIC. The search strategy was developed in consultation with a research librarian and informed by previous systematic reviews on global trans health.10 20 21 Health-related search terms were not used to avoid excluding potentially relevant articles from non-health disciplines. The final MEDLINE search strategy is presented in online supplemental table 1). We also handsearched the reference lists of included articles.
Supplemental material
For grey literature, we searched Google and Google Scholar using the search terms (‘trans men’ or ‘transgender men’) and ‘(country)’ for each LMIC and scanned the first 10 pages of results to identify potentially relevant reports. These searches were conducted in English only. We also contacted experts in global trans health (both individually and via relevant listservs) to request information on potentially eligible articles or reports. We searched for ‘transgender’ on the websites of international health organisations (eg, WHO and United Nations Development Programme, and their regional affiliates) and reviewed results for any empirical data on trans men in LMIC. Finally, we handsearched the websites of organisations recommended by subject matter experts and all publicly available abstract books from the biannual symposia of the World Professional Association for Transgender Health.
Study selection
Two independent reviewers (VK and AS) screened all titles and abstracts for inclusion in Covidence (Veritas Health Innovation, Melbourne); conflicts were resolved through discussion. Next, the full texts of remaining references were screened following the same process.
Data charting
Using a standardised form in Google Sheets, one reviewer (VK, AS for Spanish articles) extracted data from each included article and AS double checked all extracted data for accuracy and completeness. Discrepancies were resolved by discussion to reach consensus. The form was calibrated on the first ten articles and revised before extraction proceeded. The reviewers met weekly or biweekly to review data extraction and discuss any potential disagreements. Data were extracted on bibliographical information (eg, year, type of reference) and study characteristics (country, sample size, definition of trans men, methodology, study design, recruitment approach, theoretical perspective). Studies were tagged by the health domain(s) they reported on, including gender-affirming care (hormones and/or surgeries), general physical health, healthcare access (not specific to medical gender affirmation), mental health, sexual and reproductive health, social determinants of health and substance use.
Participant characteristics extracted (if reported) included age, educational attainment, sexual orientation and urban or rural residence. For quantitative data, the frequency of each health outcome and any identified correlates were charted. For qualitative data, key themes identified by the authors and representative quotes were charted; for mixed-gender samples, we focused on themes that were attributed to trans men or transmasculine participants.
Synthesis of results
Using a narrative synthesis approach, we grouped the studies by region of origin (using World Bank classifications), methodology (qualitative or quantitative), type of publication (peer-reviewed article or academic conference abstract vs grey literature) and by health domain. Reflecting the regional structure of many global health organisations, funding mechanisms and trans social movements, we stratify findings primarily by world region. Countries within these regions are highly heterogeneous, however, and study findings should not be assumed to be generalisable to the region from which they come. We chose to group conference abstracts with peer-reviewed articles to characterise the state of scientific research on trans men in LMIC. We also mapped the LMIC represented in included peer-reviewed studies.
Patient and public involvement
This review is part of an ongoing collaboration involving researchers and trans community members in India, Canada, and the USA. Trans men participated in developing the review protocol and coauthoring this manuscript.
Results
Study selection
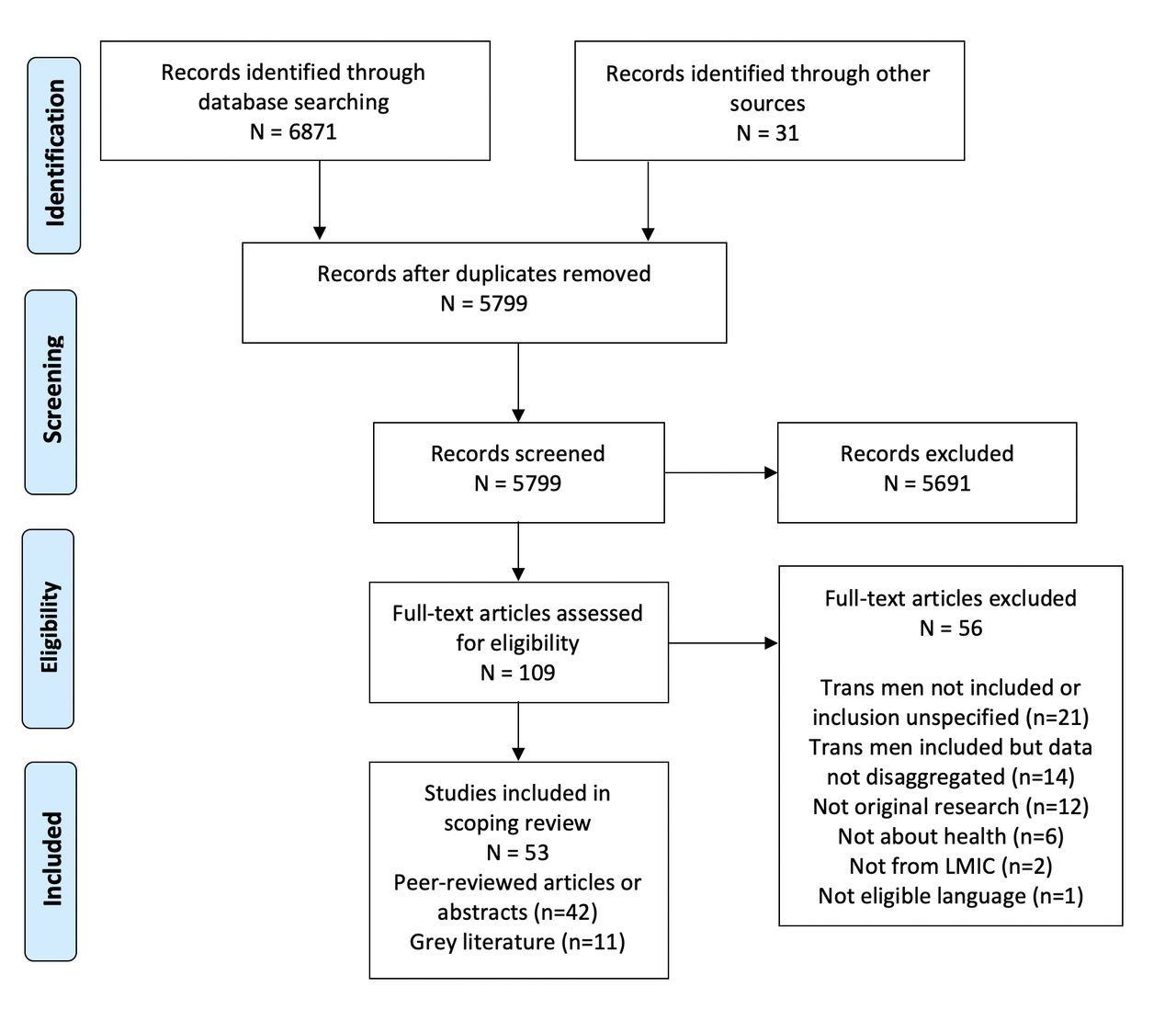
After removal of duplicates, 5799 references were screened, including 5768 identified via scholarly database searches and 31 from other sources (figure 1). We screened 109 full texts and excluded 56, most often because trans men were not clearly included (n=21) or because data from trans men were not disaggregated (n=14). Fifty-three studies met eligibility criteria; a list is included in online supplemental materials.

PRISMA flow diagram. LMIC, low-income and middle-income country; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
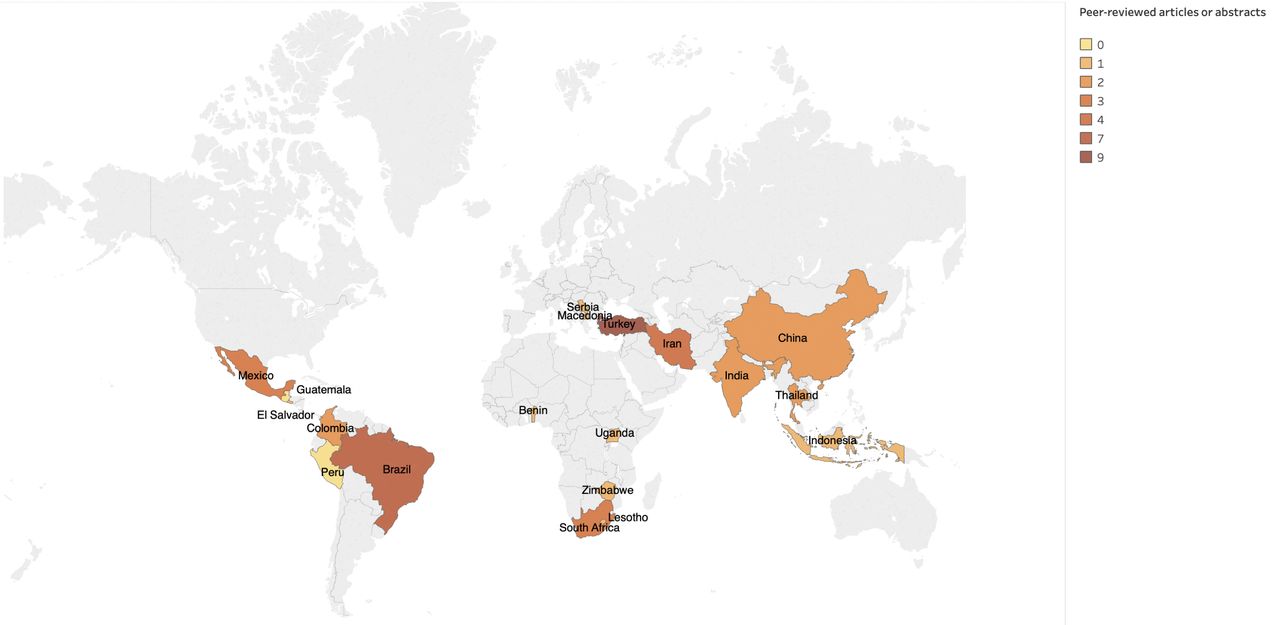
Of the 53 included studies, 42 were peer-reviewed articles or academic conference abstracts and 11 were grey literature (table 1). Studies were conducted in 19 LMIC (three low-income, four lower middle income and 12 higher middle income in 2018) across six world regions (figure 2), with most conducted in Latin America (n=16, 30.2%), the Middle East and North Africa (n=14, 26.4%) or sub-Saharan Africa (n=12, 22.6%). Grey literature was primarily from sub-Saharan Africa (n=5) and Latin America (n=3). Few studies were published in the first 15 years of the search period, with 83.0% (n=44) published in 2014 or later and 39.6% (n=21) published in 2018–2019 alone. Approximately half of studies used quantitative methods (52.8%, n=28), including one mixed-methods report. Quantitative studies were predominantly cross-sectional surveys (n=19) or chart reviews (n=8). Of quantitative studies, 64.3% (n=18) had fewer than 50 participants and only 14.2% (n=4) had over 150 participants. With the exception of three studies from East Asia,22–24 all of the quantitative studies reported only descriptive data disaggregated for trans men; regression and correlational analyses were either not conducted or pooled with other participants (generally trans women). Across study designs, only nine study samples were comprised exclusively of trans men.25–33 Five studies (9.4%) explicitly referenced theoretical or conceptual frameworks used to guide data collection and/or interpretation (not shown in table). These included ‘treatment itineraries’,26 a ‘human rights-based health framework’,34 ‘structural gender identity formation’ and intersectionality,27 intersectionality35 and social worlds theory.36 Characteristics of individual studies are described in online supplemental table 2 for qualitative data and in online supplemental table 3 for quantitative data.
Characteristics of included studies of trans men’s health in low-income and middle-income countries

{kind=link}
{kind=link}
Countries represented in peer-reviewed studies on the health of trans men in low-income and middle-income countries.
Health domains
Social determinants of health and gender-affirming care were the most commonly represented domains, included in 49.1% (n=26) and 47.1% (n=25) of studies, respectively. General physical health and substance use were least often addressed (9.4%, n=5 each). Notably, grey literature was about twice as likely as peer-reviewed studies to include social determinants of health (81.8% vs 40.5%). In boxes 1 and 2, we summarise key themes and outcomes ascertained in qualitative and quantitative studies, respectively, for each health domain. Both cross-cutting and contrasting foci emerged. For instance, related to gender-affirming care, use of unprescribed hormones obtained outside the health system was frequently reported by trans men, and related in qualitative research to a lack of willing prescribers. Studies of healthcare access highlighted perceived stigma and discrimination in healthcare settings, and consequent avoidance of care. Few qualitative studies explicitly addressed mental health; in contrast, quantitative studies frequently reported on mental health outcomes, but these were largely diagnoses extracted from clinical records or recall of historic symptoms (in adolescence), which may not reflect current mental health burden. Social determinants of health addressed across studies included legal gender recognition (ie, ability to change name or gender marker), family acceptance or rejection, and gender-based discrimination or violence. Qualitative studies specifically highlighted the use of violence and social pressure to enforce cisnormativity and heteronormativity, as well as experiences of sexual violence among trans men, which was not separately measured in any of the quantitative studies.
Themes in qualitative research on trans men’s health in low-income and middle-income countries, 1999–2019
Gender-affirming care
Health system39 40 58 (eg, lack of qualified and willing providers) and financial28 34 70 barriers to hormone therapy and surgery.
Pathologisation and restrictive gatekeeping in assessment for hormones and surgery.40 47 59
Medically unsupervised hormone use.25 26 34 40
Reliance on peer networks to access hormones and medical referrals.25 26 60
Perspectives on diagnosing gender incongruence in childhood and adulthood.40 49
‘I started using hormones a month ago. There’s a black market, you know?…I started looking for medical follow-up, because I have a health plan, so I went to several doctors. But for example, the psychiatrist I saw said he couldn’t treat me…The endocrinologist said he couldn’t see me, because he wasn’t familiar with the subject. So, I said to myself, ‘Okay, I’ll do it on my own.’…No doctor wants to treat us…’ – Trans man, Brazil, Braz 2019.26
Healthcare access
Avoidance of care due to negative experiences26 74 or gender-incongruent identification.27
Stigma and discrimination from healthcare providers.60 61 73 74
Denial of health insurance.35
‘When you go to a clinic there are so many questions in there: ‘Are you a woman? Are you a man? Why do you dress like this?’ You just get angry… I went to a clinic. I was feeling ill, and then this woman happened to come and was like, ‘Eh, are you a man or a woman?’ And she was touching my breast. She was like, ‘Let me check.’ I got pissed. After that I never went back to hospital, any other hospital.’ —Transgender/lesbian-identified Ugandan, Minor Peters 2019.74
Mental health
Negative impacts of gender normativity and harassment.27 62
Importance of self-acceptance and gender transition for positive mental health.27
‘When I began my transition socially I began to feel better. This was my true self and through acceptance and expression I felt better.’—Trans man, Peru, Perez-Brumer 2020.27
Sexual and reproductive health
Limited information about potential sexual health impacts of gender-affirming care.48
Diversity of sexual behaviours and partners29 63 69 and transactional sex.67 74
Difficulty accessing sexual and reproductive health information and care.29 69 74
‘I am happy because I was raped and was scared of being HIV positive, I am HIV negative.’—South African participant, Stevens 2012.69
Social determinants of health
Obstacles to changing name and gender marker on identity documents.27 60
Pressure, harassment and violence to enforce gender conformity and heteronormativity.25 27 36 68 71 74
Pressure to marry cisgender men; forced marriage.62 74
Sexual violence related to gender identity and/or sexuality.25 28 36 69 71 74
Impacts of stigma on sexuality and sexual health.63
Stigma and discrimination in employment and educational settings.25 27 35 60 68 71
Family rejection.25 36 62
Abuse by police.25 74
‘Where should I begin, from work, from school or from what happened in my family? It happens a lot so I’ll start from the simplest. When you start working they expect to see a woman, you have a pink identity card. But there you are standing there looking completely like a guy. They get appalled. They start attacking psychologically. They expect a lovely female, one that they can harass.’ Trans man, Turkey, Güngör et al. 2014.60
Health outcomes assessed in quantitative research on trans men’s health in low-income and middle-income countries, 1999–2019
Gender-affirming care
Hormone use22 31 42–44 54 55 66 and non-prescribed hormone use.22 31 42 55 90
Gender-affirming surgical history.38 42–45 54 55 64 66
Desire for22–24 65 and reasons for not using31 42 43 hormones or surgery.
Other hormone experiences (eg, denied prescription, monitoring, needle sharing, satisfaction).22 43
Completion of assessments required to access care (eg, ‘real-life test’, group therapy).33 55
Healthcare access
Perceived discrimination in healthcare.31 43 65
Avoidance of healthcare.31
Consults a physician regularly.65
General physical health
Polycystic ovarian syndrome.38
Health-related quality of life.22
Attitudes regarding uterus donation.32
Weight/body mass index.56
Mental health
Recall of distress and functional impairment related to gender in adolescence.44 45 66
Depressive and anxious symptomatology23 24 or psychopathology symptoms.56
Diagnosed mood,24 33 50–52 anxiety,33 50–52 personality33 51 or other psychiatric33 51–54 disorders.
Self-harm.23 24 54
Suicidal ideation and attempts.23 24 54 55 57
Health-related quality of life.22 54
Use of mental health services.24 31
Disordered eating and body uneasiness.56
Sexual and reproductive health
HIV testing and status.29 46 90
Sexually transmitted infection history.31
HIV postexposure prophylaxis awareness and use.46
Use of gynaecological care, paptesting or human papilloma virus self-testing.30 31 41
Chest self-examination.31 41
Condom/barrier use.31 41
Multiple sexual partnerships.72
Social determinants of health
Peer rejection or bullying in childhood or adolescence.24 44 45 66
Discrimination or violence related to gender.24 31 44 54 66 72
Family acceptance, rejection or conflict.22 24 45 55 64
Heath insurance status.31 55
Legal name or gender marker change.31 65
Community acceptance of gender identity.72
Substance use
Findings by world region
East Asia and the Pacific
Of five studies from East Asia and the Pacific, there were two each from China and Thailand, and one from Indonesia. Across countries, participants were young (eg, mean ages of 24–25) and urban dwelling (86%–100%). The studies from China reported on quantitative data from the same online survey and had the largest samples in the review, with 581 and 682 trans men across the two papers.23 24 Trans men were identified using the ‘two step’ method (separate questions about sex assigned at birth and current gender identity37) and 73% were university educated. The studies focused primarily on mental health but also reported data on social determinants of health and need for gender-affirming care. Correlates of mental health outcomes were identified, including need for gender-affirming surgery (depression, anxiety and suicidal ideation)23 24 and discrimination or violence in public places (suicide attempts).24
In Thailand, a survey including 60 participants described by the authors as ‘toms’ (a term used in Thailand for masculine persons assigned female at birth) provided data on gender-affirming care, health-related quality of life and familial acceptance.22 Hormone use was associated with poorer scores on a number of quality-of-life dimensions and with less parental acceptance. A qualitative study from Thailand included one trans man, self-identified in Thai as ‘phu chai kham phet’, who described discrimination in education and in obtaining health insurance, mitigated by self-advocacy. Finally, a qualitative study from Indonesia comprised 12 trans men and focused on experiences of discrimination in family, education, employment and public contexts, as well as so-called ‘corrective’ pressure and violence aimed at enforcing gender conformity.25
Europe and Central Asia
A chart review from Serbia’s gender clinic (gender clinics assess individuals seeking gender-affirming medical care) included 76 trans men and reported on the prevalence of gender-affirming surgery and of Polycystic Ovarian Syndrome, which was more common among trans men than in the general population of people assigned female at birth.38 Five trans men participated in a qualitative study of sexual and gender minorities in Macedonia and reported legal barriers to accessing medically supervised hormone therapy.39
Latin American and the Caribbean
In Latin America, there were seven studies from Brazil, three from Columbia, three from Mexico, and one study each from El Salvador, Guatemala and Peru. Three were published in Spanish.31 40 41 Where reported, participants were primarily young (eg, mean ages of 23–30) and urban dwelling (67%–100%). Educational attainment varied; some samples were predominantly university educated26 31 but completion of secondary school was the norm in most.42–46
Two Brazilian studies drew on the same survey of trans people recruited via a gender clinic and an online survey, with 156–188 trans men identified using the two-step approach.43 46 One study described HIV testing and postexposure prophylaxis histories46 while the other focused on gender-affirming care, including barriers to hormonal and surgical care, and use of unprescribed hormones.43 The other five studies from Brazil also addressed gender-affirming care, including a community survey (116 trans men)42 and a clinic-based survey (24 trans men) conducted as part of field tests for the new diagnosis of Gender Incongruence in the International Classification of Diseases, V.11 (ICD-11).45 Qualitative studies described obstacles to hormones and gender-affirming surgery including cost, need for psychiatric diagnosis, and a lack of physicians willing to prescribe hormones, leading to medically unsupervised use.26 34 47
Studies from Colombia included a grey literature report of an lesbian, gay, bisexual and transgender (LGBT) community survey that provided data on sexual and reproductive health among six trans men,41 a conference abstract on sexual health in the context of gender-affirming medical care,48 and a qualitative study of challenges in accessing appropriate gender-affirming care.40 In Mexico, two studies drew on ICD-11 field tests, including a survey of patients at a trans care specialty clinic (46 trans men) and a qualitative study describing the perspectives of four adult trans men on the proposed diagnostic category of gender incongruence of childhood.49 In Guatemala, a community organisation of trans men conducted an online survey with 50 participants that collected data on a wide range of health outcomes and social determinants of health.31 Finally, a book chapter reported on findings of a qualitative study of trans men in Peru, highlighting challenges and strengths such as the negative impacts on healthcare access of legal non-recognition of gender, as well as the positive mental health impacts of self-acceptance and online community-building.27
Middle East and North Africa
Iran and Turkey were represented in four and 10 studies respectively (all but one peer reviewed). Across the two countries, the mean age of trans men participants ranged from 24 to 29 and most were in urban areas (93%–100%) when specified. All studies from Iran were chart reviews of gender clinic patients and reported primarily on mental health diagnoses among samples of 36–143 trans men; two studies also reported on smoking prevalence.50–53 The six quantitative studies from Turkey were also gender clinic-based (chart reviews and surveys) and included 31–99 trans men.32 33 54–57 Five of six reported on mental health outcomes, including suicidality in three studies. Family and social support were captured in three studies. Data from trans men in the four Turkish qualitative studies (including one grey literature report) were primarily related to gender-affirming care and healthcare access.58–61 Key themes included healthcare stigma, a lack of providers with competence in caring for trans men, and discrimination related to gender-discordant identity documents. One qualitative study highlighted patient perspectives on the practices of gender clinics; two trans men described the assessment process, including mandatory psychotherapy, as heteronormative, therapist-centred and exclusionary of people with mental health conditions.59
South Asia
Four studies from India included a chart review with 18 trans men, a grey report on a survey including 27 trans men, a book on a qualitative study including 28 transmasculine persons, and a qualitative study with about 10 participants who we coded as transmasculine.62–65 Study participants were almost exclusively urban dwelling and young on average (eg, mean ages of 23–25). The chart review reported on surgical history and family support64 while the grey literature survey described social determinants of health including gender-congruent identity documents, access to sanitation and pressure to marry.65 In a qualitative study describing meanings of sex and intimacy among Indian sexual and gender minorities, no participants self-identified as trans men, but rather were presumably assigned female at birth and identified as non-binary, genderqueer or genderfluid.63 These participants reflected on diverse interpretations of ‘sex’ and the impacts of stigma and trauma on sexuality. In another qualitative study of queer people assigned female at birth, 10 participants identified as men and 18 expressed identities outside the gender binary.62 The study explored struggles faced by trans men and non-binary persons in family contexts, including violence, rejection and forced marriage, and consequences for mental health (ie, suicidality), forced migration, and loss of social capital and support. The study also highlighted the intersectionality of class and caste marginality with gender-based violence and discrimination.
Sub-Saharan Africa
Of 12 studies from sub-Saharan Africa, there were eight from South Africa (three peer-reviewed and five grey literature) and one each from Benin, Lesotho, Uganda and Zimbabwe (all peer reviewed). In contrast to other world regions, four studies explicitly included rural-dwelling participants. Where age was specified, all participants were 46 years old or younger; mean ages were 25–28. All used community-based recruitment approaches, with the exception of an ICD-11 field test study from South Africa, which also used clinic-based recruitment.66 The other two peer-reviewed studies from South Africa were qualitative and had just one and three trans man participants, who provided data on transactional sex67 and religiously motivated stigma in rural educational settings.68 Grey literature from South Africa included two studies on sexual and reproductive health: a mixed-methods study of HIV testing, stigma and access to sexual health services among 25 trans men who have sex with men29 and a qualitative study addressing diversity of sexual health needs and experiences of sexual violence among approximately 15 trans men.69 Other South African grey literature included a thesis with one trans man participant who reported financial barriers to medical gender affirmation,70 a report on life histories of three trans men,28 and a Human Rights Watch report on discrimination and violence faced by lesbian women and transmen.71
Elsewhere in the region, a quantitative survey in Benin with 34 trans men addressed social determinants of health such as community attitudes towards gender diversity, as well as substance use.72 Qualitative studies from Zimbabwe and Lesotho included one and three trans men and discussed healthcare discrimination and community and family rejection of gender diversity, respectively.36 73 Finally, a Ugandan qualitative study on HIV prevention and treatment interviewed 30 people assigned female at birth who self-identified as men, ‘lesbian men’, or ‘transgender lesbians’. Participants reported gender-based violence from strangers and police, pressure to engage in relationships with cisgender men and avoidance of health services.74
Discussion
Overview of findings
Over a 20-year period, we identified 39 peer-reviewed journal articles, three peer-reviewed conference abstracts, and 11 grey reports providing data on the health of trans men in 19 LMIC. Trans men were most often included in small numbers as part of larger trans or LGBT participant samples: only nine studies (five peer reviewed) focused exclusively on trans men. These findings build on a previous review of global trans health research published in 2008–2014.10 That review found rapid growth in trans health publications over time but a small number of studies focused on people assigned female at birth; these trends continue to be evident in the present review. Included studies were not representative with respect to global population distributions, with the majority coming from Latin America (n=16) or the Middle East (n=13) and relatively few from East (n=5) or South (n=4) Asia. Although the true demographic characteristics of trans populations are largely unknown, participants in these studies appeared to be disproportionately young and urban; where specified, all samples of trans men had a mean age of 30 or less.
Policy and practice implications
Our findings have implications for global health and development funding, social policies and programmes, and healthcare services. First, expanding the evidence base on trans men’s health in LMIC will require investments by global and national health research funders and donors, including potentially earmarked funds for non-HIV-specific trans health research in academic and community settings. Funders who have traditionally supported trans health research via HIV programmes could incorporate research on the holistic health needs of trans people, including trans men, within gender equity portfolios. Research foci will be context-dependent and ideally driven by community-identified needs, but this scoping review indicates a few key research gaps and cross-cutting issues warranting further investigation. These include studies of mental health status and its determinants; family, community and healthcare provider treatment of trans men; and interventions to expand access to high-quality gender-affirming care. Trans men may be considered ‘hard-to-reach’ due to their relative social invisibility and a lack of nongovernmental organisations. Therefore, community-based participatory research approaches—including capacity-building for trans-led nongovernmental organisations—should be considered to meaningfully engage trans men in research and maximise research impact.75
Second, our synthesis highlights health and human rights issues facing trans men across multiple LMIC. Themes of gender-based violence and discrimination were recurrent across studies, with some trans men reporting violence specific to the intersection of gender non-conformity and female sex assignment, such as coercion to partner with cisgender men. Gender-based violence programmes and policies that recognise and respond to violence faced by trans men, using gender-affirmative approaches, are needed. Medically unsupervised hormone use was another cross-cutting theme and underscores the urgency of increasing the number of physicians and other healthcare providers willing to prescribe and monitor hormone therapy in LMIC; testosterone therapy can generally be managed in primary care settings and clinical guidelines are available in multiple languages.76 77
Study research methods and implications
Included studies drew on a range of methods and sampling approaches but had numerous methodological limitations. Quantitative studies were almost exclusively cross-sectional and descriptive, with very small sample sizes (median=43). We did not identify any interventional studies and only one had a longitudinal design.56 Thus, understanding of determinants of trans men’s health outcomes in LMIC and potential strategies to improve their health remains largely absent. Most qualitative studies included trans men incidentally and/or in very small numbers; 15 of 24 qualitative studies included five trans men or fewer. They too, therefore, provide limited insight on health processes specific to trans men or how those processes may differ from other groups under study. We also observed that just five studies made explicit reference to theoretical frameworks used to guide study design or interpretation. Moreover, these theories were largely non-trans-specific, and no studies drew on frameworks such as gender minority stress and gender affirmation that have been commonly used in trans health research.78–81 Future research could be strengthened by adapting existing frameworks, and developing new frameworks, for research with trans men in LMIC.
As reflected in nosological changes to both the ICD-11 and the Diagnostic and Statistical Manual of Mental Disorders,82 83 trans identities are increasingly being depathologised. This depathologisation is associated with a shift towards research on trans populations—self-identified trans people in community settings—versus on trans patients with a psychiatric diagnosis. Nevertheless, in our review, 20 studies used clinic-based recruitment, of which 12 explicitly operationalised trans status based on a psychiatric diagnosis. Such studies comprised half of quantitative, peer-reviewed studies included in the review and were concentrated in the Middle Eastern region (Turkey and Iran). In addition to relying on potentially psychopathologizing frames, such studies were mostly chart reviews, which provide limited insight into the current health experiences and needs of trans men in those countries. Questions have also been raised as to the ethics and validity of research data obtained from patients seeking gender-affirming medical interventions from clinics that may be the only available source of such care.84
In studies that operationalised trans status based on identity (vs diagnosis), definitions and ascertainment methods were heterogeneous. Five studies explicitly referenced use of a ‘two-step’ method for ascertaining sex assigned at birth and gender identity. Although considered a best practice for measuring trans status, this approach has not been rigorously evaluated outside the English-speaking Global North.37 85 86 In some trans-specific studies, inclusion was based on self-identification with a trans identity (eg, ‘transgender man’); this approach may exclude persons of transmasculine experience who do not describe themselves as trans, whether because they identify outside the gender binary, use indigenous gender terms, or do not have access to transmasculine-specific terms in any language. For example, a few qualitative studies included participants who fit our expansive definition of ‘trans man’ but who self-identified with terms such as ‘lesbian man’ or ‘genderqueer’.28 63 74 Yet other studies did not indicate whether participants self-identified with the label used to describe the study population; for example, a study of ‘toms’ in Thailand.22 Particularly for ‘outsider’ (eg, non-indigenous, cisgender) researchers, it is important to appreciate that non-Euro-American identity labels such as ‘tom’, which may combine aspects of gender and sexual identity, are not necessarily commensurate with ‘transgender’.87
To ensure that trans men are included, accurately identified, and respectfully described in LMIC health research, methodological research is needed to validate measurement of gender identity in diverse cultural contexts, inclusive of both indigenous gender identities and increasingly globalised English-language terms.85 86 In recruiting trans men to their studies, researchers should consult with local communities to identify terms in local use and consider using multiple identity terms and/or descriptions in recruitment materials.
Strengths and limitations of this review
Although this review used multiple search strategies to include both academic and grey literature in four languages, it was subject to some important limitations. First, searches were conducted in English, which may have limited identification of relevant non-English references; all included studies were published in English or Spanish. Second, we defined trans men or transmasculine broadly to include persons assigned female at birth who self-identify as a different gender, and excluded studies in which participants self-identified or were described solely as women. Considering the interwovenness and conflation of sexual orientation and gender identity in many cultural contexts (eg, self-identification as a ‘lesbian man’74), this may have led to exclusion of studies on the health of persons who might be considered to have a transmasculine experience, as well as inclusion of studies wherein participants would not consider themselves as having such experience. In addition, studies that captured data on non-binary identities generally did not disaggregate non-binary participant data by sex assigned at birth,23 39 43 44 limiting our ability to extract and synthesise those data. Finally, LMICs were classified based on World Bank categories as of June 2019, which have since been updated.
Conclusions
Our review found scant research on trans men’s health in LMIC, with existing research limited in geographical coverage, demographic diversity and sample sizes. This underscores the need for inclusion and disaggregation of trans men and transmasculine persons in health research in LMIC. The need for sex-based and gender-based analysis across all fields of health research is increasingly recognised, for example, in reporting guidelines that stress disaggregation of data by sex and/or gender (as relevant) as a necessary first step.88 Similarly, trans health researchers have been called to ‘put the gender back into transgender health’10 and practitioners to address the root causes of gendered health inequities through gender-transformative approaches.89 This requires studying how biological and social sex-based and gender-based mechanisms and their interactions impact the health of trans women, trans men and gender non-binary persons, and begins with the collection of gender-specific and gender-disaggregated data. Strategies to improve data collection on trans men in LMIC may include investments in community-based organisations and health services, as well as targeted, non-HIV-specific research funding. If implemented, such strategies have the potential to benefit trans people of all genders.
Acknowledgments
This research was supported by the Canadian Institutes of Health Research—Institute of Gender and Health (Grant # PCS 161850). VC was supported, in part, by the DBT/Wellcome Trust India Alliance Senior Fellowship (IA/CPHS/16/1/502667). CL and VK’s participation was funded by an Ontario Ministry of Research & Innovation Early Researcher Award, and CL is also funded by Canada Foundation for Innovation and the Canada Research Chairs programprogramme. The authors wish to thank Rodrigo Aguayo Romero for sharing relevant grey literature.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @aydenisaac, @carmenlogie
Contributors All authors contributed to development of the review protocol, interpretation of findings and revising the manuscript for important intellectual content. AS and CL obtained funding and provided supervision. VK designed and conducted the literature searches. VK and AS conducted screening and data extraction. AS drafted the manuscript.
Funding This study was funded by the Canadian Institutes of Health Research, Institute of Gender and Health (PCS 161850).
Map disclaimer The depiction of boundaries on this map does not imply the expression of any opinion whatsoever on the part of BMJ (or any member of its group) concerning the legal status of any country, territory, jurisdiction or area or of its authorities. This map is provided without any warranty of any kind, either express or implied.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Research ethics board approval was not required for this review of published research.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.