Article Text

Abstract
Background Sub-Saharan African (SSA) countries have the highest worldwide levels of unmet need for modern contraception. This has led to persistently high fertility rates in the region, rates which have had major adverse repercussions on the development potential there. Family planning programmes play a key role in improving the uptake of modern contraception, both by fostering women’s health and by lowering their fertility. Increasing awareness of contraception benefits is a major component of such programmes. Here, we ask whether internet access can bridge the gap between women’s need for modern contraception and women’s uptake of the same.
Methods We use a compendium of data for 125 242 women, aged 15–49, from the Demographic Health Survey, Akamai and International Communication Union data, covering eight SSA countries, for the period 2014–2019. We apply a Two-Stage Least Square model, using as instruments for individual internet exposure the distance to the main server in the country and whether the backbone network in the country has been connected to at least one submarine cable.
Results Internet exposure, measured as women access the internet at least monthly (almost daily), is associated with a positive, 11.4% (95% CI 10.6% to 12.2%) (53.8% (95% CI 13.4% to 94.1%)), increase in modern contraception uptake. Education is an important moderator. Poorly educated women benefit the most from internet exposure.
Discussion Internet exposure appears to have significantly increased the uptake of modern contraception among sub-Saharan women. The poorly educated appear particularly to benefit. There are two mechanisms at play: the internet increases women’s knowledge of contraception; and, in parallel, fosters their empowerment.
- health policy
- maternal health
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
SSA countries have persistently high fertility rates, which in turn have had important negative repercussions for SSA’s development potential.
The main reason behind this issue is that the region also shows the highest worldwide levels of unmet need for modern contraception.
Family planning programmes play a key role in improving the uptake of modern contraception, both by fostering women’s health and by lowering their fertility.
Little is known about the potential implication of internet exposure on bridging the gap between women’s need for modern contraception and their uptake.
What are the new findings?
Our results show that internet exposure facilitates the use of modern contraception uptake and that the effect varies according to a woman’s education, less educated women being those who benefit the most.
Internet access shrinks the educational inequalities in unmet need for modern contraception.
What do the new findings imply?
Our study provides evidence that the internet might be an effective way of delivering family planning, which in turn will contribute to the achievement of Sustainable Development Goals.
Background
SSA has experienced remarkable population growth in the last three decades, rising from 510 million inhabitants in 1990 to 1.08 billion in 2018.1 Forecasts suggest that the upward trend is likely to continue, with numbers expected to double again by 2050.2 However, this growth comes at a price. As population grows, the pressure on the environment and especially on fertile land and potable water grows. This exacerbates poverty and food insecurity in countries that already have problems in these areas.3 The main reason for population growth in SSA is that births outnumber deaths four to one.1 Despite declining fertility rates, births have not kept pace with the decline in mortality. According to the World Bank, the total fertility rate in the region declined from 5.7 births per woman to 4.8 in the period 1990–2017.1 These persistently high rates have had important negative repercussions for SSA’s development potential.4 Policy-makers have acknowledged that a solution to these kinds of threats would be the promotion of family planning programmes, which would, it is argued, alter reproductive and childbearing behaviour.5 The Sustainable Development Goals (SDGs) elevated family planning programmes to a top priority. More specifically, SDG 3.7 sets out that the international community should further “ensure universal access to sexual and reproductive health care services, including for family planning, information and education, and the integration of reproductive health into national strategies and programs”.6
In parallel, SSA is challenged by a persistent and severely limited public health infrastructure, with a matching human resource shortage.7 According to WHO, among the 57 countries under the threshold for ‘critical shortage’ of health workers, 36 of them are in SSA.7 As such, information and communication technologies (ICTs), such as the internet, appear to be an effective, time-saving and cost-effective way of improving population health. The internet provided opportunities for global health promotion by, for example, building a stronger health system.8 As such, policy-makers show an increasing interest in investing in eHealth (the use of ICT for health) and mHealth (the use of a mobile phone infrastructure for health).9 In parallel, SSA, where currently 25% of the total population have access to the internet, is the world’s fastest growing internet access region.10 11 However, little research has been carried out on the impact of internet exposure for family planning or modern contraception use.12 The little evidence, that there is, suggests that internet exposure leads to a better understanding of HIV transmission.8 13
Establishing estimates of a causal nature for the effect of internet exposure on modern contraceptive use is challenging. Internet use is closely related to factors such as wealth,14 psychological traits15 and preferences. These are difficult to fully control for in observational studies and they can, in turn, affect an individual’s socioeconomic status. Thus, bivariate and covariate-adjusted associations between the two might not reflect the true effect the internet has on modern contraception use. In this study, we, therefore, exploit the availability of internet sources which are proxied by: the distance from the main country server and the largest city (distance), and whether the backbone network in the country has been connected to at least one submarine cable (submarines). Those two measures affect the likelihood that a woman accesses the net, but it is unlikely that they would directly affect her modern contraception usage. In other words, both the distance and the presence of submarines are measures of a more exogenous nature compared with women’s actual internet use. In so doing, this paper contributes to the literature analysing the role of digital technologies on achieving SDGs, in several ways. First, we specifically focus on internet access whereas most of the literature has focused on mobile phones. Second, we make an innovative use of the DHS on a large set of countries. This provides more information on contextual factors that may influence contraceptive use. Third, our identification strategy allows us to deal with reverse causality issues that were previously ignored in the literature.
Methods
Data sources
Outcome variables
We linked data on the use of modern contraception and internet exposure for eight SSA countries, namely Benin, Burundi, Guinea, Mali, Nigeria, South Africa, Tanzania and Zimbabwe. Data on modern contraception come from the Demographic Health Survey (DHS).16 The DHS is an ongoing cross-sectional survey, which gathers data from national representative samples of households and women of a fertile age (generally 15–49). Here, we use round seven, where individuals were interviewed between 2015 and 2019. From the DHS, each woman is asked “Between (EVENT) in (MONTH/YEAR) and (EVENT) in (MONTH/YEAR), did you or your partner use any method of contraception? Which method was that?”. The dependent variable represents, therefore, a binary variable which is equal to 1 if the interviewed woman or her partner uses modern contraception, and 0 otherwise. The final sample consists of 125 242 women of 15–49 years of age. Among them, 18.4% reported using modern contraceptives, while 17.7% had an unmet need for modern contraception. The proportions of women using these methods varies among countries; however, 47% and 48.3% of women in, respectively, South Africa and Zimbabwe reported using these methods, but only about 10% of women in Benin, Guinea and Nigeria did so (see online supplemental figure 1).
Supplemental material
Exposure variables
Each woman is also asked about her household internet use, which is measured in the DHS with two questions: “In the past 12 months did you use the internet?”; “If so, how often did you use the internet? Not in the past month/Less than once a week/At least once a week/Almost every day”. On average 86.1% of our sample never access the internet, while among those who are exposed to the internet the lion’s share accesses it daily (8.34%), then weekly (3.84%) and 1.77% access the internet less than once a week. Again, these aggregate figures mask heterogeneity across countries. In fact, the share of women who are exposed to the internet varies from 26.7% in Nigeria to 6% in Burundi (see online supplemental figure 2).
Important variables consistently capture the supply of internet exposure. These data come from Akamai and International Communication Union (ITU).17 18 We use a dummy variable equal to one if the backbone network in the country has been connected to at least one submarine cable. This measure was recently used by Hjort and Poulsen to investigate the impact of fast internet arrival on finding employment.17 The authors highlight how submarine cables increase internet speed and also how they decrease the price of a broadband plan, which, in turn, leads to broader access. Obviously, cables were not randomly allocated but they were, rather, introduced where economic benefits were expected, above and beyond the morphology of the country. Therefore, we also use the distance between the centre of the largest city and the main communication servers for each country. We might expect that a shorter distance from the main server will lead to faster communications, which in turn will lead to a higher probability that citizens can access the internet. However, we might also expect the opposite sign in the association as people close to the main server are centrally located, that is, in wealthier areas. This, in turn, might lead to better chances of accessing more services, including family-planning programmes. We observe both variables in 2014. No data beyond this year were available. Figure 1 describes the sample selection, whereas table 1 presents some descriptive statistics.
Sample selection.
Descriptive statistics (N=125 242)
Patient and public involvement
We use secondary data for the analysis. Therefore, no patient consent was needed.
Statistical analysis
The key exposure variable is individual access to the internet: for our purposes, internet ‘exposure’ and ‘access’ are synonyms. We included in our analysis the following: controls for age in years; educational level (no education/primary/secondary/higher education); whether the woman is working; whether her partner is living in the household; number of living children; place of residence (i.e. urban vs rural); household income (divided into quintiles of distribution for the country of residence). Our analysis proceeds in three steps. First, we estimate the association between internet access and the probability of using modern contraception. We do this with descriptive multivariate ordinary least square (OLS; linear probability) regression model. Second, we estimate the moderator effect of the respondent’s educational attainment. Third, in order to ensure that internet exposure is, indeed, exogenous, we estimate a two-Stage Least Square (2SLS) regression model using two instrumental variables (IVs). For this, exposure to the internet is captured by (1) the question of whether the connection of the backbone network in country has been connected to, at least, one submarine cable; and (2) the distance between the main server and the largest city of the country; adjusting for covariates.
The interpretation of the IV estimates are specific to the subpopulation who complied with their treatment assignment: that is, individuals who increased modern contraception use because of internet access. In the IV regression framework, three assumptions must be satisfied. First, the instrument (submarines and distance (Z)) must have had an effect on women’s exposure (X). This is testable and we found large effects (see column 1 in tables 2 and 3). Second, we assume that exposure to the instruments (Z) affected modern contraception (Y) only through women’s exposure to the internet (X; exclusion restriction); this assumption is highly plausible given that the two instruments we use can directly affect women’s modern contraception use only because it is a proxy of the wealth of the area where she lives. However, we already control for individual wealth and for place of residence. Third, to interpret our results as complier causal effects, we assume that easier internet access will only increase (and not decrease) women’s internet access. We make the so-called monotonicity assumption: an individual had access to the internet previously, when it was uncommon or less accessible, but as soon as it becomes more accessible, she refrained from using it. This seems an unlikely turn of events.
Estimation results using a 2SLS
Robustness checks
We used Stata V.15 for all data management and analysis.
Results
Table 4 presents the estimation results. Column 1 presents the crude bivariate association between the use of modern contraception and internet exposure, whereas column 2 presents the results adjusting for covariates. The association appears to be positive and to increase with frequency. Specifically, one increment in internet exposure increases by 5.37% (95% CI 2.41% to 8.33%) the use of modern contraceptives among women. Next, we adjust for individual observable characteristics such as age, education, employment status, whether she has a partner, her wealth in quintiles of distribution, type of residence (urban vs rural), year and country fixed effects. The results show that the effect is still positive and significant, but its magnitude decreases. Specifically, the estimated coefficient amounts to 1.6% (95% CI 0.75% to 2.54%).
Estimation results
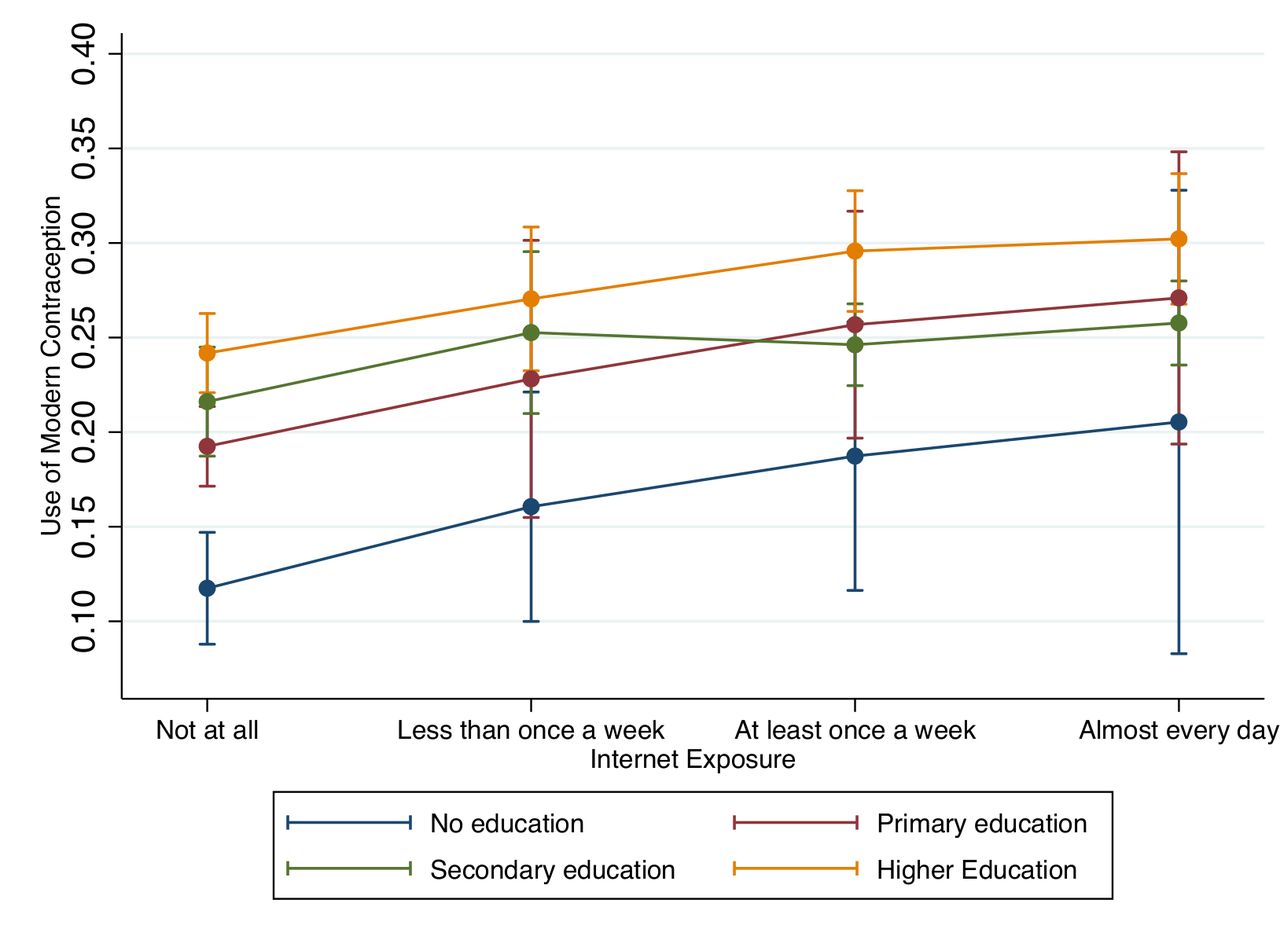
Women’s education has been one of the most thoroughly studied determinants of contraceptive use. There is a positive association between the two. This is true both directly at the individual level through women’s empowerment, which leads to higher financial autonomy and cultural access to reproductive health services, and, also indirectly, through social interaction.19 20 However, little is known of the role played by the internet in this association and particularly the question of whether education can moderate the association between modern contraception and the internet. Figure 2 presents the results graphically by providing a set of predictions. The vertical axis represents the probability of using modern contraception, whereas the horizontal axis represents internet exposure measured at four levels: not at all; less than once a week; at least once a week; almost every day. All the predictions include a 95% CI. Predictions are then made for the non-educated: that is, those women who do not have a primary education (blue line), those with only primary education (red line), those who finished only primary and secondary level education (green line), and those with a college degree or above (yellow line). The figure clearly displays the moderating role of education. As internet exposure becomes more frequent, the educational gap among the groups narrows in terms of contraception use. More specifically, the modern contraception usage of less educated women tends to catch up with the usage of more educated groups. Column 3 in table 4 presents the estimation results.

Moderating role of education in the association between internet exposure and modern contraception use.
Instrumental variable approach
The 2SLS regression models still use individual observations, but the IV is based on the subpopulations living in the same geographical unit. Table 2 presents the estimation results. Column 1 presents the first stage, which tests whether women’s exposure to the internet is correlated with the percentage of population in the same geographical level. Our results show that a 1-mile increase in the distance between the main server and the largest city increases the probability that a woman accesses the internet seems to lead to an increase by about 4% (95% CI 3.61% to 4.42%). In parallel, if the network backbone is connected with at least one submarine cable, it is associated with an increase in the probability that a woman has access to the internet by 5.39% (95% CI 4.17% to 6.61%). Column 2 presents the estimation results of the second stage. We make one caveat. The interpretation is different from the one presented in table 4. The effect estimated here refers to the subpopulation of compliers: that is, those induced to increase their internet exposure because the internet became more accessible; whereas the coefficient estimated in table 4 represents the variation in modern contraception between a woman exposed to the internet and one who is not. As such, the results are not directly comparable. Our results show that an increase in the frequency of internet exposure is likely to increase the probability of using modern contraception by about 11.4% (95% CI 10.6% to 12.2%).
Robustness checks
To gather evidence for the robustness of our results, we applied a series of sensitivity tests to our main statistical models, presented in tables 3, 5 and 6. Specifically, we change our main exposure variable from a modal variable to a dummy one (tables 3 and 5): one if the woman has access to the internet almost daily, and zero otherwise. The idea, here, is to see whether our results are mainly driven by frequent users. Our results are in line with the main ones, even though the magnitude is larger. Column 1 presents the crude bivariate association between modern contraception use and internet exposure, whereas column 2 presents the results adjusting for covariates. The association appears to be positive and to increase with frequency. Our crude bivariate association shows that using the internet almost every day seems to lead to an increment in the probability of using modern contraception by 16% (95% CI 15.1% to 16.9%). Once we adjust for observable characteristics, the effect is still positive and significant but the magnitude is smaller and using internet almost every day appears to lead to an increment in modern contraception use of about 3.9% (95% CI 2.92% to 4.91%). Looking at the moderating role of education in the association between internet exposure and the use of modern contraception, figure 3 confirms our main results. The internet appears to narrow the gap between highly educated women and those with little education. However, unlike our main results, the effect turns out not to be statistically significant, coming in at the 5% level or below.

Moderating role of education in the association between using internet almost every day and modern contraception use.
Robustness checks
Robustness checks
Table 3 below presents the estimation results using a 2SLS estimation strategy, again using the dummy indicating whether a woman has access to the internet almost every day as an exposure variable. The results are in line with the ones presented in table 2 in terms of sign and significance. However, the magnitude is much larger, showing that the ones who become frequent internet users seem to have the largest uptake in terms of modern contraception. More precisely, those women who switch from being an infrequent internet user to using the internet almost daily appear to increase their use of modern contraception by 53.8% (95% CI 13.4% to 94.1%).
Table 6, instead, presents the estimation results using, again, a 2SLS estimation strategy, but rather than using as wealth measure the quintiles of the wealth distribution, we use a series of dummies denoting ownership of physical assets both at individual and at household level. More specifically at individual level, each dummy indicates whether the woman own the house, and/or land, and/or a mobile phone. At household level, each dummy indicates whether in the household there is a car or a truck and/or a fridge and/or a television and/or electricity. The idea behind, here, is to check whether it is actually access to the internet that is driving our results, rather than wealth. In fact, previous evidence suggest that wealth quintiles might not accurately represent the individual’s wealth as it is an aggregate of the wealth at the cluster level,21 rather than a measure that captures the actual individual wealth, which in turn might explain an individual’s access to family planning services. The results are in line with the ones presented in table 2 in terms of sign and significance. More precisely, those women who have access to the internet increase their use of modern contraception by 11% (95% CI 9.48% to 11.7%).
Discussion
We show that internet exposure among sub-Saharan women is associated with an increment in their use of modern contraception. Effects were particularly striking among poorly educated women. This result is in line with previous evidence on the impact on mHealth and big-data analytics technologies in providing everyone with access to basic healthcare services especially in low-income to middle-income countries. More precisely, previous research shows that media technology, for example, TV, empowers women in terms of attitude, knowledge and behaviour.22 23 Likewise, mobile-phone access is associated with enhanced financial independence, improved occupational choice,24 improved antenatal care attendance,25 lower perinatal mortality26 and increased contraceptive use, both at the micro and macro level.27
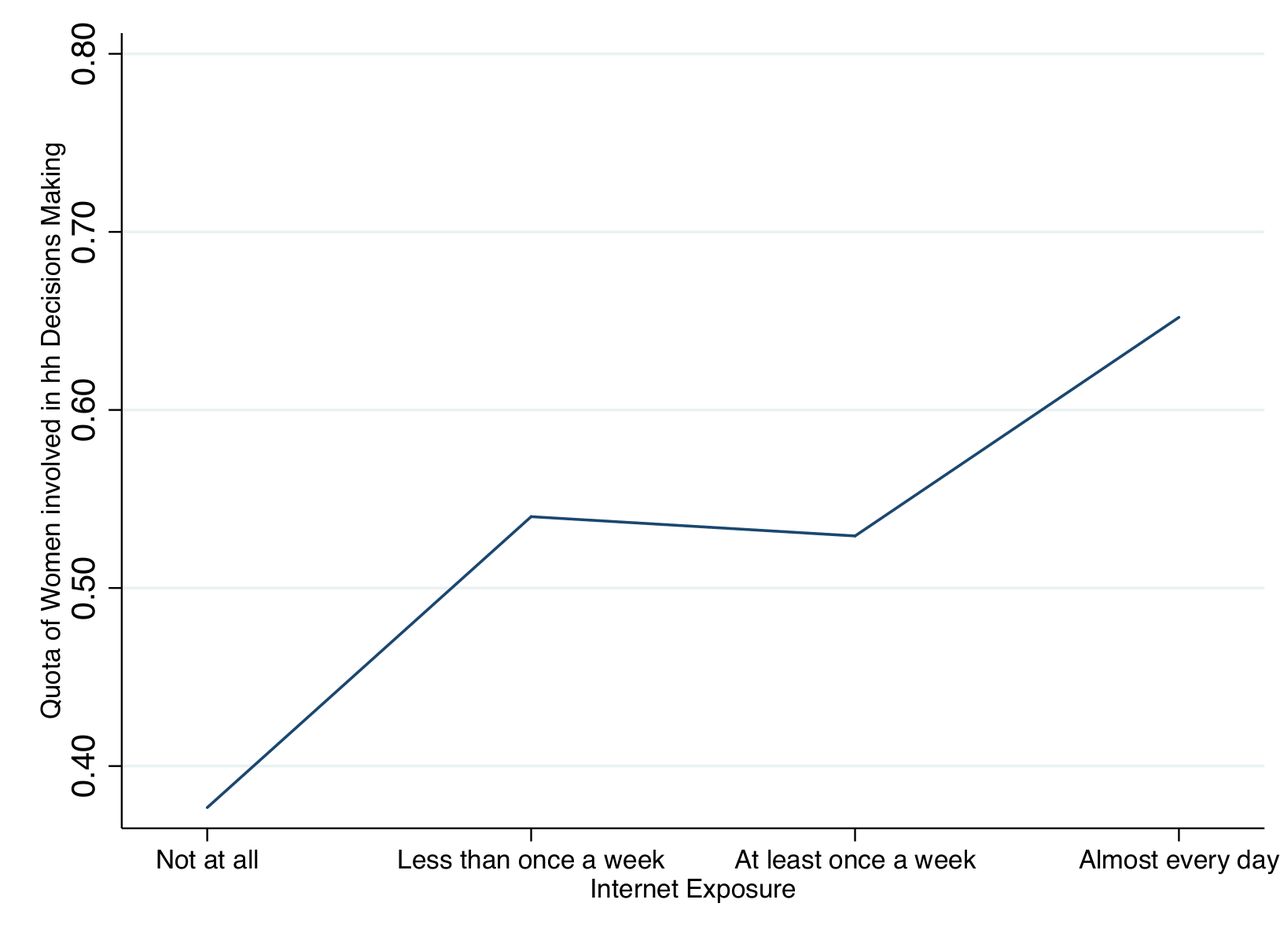
There are two mechanisms at play here. First, women with lower levels of education seem to be less likely to use family planning services as they know less about them compared with their highly educated peers. The internet acts as an equalising force in society, as online platforms increase awareness of family planning services. Less educated women are more likely to adopt modern contraception thanks to the internet, allowing them to potentially close the contraception gap with highly educated peers. Second, the internet arguably triggers women’s empowerment within the household. Knowledgeable women become more confident in talking to their partners about reproductive decisions. Figure 4 tests this kind of mechanism providing evidence of the bivariate association between women’s empowerment and internet exposure. Women’s empowerment is measured by the percentage of women involved in household decision-making. The graph highlights how the share of women involved in decision-making is almost twice as high among those who are exposed to internet daily as among those who have no access to the internet. Apparently, there are no differences between those who use internet at least once a week and those who use it less frequently.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Association between female empowerment and internet exposure.
Our estimates are somewhat larger, but generally consistent with the strong positive associations that are evident between internet exposure and modern contraception use in multivariate OLS regression, although the two coefficients cannot be compared as they have two different interpretations. Our estimates are adjusted for factors that may otherwise confound the relationship (eg, psychological traits, unmeasured socioeconomic status). Nevertheless, they have important specificities in terms of interpretation. First, the estimates are local to a given geographical unit; this granular level of detail might be crucial in uncovering different levels of exposure in quantitative and qualitative terms. Indeed, in our descriptive analysis, we found that the geographical level plays a role in the relationship. Second, the effects that we estimate are local to the subpopulation of compliers: that is, those who had increased internet exposure because the internet was available at the community level. Third, the results are local in public health terms, as we are looking at a context in which the unmet need for modern contraception is very high; effects of this magnitude might not be observed in a different setting. Fourth, the effects are local to the years of risk exposure under study (2011 through early 2019). These were years characterised by a surge in internet exposure generally, and this was especially true in SSA. We are, therefore, cautious about generalising to other settings; however, we suspect that our effect estimates are likely to be applicable in any society which urgently needs family planning and that the estimates give some sense of the probable benefits of mHealth and eHealth there. In addition to the heterogeneity of treatment effect, 2SLS results might be larger than the OLS result because unobserved factors, such as personal interest, are perhaps positively associated with both internet exposure and modern contraception, thereby leading to a downward bias in the OLS coefficients.
Our study has several limitations. First, we only observe individuals once. We cannot, therefore, identify individual preferences towards internet and/or modern contraception. Second, we observe women starting from the age of 15. We assume that this is the age that they become sexually active. However, it is worth asking whether this is really the case. There are many reasons why modern contraception use might change among younger women especially in younger generations. For instance, access to family planning programmes at school would result in gradual changes in the association across educational categories; something we control for. Third, our results are limited to eight SSA countries, the only ones for which information on internet exposure is available. We have no reasons to believe that those countries are different from other SSA nations, but one cannot, on current evidence, make sweeping generalisations for the entire SSA region. Fourth, unfortunately at its current stage, the DHS does not provide information on what the internet is used for. The question has been introduced for wave 8, which will be released in Spring 2021. Therefore, we cannot test whether internet is used to search for modern contraception; however previous evidence shows that digital devices are positively associated with contraception.27
These findings have important implications. The internet appears to be an effective way to deliver family planning and sexual health programmes. Not only that, internet access appears to narrow the gap between highly and less educated women and possibly it empowers women as well. The internet is, on this evidence, an important tool for achieving SDGs. Governments should encourage internet access and broadband development, and aim to keep access as affordable as possible.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
VT and HM are joint first authors.
Handling editor Seye Abimbola
Contributors VT, EB, GM, DM and AA conceived the idea. EB, GM and DM created the dataset. VT, EB, GM and DM carried out the analysis. AA supervised the analysis. VT drafted the manuscript. All the authors contributed to the interpretation of the results and the writing of the article.
Funding This work was funded by the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme (grant agreement n° 694145), project IFAMID - Institutional Family Demography (AA, VT).
Disclaimer The funder had no role in the analysis or interpretation of these results. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data are available from the Demographic Health Survey Database on formal request.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.