Article Text

Abstract
Introduction The rising burden of drug resistance is a major challenge to the global fight against malaria. We estimated national Plasmodium falciparum resistance to sulfadoxine-pyrimethamine (SP) across Africa, from 2000 to 2020.
Methods We assembled molecular, clinical and endemicity data covering malaria-endemic African countries up to December 2018. Subsequently, we reconstructed georeferenced patient data, using pfdhps540E and pfdhps581G to measure mid-level and high-level SP resistance. Gaussian process regression was applied to model spatiotemporal standardised prevalence.
Results In eastern Africa, mid-level SP resistance increased by 64.0% (95% uncertainty interval, 30.7%–69.8%) in Tanzania, 55.4% (31.3%–65.2%) in Sudan, 45.7% (16.8%–54.3%) in Mozambique, 29.7% (10.0%–45.2%) in Kenya and 8.7% (1.4%–36.8%) in Malawi from 2000 to 2010. This was followed by a steady decline of 76.0% (39.6%–92.6%) in Sudan, 65.7% (25.5%–85.6%) in Kenya and 17.4% (2.6%–37.5%) in Tanzania from 2010 to 2020. In central Africa, the levels increased by 28.9% (7.2%–62.5%) in Equatorial Guinea and 85.3% (54.0%–95.9%) in the Congo from 2000 to 2020, while in the other countries remained largely unchanged. In western Africa, the levels have remained low from 2000 to 2020, except for Nigeria, with a reduction of 14.4% (0.7%–67.5%) and Mali, with an increase of 7.0% (0.8%–25.6%). High-level SP resistance increased by 5.5% (1.0%–20.0%) in Malawi, 4.7% (0.5%–25.4%) in Kenya and 2.0% (0.1%–39.2%) in Tanzania, from 2000 to 2020.
Conclusion Under the WHO protocols, SP is no longer effective for intermittent preventive treatment in pregnancy and infancy in most of eastern Africa and parts of central Africa. Strengthening health systems capacity to monitor drug resistance at subnational levels across the endemicity spectrum is critical to achieve the global target to end the epidemic.
- health policy
- malaria
- epidemiology
- maternal health
- child health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
In the period from 2000 until 2015, malaria burden reduced substantially in Africa.
The annual incidence, prevalence, deaths and disability-adjusted life years were reduced by 40%, 50%, 57% and 24%, respectively.
However, the disease remains a major cause of morbidity and mortality throughout the continent, with more recent evidence indicating an increase in the number of cases.
The WHO recommends countries to withdraw intermittent preventive treatment in pregnancy when the prevalence of pfdhps540E >95% and pfdhps581G >10%, and intermittent preventive treatment in infancy when the prevalence of pfdhps540E >50%.
Comparable evidence on anti-malarial drug resistance, applicable to the general population at national level, that can reliably inform the translation of WHO recommendations into effective national policies, is currently limited.
Key questions
What are the new findings?
This is the first systematic analysis of nationwide standardised levels of Plasmodium falciparum resistance to sulfadoxine-pyrimethamine (SP).
The evidence provided here allows comparability of trends across time and locations and helps policymakers understand the policy impact of the WHO frameworks at country level.
Our metrics illustrate a gradual reduction of mid-level resistance to SP in eastern Africa since 2010, as well as increasing levels in central Africa and a largely stable drug efficacy in western and southern Africa in the period between 2000 and 2020.
However, there is a continued reduction of drug efficacy on the continent, driven by increasing levels of high-level resistance, mostly in eastern Africa.
Using our metrics in conjunction with the current WHO protocols, we identified countries where continued implementation of SP-based malaria control policies for maternal and child health outcomes are warranted, as well as regions where these policies are no longer effective.
What do the new findings imply?
We detected areas where a careful monitoring of resistance levels is critical.
We also identified areas with limited coverage of patient data for resistance tracking in the regions where the largest share of P. falciparum infection is concentrated.
This includes Nigeria, the Democratic Republic of the Congo, Mozambique and Uganda, which alone account for 45% of the global burden of malaria cases.
Therefore, to realise the global agenda to end the epidemic of malaria by 2030 in the context of the Sustainable Development Goals target 3.3, it is essential to strengthen health systems capacity to monitor resistance at subnational level across the endemicity spectrum on the continent.
Background
Malaria remains a major cause of morbidity and mortality in Africa. Annually, Plasmodium falciparum infection causes more than 200 million clinical cases and over 400 000 attributable deaths on the continent, which accounts for 92% of the global malaria burden.1 In the period from 2000 to 2015, malaria burden reduced substantially in part due to a reinvigorated multilateral commitment to, and a 20-fold increase in international investment in, malaria control. The annual incidence, prevalence, deaths and disability-adjusted life years were reduced by 40%, 50%, 57% and 24%, respectively.2–4 Despite the declining trends through 2015, more recent estimates show that if the current increases in malaria cases and deaths continue, then the Sustainable Development Goals (SDG) target 3.3—ending the epidemic of malaria by 2030—might not be achieved.1 5
The rising burden of P. falciparum resistance to essential anti-malarial drugs is a major challenge to the global fight against malaria.1 4 Despite the widely reported resistance to sulfadoxine-pyrimethamine (SP), it is still the drug of choice for intermittent preventive treatment in both pregnancy (IPTp) and infancy (IPTi). SP, combined with chloroquine (CQ) or artesunate (AS), was used as treatment in much of Africa, although most countries changed to artemisinin-based combination therapy (ACT) between 2003 and 2008.6 This change in usage reduced selection for antifolate resistance and may have allowed for changes in the prevalence of markers of resistance. Two countries, Somalia and Sudan, continued to use AS+SP until 2016 and 2017, respectively.7–9 This change further reduced the selective pressure on antifolates. In Sudan, the adoption of AS+SP in 2004 as the first-line ACT was based on an open-label randomised controlled trial conducted in the country the same year that indicated superiority of AS+SP compared with SP for the treatment of uncomplicated malaria, which was confirmed by subsequent trials.7 10 11 Likewise, in Somalia, AS+SP was adopted in 2006 as the first-line ACT based on therapeutic efficacy studies conducted between 2003 and 2006 that indicated high therapeutic efficacy of this drug (as well as AS+amodiaquine (AQ)) compared with CQ, AQ and SP in the country.12
The WHO recommends member states to closely monitor the efficacy of essential anti-malarial drugs and use resistance levels to inform policymaking at the country-level.13–15 However, most malaria-endemic countries do not have the capacity to establish the needed networks of well-functioning resistance surveillance sites across their epidemiologically diverse territories to track resistance. To date, data on molecular markers measured in clinical samples have been used to infer country scale levels of drug-resistant P. falciparum. These molecular markers indicate mutations in the genes for two enzymes of the folate pathway, dihydropteroate synthase (DHPS) (mutations: 437G, 540E, 581G) and dihydrofolate reductase (DHFR) (mutations: 51I, 59R, 108N), which have been associated with resistance to S and P, respectively. The intensity of the resistance to SP increases with the number and types of mutant codons, with quintuple mutations (five mutations including 540E, excluding 581G) being associated with mid-level resistance, and sextuple mutations (six mutations including 581G) with high-level resistance. These can be measured using pfdhps540E and pfdhps581G, respectively. A previous modelling study16 used data on pfdhps540E mutations from 1987 to 2008 to create predictive surfaces on the continent. The study provided maps visualising the variation of the prevalence of pfdhps540E across the continent, and probability distribution for locations without data. However, it covered only the period between 1990 and 2010. Therefore, the estimates provided do not reflect recent variations in SP resistance following the changes in anti-malarial policies.1 6 Additionally, the models used in the study16 did not account for real world data including clinical characteristics of patients, as well as population level anti-malarial immunity, which is a function of age and endemicity.17–20 A more recent meta-analysis21 used pfdhps540E and pfdhps581G to measure the association between resistance and low birth weight (LBW). This did not provide country-specific adjusted estimates of prevalence levels, nor did it quantify the potential policy implications of mutation levels. Thus, no evidence is available to date on age-endemicity standardised prevalence of malaria resistance to SP, or its implication for anti-malarial policy. This complicates comparability of resistance trends across the continent and global efforts to tackle the burden of drug resistance.
We provide a comprehensive analysis that leverages data systematically derived from clinical records and community surveys conducted across the continent, over the last two decades. We employ recent advances in infectious disease modelling to generate comparable tempo-spatial trends and projections of P. falciparum resistance to SP and drug effectiveness for IPTp and IPTi policies at the national level from 2000 to 2020.
Methods
Study setting and data sources
We assembled molecular, clinical and endemicity data derived from multiple sources covering malaria-endemic African countries from January 1998 to December 2018. For data on pfdhps540E and pfdhps581G mutations associated with SP resistance, as well as national anti-malarial treatment policy implementations, we conducted an extensive search of medical databases detailed in online supplemental files 1.1–1.2. We cross-validated our molecular data with Worldwide Antimicrobial Resistance Network (WWARN) databases. WWARN repository does not have clinical and endemicity data. We contacted the authors of the eligible trials and experts for clarification and/or additional molecular and/or clinical data (online supplemental file 1.1). For data on anti-malarial treatment policy implementations, we additionally consulted National Malaria Control Programs (NMCP), African Malaria Reports (AMR) and World Malaria Reports (WMR). From each eligible survey, the number of patients enrolled, clinical samples successfully genotyped and positive for each of the molecular markers under study, as well as demographic and clinical characteristics of patients tested, study design, geospatial coordinates, clinical context and year, as well as season of sample collection, were extracted. From NMCP, AMR, WMR and articles eligible for anti-malarial policy data, we extracted data on anti-malarial drug combination adopted and the year when policy implementation began (online supplemental file 1.4).
Supplemental material
Subsequently, we geolocated data on resistance markers from the eligible surveys and then linked with malaria endemicity data from the Malaria Atlas Project by matching sampling site and year that the clinical samples were collected.4 We further derived data on Socio-demographic Index (SDI) from the Global Burden of Disease Study 201722 and HIV prevalence data from the Joint United Nations Programme on HIV/AIDS databases, matching them to each P. falciparum resistance survey datapoint using geolocation and year of sample collection. Finally, we used the resulting pool of evidence to reconstruct georeferenced patient data across space-time clusters. The current analysis was conducted within the context of a study exploring trends in comparative efficacy and safety of malaria control interventions for maternal and child health outcomes in Africa, which has been registered on PROSPERO under CRD42018095138.23 The primary purpose of this current analysis is to provide country level data on the prevalence of P. falciparum resistance to SP. This study complies with the Guidelines for Accurate and Transparent Health Estimates Reporting statement24 (online supplemental files 1.1–3.6).
Data processing and modelling framework
We use pfdhps540E and pfdhps581G mutations validated to measure mid-level and high-level P. falciparum resistance to SP, respectively13–15 (see online supplemental files 1.6–1.8 for marker groupings and diagnostic accuracy). We included a variable denoting the proportion of mixed genotype infections as a covariate in our model (online supplemental file 1.5). We also incorporated SDI in our modelling framework to account for lag distributed income per capita, educational attainment for those aged ≥15 and total fertility rate among women aged <25 years in our estimates.22 These are known to influence anti-malarial treatment-seeking behaviour in malaria-endemic countries.25 The inclusion of HIV prevalence in the dataset aimed to account for any potential effect of trimethoprim-sulfamethoxazole (TMP-SMX), which is used to prevent opportunistic infections among HIV-infected patients. TMP-SMX targets the same folate pathway as SP (trimethoprim: DHFR; sulfamethoxazole: DHPS), although clinical evidence on cross-resistance is still limited.26 27 We used Bayesian principal component analysis to identify the principal subspace of the observed age data. This showed that four and three latent variables capture the most important variability in the age of the patients from whom the blood samples genotyped for pfdhps540E and pfdhps581G were collected, respectively (online supplemental file 2.2). These latent variables for patient age along with the other covariates including malaria endemicity, were then incorporated in the modelling framework, for each marker. These covariates were evaluated by Bayesian additive regression trees to compute generalised propensity scores. This allowed us to effectively summarise and balance the covariate information, while accounting appropriately for non-linearities and interactions, thereby standardising our quantities. Our approach allows effective redundancy reduction and stability optimisation by keeping only the best covariates. This helps achieve a parsimonious model and avoid overfitting (online supplemental file 2.3).
Gaussian process regression (GPR) model was subsequently applied to compute country-level adjusted prevalence of, and temporal change in, malaria resistance to SP, spanning the period from 2000 through the end of 2020. We used inverse logit function to map our estimates from the real space into the probability space. The year of sample collection is used as predictor and the administrative level one corresponding to the sampling site as a random effects variable. We employ predictive comparisons to derive temporal change in resistance quantities. Finally, we computed the posterior probability to quantify the amount of evidence in favour of IPTp and IPTi being effective in each country under the current WHO thresholds,13–15 given the estimated levels of P. falciparum resistance to SP. For IPTp, the WHO thresholds for withdrawal of policy is when pfdhps540E >95% and pfdhps581G >10%. For IPTi, the WHO thresholds for withdrawal of policy is pfdhps540E >50%. For countries with limited data on pfdhps581G, we use regional trends of high-level resistance to compute the posterior probability of IPTp effectiveness. GPR is a high-level non-parametric probabilistic method with demonstrated prediction accuracy, reliable quantification of uncertainty, and ability to recover an underlying dynamic process from noisy observations in the face of data sparsity and non-linear problems, with minimal assumptions28 (online supplemental file 2.4). We developed our GPR model in Stan V.2.19.1 and implemented it in R V.3.5.1.
Sensitivity analysis and uncertainty quantification
We conducted out-of-sample cross-validation to check the performance of our model. This showed that the model was reasonably well calibrated, which was confirmed by Markov chain Monte Carlo diagnostics (online supplemental files 2.4 and 3.3). We also assessed the robustness of our empirical estimates to sensible changes in model specification. The results were relatively stable, confirming that the predicted resistance quantities are not artefacts of our modelling assumptions. Previous studies16 29 30 were used to draw our prior hypothesis in resistance patterns per region across the continent. This informed our hyperparameters’ priors pool, from which we selected the best performing sets for each country. A detailed account of the method is provided in the appendix (online supplemental files 1.1–2.5).
Results
We identified a total of 703 unique records, of which 392 were found to be eligible for full-text eligibility assessment. Ultimately, 198 and 39 surveys reporting data on validated SP resistance markers and malaria control policy implementations, respectively, were included in the resistance quantities estimation (figure 1). Taking these eligible surveys into account, georeferenced data derived from 68 433 clinical samples successfully genotyped for pfdhps540E and collected between 1998 and 2017 in 38 countries from over 195 189 patients were included in the analysis. For pfdhps581G, georeferenced data derived from 39 916 successfully genotyped clinical samples collected between 1998 and 2016 in 30 countries from over 108 374 patients were included in the analysis (figure 2). The surveys included in the analysis enrolled patients with heterogeneous clinical presentations of P. falciparum infection, spanning all demographic groups and malaria endemicity classes (online supplemental file 1.3).

Evidence gathering flowchart. The full description of the search algorithm and the eligibility criteria considered for each outcome cluster is provided in online supplemental files 1.1–1.2.
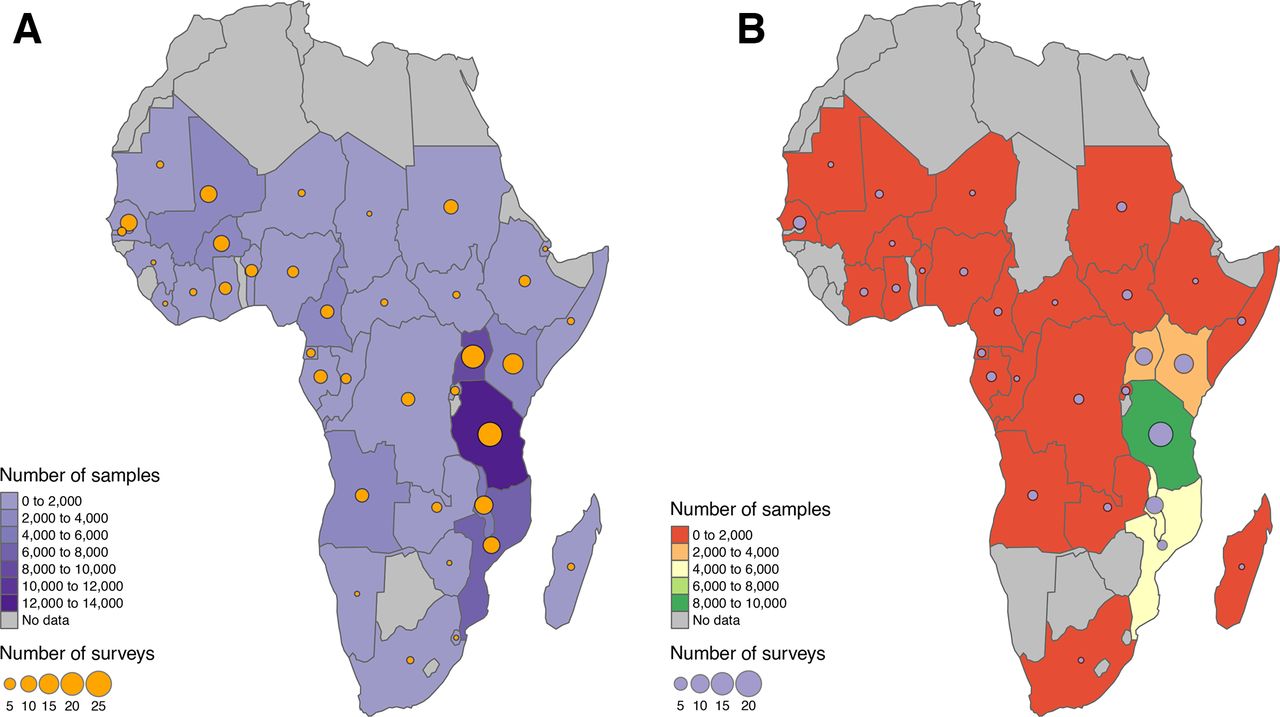
Patient data coverage. The circle sizes are proportional to the number of surveys reporting patient data in each country. The shading depicts the number of clinical samples tested in each country. The intervals are left-opened and right-closed. (A) pfdhps540E patient data. (B) pfdhps581G patient data.
In the period from 2000 through 2020, the prevalence of P.falciparum resistance to SP rose in most malaria-endemic countries in Africa (figure 3). The largest variations in SP-resistant malaria were observed in eastern Africa, where despite important cross-country heterogeneity, mid-level resistance rose until 2010, dominated by Sudan with a net increase of 55.4% (95% uncertainty interval, 31.3%–65.2%), Kenya with 29.7% (10.0%–45.2%), Tanzania with 64.0% (30.7%–69.8%), Mozambique with 45.7% (16.8%–54.3%) and Malawi with 8.7% (1.4%–36.8%). Subsequent to 2010, mid-level resistance takes a downward trajectory as highlighted by a decline of 76.0% (−92.6% to –39.6%) in Sudan, 17.4% (−37.5% to –2.6%) in Tanzania and 65.7% (−85.6% to –25.5%) in Kenya. In Malawi, Ethiopia and Zambia, mid-level resistance to SP is estimated to remain largely unchanged until 2020. Malawi, however, is projected to have the highest levels of resistance among these countries at 100.0% (99.6%–100.0%). In central Africa, our evidence highlights two distinct patterns, with mid-level resistance showing a net increase of 28.9% (7.2%–62.5%) in Equatorial Guinea and 85.3% (54.0%–95.9%) in the Congo from 2000 to 2020, while remaining relatively unchanged in Angola, Cameroon and the Democratic Republic of the Congo. Apart from Nigeria, whose mid-level resistance levels decreased by 14.4% (−67.5% to –0.7%), and Mali, where the levels increased by 7.0% (0.8%–25.6%), in western Africa P. falciparum has remained highly sensitive to SP over the last two decades. High-level resistance to SP has remained largely unchanged in western Africa, most of central Africa and parts of eastern Africa. However, the levels increased by 5.5% (1.0%–20.0%) in Malawi, 4.7% (0.5%–25.4%) in Kenya and 2.0% (0.1%–39.2%) in Tanzania in eastern Africa, and declined by 99.9% (−100.0% to –99.7%) in Equatorial Guinea in central Africa, from 2000 to 2020 (table 1).

{kind=link}
{kind=link}
{kind=link}
National scale temporal trends in, and projections of, Plasmodium falciparum resistance to sulfadoxine-pyrimethamine. The upper and lower lines denote upper and lower bounds of the 95% uncertainty interval, respectively, and the middle, the median of the posterior distribution. The estimates are population-level resistance levels per respective geography. The points and vertical bars indicate point estimates from each survey with respective uncertainty interval, whereas the colours denote the administrative level one of the sites where the patients were recruited, and clinical samples collected. National trends and projections are shown as graphs for selected countries. Countries with the smallest, largest and/or typical changes in resistance in each region (eastern, central and western Africa) are shown, to illustrate the regional trends and cross-country heterogeneity across the continent. Figures for all countries analysed are provided in online supplemental file 3.4. The full list of site-years is summarised in online supplemental file 1.3. Posterior probability distribution of prevalence per survey is given in online supplemental file 3.5. (A) Mid-level P. falciparum resistance to sulfadoxine-pyrimethamine. (B) High-level P. falciparum resistance to sulfadoxine-pyrimethamine.
Estimated change over time per geography in adjusted prevalence of Plasmodium falciparum resistance to sulfadoxine-pyrimethamine, with 95% uncertainty interval
In table 2 we provide the posterior probability that IPTp and IPTi with SP are effective in each country-year under the current WHO thresholds for eligibility of the drug for interventions for maternal and child health outcomes. The posterior probability value reflects the amount of evidence that each intervention is effective under the current WHO frameworks, given the observed levels of mid-level and high-level resistance. We consider the drug effective when the posterior probability >95%. This probability threshold means that the drug is considered effective when the strength of evidence in favour of it being effective is >95%, compared to the alternative hypothesis of it not being effective. For IPTp, the WHO thresholds for withdrawal of policy are pfdhps540E >95% and pfdhps581G >10%. For IPTi, the WHO threshold for withdrawal of policy is pfdhps540E >50%.
Effectiveness of sulfadoxine-pyrimethamine for intermittent preventive treatment in pregnancy (IPTp) and in infancy (IPTi)
This measure shows that in 2000, 14 (63.6%) and 13 (59.1%) countries were fully eligible for IPTp and IPTi, respectively. For IPTp, these countries included Angola, Benin, Burkina Faso, Cameroon, Congo, Democratic Republic of the Congo, Gabon, Ghana, Kenya, Mali, Mozambique, Senegal, Tanzania and The Gambia. For IPTi, the countries eligible in 2000 were Angola, Benin, Burkina Faso, Cameroon, Congo, Equatorial Guinea, Gabon, Ghana, Mali, Senegal, South Africa, Sudan and The Gambia. In 2010, drug effectiveness for IPTp reduced notably in Angola, Benin, Cameroon, Congo, Democratic Republic of the Congo, Kenya and Tanzania. In Equatorial Guinea, SP was not effective for IPTp in the period from 2000 until 2010, due to high levels of high-level resistance. Subsequent to 2010, there is a continued reduction in drug effectiveness for IPTp in most of the continent; however, there is a recovery of drug effectiveness in Equatorial Guinea as a result of decline in high-level resistance in the country. As a result, in total only 7 (31.8%) countries are projected to exhibit full eligibility for IPTp in 2020. These include Burkina Faso, Equatorial Guinea, Gabon, Ghana, Mali, Senegal and The Gambia. In relation to IPTi, 11 (50.0%) countries are projected to remain fully eligible on the continent in 2020. These include Angola, Benin, Burkina Faso, Cameroon, Gabon, Ghana, Mali, Nigeria, Senegal, Sudan and The Gambia. For South Africa, no regional and national data on high-level resistance is available. Therefore, drug effectiveness for IPTp was not computed for this country.
Discussion
This is the first systematic analysis of national trends of standardised levels of P. falciparum resistance to SP. This is an essential drug used as prophylactic combination for maternal (IPTp) and child (IPTi) health outcomes in malaria-endemic countries. The WMR 2019 indicated that approximately 11 million pregnant women would have been exposed to malaria infection and 24 million children were infected with P. falciparum on the continent in 2018.1 Controlled clinical trials have shown that a reduction of 38% (22%–50%) (data: 3 trials), 73% (56%–83%) (6 trials), 43% (28%–54%) (6 trials) and 27% (1%–47%) (3 trials) in the risk of severe antenatal anaemia, antenatal parasitaemia, LBW and perinatal death, respectively, is attainable with effective control of malaria in pregnancy.31 For IPTp, the WHO recommends at least three doses of SP to all pregnant women during antenatal care in the second trimester, each dose given at least a month apart.32 Based on the negative association between SP resistance and birth outcomes reported in meta-analyses and trials that explored the variation of the protective efficacy of SP across resistance levels and types, countries are recommended to withdraw IPTp with SP based on the levels of both mid-level and high-level resistance to SP.14 The WHO thresholds of >95% pfdhps540E and >10% pfdhps581G for IPTp used in the current analysis jointly reflects the fact that on the one hand SP retains a small protective efficacy when mid-level resistance levels are high (protection against LBW when pfdhps540E >90% but pfdhps581G <10%: relative risk reduction: 10% (7%–12%) (13 trials)), and on the other hand the drug is not efficacious to avert adverse birth outcomes even with relatively low levels of high-level resistance (protection against LBW when pfdhps581G >10%: relative risk reduction: 0.5% (−16% to 14%) (13 trials); OR: 1.0 (0.7–1.3) (9 trials)).21 33 For IPTi, the WHO recommends treatment with SP given three times during the first year of life at 10 weeks, 14 weeks and 9 months of age through immunisation services, in areas with <50% pfdhps540E.15 This treatment, which is contraindicated in HIV-infected infants receiving prophylactic TMP-SMX, has been associated with a protective effect against clinical malaria, anaemia, hospital admissions associated with parasitaemia and all-cause hospital admissions in infants of 30.3% (19.8%–39.4%) (6 trials), 21.3% (8.3%–32.5%) (6 trials), 38.1% (12.5%–56.2%) (6 trials) and 22.9% (10.0%–34.0%) (6 trials), respectively.13 However, SP resistance is not measured routinely across all subnational sites, so evidence to inform national level malaria control policy is usually unavailable in many countries. Therefore, our resistance quantities based on a rigorous analysis and two decades of data are paramount for timely and evidence-based translation of the WHO frameworks for decision-making at the country level. These estimates, for the first time, help identify countries where the current evidence on the dynamics of P. falciparum resistance to SP supports, as well as areas where there is no evidence to support the effectiveness of continued use of SP as IPTp and/or IPTi. These quantities may also be important in flagging areas that require additional surveillance.
Our metrics illustrate a gradual decline of mid-level resistance to SP in eastern Africa since 2010, as well as increasing levels in central Africa and largely unchanged levels in western Africa in the period between 2000 and 2020. However, there is a continued decline of drug efficacy in most of the continent, driven by increasing and/or relatively high prevalence of high-level resistance, mostly in eastern Africa. This finding is important because more recent WHO reports have neglected the implications of levels and temporal trends in sextuple mutations when making policy recommendations.32 34 Overall, under the WHO thresholds for drug eligibility for IPTp and IPTi,13–15 the national level metrics provided here indicate that SP is no longer effective for IPTp in eastern Africa and most of central Africa, and for IPTi in most of eastern Africa and parts of central Africa.
The reversal of trends in mid-level resistance observed since 2010 in eastern Africa might be because from 2003 through 2008 many countries in the region began adopting ACT as the first line for the treatment of uncomplicated malaria for the general population. Consequently, countries stopped using SP for curative treatment (as SP, CQ+SP or AQ+SP), but started or continued using SP for prophylactic treatment.1 The period that countries initiated using SP varies across countries, from 1993 to 2007 (online supplemental file 1.4). Those countries that started using SP sooner and/or that delayed withdrawing the drug as part of combinations for curative treatment tend to experience sustained increases in mid-level resistance levels. For instance, Malawi was the first African country to replace CQ with SP in 1993, and among the last to continue using SP as the first-line policy for malaria treatment, until 2007.6 Additionally, SP might continue to be used without prescription for malaria treatment (by populations other than pregnant women (IPTp) or infants (IPTi)) even after it stops being the official first-line treatment in the country. The prevalence of antimicrobial self-medication is high across Africa, despite heterogeneity across countries and sociodemographic groups.35 Illicit sale of drugs, including those that are no longer officially indicated for certain populations and/or conditions, has been documented as an important contributor.36 Nevertheless, taken together, the trends in mid-level and high-level resistance in eastern Africa suggest that accumulation of pfdhps581G mutation in the population is a function of a relatively longer exposure to drug pressure, compared to pfdhps540E mutation (online supplemental file 3.2).
Our in-depth analysis on the effectiveness of SP for IPTp and IPTi for each country-year is valuable in the context of the current debate20 21 33 37–43 on whether the drug should continue to be used in areas of high resistance. A recent meta-analysis indicated that IPTp with SP is associated with improved birth outcomes even when pfdhps540E >90% but not when pfdhps581G >10%.21 However, this meta-analysis did not provide year-specific country-level data either on mid-level and high-level resistance or on the effectiveness IPTp and IPTi policies. Nevertheless, SP resistance changes across space-time both subnationally and across countries as demonstrated here. Additionally, SP-based policies are implemented nationally in most countries, and SP resistance is not measured yearly in all subnational administrative level one sites or lower in each country (eg, in all provinces and/or districts). Therefore, the findings from this study21 cannot be translated into national policy across Africa. In our analysis of the effectiveness of SP for IPTp we accounted for both mutations and standardised our quantities at national level. Overall, our evidence for eastern Africa converges with previous assessments that in this region the effectiveness of SP for IPTp and IPTi is limited.20 38–40 42 43 Here we provide a detailed account of the spatial distribution and temporal dynamics at national level of the eligibility of SP for IPTp and IPTi across the continent. The variability across space-time in parasite resistance and its drivers might explain in part the current controversy in relation to the effectiveness of SP for interventions for maternal and child health outcomes in endemic countries. This is because the effect modification by year of sample collection and the geolocation of patients on P. falciparum resistance to SP has not been accounted for in previous assessments of SP effectiveness for IPTp and IPTi.13 21 37
Even though the current analysis is focused on the use of SP for IPTp and IPTi, our evidence is relevant for seasonal malaria chemoprevention (SMC). This is because the drug combination recommended by the WHO for SMC is AQ+SP, which is administrated as intermittent courses of full treatment to children aged 3–59 months in geographies with highly seasonal malaria transmission in the Sahel subregion of Africa, typically during the rainy season (3–4 months), at 1-month intervals (SMC cycle) up to a maximum of four cycles in a year (SMC round).44 SMC, recommended by the WHO in 2012 and previously referred to as intermittent preventive treatment in children, is indicated in areas where therapeutic efficacy of AQ+SP >90% and is contraindicated in locations where IPTi is being implemented and in HIV-infected children receiving prophylactic TMP-SMX.45 Despite important heterogeneity across trials, it has been associated with a significant protection against all-cause mortality (protective efficacy: 57% (24%–76%) (12 trials); mortality rate ratio: 0.4 (0.2–0.9) (1 trial); risk ratio: 0.7 (0.3–1.4) (6 trials)), all clinical malaria episodes (rate ratio: 0.3 (0.2–0.4) (6 trials)), severe malaria episodes (rate ratio: 0.3 (0.1–0.8) (2 trials)), all-cause hospital admission (incidence rate ratio: 0.6 (0.4–0.8) (1 trial)), moderate anaemia (OR: 0.3 (0.1–0.7) (1 trial)), moderately severe anaemia (risk ratio: 0.7 (0.6–1.0) (5 trials)) and parasitaemia (OR: 0.4 (0.2–0.6) (1 trial)).46–49 However, even though SP is one of the components of the drug combination recommended for SMC, no study has so far quantified how these protective effects of SMC are modified by pfdhps540E and pfdhps581G mutations. Therefore, no thresholds based on the levels and types of SP resistance markers have been established by the WHO for SMC to inform countries when to withdraw this policy. Nevertheless, given the relatively low levels of mid-level and high-level SP resistance across the Sahel subregion of Africa where SMC is deployed, our evidence indicates that this policy continues being largely effective in the subregion in those sites with low prevalence of parasite resistance to AQ. Trials providing data on the protective effect of SMC with AQ+SP stratified across levels and types of AQ and SP resistance markers are needed for a comprehensive assessment of the effectiveness of this policy.
The current analysis highlights the importance of standardised resistance quantities for effective policymaking. Several studies have linked age of patients with their anti-malarial immunity.19 20 Along with the endemicity, age is known to be an important confounder of the predictive performance and diagnostic accuracy of the molecular markers validated for measuring P. falciparum resistance to SP.17 18 However, surveys conducted across the continent usually provide sparse and inconsistent measures of patient age, thus making generation of reliable and comparable estimates of resistance levels challenging. In an era of declining international funding,5 an inability to account for epidemiological and demographic dynamics, within and across populations and countries, inhibits the ability of the scientific community to provide evidence that can reliably inform the translation of the WHO recommendations into effective national policies. Therefore, national measures to strengthen health systems capacity to generate quality data through improved active surveillance of resistance, particularly high-level resistance, are critical to achieve the global target to end the epidemic.
In our analysis, data availability in southern Africa was limited. South Africa is the only country with data sufficient to generate national trends of mid-level resistance in the region; however, data from Namibia and Eswatini were also fed into the regional model. The eligible datasets used in our analysis indicated that the drug is stable in South Africa for IPTi, but the data are not sufficient to generate evidence on drug effectiveness for IPTp in the region due to unavailability of data on high-level resistance (online supplemental files 1.3, 3.2, 3.5, and 3.6). We also detected areas of limited coverage of patient data in eastern Africa and central Africa. These are also the regions where the largest share of P. falciparum infection is concentrated on the continent.4 Importantly, nationally representative data on molecular markers of malaria resistance are limited in Africa. Therefore, while our modelling framework based on a random effects model and georeferenced covariates known to affect the variability in resistance patterns partially mitigates this issue, the national representativeness of our estimates might be limited in some countries. Most of the country data on resistance molecular markers are from prior to 2010, with some countries having no data on resistance molecular markers beyond 2015. We address this limitation in data availability on resistance molecular markers analytically by leveraging regional temporal trends in parasite resistance in conjunction with subnational dynamics in malaria endemicity to project national trends in resistance quantities across time, provided that the available data points in each country are sufficient to model national trends (online supplemental files 1.2–1.3, also see sensitivity analysis). To ensure quality in our geostatistical analysis we did not conduct extrapolation to infer subnational resistance levels to attain a higher spatial–temporal resolution. Rather, we focus on providing adjusted national averages, whose relevance for nationwide policy regarding SP is our major theoretical justification. Furthermore, given the amount of variability in the prevalence of pfdhps540E and pfdhps581G within each country-year (online supplemental files 3.2 and 3.5), the applicability of the WHO thresholds across the resistance spectrum at subnational level might be limited in some countries. For optimal drug effectiveness, a different set of malaria control policies might be required for each resistance cluster at subnational level. The feasibility of our proposed policy implementation has been demonstrated in Kenya, where IPTp is implemented in 14 of the 47 counties.50 However, evidence-based implementation of this strategy requires predictions of resistance quantities with a higher spatial resolution, which should be the direction of future research. Our survey of current evidence on preventive therapies for malaria indicates that most studies guiding the WHO protocols on IPTp,14 21 33 37 41 which informed our modelling framework, have generally focused on LBW, neglecting other maternal and child adverse outcomes that might be impacted differently by the effect of parasite resistance on SP protective efficacy.20 38–40 42 These outcomes, including fetal anaemia, stillbirth, preterm delivery, perinatal deaths, neonatal anaemia, neonatal deaths, maternal anaemia, maternal deaths and others, should be a priority of future studies. Despite these limitations, our analysis, the first of its scope, provides results of unique practical value for effective policymaking in malaria-endemic countries. Importantly, our metrics and recommendations are directly translatable into actions by informing the formulation and implementation of evidence-based responses at the national level in the face of the public health threat and uncertainty posed by drug-resistant malaria in resource-constrained settings, thus effectively helping African nations achieve the SDG for health.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Alberto L Garcia-Basteiro
Contributors FA conceived of and designed the research, prepared the data, conducted statistical analysis, drafted the manuscript, drafted the supplemental material of the manuscript, discussed the results and contributed to the revision of the final manuscript. BL supported statistical analysis, reviewed the manuscript, supported interpretation and policy contextualisation, and contributed to the revision of the final manuscript. JS supported data preparation, reviewed the manuscript, supported interpretation and policy contextualisation, and contributed to the revision of the final manuscript. AM, MH and KS reviewed the manuscript, supported the interpretation and policy contextualisation, and contributed to the revision of the final manuscript. All authors read and approved the final manuscript.
Funding This study was funded by Ministry of Education, Culture, Sports, Science and Technology of Japan.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon a reasonable request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.