Article Text

Abstract
Introduction Substantial disparities in care outcomes exist between different subgroups of adolescents and youths living with HIV (AYLHIV). Understanding variation in individual and health facility characteristics could be key to identifying targets for interventions to reduce these disparities. We modelled variation in AYLHIV retention in care and viral suppression, and quantified the extent to which individual and facility characteristics account for observed variations.
Methods We included 1170 young adolescents (10–14 years), 3206 older adolescents (15–19 years) and 9151 young adults (20–24 years) who were initiated on antiretroviral therapy (ART) between January 2015 and December 2017 across 124 healthcare facilities in Nigeria. For each age group, we used multilevel modelling to partition observed variation of main outcomes (retention in care and viral suppression at 12 months after ART initiation) by individual (level one) and health facility (level two) characteristics. We used multiple group analysis to compare the effects of individual and facility characteristics across age groups.
Results Facility characteristics explained most of the observed variance in retention in care in all the age groups, with smaller contributions from individual-level characteristics (14%–22.22% vs 0%–3.84%). For viral suppression, facility characteristics accounted for a higher proportion of variance in young adolescents (15.79%), but not in older adolescents (0%) and young adults (3.45%). Males were more likely to not be retained in care (adjusted OR (aOR)=1.28; p<0.001 young adults) and less likely to achieve viral suppression (aOR=0.69; p<0.05 older adolescent). Increasing facility-level viral load testing reduced the likelihood of non-retention in care, while baseline regimen TDF/3TC/EFV or NVP increased the likelihood of viral suppression.
Conclusions Differences in characteristics of healthcare facilities accounted for observed disparities in retention in care and, to a lesser extent, disparities in viral suppression. An optimal combination of individual and health services approaches is, therefore, necessary to reduce disparities in the health and well-being of AYLHIV.
- HIV
- public health
- health services research
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Adolescents and youths living with HIV have worse care and treatment outcomes compared with other groups.
Significant disparity in care and treatment outcomes exist between different adolescent and youth subgroups.
What are the new findings?
Differences in characteristics of healthcare facilities delivering services are associated with disparities in outcomes within and across adolescent and youth age groups.
What do the new findings imply?
An optimal combination of individual and health services approaches is necessary to reduce disparities in the health and well-being of adolescent and youths living with HIV.
Introduction
Adolescents and youths are an important group in global efforts to eliminate HIV. Compared with adults, adolescents and youths engage less with healthcare services and have lower viral suppression rates,1–5 resulting in increases in AIDS-related deaths despite a global reduction of AIDS mortality among other age groups.6–8 Under current circumstances, the global optimism to eliminate HIV by 2030 does not appear to hold for adolescents and youths.9 10
Suboptimal outcomes among adolescents and youths living with HIV (AYLHIV) have been ascribed to vulnerabilities associated with the developmental challenges faced in the transition to adulthood.11–13 Health service interventions designed to address these vulnerabilities include transitional and adolescent friendly care models which aim to address a limited range of clinical and psychosocial needs of AYLHIV.14–24 However, a wider consideration of the multiple, diverse and potentially interactive influences is necessary given that factors at the individual, community and health service levels individually and jointly influence outcomes. Current studies14–24 do not sufficiently disentangle the influence of these multilevel factors, and this hinders the design of specific individual-level or higher-level interventions across often heterogeneous groups of AYLHIV.
In this multilevel study, we, therefore, examined the interplay of factors influencing AYLHIV outcomes at the individual and health services levels as they relate to retention in care and viral suppression among a large sample of AYLHIV in Nigeria. Nigeria accounts for a significant proportion of AYLHIV burden in sub-Saharan Africa, and one of the few countries where mortality among AYLHIV continues to increase.25 The national HIV programme began in 2002 in only 25 public (government-owned) tertiary-level healthcare facilities. Gradual decentralisation since then has resulted in an increased mix in types and levels of healthcare facilities delivering HIV services.26 While this has significantly increased access to HIV services, it has also brought about heterogeneity in terms of how national HIV guidelines are interpreted and implemented. The extent to which these differences in service delivery channels have shaped HIV-related outcomes have received little attention partly because of little information sharing between the public and private health sectors. Our study will characterise how this heterogeneity operates alongside individual-level characteristics to affect retention in care and viral suppression within and between AYLHIV age groups. We hypothesise that differences in characteristics of healthcare facilities delivering HIV services will be associated with differences in outcomes within and across AYLHIV age groups.
Methods
Study setting and study population
Comprehensive HIV services are freely provided by the Government of Nigeria with funding support from external donors. We retrospectively evaluated routine data for AYLHIV enrolled in care between 1 January 2015 and 31 December 2017 within a network of healthcare facilities supported by APIN Public Health Initiatives Ltd/Gte treatment network (APIN). APIN is a US President’s Emergency Plan for AIDS Relief (PEPFAR) implementing agency that support delivery of comprehensive HIV services in 285 healthcare facilities spread across 95 local government areas (LGAs) in eight states of Nigeria (the country has a total of 774 LGAs distributed across 36 states; LGAs may be the equivalent of districts in other settings). The AYLHIV cohort for this study was enrolled across 124 secondary and tertiary level healthcare facilities in two of the programme’s eight states (Benue and Plateau states). Secondary facilities provide HIV services within a generalist, non-specialised clinic setting, while tertiary facilities provide services in specialist hospital settings. Healthcare facilities were included if they had provided comprehensive HIV services for at least 1 year at the time of the study.
Enrolment into care and follow-up
All AYLHIV in our study received free comprehensive HIV care according to Nigeria’s national guidelines for HIV prevention, care and treatment, which is regularly updated in line with WHO recommendations. These include antiretroviral treatment (ART) for children, adolescents and adults; the prevention of mother-to-child transmission (PMTCT) services; laboratory services including viral load (VL), CD4 count and pharmacy services.
Patients receiving care within the national ART programme are typically assigned a unique ID at care enrolment, which is maintained for every patient throughout their care/treatment life cycle. When care re-entry, care transfers or ART re-start occur, patients keep this ID and are documented as ‘existing’ (ART restart, transfer out/in and so on) and not ‘new’ enrolments. For this study, we analysed only data of AYLHIV who were newly initiated on ART within the study period. Clinical data on AYLHIV restarting ART were omitted from source during data extraction.
Outcome variables
Retention in care
For this outcome, we adapted indicator 1.3 of the 2018 Global AIDS Monitoring tool (GAM)27 which describes the percentage of adults and children living with HIV known to be on ART 12 months after starting. The GAM numerator includes number of people known to be alive and on antiretroviral therapy 12 months after starting ART, including those who interrupted care (missed one or two appointments or drug pick-ups) during the 12 months. Following the GAM, we included as our denominator (1) AYLHIV who were still alive and receiving ART 12 months after initiating treatment between January 2015 and December 2017 and (2) AYLHIV who interrupted care (missed one or two appointments or drug pick-ups). Within the numerator groups, we defined study outcomes according to the pattern of care contact at three time points (30, 90 and 365 days) within the first 12 months after initiating ART. AYLHIV were considered retained in care if they established care contact at all the three time points as evidenced by documented clinic visit and/or drug pick ups. AYLHIV were considered to have interrupted care if they did not make care contact on one or two of the three time points.
The GAM denominator includes the total number in the numerator plus those who have died, stopped treatment or were recorded as lost to follow-up (LTF) at month 12. Following the GAM, we included as denominator the AYLHIV in our numerator plus AYLHIV who were dead, stopped treatment, transferred out and LTF during the 12 months after starting ART. AYLHIV were considered LTF if there was no care contact at any of the three time points (30, 90 and 365 days) within 12 months after initiating ART. AYLHIV were considered transferred out if they were documented to have moved their care to another facility with the knowledge of their providers. Adolescents whose death were confirmed and documented in the facility records were categorised as ‘dead’. Adolescents who established care contact but had stopped HIV treatment for any reason were classified as ‘stopped treatment’.
Viral suppression
For this outcome, we adapted indicator 1.3 of the 2020 GAM tool.28 This indicator assesses the percentage and number of adults and children living with HIV who have a suppressed VL. The recommended denominator for this is the estimated number of people living with HIV who are on treatment. In line with this recommendation, we excluded from our VL analysis AYLHIV who died, transferred out or stopped treatment; and included AYLHIV who were retained in care, and those who interrupted care but returned within the 12 months. However, we also included in the denominator AYLHIV who were LTF as they represented a subgroup of interest for our study. Client tracking was conducted for all AYLHIV who interrupted care or LTF within the first 12 months after ART initiation. For our analysis, we included VL test of those AYLHIV who returned to care within a 6-month window after expiration of the first 12 months after ART initiation.
For the numerator, the GAM recommends (1) reporting the estimated number of people who have suppressed VL if VL testing coverage (ie, the number of people routinely tested among all people on treatment) is higher than 50%; or (2) reporting only the number of routine VL tests if VL testing coverage is less than 50%. Since the overall VL coverage in our total study population exceeded 50%, we report viral suppression as one of our outcomes. Consistent with the GAM indicator, we defined viral suppression as HIV-RNA VL <1000 copies/mL.
Exposure variables
Individual-level data measures
We included demographic and clinical information routinely collected during enrolment into HIV care. Demographic information collected included age at enrolment, sex, marital status, pregnancy status and level of education. Clinical characteristics included CD4 cells/mL count at enrolment, TB status, WHO clinical stage and patient-preferred ART regimen following treatment adherence counselling. Information about the follow-up drug or clinic appointments visits were also available. However, information about modes of transmission (perinatal vs behavioural infection) was not available.
Facility-level measures
We used characteristics of health facilities to assess determinants at the level of service delivery. Variables assessed included type/level of services offered (secondary or tertiary level care), the facility size (ie, total number of AYLHIV enrolled in care categorised as <200, 200–500, >500), VL test coverage (proportion of enrolled AYLHIV who have had at least one VL test at 12 months or more after initiating ART) and whether the health facility was a designated adolescent/youth friendly centre. Adolescents and youth centres within the APIN programme refer to any healthcare facility implementing dedicated services to adolescents and youths in addition to routine HIV service provision. Such services are focused on modifying certain structures of care and may include reorganising or changing the location of the clinic, establishing dedicated clinic days, formation of peer support groups, establishing adolescent–provider communication modalities, implementing appointment availability and scheduling, and training providers on adolescents and youth focused services.
Data management
We retrieved deidentified clinical data from the APIN/PEPFAR electronic database, which routinely captures patient demographic, clinical and laboratory data. APIN supports health facility information systems with a relational database management that is open source (OpenMRS; www.openmrs.com).
Statistical analysis
We first conducted descriptive analyses of baseline individual-level and facility-level characteristics using proportions, frequencies, means and median. AYLHIV in the cohort were categorised into three age groups (10–14 years young adolescents, 15–19 years older adolescents, 20–24 years young adults) and the baseline characteristics were compared for the three age groups using χ2 statistics. Next, we conducted a bivariate analysis of age group comparisons of patterns of retention in care and viral measures.
To develop multilevel models to examine the association between individual-level and facility-level factors and the two outcomes of interest (retention in care and viral suppression), we adopted a binary outcome logistic multilevel modelling approach, partitioning each outcome’s variance by its individual-level (level one) and facility-level (level two) components concurrently to account for the nested structure of our data. In this approach, we allow the model intercepts to vary at random. We conducted the modelling analysis in three steps. In the first step (Model 1, null model), we did not include any explanatory variable, allowing an estimate of the total variation in outcomes by health facilities. In the second step (Model 2), we included only individual-level factors. This step allowed us to test whether or how much of the total random variation observed in the first stage could be explained by our individual-level data. In the third step (Model 3), we added facility-level factors to Model 2. This allowed us to test whether or how much of the random variation could be explained by the facility-level characteristics. For each outcome, we repeated these model steps for each of our three AYLHIV age groups.
Measures of association (fixed effects) in our models are presented as ORs and their p values.
Measures of variation (random effects) in the models are random slope variance, intracluster correlation (ICC) and explained variation. Random slope variance indicates whether a contextual phenomenon differs in magnitude for different groups and whether the facility-level modifies associations between individual-level exposures.
To check whether the effect of explanatory variables differed across AYLHIV age groups, we conducted a multiple group analysis. We used mysuest program to combine models from the three AYLHIV age groups and then used mitesttransform command to test for equality of each variable coefficients across the three age groups using a 5% significance threshold.
To minimise potential bias due to missing data, we performed multiple imputations with chained equations after data exploration to verify that data were missing at random. A total of 163 data imputations were done as determined by the STATA module ‘how_many_imputations’.29
All statistical analyses were conducted using Stata V.16.1 (Stata Corporation, College Station, Texas, USA).
Patient and public involvement
We did not directly include the patient and public in this study, but the database used in the study was developed and is being overseen by a review board that includes patient representatives.
Patients were not invited to comment on the design of this study and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy. Study findings will be shared with the Network of People Living with HIV (NEPHWAN) as part of the dissemination strategy of this study.
Ethics
As part of the APIN protocol, written informed consent and, where necessary, assent for service provision and participation (or data use) for future evaluations were obtained at the point of enrolment into HIV care and treatment. Adolescents or minors less than 15 years at enrolment provide another written and signed informed consent as soon as they become 15 years or older when transferred/transitioned to the adult ART programme. Ethical approval for this study was obtained from the IRBs of APIN and the Institute of Tropical Medicine, Antwerp.
Results
Baseline characteristics
Our study included a total of 13 527 AYLHIV who were initiated on ART between 1 January 2015 and 31 December 2017. Table 1 presents the baseline characteristics.
Baseline characteristics of AYLHIV by age group
The demographic and clinical characteristics of the study population at ART initiation were compared by three age groups: 10–14 years, 15–19 years and 20–24 years. The three age groups were similar in terms of pregnancy status and TB status at baseline (p=0.06, p=0.27, respectively) but differed in other characteristics. As expected, young adolescents (10–14 years) were predominantly single (p<0.00), with the highest level of education at the primary level (p<0.00). Compared with the other age groups, young adolescents also had higher enrolment at a tertiary healthcare facility (p<0.00), enrolled at earlier stages of immune-deficiency (median CD4 399 cells/mL) with mostly mild or no immune deficiency at baseline. Predominant ART regimen at baseline among young adolescents was ABC or AZT/3TC/EFV or NVP, compared with the other age groups that were predominantly initiated on TDF/3TC/EFV or NVP. Older adolescents and young adult ART enrollees were almost exclusively female (82.90%–88.10%), commonly married (42.90%–59.80%) and educated up to a secondary or higher level of education (43.80%–47.60%).
Continuity of care and viral outcomes
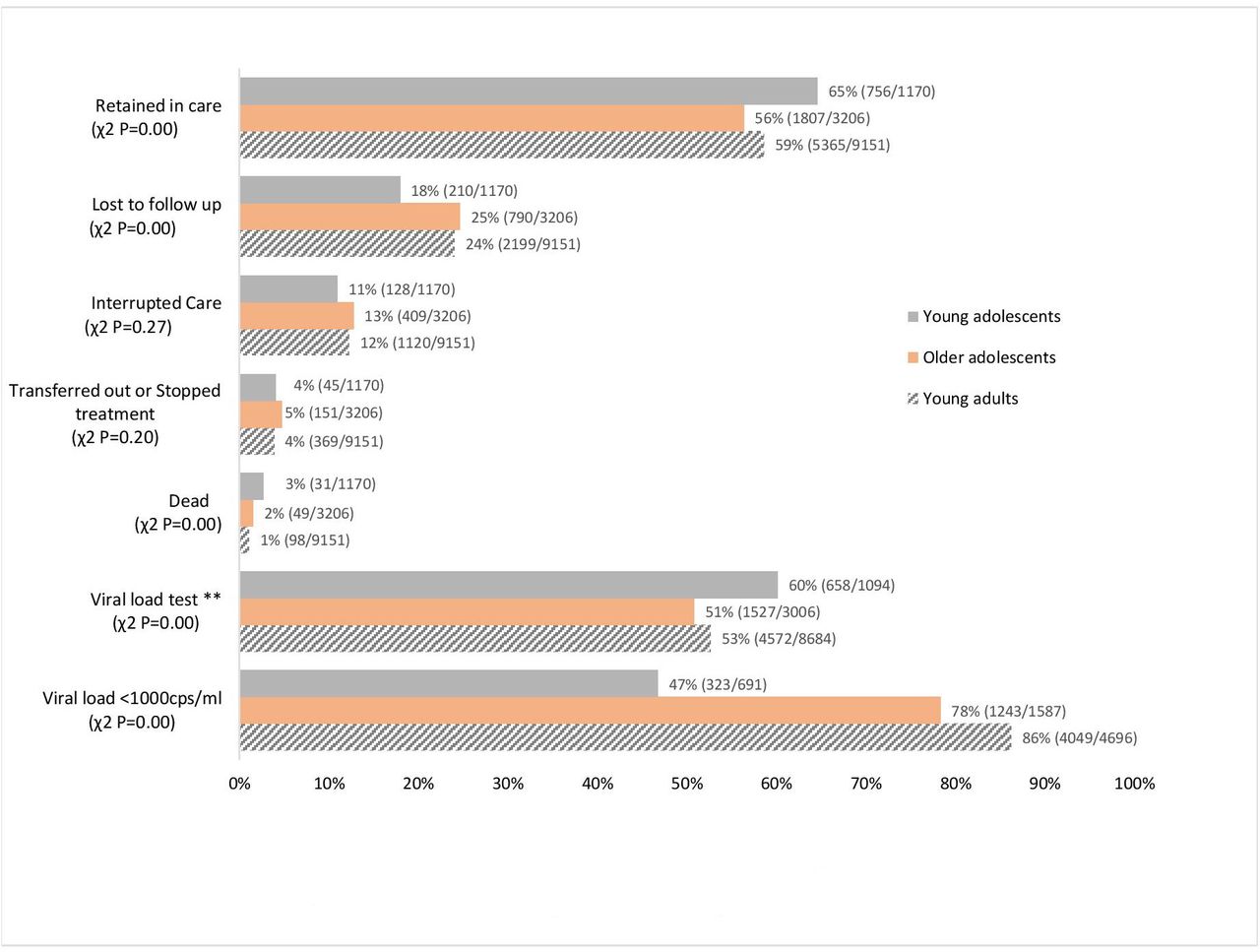
Figure 1 shows the different outcomes by AYLHIV age group. Young adolescents had a higher proportion retained in care compared with older adolescents and young adults (65% vs 56% and 59%; χ2 p=0.00). Older adolescents had a higher proportion of AYLHIV who were LTF and interrupted care (25% and 13%; χ2 p=0.00) when compared with the other age groups. However, all the age groups were similar in terms of the proportion that transferred out, stopped treatment or died (figure 1).
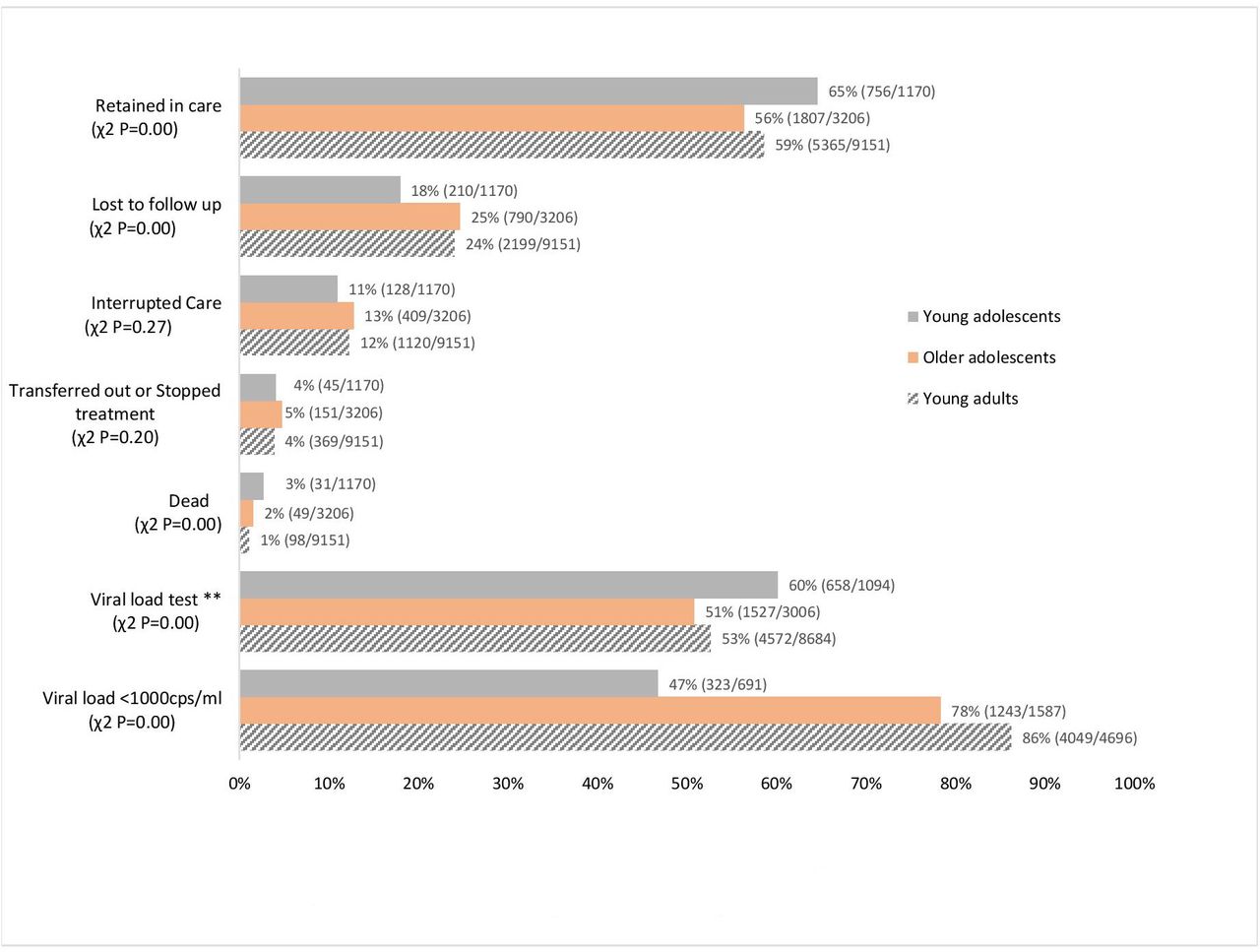
Continuity of care and viral outcomes by age groups. **Excludes adolescents and youths living with HIV (AYLHIV) who were dead, transferred out or stopped treatment.
After excluding AYLHIV who died, transferred out or stopped treatment, the overall proportion of AYLHIV who had VL testing was higher among young adolescents when compared with older adolescents and young adults (60% vs 51% and 53%; χ2 p=0.00). Of AYLHIV who had VL testing, younger adolescents had the lowest proportion with viral suppression (VL less than 1000 copies/mL) compared with older adolescents and young adults (47% vs 78% and 86%; χ2 p=0.00) (figure 1).
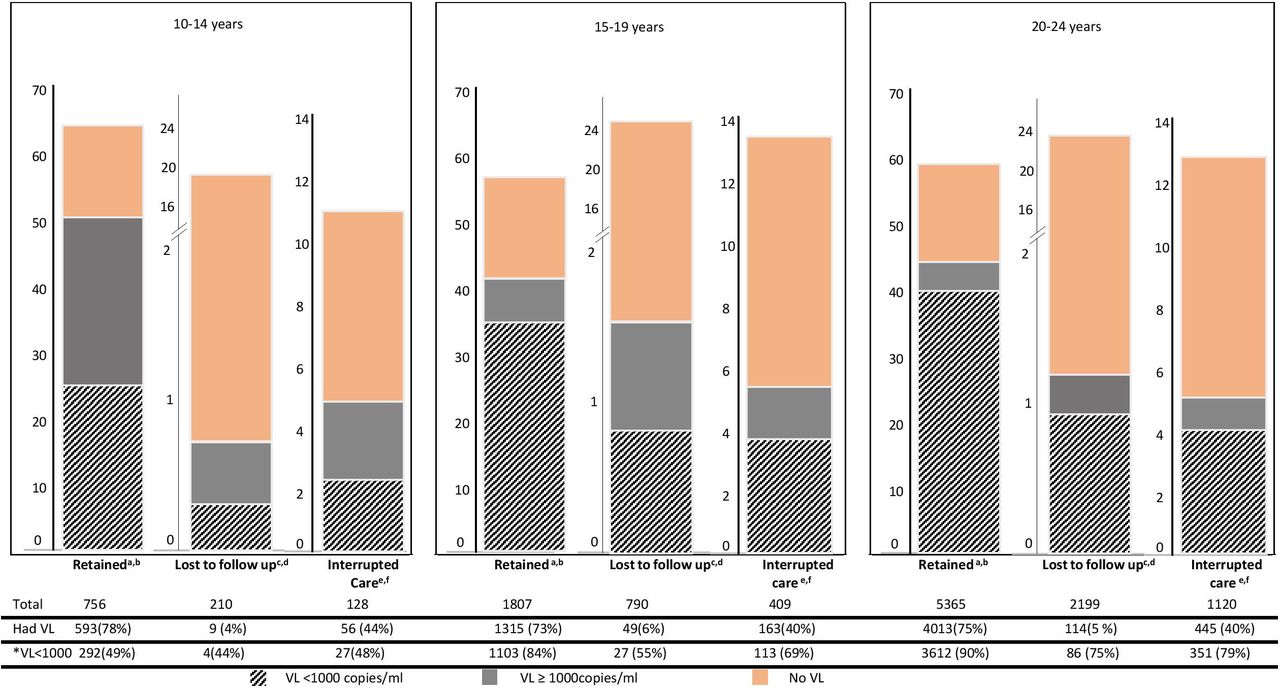
Figure 2 shows a further breakdown of VL testing and viral suppression by age groups and continuity of care. Among all the AYLHIV who were retained in care, the proportion who had VL testing was highest among young adolescents (78%) compared with older adolescents and young adults (73% and 75%; χ2 p=0.01). Among all retained AYLHIV who had VL testing, the proportion that achieved viral suppression was lowest among young adolescents (49%) compared with older adolescents and young adults (84% and 90%; χ2 p=0.00) (figure 2).

{kind=link}
{kind=link}
Breakdown of viral outcomes by adolescents and youths living with HIV (AYLHIV) age group and continuity of care. aχ2 p value=0.01; proportion of retained AYLHIV who had viral load (VL) test across all three age groups. bχ2 p value=0.00; proportion of retained AYLHIV with VL<1000 across all three age groups. cχ2 p value=0.42; proportion of LTF AYLHIV who had VL test across all three age groups. dχ2 p value=0.01; proportion of LTF AYLHIV with VL<1000 across all three age groups. eχ2 p value=0.00; proportion of interrupted care AYLHIV who had VL test across all three age groups. fχ2 p value=0.00; proportion of interrupted care AYLHIV with VL<1000 across all three age groups. *Denominator is the number of AYLHIV who had VL test.
Among all the AYLHIV who were LTF, the proportion who had VL testing was similar across the age groups, ranging between 4% and 6% (χ2 p=0.42). Among AYLHIV LTF who had VL testing the proportion that achieved viral suppression was lowest among young adolescents (44%) compared with older adolescents and young adults (55% and 75%; χ2 p=0.01). Among all AYLHIV who interrupted care, the proportion who had VL testing was higher among young adolescents (44%) compared with older adolescents and young adults (40%; χ2 p=0.00). Among AYLHIV with interrupted care who had VL testing the proportion that achieved viral suppression was lowest in young adolescents (48%) compared with older adolescents and young adults (69% and 79%; χ2 p=0.00) (figure 2).
Measures of associations (fixed effects)
Continuity of care
Table 2 shows both fixed effect (measures of association) and random effects (measures of variation) from the multilevel analysis by age group with non-retention (LTF or interrupt care) in care as the outcome.
Multilevel multivariable logistic regression of non-retention in care by age group
Young adolescents
After controlling for both individual and facility characteristics, young adolescents initiated on an ART regimen categorised as ‘Others’ were less likely to be LTF or interrupt care (non-retention), compared with young adolescents initiated on a regimen consisting of ABC or AZT/3TC/ ATVr or LPVr (aOR=0.25; p<0.05). Increasing facility-level VL testing was associated with reduced likelihood of being LTF or interrupting care (non-retention) among young adolescents. For each one-unit increase in health facility VL test, the odds of being LTF or interrupting care (non-retention) in this group decreased by 1% (adjusted OR (aOR)=0.99; p<0.00).
Older adolescents
In this group, non-retention was less likely among those enrolled in 2017 compared with enrollees in 2015 (aOR=0.74; p<0.00); no significant association between retention and any other individual-level factor was observed. At the level of health facility, the likelihood of non-retention in care reduced with increasing VL testing coverage among enrolled AYLHIV. For each one-unit increase in health facility VL test coverage, the odds of non-retention among older adolescents decreased by 7% (aOR=0.93; p<0.00).
Young adults
In this group, the odds of non-retention was higher among males (aOR=1.28; p<0.00) compared with females; the odds for non-retention was lower among those initiated on the ART regimen category ‘Others’ compared with those initiated on regimen ABC or AZT/3TC/ATVr or LPVr (aOR=0.15; p<0.05). At the level of the health facility, the likelihood of non-retention in care reduced with increasing VL testing coverage among enrolled AYLHIV. For each one-unit increase in health facility VL test coverage, the odds of non-retention among young adults decreased by 2% (aOR=0.98; p<0.00).
Viral suppression
Table 3 shows both fixed effect (measures of association) and random effects (measures of variation) from the multilevel analysis by age group with viral suppression as the outcome.
Young adolescents
After controlling for both individual-level and facility-level characteristics, young adolescents who interrupted care were less likely to achieve viral suppression, compared with those retained (aOR=0.4; p<0.00). No facility-level characteristic was significantly associated with viral suppression in the age group.
Multilevel multivariable logistic regression of viral suppression by age group
Older adolescents
The odds for viral suppression was higher among married, compared with single older adolescents (aOR=1.74; p<0.05). Compared with older adolescents with no immune suppression at baseline, those with severe immune suppression at baseline had a reduced likelihood of achieving viral suppression (aOR=0.54; p<0.05). Compared with older adolescents retained in care, the odds for viral suppression was lower among older adolescents who were LTF (aOR=0.19; p<0.00) or who interrupted care (aOR=0.41; p<0.00).
Young adults
Compared with young adults with no immune suppression at baseline, those with severe immune suppression at baseline had a reduced likelihood of achieving viral suppression (aOR=0.55; p<0.00). Young adults initiated on ART regimen TDF/3TC/EFV or NVP had higher odds of achieving viral suppression compared with young adults initiated on ABC or AZT/3TC/ATVr or LPVr (aOR=6.47; p<0.05). Compared with young adults retained in care, the odds for viral suppression was lower among those who were LTF (aOR=0.35; p<0.00) or who interrupted care (aOR=0.42; p<0.00).
Measures of variations (random effects)
Continuity of care
The results of the null models (Model 1) across AYLHIV age groups showed significant variance of 12%–14% in the log-odds of non-retention in care attributed to health facilities (τ=0.47; p<0.00 (young adolescents), τ=0.52; p<0.00 (older adolescents), τ=0.54; p<0.00 (young adults)). The variations at health facility level remained statistically significant even after controlling for individual-level (Model 2) and facility-level characteristics (Model 3), thereby lending support for the use of multilevel modelling to account for variations at the two levels. As judged by the proportional change in variance among young adolescents, 4.26% of the variance in retention across health facilities was explained by individual factors (Model 2) and 22.22% of the variation explained by facility factors (Model 3). For older adolescents, 3.84% of this variance in retention was explained by individual factors alone (Model 2) and 14% explained by facility factors (Model 3). For young adults, none of the variations in retention was explained by individual factors alone (Model 2), while 16.67% was explained by both individual and facility factors (Model 3).
Viral suppression
The results of the null models (Model 1) across AYLHIV age groups show significant variance of 9%–13% in the log-odds of viral suppression attributed to health facilities (τ=0.39; p<0.05 (young adolescents), τ=0.49; p<0.00 (older adolescents), τ=0.34; p<0.00 (young adults)). The variations at the health facility level also remained statistically significant even after controlling for individual-level and facility-level factors. As judged by the proportional change in variance among young adolescents, 2.56% of the variance in viral suppression across health facilities was explained by individual factors alone (Model 2) and 15.79% of the variation explained by facility factors (Model 3). For older adolescents, 10.20% of this variance in viral suppression was explained by individual factors alone (Model 2), while facility factors did not explain any of the variance (Model 3). For young adults, 14.71% of the variation was explained by individual factors alone (Model 2) and 3.45% by facility factors (Model 3).
Multiple group analysis
We detected statistically significant group differences in the association between retention in care and two variables: sex and ART regimen at baseline (table 2).
The association between sex and retention in care differed in magnitude and direction of effects across the age groups, reaching statistical significance only among young adults with male young adults having an increased likelihood of not being retained in care (aOR 1.28, p<0.00).
The association between ART regimen at baseline and retention in care had similar direction but differed in the magnitude of effects across the age groups. Initiation of regimen baseline ‘Others’ was associated with a reduced likelihood of not being retained in care in the three age groups, with effect highest among young adults and lowest among older adolescents.
We did not find any significant group differences in the association between any of the explanatory variables and viral suppression (table 3).
Discussion
In this multilevel and multiple group study, we estimated the relative contributions of individual-level and facility-level determinants to retention in care and viral suppression across AYLHIV age groups. We showed similarities and differences in magnitude and direction of effects across age groups for individual level (age group, sex, ART regimen and pattern of care continuity) and facility-level factors (VL testing coverage) associated with retention in care and viral suppression. We discuss these findings according to the levels of influence.
Individual-level factors
Although we found differences in the magnitude and direction of effects for the individual-level variables, two factors emerged as consistent predictors across age groups: baseline ART regimen and pattern of care continuity.
Similar to other study findings,8 11 12 18 higher proportions (65%) of young adolescents were retained in care compared with older adolescents (56%) and young adults living with HIV (59%). Despite their higher rates of retention, young adolescents had comparatively much lower viral suppression rates (47%) compared with older adolescents (78%) and young adults (86%). Also, while the odds for viral suppression reduced with lower levels of retention in older adolescents and young adults, there was no significant difference in odds for viral suppression among young adolescents retained in care and those who were not. Although these findings seem counterintuitive since better retention in care is expected to lead to higher rates of viral suppression, it corroborates findings from other studies30–36 showing high rates of viral non-suppression among young adolescents despite perfect adherence, most notably among young adolescents initiated on AZT+3 TC+NVP/EFV. In our study, young adolescents were also initiated predominantly on ART regimen AZT+3 TC+NVP/EFV(63.2%), in contrast to older adolescents and young adults who were initiated predominantly on TDF/3TC/EFV or NVP (83.90% and 90.1%, respectively). We also found that the likelihood of achieving viral suppression irrespective of age groups was highest with initiation on TDF/3TC/EFV or NVP regimen, reaching significance only among AYLHIV.
These findings suggest a rise in regimen-specific disparity in viral outcomes, with increasing rates of viral non-suppression with AZT+3 TC+NVP/EFV regimen use predominantly among young adolescents. When coupled with the relatively higher baseline CD4 level in young adolescents, increased viral non-suppression point to the possibility of pretreatment drug resistance (PDR) arising either from perinatally transmitted drug resistance or acquired through exposure to ARVs during PMTCT.5 8 11 12 This is all the more likely given our speculation that the majority of younger adolescents in our study are perinatally HIV infected compared with older adolescents and younger adults who we assume to be mostly behaviourally infected. Studies from Nigeria37–39 and other African countries38 40 have reported a rapidly increasing prevalence of PDR among both PMTCT exposed (more than 42%) and PMTCT unexposed (up to 35%) children and young adolescents. Although the majority of these PDR are to non-nucleoside reverse transcriptase inhibitors, increasing rates of multiclass PDR involving nucleoside reverse transcriptase inhibitors are also being reported, and this is concerning because of the potential impact on alternative regimen options. The emergence of PDR as a major driver of first-line ARV treatment failure among young adolescents call for increased effort to overcome the practical barriers in expanding the use of Integrase inhibitor-based regimens to optimise treatment for young adolescents in sub-Saharan Africa. Point-of-care resistance tests41 could be implemented to inform decision-making on appropriate regimens for ART initiations, in addition to scale-up of regular VL monitoring for early detection of virological failure.
We observed ART regimen-specific differences on retention in care. Compared with AYLHIV initiated on regimen ABC or AZT/3TC/ ATVr or LPVr, AYLHIV initiated on other regimens were less likely to be LTF or have interrupted care (ie, not retained) in the three age groups. We speculate these differences to be due to drug side effects from ART which studies have shown to be a major barrier to retention and adherence. The current HIV policy climate of ‘test and start’ no longer requires laboratory and clinical assessments as eligibility requirements for ART initiation. In high-burden-limited resource settings, this may lead to an underemphasis on clinical assessment processes including the management of side effects in favour of quicker ART initiations.42 Such underemphasis on clinical management of side effects signifies potentially higher rates of care disengagement among AYLHIV, who in the era of ‘test and treat’ are generally more likely to initiate ART feeling healthy and feel less need for adherence.
We observed a preponderance of female AYLHIV among our cohort with age, suggesting that female adolescents and young adult women represent a behaviourally vulnerable population. This supports previous findings from sub-Saharan Africa countries, where being young, female and less-educated increases the chances for transgenerational HIV transmission.36 Combined with high adolescent fertility rates in Nigeria, poor retention and low viral suppression rates among older adolescents and young adults in our study might undermine ongoing efforts at eliminating HIV mother-to-child transmission. However, we also found other gender-specific disparities within our cohort in which male young adult living with HIVs had a higher likelihood of interrupting care or being LTF, and male older adolescent living with HIV being less likely to achieve viral suppression.
Our findings on sex differences suggest the need to factor in gender considerations as services become increasingly differentiated for AYLHIV. Studies have shown promising practices among the different approaches targeting men/male for improved HIV testing, prevention, treatment, care and support services.43–53
Health facility-level factors
We found significant variation in outcomes attributable to differences at the health facility level. The variations across facilities remained statistically significant, even after controlling for individual-level and facility-level factors (Models 2 and 3).
Although compared with individual-level factors facility-level characteristics accounted for a higher proportion of the total variance observed, the magnitude of this facility-level contribution to variance (ie, facility effects) differed between AYLHIV age groups. For retention in care, higher increases due to facility effects were observed among young adolescents and young adults than among older adolescents. For viral suppression, there was no change in variance from facility effect, only a modest increase among young adults and a much higher increase in young adolescents. These differences suggest that interventions at the level of health services may be less effective than those targeting individual-level determinants for improving viral outcomes among older adolescents. This supports other studies showing that adolescent-focused health services interventions, though desirable, are not uniformly effective across all adolescent age groups.54
We found that an increase in facility-level VL testing reduced the likelihood of being LTF or interrupting care (non-retention) among AYLHIV. This suggests that facility-level differences in access to disease monitoring laboratory services (eg, CD4 or VL) might be important for how AYLHIV engage with care. Studies have shown that inability to access such services often triggers disengagement with care.55–57 Scale-up of routine VL testing is therefore necessary not only to allow providers make informed decisions on clinical management but also to encourage and sustain optimal engagement with care among AYLHIV.58
Study limitations
Our findings should be interpreted in light of some important limitations. Although we imputed for missing information to minimise bias, the possibility of non-differential errors cannot be ruled out. Due to differences in the age-group cohort sizes, there was greater power to detect covariate effect sizes among older adolescents and young adults age groups, compared with young adolescents. Although case finding was conducted for those AYLHIV who were not retained in care, the percentage of these patients who returned to clinical care and had VL assessment was low and may not be representative of their respective categories. We also lacked information to categorise our adolescent cohort by modes of transmission (perinatal vs behavioural infected). Despite our use of multiple imputations to address missing data, we still cannot completely rule out some bias in our estimates given that health facilities with more missing data may also be the ones with poorer outcomes on the aggregate. Lastly, our study was carried out within the context of healthcare facilities receiving PEPFAR support. Findings may therefore not be generalisable to other AYLHIV receiving care at health facilities not supported by PEPFAR who may differ in patient outcomes. Despite attempting to delineate the different levels of effects in our multilevel modelling, our study still did not fully account for variations in outcomes at facility levels. This unobserved heterogeneity suggests the existence of other important explanatory factors that were not measured in our study.
Conclusions
Our study supports our hypothesis that important differences exist in health service conditions between healthcare facilities that can explain variations in treatment outcomes among AYLHIV. We also demonstrate key individual (ART regimen, baseline immune suppression, sex) and facility-level factors (facility-level VL testing) that may serve as entry points for both broad-based and targeted interventions to improve outcomes among AYLHIV. Despite limited data to explore the whole range of factors at individual and service delivery levels potentially affecting treatment continuity and VL suppression, we demonstrate a need to better understand and unpack these potentially modifiable factors at the individual and facility levels to design interventions that ensure equity of among all AYLHIV groups and ensure that no one is left behind.
Acknowledgments
The authors thank Professor Anne Buve for her review and useful comments The authors also acknowledge enabling support from APIN management during the conduct of this study, and thank programme managers and health workers who provide services to people living with HIV. Finally, we thank all the patients (adolescents and youths living with HIV) and their advisers/caregivers whose consent to having their information used for research purposes has made this study possible.
References
Footnotes
Handling editor Sanni Yaya
Twitter @badejokikiolu
Contributors OB conceived the study, conducted the analysis and wrote all drafts of the manuscript. All authors provided critical reviews of the drafts. All authors read and approved of the final draft.
Funding The data on which this study is based are from a project funded by the US Presidents Emergency Plan for AIDS (PEPFAR), awarded through the Centre for Disease Control. OB received doctoral research funding from the Belgium Directorate-General for Development Cooperation (DGD) awarded through the Institute of Tropical Medicine Antwerp, Belgium.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Ethical approval for this study was obtained from the IRBs of APIN and the Institute of Tropical Medicine, Antwerp.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available. Data not publicly available but may be obtained upon request and approval from APIN-PEPFAR clinical data repository.