Article Text

Abstract
Introduction International calls for universal health coverage (UHC) have led many countries to implement health sector reforms, however, since the 2008 global recession, economic growth has slowed in many lower-income and middle-income countries. In a renewed interest in public financial management (PFM), international organisations have emphasised the importance of giving spending control to those responsible for healthcare. However, centralisation is a common response when there is a need to cut expenditure due to a reduced budget; yet failure to decentralise often hampers the achievement of important goals. This paper examines the effect of centralising financial decision-making on the functioning of the South African health system.
Methods We used a case study design with an ethnographic approach. Primary data collection was conducted through participant-observation and semistructured interviews, over 1 year. Member checking was conducted.
Results New management implemented centralisation due to a reduced budget, a history of financial mismanagement, the punitive regulatory environment financial managers face, and their fear of poor audit outcomes. The reform, together with an authoritarian management style to ensure compliance, created a large power distance between financial and clinical managers. District managers felt that there was poor communication about the reform and that decision-making was opaque. This lowered commitment to the reform, even for those who thought it was necessary. It also reduced communal action, creating an individualistic environment. The authoritarian management style, and the impact of centralisation on service delivery, negatively affected planning and decision making, impairing organisational functioning.
Conclusion As public health systems become even more financially constrained, recognising how PFM reforms can influence organisational culture, and how the negative effects can be mitigated, is of international importance. We highlight the importance of a participatory culture that encourages shared decision making and coproduction, particularly as countries grapple with how to achieve UHC with limited funds.
- health systems
- public health
- health policy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Health systems are facing demands for improved access to care in the context of constrained fiscal space.
Decentralisation of financial control to managers responsible for service delivery should, in theory, improve the use of funds.
What are the new findings?
A fear of poor audit outcomes can lead finance managers to hold onto financial control; this fear is exacerbated in austerity climates and in systems with a history of financial mismanagement.
Finance and clinical managers often do not have a shared vision of the goal of the health system, and this drives tension and impacts negatively on relationships.
This leads to an organisational culture that is competitive and dismissive of the needs of the collective.
This further weakens the health system.
What do the new findings imply?
Austerity can lead to radical public financial management reforms to attempt to control expenditure.
Finance and clinical managers need to find more opportunities to coproduce the shared goals of the department to ensure policy reform is aligned to systems goals—this can be done through multidisciplinary committees.
Relational accountability, which is fostered by working more closely together, can increase acceptability of decentralised control, which would improve participation and ultimately health systems functioning.
Introduction
In the last decade, international calls for universal health coverage (UHC), coupled with the Sustainable Development Goals’ inclusion of UHC, has led many countries to implement health sector reforms. However, fiscal space for public services has narrowed during this period given the 2008 recession, leading to a renewed interest in public financial management (PFM), given its intention to support service delivery, while controlling expenditure.1
The World Bank and World Health Organization (WHO) have re-emphasised the importance of giving spending control and flexibility to those responsible for healthcare such as facility managers and district health offices (DHOs). The aim of this decentralisation is to achieve more efficient use of funds.2 The reasons why this shift in control has not been widely implemented vary from a lack of capacity at the lower levels of the health system, to poor accountability mechanisms.3 Centralisation of financial decision making is in fact a more common response when there is a need to cut expenditure in line with a reduced budget. It is also likely to be a widespread response to the austerity that will follow the COVID-19 pandemic.3 However, failure to decentralise decision-making is likely to hamper the functioning of health systems, constraining their ability to maximise value from limited resources.
Since the 2008 global recession, South Africa (SA), like many other lower-income and middle-income countries (LMICs) has been experiencing low, or no, economic growth.4 The government has instituted widespread austerity measures, particularly to reduce the public sector wage bill.5 In 2012, the South African National Department of Health (NDoH) announced its intentions to implement UHC, through a national health insurance (NHI) scheme.6 As a result, the health system is grappling with how to responsibly manage public funds while responding to the new UHC policy goals,7 a problem that has come to the fore in many LMICs.8 In this paper, we examine the effect of centralising financial decision making on the functioning of a South African provincial department of health (PDoH), in an environment of health system reform.
Country context
SA is a middle-income country with a federal system of government. Until financial year 2012/2013, SA had been able to largely protect its social services sectors (eg, health, education) from the effects of slower economic growth and a decline in tax revenue. However, since 2014, this has no longer been possible and the social sector has been negatively affected by declining budgets in real terms, despite an increasing burden of disease. The austerity climate in the country has substantially worsened since 2019, due to attempts to recover from a period of widespread corruption.9 SA has a quadruple burden of disease which increases the need for health services.10 However, quality of care remains poor11 due to insufficient budgets and ineffective use of funds.
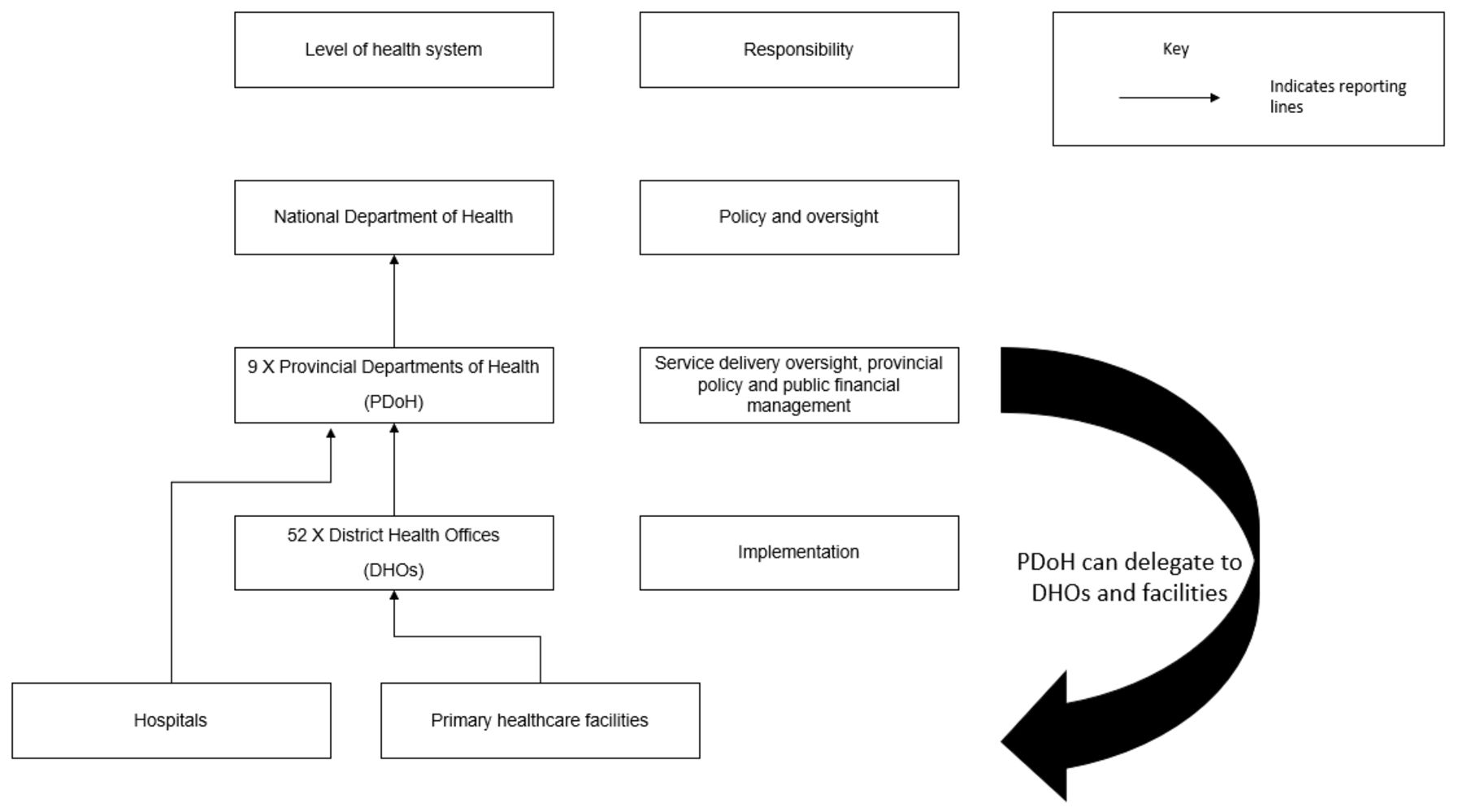
SA has an NDoH, nine PDoHs and 52 DHOs.12 Figure 1 illustrates the levels and responsibilities of the health system and shows that it is the responsibility of the PDoH to delegate financial decision-making to districts and facilities.
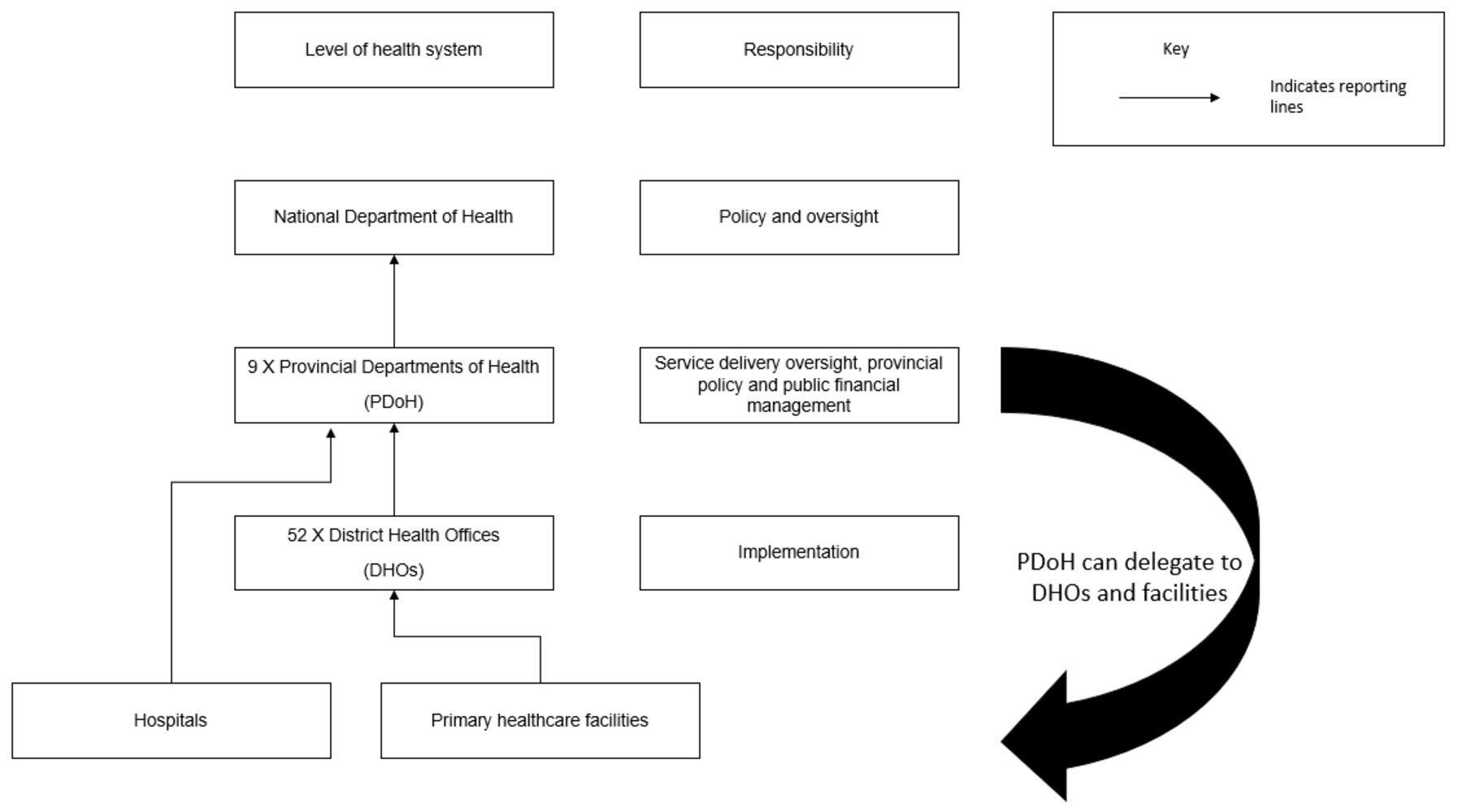
South African health system structure.
SA’s health sector has a long history of trying to decentralise governance to the DHOs, with the National Treasury and the NDoH encouraging PDoHs to deconcentrate power.13 14 Most of the PDoHs have experimented with ‘delegations’, which legally allows a lower level official to be responsible for a task that has been assigned to a more senior manager. However, the use of delegations remains limited. With NHI, the NDoH plans to shift financial accountability away from provinces to districts, essentially forcing decentralisation onto the health system.
Conceptual framework
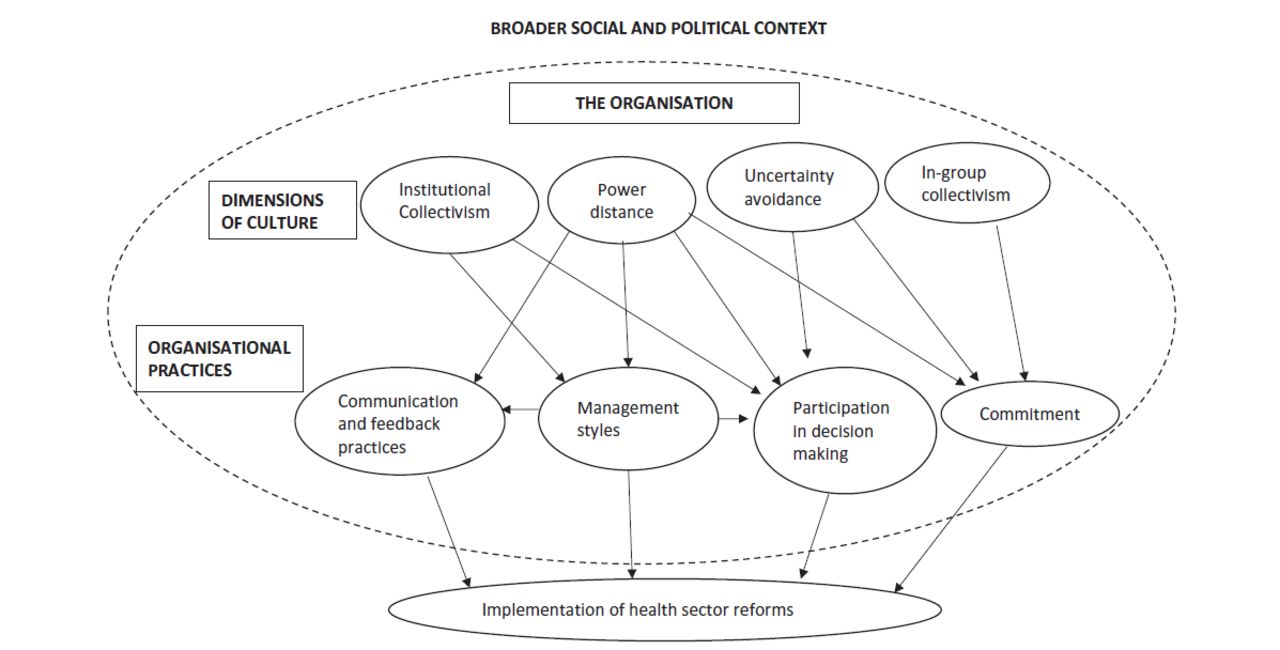
Since the 1980s, the field of organisational management has studied how people influence their organisation’s performance.15 ‘Organisational culture’ (OC), a theoretical construct within organisational management science, is generated as an organisation performs its functions, creating a pattern of shared assumptions. This culture governs the way people perceive, experience and, in turn, influence how the organisation functions.16 OC can answer questions about how decisions are made and offer possible reasons for why implementation is difficult despite an organisation having all the requisite infrastructure and resources (‘hardware’).17 OC is often seen as the connector between individual and collective behaviours and therefore is a useful paradigm when trying to analyse systemic policy failure.18 Within health systems and policy research, it is widely accepted that the functioning of a health system is influenced by the people working within it, and their relationships (‘software’).19 However, framing this phenomenon using OC is relatively new in the field. Therefore, a recent synthesis of evidence by Mbau and Gilson (2018) has been valuable in determining an analytical framework through which to analyse OC in LMIC health systems. Their framework illustrates the ways in which OC influences organisational functioning in LMICs (figure 2).20
{kind=link}
{kind=link}
Conceptual framework: Mbau and Gilson (2018).
The framework contains two layers: ‘dimensions of culture’ and ‘organisational practices’. Table 1 describes the dimensions of culture21 (we have renamed three of the dimensions for clarity), and table 2 the organisational practices.20 The dimensions and practices are interrelated. For example, managers, afraid of poor outcomes, may adopt an authoritarian management style to avoid uncertainty and control outcomes, resulting in a large power distance between managers and employees. A participatory management style, on the other hand, increases managers familiarity with the lower levels of the organisation, and so can reduce their fear of uncertain outcomes by improving their understanding of the challenges at lower levels. The resulting collective process facilitates better communication and feedback, increasing participation in decision making. It also fosters communal action across, and commitment to, the organisation.
Dimensions of culture
Organisational practices
Methods
Study design
We used a case study design, with ethnographic methods.22 These methods are appropriate when looking to explain ‘how’ or ‘why’ events happened, and health systems actors’ perspectives on them.23 Case studies are particularly valuable for research looking to understand OC within a particular setting, like a PDoH.24 Case studies allow for holistic research within the real context of the participants. It therefore pairs well with ethnography, which aims to understand the reality of participants from inside their context.22
Study setting and negotiating access
The PDoH studied is situated within a poor, predominantly rural province in SA. It has a long history of financial mismanagement and is one of the poorer performers in the country in terms of service delivery. The province has experimented with widespread delegations to the DHOs in the past but revoked them due to mismanagement. The austerity measures and PFM centralisation have been in place since 2015.
JW had previously worked with the province in her capacity as a health financing specialist and was known to many of the senior and middle managers. She met with one of the senior finance managers to ask whether the PDoH would be willing to participate in the study. From there, the research protocol was shared with the executive management of the province and the PDoH agreed to be involved.
Informed consent was obtained for all observations, interviews and audio recordings.
Participant selection
JW received informed consent from 60 individuals to be observed and was a participant observer in 10 meetings, which varied from routine financial management meetings to meetings with hospital chief executive officers (CEOs) at their facilities. In these meetings, she was allowed to ask questions and provided technical advice when invited to do so.
JW used purposive sampling for her interviews, contacting employees responsible for financial and clinical management at the PDoH head office, DHOs and public hospitals. She then used snowball sampling either through the introductions made at meetings or through a referral by an interviewee. No one explicitly refused to participate in the study, however, some never responded to several requests for an interview. She conducted 30 interviews (table 3).
Demographic characteristics of interviewees, by level of management and health system
Data collection
Data collection ran from July 2017 to June 2018. At the start of data collection, JW attended two 1-day meetings to introduce the research to key stakeholders.
JW collected all the data for the research. Data collection was conducted using participant observations and semistructured interviews. Data were collected by visiting the province for several days at a time. During these visits, JW attended meetings and conducted in-person interviews.
The majority of the observations and interviews took place either within the head office, DHO or a public hospital. For the observations, JW used an observation guide25 to make detailed meeting notes.
A semistructured interview guide26 was used for data collection. JW used a ‘grand tour’26 approach. Grand tour is useful when you want to elicit a thick description within case study research.27 The grand tour questions were adapted for interviews at the different levels of the health system. The questions were designed to prompt participants to share their experiences in their own words. Some of the questions included: ‘describe your average workday’ and ‘tell me about a time you interacted with the PDoH and how that impacted you’.
Interviews ranged from 20 min to over an hour. No one else was present at the interviews. Only one participant refused to be audio recorded; he felt this was necessary to be able to participate fully.
While repeat interviews were not conducted, the researchers did amend the interview questions during data collection to take into account knowledge already gained from previous interviews and observations. The authors discussed when no new information was emerging and determined data saturation had been reached.
Data analysis
JW wrote up her observation notes after each interaction. The audio files were deidentified and transcribed by an external company, and then checked for accuracy.
The authors read the data, with JW coding the data according to common themes, following which the authors discussed the emergent codes. JW then analysed the codes and grouped them into high-level themes. The authors interrogated these themes, discussing the strength of the evidence for each. We selected Mbau and Gilson’s (2018) framework as a useful way to frame the data. We used Dedoose to deductively recode the data,28 using themes from the framework, with a total of eight codes (four dimensions of culture and four organisational practice codes).
Identifiers are used to anonymise the quotations. We used ‘i’ for data gathered via an interview, followed by either a ‘P’ for PDoH, ‘D’ for DHO or ‘H’ for hospital. Observation notes were used to inform the analysis, but we do not use verbatim quotes from these.
Member checking was done through a participatory workshop to discuss the research findings. The invitation was extended to everyone within the head office, the two DHOs studied and the four public hospitals. The workshop was held over 1 day, with all attendees in the same workshop. The workshop was interactive, splitting attendees into groups to consider the research findings. These groups were heterogeneous, with at least one member from the different levels of the health system, as far as possible. Attendees gave input on whether the key themes were appropriate and engaged with the findings. The discussions at the workshop contributed to the proposed recommendations in this paper. This, along with the rigorous data analysis methods, have ensured the credibility and confirmability of the findings.29
Reflexivity
JW asked participants to clarify the background behind a statement, even though she was familiar with the history. This approach, combined with reflexive note taking and JG’s interrogation of the data, enabled JW to separate her perceptions from the respondents’ interpretations of events. JW also wrote down her thoughts on the quality of the interview and any insights that emerged.
Patient and public involvement
No patients or members of the public were involved in the research design, analysis nor dissemination of the findings; however, provincial managers contributed to the research focus in the planning stages, and provincial, district and hospital managers were involved in the interpretation of the findings.
Findings
Delivering health services in an austerity climate
Finance and clinical managers agreed that the current budget was insufficient for the health needs in the province: “The Department is underfunded, it might appear that it’s getting a huge piece of the cake within the provincial allocation, but all sectors are underfunded.” [iP7]. Many participants echoed this view: “It’s a joke budget. There was no way we could use it for the whole year.” [iH3]. Managers described their budgets as decreasing annually: “Normally, when the budget comes, it’s last year’s budget plus a percentage, but most recently, it’s last year’s budget less [a percentage]!” [iH3]. This has forced managers to purchase services that they do not have the funds for (resulting in accruals), to maintain service delivery: “When you do not have any money left, you just borrow! So, we owe our suppliers from way back!” [iH30]. As accruals from the previous year must be settled first; the impact of austerity is cumulative from one year to the next. A hospital manager highlighted the impact of this narrowing fiscal envelope for service delivery: “At the beginning of the year, we had a R120 million gap between the authorised budget and expected expenditure, but we were only left with a R70 million budget shortfall at the end of the year. That means we cut expenditure by R50 million somewhere, either by reducing services, or compromising the quality of care.” [iH30].
Over the last decade, the province has been attempting to rationalise the service delivery platform (reduce the number of facilities), to bring down the running costs, but these attempts have been unsuccessful largely due to resistance from surrounding communities who did not want to lose their facility. In addition, the PDoH has experienced a proliferation of ‘unfunded mandates’ in the pursuit of UHC: “A decision was made that we are […] to rollout the National Health Insurance (NHI) initiatives […] but there is no budget. When a decision is made by the political head, […] it must be implemented, so it is always at the expense of something else.” [iP7]. As a result, recent service delivery plans have become divorced from the available funding: “So, you would have ideas and plans, but they are then not implemented because you do not have the resources to carry them through.” [iP6]. This has resulted in tension between finance and clinical managers. For finance managers, it was imperative that the PDoH work within the available budget: “Of course I agree the budget is insufficient, but it does not mean we should not manage the one we've been allocated.” [iP9]. Clinical managers felt the burden of this approach, given their proximity to service delivery: “It’s very stressful, […] we are trying to deliver [services] to communities, but one of the major challenges is resource constraints.” [iP6].
Financial mismanagement, fear of uncertainty and centralisation
The province has a history of financial mismanagement and poor audit outcomes: “The district managers were given financial delegations, but they would go out for meetings on consecutive days and they would leave the order books signed, and then anybody who wanted to buy anything would just fill in the particulars!” [iP2]. The National and Provincial Treasury have had to intervene several times: “If the Department can't manage their salary payments, then provincial treasury takes that function away.” [iP4].
Emulating the Treasury’s approach, the PDoH tends to revoke financial control from the lower levels when there is evidence of mismanagement. This is implemented across the board, not just for the offending manager: “Something small happens, and then they just pull the delegations away! So, it’s like a knee-jerk reaction!” [iP4].
Since 2015, under new leadership, the PDoH has endeavoured to improve the financial audit outcomes by instituting a radical PFM centralisation reform. They established a ‘centralisation committee’, which is comprised of financial, clinical and support service managers who meet once a week to review expenditure and payment requests for the whole province. The committee is chaired by the chief financial officer (CFO), and its establishment revoked all delegations from the districts and facilities. Members of the committee are senior managers within the head office, with none from the DHOs or hospitals.
A hospital manager empathised with the rationale for the reform: “I understand why [they instituted this reform], and maybe, I would feel inclined to do the same. Health is an underfunded mandate, so, on paper, we try and prevent unauthorised expenditure because the CFO and financial managers will lose their jobs.” [iH30]. Several finance managers echoed the sentiment that the finance environment was very punitive: “So, if we want to see some bloodshed, one needs to look within the finance department, where I think the greatest amount of correspondence is sent out in terms of financial misconduct and I think that’s because Treasury has quite vigilant consequence management.” [iP10].
Power distance, commitment to the reform and effect on relationships
Clinical managers within the head office reflected on the centralisation of power: “Sometimes, when I engage fellow middle managers, I feel that they are not sure of certain decisions […], decision-making power is very much controlled at the executive management level.” [iP12]. It was not only clinical managers who felt aggrieved by the centralisation, finance managers in the districts also felt shackled: “I feel like head office are not giving you space. Even the district managers, the senior managers, are not given a space to cooperate and prove their worth or their capabilities.” [iD18]. Hospital managers were also dissatisfied: “To be a CEO in the department of health is a nightmare because we are given the responsibility, but you’re not given the necessary authority; you don’t have the financial delegations to do your job.” [iH20].
Many managers lamented the inefficiency of the new committee: “It can take a month for the committee to approve an order of a simple item, then there is the procurement, and then we still need the committee to approve the payment! It’s a nightmare from the facility’s point of view.” [iP4]. Managers were reluctant to support the reform, even those who felt centralisation was acceptable: “I feel the centralisation committee is necessary, but the committee does delay us. If communication were free flowing with actual turnaround times that are within reason, we wouldn’t mind.” [iD19]. Most managers felt centralisation was not the right solution and found it both inefficient and unfair to those who had not transgressed: “[They said] everything had to be centralised. I am saying, ‘that is not fair, why are we getting impacted in a negative way, it is not right.” [iH30].
Clinical managers described the strained relationship between the finance teams and them: “There is a huge discrepancy in understanding our individual roles and our team roles. We feel very strongly, from the clinical branch, that we should give direction, and then they should say how that can be supported. This is now not me alone [that holds this view], that I am sure of! We feel very strongly they are not a support to us. They are dictators.” [iP6]. In turn, finance managers bemoaned clinical managers’ lack of concern for the constrained fiscal environment: “Why are all clinical needs given a much higher priority than staying within the budget, when services cannot operate if we have run out of money?” [iP2].
To try and repair the relationship, the finance team at the head office assured managers that this reform was a short-term necessity to prevent continued financial disrepute. However, there has been no change to the reform in several years: “There has been this verbal commitment to differentiate the delegations, but there has been no follow through. I am told that it is going to happen now, but I have been told it is going to happen for the last year and a bit.” [iH30]. Once the audit outcomes begun to improve, finance managers cited fear of regression as the reason to maintain the reform: “The delegations have not been cascaded in order to manage the risk of [audit] regression. It would be a catastrophe if we were to regress.” [iP10]. This fear of uncertainty has permeated the department, impacting on relationships.
Management style
Head office admitted that they defaulted to an authoritarian management style to ensure compliance: “We bully the districts, and they basically just do what we tell them to do. It’s sometimes like malicious compliance; they just do it because they have to, but they don't see the value in it.” [iP4].
The authoritarian management style created extra unnecessary work: “I really feel that lots of work could be avoided if we have a ‘bottom up’ approach. We just hand over the paperwork for decisions that have already been made by the head office. We need to meet each other halfway and it’s really not happening.” [iP16]. The lack of a participatory environment de-motivated staff: “You are unable to take a decision; you are unable to deal with any challenges on your own. All the challenges are thrown to the seniors and then you are only told what to do. So, you become stagnant.” [iP8].
Finance managers were sceptical about involving others in decision-making spaces: “If you allowed a ‘bottom up’ approach, the Department would close tomorrow. Clinical managers see patients, rather than the resources. They don’t seriously consider what is available, they want what they want.” [iP9].
However, many clinical managers suggested that agile accountability mechanisms that are able to identify and correct mistakes quickly could help reduce financial mismanagement: “If we are being wasteful or have done it incorrectly, then charge us! We will quickly do the right things!” [iH30]. District finance managers also pushed for delegated control: “They are saying we will mess up the budget, it won’t balance, but I don’t think that’s true, [if there is a mistake] they know where to take that complaint to.” [iD21].
The effect on communal action
Many managers reported feeling loyal to the organisation: “I love what I do so, maybe that’s why, even though it is stressful, there are things that cause you to wake up and come to work. Being a provider of a public service is not always easy, but I think passion drives us.” [iD13]. This was not limited to clinical managers, finance managers felt similarly: “If I look at my job, it’s a job that I love, that I'm absolutely motivated and inspired to be doing.” [iP10]. This loyalty to the organisation appeared to be a major consideration for managers remaining in the organisation during exceptionally difficult circumstances.
However, the lack of a participatory management style affected organisational functioning: “I find the misalignment comes […] when we are doing the annual performance plan (APP). The head office managers are not so in tune with what is happening at district […] The district health plans should find expression within the APP […] but they do not.” [iP12]. Clinical managers reported not participating in budget related meetings: “I stopped presenting at the provincial hospital forum because it’s useless. I said to the head of hospital services, I can’t understand the rationale behind the final allocation!” [iH3].
By not attending these meetings, clinical and finance managers were not always aware of the needs of their peers, making it easier to turn inwards: “People are territorial. If I am a district manager, and I have R50m budget, […] I will not use my R50m to save someone else who has a challenge.” [iP1]. Managers reported competing for resources: “We have had a 16% increase in patients coming through our hospital and yet the budgets have actually decreased, because we are competing with primary healthcare.” [iH30]. One participant described how this competitive culture played out: “A clinic was congested, staff seeing patients in every corner. There was an empty hospital, with a big outpatient department (OPD), but the CEO [of that hospital] said ‘no, the clinics can’t use the OPD to see the [overflow] patients.” [iD17]. The absence of a participatory culture affected how the organisation functioned: “People work in siloes and are protective of their status.” [iP8].
Several managers expressed a desire for a more collectivist culture: “We need interaction between both levels [of management] and understanding and [to be] working together. If I support the top manager, then it becomes easy for them, and if I'm an administrator at the lower level, if I get the support of my manager, then it becomes easy for me!” [iP8]. The district management team (DMT) attributed some of their successes to the integration and communal action they have managed to foster: “There’s a team there with everybody in the DMT, the finance people, everyone, everyone with their specific duties.” [iD11]. One hospital manager suggested a more participatory approach: “If I was the Head of Department, my management team would not just be people from the head office. My team would be district managers and CEOs of the big hospitals. We would all drive implementation together. So, your planning and priorities come from that team in full cooperation and we are bound together.” [iH30].
Discussion
In this paper, we have described how centralisation was implemented in response to austerity and financial mismanagement, the punitive regulatory environment financial managers face and their fear of poor audit outcomes. The reform, together with an authoritarian management style to ensure compliance, created a large power distance. Managers felt that the committee gave insufficient feedback and that decision-making was opaque. This lowered commitment to the reform, even for those who thought, given the PDoHs financial history, the reform was necessary. It also reduced communal action, creating a more ‘territorial’/individualistic environment. While many managers expressed their loyalty to the organisation and how this had kept them motivated, the authoritarian management style, and the impact of centralisation on service delivery, had negatively affected organisational planning and decision-making.
Problems with implementation are often attributed to misalignment and misunderstanding between actors in health systems.30 Many managers in our study reported that the head office was disconnected from the rest of the health system, making them ill suited for centralised control. However, given the fear of uncertainty, finance managers remained wary of financial decentralisation, as is common during fiscally constrained periods,31 and therefore, the reform has remained in place.
Different parts of an organisation often have their own subcultures that may be in conflict with one another. However, as long as the subcultures are aligned to the overarching organisational goals, this may not be a problem.16 Studies of hospital wards have explored how a punitive PFM regulatory environment exacerbates the harmful effect of austerity on service delivery, and can lead to irrational purchasing decisions.32 We have reported on the punitive subculture within the finance teams and the disagreement between finance and clinical teams on the organisation’s goals. Where spaces for shared decision making were created, clinical managers often refused to participate as their contributions were not truly considered, reducing communal action, and impacting negatively on departmental performance.
Organisations with an authoritarian management style often rely on ‘bureaucratic’ and punitive accountability mechanisms to ensure adherence to policies.33 In contrast, ‘relational’ accountability theory points to the importance of positive supervisory relationships to exist alongside accountability measures for the latter to be effective. If the supervisor has a greater understanding of the challenges the supervisee is facing, a realistic compromise is possible.33 Relational accountability requires a participatory management style and coproduction.
Changing to a participatory environment can, however, be difficult when an organisation’s culture favours ‘command and control’ and top-down decision making,34 as seen in the province studied. Our recommendations below centre on bringing diverse managers together more often, and in different settings, as a start toward building the relationships (and culture) needed for a functional organisation.
SA, like many other LMICs, envisions using capitation and similar methods for reimbursement under its NHI,35 with predetermined limits on what can be spent, and financial accountability shifting to the district health offices. In preparation for NHI reform, managers could use a similar approach, even if just for a discrete list of items, to facilitate the shift to decentralisation. For example, a cost per capita for primary healthcare (PHC) services is fairly easy to determine given available data, and the province could decentralise sufficient funds to cover PHC visits, to the DHOs. This shifts spending power to the lower levels while still maintaining control over the spending ceiling, a core goal for successful PFM.
We suggest recommendations (box 1) that facilitate engagement and communication across finance and clinical managers, a key challenge especially for LMICs who are under the dual pressure of austerity and UHC implementation. In following these recommendations, PFM reforms can be developed collaboratively, which can ensure both reform success and safeguarding of OC and so, an organisation’s functioning.
Recommendations
For the study setting
Include district managers and hospital chief executive officers in the provincial executive team.
Rotate provincial finance managers through district health offices (DHOs) and hospitals to facilitate greater understanding of the challenges on the ground; this will allow for relational accountability.
Rotate the chair of the centralisation committee on a weekly basis.
Invite key stakeholders from the districts and facilities to sit on the centralisation committee, including members of the district centralisation committees, even if on an ad hoc/as possible basis, to build capacity at lower levels, and foster trust between the levels of the health system, in preparation for decentralisation and National Health Insurance.
In time, the centralisation committee could determine a list of decisions that could be delegated to district-level committees. The time spent together should provide a foundation for relational accountability, which should improve public financial management.
For international application
Finance managers should spend time in facilities and DHOs to better understand the reality on the ground.
The time spent together on the ground would support relational accountability between clinical and finance managers.
Once the relationship between clinical and finance managers begins to strengthen, finance teams should determine an initial list of decisions that can be delegated to the lower levels of the system to support a transition to decentralisation.
As we grapple with the COVID-19 pandemic, the austerity climate is bound to worsen. We need to be mindful of the ways in which austerity and the PFM policies it brings, can impact on OC, and so affect organisational functioning. The World Bank Group has already started publishing guidance for treasuries on how to be able to respond agilely to the needs of social sectors,36 for example, by making it easier for facilities to access funds to procure needed goods and by allowing for more real time reporting of available cash. Our paper showcases the deleterious effects of a health system that is unresponsive and authoritarian and feeds into this new body of recommendations that call for greater collaboration across finance and clinical managers. The pandemic could further tip the scales of power toward finance managers, as they attempt to control the shrinking public purse. We caution against this and highlight the system benefits of a participatory culture, especially for effective PFM.
JWs access to managers was linked to her existing relationships and these were mostly with senior managers. This was a possible reason for only four junior managers agreeing to be interviewed. The distance between her home province and the study province restricted how often she could conduct data collection. This was mitigated through longer data collection periods. Lastly, the findings are limited to one province; while they cannot be generalised, the experiences documented are similar in other South African provincial departments of health and LMICs.
Conclusion
The PDoHs centralisation reform influenced its OC, reducing opportunities for participatory decision making and polarising finance and clinical managers. This not only hindered reform implementation, but also impacted negatively on the overall functioning of the health system. The pressure placed on the department by the socio-political context of austerity and financial mismanagement, had a direct bearing on reform choice and design. As public health systems become even more financially constrained, alongside the pressure to rollout massive system restructuring to support UHC, recognising the ways in which PFM reform can influence OC, and how the negative effects can be mitigated, is of international importance.
Acknowledgments
We would like to acknowledge the PDoH and all participants for their contribution.
Footnotes
Handling editor Stephanie M Topp
Twitter @jodi_wishnia
Contributors Both authors conceived of and planned the paper. JW is the principal researcher and conducted data collection and primary data analysis. JG reviewed the data analysis results and provided expert guidance. JW was the primary manuscript writer, with JG providing detailed input. Both authors approved the final version of the manuscript.
Funding JW’s research is funded by the South African Research Chair Initiative.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Ethics approval Ethical approval was granted by the University of Witwatersrand’s Human Research Ethics Committee (Medical) (M170346) and the PDoHs research committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information. All relevant data are included in the paper.