Article Text

Abstract
Introduction Although universal drug susceptibility testing (DST) is a component of the End-TB Strategy, over 70% of drug-resistant tuberculosis (DR-TB) cases globally remain undetected. This detection gap reflects difficulties in DST scale-up and substantial heterogeneity in policies and implemented practices. We conducted a systematic review and meta-analysis to assess whether implementation of universal DST yields increased DR-TB detection compared with only selectively testing high-risk groups.
Methods PubMed, Embase, Global Health, Cochrane Library and Web of Science Core Collection were searched for publications reporting on the differential yield of universal versus selective DST implementation on the proportion of DR-TB, from January 2007 to June 2019. Random-effects meta-analyses were used to calculate respective pooled proportions of DR-TB cases detected; Higgins test and prediction intervals were used to assess between-study heterogeneity. We adapted an existing risk-of-bias assessment tool for prevalence studies.
Results Of 18 736 unique citations, 101 studies were included in the qualitative synthesis. All studies used WHO-endorsed DST methods, and most (87.1%) involved both high-risk groups and the general population. We found only cross-sectional, observational, non-randomised studies that compared universal with selective DST strategies. Only four studies directly compared the testing approaches in the same study population, with the proportion of DR-TB cases detected ranging from 2.2% (95% CI: 1.4% to 3.2%) to 12.8% (95% CI: 11.4% to 14.3%) with selective testing, versus 4.4% (95% CI: 3.3% to 5.8%) to 9.8% (95% CI: 8.9% to 10.7%) with universal testing. Broad population studies were very heterogeneous. The vast majority (88/101; 87.1%) reported on the results of universal testing. However, while 37 (36.6%)/101 included all presumptive TB cases, an equal number of studies applied sputum-smear as a preselection criterion. A meaningful meta-analysis was not possible.
Conclusion Given the absence of randomised studies and the paucity of studies comparing strategies head to head, and selection bias in many studies that applied universal testing, our findings have limited generalisability. The lack of evidence reinforces the need for better data to inform policies.
- tuberculosis
- epidemiology
- systematic review
- diagnostics and tools
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Globally, less than one-third of the estimated 560 000 drug-resistant tuberculosis (DR-TB) cases are reported.
This gap is due in part to differential policies in drug susceptibility testing (DST) between and within countries.
What are the new findings?
Although universal DST is a key component of the End-TB Strategy, the existing literature has several limitations making it difficult to estimate the added value of universal testing for DR-TB detection compared with only selectively testing high-risk groups.
In the absence of evidence from randomised studies, we found very limited representative data by country or region and only few studies that compared the targeted versus universal testing strategy.
Across studies, participants were often preselected, and a true universal DST approach was rarely implemented.
What do the new findings imply?
Given the substantial resources necessary in maintaining and operating universal DST systems, more studies on the differential impact and cost-effectiveness of universal DST versus targeted DST would be very important.
This data would serve to better inform country-specific guidelines, prioritise effective programmatic interventions and funding.
Introduction
The WHO’s End TB strategy prioritises the early diagnosis of tuberculosis (TB) including universal drug susceptibility testing (DST).1 2 If resistance to key drugs such as rifampicin and isoniazid is not detected, the probability for treatment failure is high.3 In 2018 only half of the 3.2 million bacteriologically confirmed pulmonary TB cases notified globally were tested for rifampicin resistance (RR), only one-third of the estimated 560 000 drug-resistant tuberculosis (DR-TB) cases were reported at all, and only 59% received further DST beyond RR testing among patients with DR-TB notified in 2018.1
This discordance between the estimated burden of DR-TB and the number of cases identified represents a grave failure in health systems management of this condition, despite the fact that WHO recommends to do at least RR testing on all TB cases identified.3 4
A modelling study which informed the End-TB Strategy concluded that the performance of a rapid DST for RR detection in patients before beginning treatment would be the most cost-effective of several test-and-treat strategies for DR-TB in terms of Daily Adjusted Life Years gained, multidrug-resistant tuberculosis (MDR-TB) prevention and deaths averted.5 Those diagnosed with RR-TB are to be further evaluated for resistance to the next level of drugs proposed in second-line treatment regimens. In 2018, the WHO also recommended that all efforts need to be made by all countries to move towards universal testing of isoniazid at the start of TB treatment in addition to rifampicin.6
However, universal DST is often only achieved in higher-income countries with a low TB burden, and DST coverage varies substantially among high TB burden and also high MDR-TB burden countries.1 7 8 Due to funding restraints, laboratory capacities and general health systems failings, most low-income and middle-income countries currently offer routine DST only for patients at high risk of DR-TB (eg, patients who fail therapy or have a record of previous treatment).2
Culture-based DST represents the gold standard method for evaluating the resistance pattern of a TB isolate. Substantial progress in bolstering laboratory services and expanding culture capacity has been achieved due to the collective effort of global partnerships through funding and technical training. However, high costs and complex technical requirements significantly hinder large-scale implementation. Among the key advancements for TB DST over the past few years, have been molecular technologies such as line probe assays (LPAs) for first-line and second-line anti-TB drugs, Xpert MTB/RIF assay (Xpert; Cepheid, Sunnyvale, California, USA) and more recently the Molbio (Truenat MTB) and large centralised platforms. While tests other than the GeneXpert and Molbio still require sophisticated infrastructure with Biosafety Level 2 and therefore are implemented at central laboratories in National Tuberculosis Programmes,1 9 the Xpert and Molbio enable identification of TB bacteria and RR-TB closer to the patient.10–12 These advancements in TB diagnostics could allow for broader coverage of DST in different levels of the healthcare system.
This systematic review assessed the comparative yield of universal DST versus DST targeted to high-risk groups only to better understand potential benefits of one strategy over the other.
Methods
This systematic review and meta-analysis is reported in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (see online supplemental file for the PRISMA checklist).13 The protocol for this work was registered in the International Prospective Register of Systematic Reviews (PROSPERO, identifier: CRD42017065030).
Supplemental material
Eligibility criteria
Studies eligible for inclusion reported on the number of RR-TB and/or MDR-TB among the total number of patients tested through universal and/or selective DST implementation. Cross-sectional studies, cohort studies, randomised and non-randomised controlled trials as well as reports on programmatic evaluations were considered for inclusion. No specific restrictions were placed in terms of demographic and clinical characteristics (eg, age, sex, pregnancy status, HIV status) of the population being studied, but we did exclude studies solely focused on special groups (eg, occupational cohorts, prisoners and institutionalised individuals). Furthermore, we excluded any diagnostic accuracy study based on panels of samples with minimum clinical details. Conference proceedings and abstracts were also deemed ineligible.
Search strategy
Medline (PubMed), EMBASE (Ovid), Global Health (Ovid), SCI-EXPANDED, CPCI-S, ESCI (Web of Science Core Collection), Cochrane Reviews and CENTRAL (Cochrane Library) were systematically searched from 1 January 2007 until 28 June 2019. The strategy was developed in collaboration with a medical librarian (GG) using combinations of subject headings (when applicable) and text-words for the concepts of DST and DR-TB, restricting to publications in English, French, Italian, Spanish or Portuguese. The full search strategy used for PubMed is presented in the online supplemental file.
Main definitions
For the purpose of this study, we defined ‘universal’ as any DST strategy where all individuals included in the study were tested, as opposed to ‘selective’ strategies where select, high-risk groups underwent DST. With regards to DST methods, we distinguished between ‘molecular tests’ (genotypic), defined as those able to detect resistance-associated mutations in the genome of Mycobacterium tuberculosis, versus ‘culture-based’ (phenotypic) tests, defined as those based on the evaluation of a TB isolate’s growth in the presence of a given drug. For the purpose of this review, resistant cases were defined as those infected with MTB strains with RR or MDR.
Study countries were categorised according to TB burden into ‘low’ (TB incidence below 50 cases per 100 000), ‘intermediate’ (50 to 100 cases per 100 000) and ‘high’ (incidences greater than 100 per 100 000). The WHO’s high-burden country lists were utilised to differentiate studies as conducted in high-TB, MDR-TB or TB/HIV burden areas versus others. The 2015 lists and the 2016–2020 update were considered in separate analyses.8
We referred to the World Bank categorisation to classify study countries as low-income, lower-middle-income, upper-middle-income or high-income based on gross national income per capita of the study start year.14 ‘Urban’ and ‘rural’ areas were categorised in accordance with the authors’ descriptions.
Study screening and data extraction
All records obtained through our searches were imported into a citation manager (EndNote X9, Clarivate Analytics). Two authors (AS and GS) independently screened all publications by title and abstract against predefined eligibility criteria, followed by full-text review for those eligible; all texts were double extracted. An electronic data extraction form was piloted on five randomly selected papers and then used to extract information from included studies. A comprehensive list of data items that were collected at this stage is presented in the online supplemental file. Throughout the screening and data extraction process, disagreements were discussed until consensus was reached, and a senior author (CMD) was consulted when necessary. Study authors were contacted to request clarifications or additional data if needed.
Assessment of study quality and publication bias
A revised version of an existing tool developed by Hoy et al15 was utilised to assess the risk of bias in individual studies by AS and GS, independently (see online supplemental file). We considered eight specific items related to participants’ selection, case definitions and methods used, and assigned a qualitative score of ‘high’ or ‘low’ risk to each of them. A summary items for overall risk of study bias was also defined and rated as ‘low’, ‘moderate’ or ‘high’ in line with what was suggested in the original tool. No numeric scores were applied. We could not perform any formal assessment of publication bias because traditional approaches such as funnel plots and tests for asymmetry are known to be inappropriate for the type of studies included.16
Statistical analysis
For all included studies, we calculated the proportion of resistant cases detected among those tested through various DST strategies (universal or selective), both overall and across strata of key variables of interest (ie, age, sex, HIV status, previous anti-TB treatment status, country TB or MDR-TB burden, country income level). We used the more conservative Clopper-Pearson (or exact) method to calculate 95% CIs for each prevalence proportion.
We planned to conduct random effects meta-analyses with and without Freeman-Tukey transformation in order to estimate pooled proportions.17 As we anticipated considerable levels of between-study heterogeneity, we only pooled sufficiently homogeneous studies thus performing various predefined subgroup analyses (eg, by MDR-TB burden country category, previous treatment status, etc). Higgins test and prediction intervals (ie, a type of CI that provides the 95% range of true values to be expected in similar studies) were utilised to evaluate heterogeneity.18 19
All analyses were conducted in STATA (V.16; Stata Corp, USA). The Metaprop package was used to conduct the meta-analysis.20 21
Patient and public involvement
It was not appropriate or possible to involve patients or the public in the design, or conduct, or reporting or dissemination plans of our research.
Results
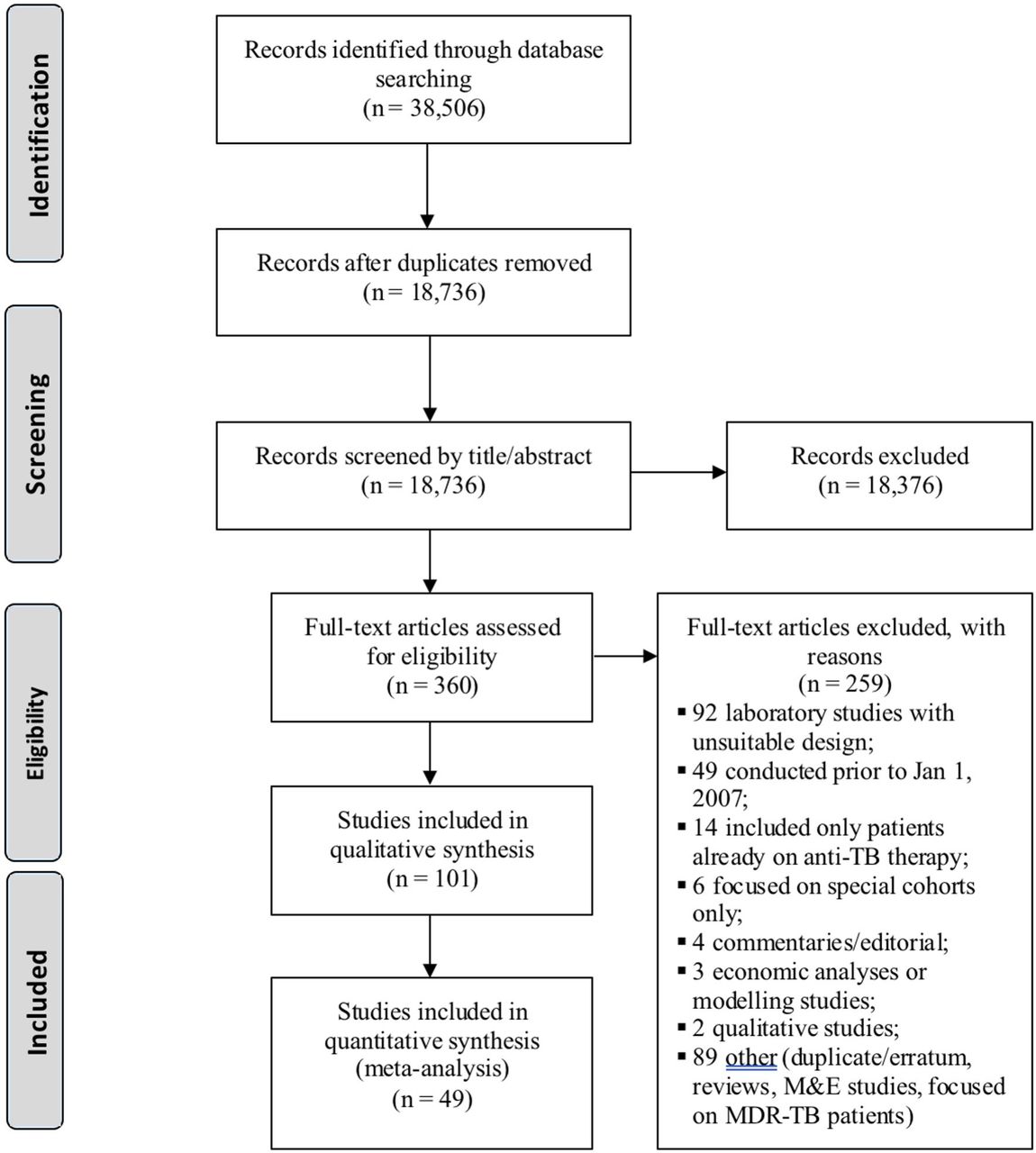
Our search yielded 38 506 records resulting in a total of 18 736 unique citations, of which 101 were included in the analyses (figure 1). The main features of included studies are summarised in table 1.22–122
Main features of included studies

PRISMA flow chart. M&E, Monitoring and Evaluation; MDR-TB, multidrug-resistant tuberculosis; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
We did not identify any randomised trials that compared universal with selective DST strategies. We found only observational studies, and all were cross-sectional and most (88/101; 87.1%) included high-risk groups. When broad population studies were analysed, we found that study samples were quite heterogeneous across studies. The vast majority (88/101; 87.1%) reported on the results of universal DST strategies. However, while 37 (36.6%)/101 included all presumptive TB cases, an equal number of studies applied sputum-smear as a preselection criterion and included only smear-positive individuals. In the remaining studies, even more restrictive selection criteria were applied (eg, culture-positive cases without clear description of criteria that led the healthcare provider to refer the patient for culture).
Selective testing was the only strategy adopted in nine studies (of which seven were carried out in high MDR-TB burden countries), with proportions of DR-TB cases ranging from 12% (95% CI: 8% to 17%) to 69% (95% CI: 66% to 71%).32 86
Among the 87 studies that provided some information on patients’ age, only 2 (2.0%) were focused on children, 39 (38.6%) on adults and 45 (44.6%) involved subjects of any age. Only 60 (59.4%) studies reported on patients’ HIV status, and the majority of those (55/60; 91.7%) included a mixed population. Nearly half of included studies were conducted in the African Region (48/101; 47.5%), 23 (22.8%)/101 took place in South-East Asian countries and 14 (13.9%)/101 in the Western-Pacific Region. Most studies were carried out in lower-middle income countries and in high-TB incidence settings, with urban areas being disproportionately represented. Around two-thirds of the studies took place in high-MDR-TB burden countries (69 according to the 2015 list and 75 based on the post-2015 classification).
Study quality
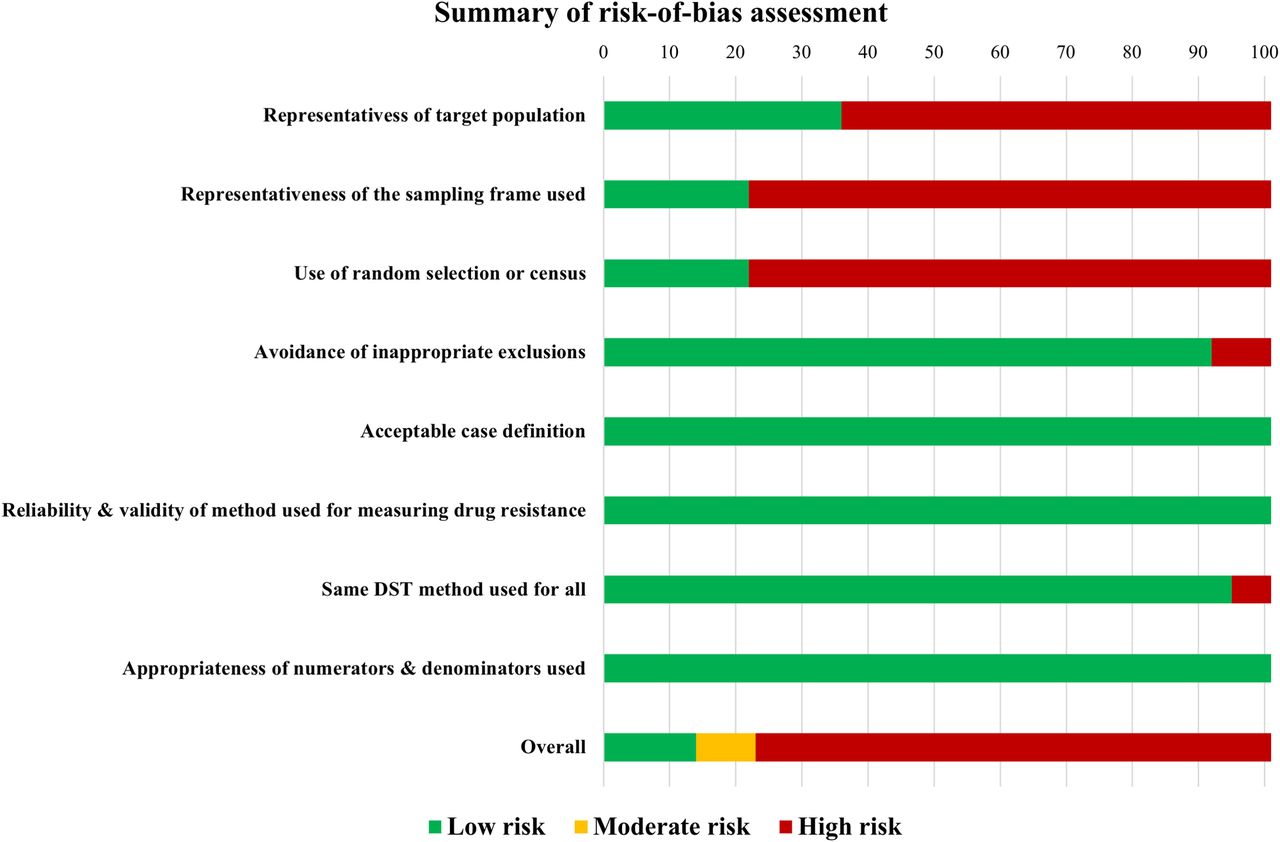
Figure 2 shows the summary of risk of bias assessment, while the individual studies’ quality assessment results are reported in the online supplemental file. The overall risk of study bias was scored as high for 78 (77.2%)/101, moderate for 9 (8.9%) and low for 14 (13.9%) studies. Representativeness of the studies was very limited. Most studies were conducted in one or few facilities, were usually restricted to limited geographic areas and did not employ any form of random selection to identify participants. About 1 out of 10 studies made exclusions of patients with prespecified characteristics, thus increasing the risk of selection bias. All studies utilised WHO-endorsed diagnostic methods and adopted international standards for the identification of presumptive cases and the categorisation of risk groups. Therefore, both the case definition and the validity and reliability of the DST methods used were always judged as adequate.

Summary of study risk-of-bias assessment.
Head-to-head comparison of universal versus selective testing
As shown in table 2, only four studies directly compared universal and selective DST strategies in the same study population.45 60 96 123 Prevalence proportions of DR-TB cases ranged from 2.2% (95% CI: 1.4% to 3.2%) to 12.8% (95% CI: 11.4% to 14.3%) with selective testing,60 123 versus 4.4% (95% CI: 3.3% to 5.8%) to 9.8% (95% CI: 8.9% to 10.7%) with universal testing.60 123 Estimates were not pooled across studies due to the small number of available studies.
Main findings of studies that compared universal and selective testing strategies
These were all non-randomised studies without an explicit intention to conduct a head-to-head comparison of different strategies. Moreover, three out of four studies were carried out in South Africa,45 60 85 while the remaining was done in India.96
In India, Raizada et al96 involved a cohort of HIV-infected individuals with presumptive pulmonary TB, all of whom were offered Xpert testing regardless of their risk profile for DR-TB; phenotypic DST was performed only on RR specimens based on Xpert testing. The proportion of resistant cases detected among those tested was presented separately for presumptive DR-TB cases and others, thus allowing to compare the results of selectively testing only high-risk groups versus providing universal DST. However, all patients in the study were HIV infected and thus in itself a high-risk group. The proportion of DR-TB cases identified through universal testing was 9.5% (95% CI: 7.5% to 11.8%), as opposed to 11.2% (95% CI: 6.5% to 17.5%) with selective testing. As shown in table 2, the prevalence of RR-TB found among high-risk groups in this study reflects the WHO estimates for previously treated patients in India, although only 20.8% of patients included in the study had a known history of TB.
Cox and colleagues conducted a two-arm non-randomised study in South Africa where one arm was assigned to universal Xpert testing, while the other arm was assigned to routine diagnostic work-up whereby DST was performed only if an individual was considered high-risk (such as previously treated, any prison contact etc).45 Among those tested, the number resistant was small, and the proportions resistant were 11/199 (5.5%; 95% CI: 2.8% to 9.7%) and 8/109 (7.3%; 3.2% to 14.0%) for universal and selective strategies, respectively. Yet, the study was likely underpowered to detect meaningful differences across groups.
Hanrahan et al60 aimed at evaluating the impact of introducing the LPA method for the rapid detection of DR-TB across 25 public health facilities in South Africa. The researchers employed the universal testing on all presumptive TB cases and in the selective algorithm only performed DST on presumptive TB cases at high risk for MDR-TB. In this setting, universal testing allowed to identify twice as many resistant cases as those found with selecting testing: 52/1177 (4.4%; 95% CI: 3.3% to 5.8%) and 26/1176 (2.2%; 95% CI: 1.4% to 3.2%), respectively.
Finally, Naidoo and coworkers evaluated patients who were identified through a previous stepped-wedge study and compared DR-TB detection during and after the implementation of Xpert-based testing.123 In this study, the ‘universal DST’ group included all presumptive TB cases, whereas the ‘selective’ group included all previously treated TB cases, those from congregate settings or with MDR-TB contact.123 The investigators found that 415/4235 (9.8%; 95% CI: 8.9% to 10.7%) of all presumptive TB cases (universal testing) had MDR-TB, while the prevalence of MDR-TB among selected high-risk individuals amounted to 269/2099 (12.8%; 95% CI: 11.4% to 14.3%).
The high levels of between-study heterogeneity in terms of population, selection criteria and settings prevented us from pooling estimates.
Yield of universal testing
When assessing 90 studies that adopted the most inclusive (‘universal’) testing approach, the studies were very heterogeneous, and the overall proportion of DR-TB cases detected ranged from 0% in two studies conducted in Malawi and Nepal, to 52.8% in a study from India where presumptive TB cases with and without risk factors for DR-TB were involved.39 44 106 When assessed by different burden of DR-TB as reported in the 2015 WHO list, 62 studies reported on universal DST in high MDR-TB burden countries. The yield of resistant cases identified across these studies also varied widely, ranging from 0% to 86%. Even if proportions of resistant cases were generally much higher among previously treated cases (2%–81%) as opposed to new patients (0%–66%), differences across studies were too pronounced to allow any kind of further analysis or pooling even by smaller subgroups.
Prevalence surveys
Out of the 37 studies that included all patients with presumptive TB only two were prevalence surveys. Noeske et al performed a cross-sectional survey in all 10 regions of Cameroon over a period of 6 weeks, enrolling all adults presenting at each testing centre with symptoms compatible with pulmonary TB. The explicit objective of this study was to estimate the prevalence of MDR-TB in new bacteriologically confirmed pulmonary TB cases, which was found to be 2% (95% CI: 1% to 3%).87
In another study, Lukoye and colleagues collected specimens from a nationally representative sample of new and previously treated sputum smear-positive patients with TB registered at TB diagnostic centres in Uganda, using of a weighted cluster sampling method. DST on these samples yielded a proportion of MDR-TB of 1.4% (95% CI: 0.6% to 2.2%) and 12.1% (95% CI: 6.8% to 19.4%) for new and previously treated patients, respectively.75
Studies from selected high MDR-TB burden countries
In the attempt to identify more homogeneous studies, we focused our attention on four high MDR-TB burden countries (China, Ethiopia, India and Nigeria) for which at least five studies were available. Across studies, the ranges of proportion of resistant cases detected through universal testing were as follows: 4%–22% in China; 0%–61% in Ethiopia; 0%–59% in India; and 0%–44% in Nigeria. Country-specific pooled estimates are shown in figure 3 along with WHO estimates for new and previously treated patients. Forest plots for country-specific estimates obtained from our meta-analysis are reported in the online supplemental file.

{kind=link}
{kind=link}
{kind=link}
DR-TB prevalence estimates for selected high MDR-TB burden countries. DR-TB, drug-resistant tuberculosis; MDR-TB, multidrug-resistant tuberculosis.
The wide range of resistance proportions in these studies indicate large heterogeneity, which was particularly pronounced among studies from Ethiopia. For this reason, we will report on a subset of studies within these countries that produced a representative sample in a specific setting but not on a country level (eg, by including all consecutive patients presenting with presumptive TB to a big reference centre or a certain number of facilities in a given area). Across five studies conducted in Ethiopia between 2015 and 2019, the proportion of resistant TB cases ranged from 4% to 16%.26 33 66 83 124 Jaleta and colleagues found the highest proportion of resistant cases: 16% of all patients with presumptive TB who visited the University of Gondar Hospital TB DOTS between January 2013 and August 2015 had DR-TB, and most resistant cases had been previously treated for TB, suggesting a selection bias in the population seeking care at a referral hospital.66
Three studies were conducted in India. Two studies by Raizada and collaborators examined paediatric populations in four major cities (Chennai, Delhi, Hyderabad and Kolkata) and found a proportion of resistant cases of 10% (95% CI: 7% to 12%) and 9% (95% CI: 8% to 10%), respectively.97 98 In contrast, Das and colleagues detected the lowest prevalence of resistance at 2% (95% CI: 1% to 6%). This study included all patients with symptoms suggestive of TB attending a ‘Designated Microscopy Center of the Capital Hospital in Bhubaneswar, Odisha.50
Discussion
While universal DST is a key component of the End-TB Strategy and a laudable goal,2 the existing literature has several limitations that make it hard to estimate the added yield of universal testing for DR-TB detection compared with only selectively testing high-risk groups. Our analysis did not allow further insights into our primary objective to compare the proportion of resistant cases detected through different testing strategies. This highlights the need for additional comparative data on universal versus targeted DST to inform decisions on implementation strategies.
In the absence of randomised evidence, we found very limited representative data by country or region and only few studies that compared the targeted versus universal testing strategy, indicating that study participants were often preselected, and a true universal DST approach was rarely implemented.
Nationally representative prevalence surveys showed resistance prevalence comparable to WHO estimates.1 For instance, Noeske et al found a 1.6% (95% CI: 0.9% to 2.5%) prevalence of MDR-TB among new bacteriologically confirmed pulmonary TB cases,87 which is equal to what was reported in Cameroon by the WHO.1 In Uganda, Lukoye and colleagues found a proportion of MDR-TB of 1.4% (95% CI: 0.6% to 2.2%) in new cases and 12.1% (95% CI: 6.8% to 19.4%) in previously treated cases.75 This closely approximates figures reported by the WHO in 2018, with the latter reporting a prevalence of 1% (95% CI: 0.91% to 1.2%) and 12% (95% CI: 6.5% to 19%) for new and previously treated cases, respectively. It must be noted that the WHO estimates were for the first time estimated and reported for every country from 2018. However, even within a 10-year period, as is the case for the study in Uganda, we would not expect substantial changes in resistance patterns on a country-wide level.
Other studies that had representative sampling methods in a defined setting reflected the local prevalence and most findings diverged substantially from expected country-specific RR/MDR-TB prevalence obtained from prevalence surveys or estimated by WHO based on national surveillance data.1 Where multiple studies were available for one country, setting-specific prevalence was highest in referral centres (eg, Ethiopia).
Even the four studies that aimed to compare universal versus selected DST had limitations in respect to selection of the population. The most representative study was done in South Africa by Hanrahan et al,60 which most closely approximates the ideal study design to answer our specific research question. In this study, an even higher proportion of resistance was found in the universal testing group, highlighting the importance of systematically assessing the yield of universal testing as opposed to more selective approaches. Such an assessment could potentially give different results in different countries and contexts, reflecting the peculiarities of local TB epidemiology. Yet, all four studies suggested that universal DST would be able to detect a substantial number of additional cases with resistance in non-high-risk groups. Given the scale of persons without risk factors with presumed TB, these could be a substantial driver of the drug-resistant TB epidemic.
Most studies that used a universal DST approach restricted study populations to specific categories of individuals thus narrowing the target of such ‘universal’ testing. While some studies included all presumptive TB cases defined in accordance with international recommendations, often the nature of the testing sites resulted in a selection.125 Others only included sputum-smear positive cases, thus making a preselection of subjects that would eventually have access to DST. This is mostly driven by technical restriction where some tests, for example LPAs, allow for reliable testing only in smear-positive samples.126 Similarly, studies that only involved culture-confirmed TB cases can be misleading because patients may have their sputum or other specimens sent for culture only under selected circumstances, particularly in resource-constrained settings. Thus, testing was not universal, but only representative in subsets of the population and TB cases.
Only studies that utilised WHO-endorsed methods for assessment of drug-resistance were included,3 4 thus differences in methods to assess resistance across studies are unlikely to be a driver of heterogeneity. It should be noted, however, that the diagnostics themselves represent vastly different technologies (for example, LPA has very different capabilities, usage, exigencies and so on as compared with Xpert).
Notwithstanding the inconclusiveness of the evidence about differential yield of universal and selective testing, there is a compelling rationale for integrating routine DST into diagnostic algorithms for all TB cases. Performing DST on all TB cases provides valuable information on the magnitude of the DR-TB problem, and is essential for the evaluation of control interventions, such as drug stewardship, adherence and personalised medicine to improve outcomes.3 4 Furthermore, while high-risk groups might have the largest burden of drug resistance, non-high-risk groups are often larger in size and thus even a lower burden of resistance can reflect a substantial number of resistant cases and thus an important driver of resistance.
However, since substantial resources are necessary to establish and maintain universal DST, more studies on the differential impact and cost-effectiveness would be important. Such information would serve to better inform country-specific guidelines and prioritise effective programmatic interventions and funding allocation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Seye Abimbola
Twitter @svadzianita, @giorgiasulis, @genski_g, @paimadhu, @cdenki
AS and GS contributed equally.
Contributors AS, GS, MP and CMD conceived the study and developed the review protocol. GG built the search strategies in collaboration with AS and GS. AS and GS conducted the study screening, data extraction, quality assessment and analyses under CMD’s supervision. AS and GS wrote the initial draft and contributed equally to all aspects of the paper. All authors revised and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MP is on the editorial boards of BMJ Global Health. Dr Denkinger reports working for FIND until April 2019. FIND is a not-for-profit foundation, whose mission is to find diagnostic solutions to overcome diseases of poverty in LMICs. It works closely with the private and public sectors and receives funding from some of its industry partners. It has organisational firewalls to protect it against any undue influences in its work or the publication of its findings (incl. Cepheid). All industry partnerships are subject to review by an independent Scientific Advisory Committee or another independent review body, based on due diligence, TTPs and public sector requirements. FIND catalyses product development, leads evaluations, takes positions and accelerates access to tools identified as serving its mission. It provides indirect support to industry (eg, access to open specimen banks, a clinical trial platform, technical support, expertise, laboratory capacity strengthening in LMICs, etc) to facilitate the development and use of products in these areas. FIND also supports the evaluation of prioritised assays and the early stages of implementation of WHO-approved (guidance & PQ) assays using donor grants. In order to carry out test validations and evaluations, has product evaluation agreements with several private sector companies for the diseases FIND works in which strictly define its independence and neutrality vis-a-vis the companies whose products get evaluated, and describes roles and responsibilities. Since leaving FIND, Dr Denkinger continues to hold a collaborative agreement with FIND. All other authors declare that they have no conflicts of interest.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. The information used for analysis was obtained from original publications.