Article Text

Abstract
Introduction We aimed to assess the magnitude, temporal trends and socioeconomic disparity in the global burden of tracheal, bronchus and lung (TBL) from 1990 to 2017, using data extracted from the Global Burden of Diseases study (GBD 2017).
Methods We extracted data from the GBD 2017 study. A series of comparative and descriptive analyses of the disease burden between females and males and countries with different socioeconomic development statuses (Social Demographic Index, SDI). We also analysed the temporal trends of age-standardised disability-adjusted life year rates (ASDR) of TBL cancer at the global and super-regional level by means of joinpoint regression. Finally, we also calculated Concentration Index to explore trends of between-country inequality in cancer burden from 1990 to 2017.
Results During the past 27 years, the global incidence of TBL cancer cases and death cases has increased by 100% and 82.3% respectively, but the increase number was mainly influenced by population growth and ageing. After adjustment, from 1990 to 2017, the ASDR of TBL has increased by 3% and the age-standardised death rate has decreased by 7%. The global TBL cancer burden fell by 15.3%. The joinpoint analysis revealed that the overall trend of age-standardised TBL cancer burden for both females and males significantly changed twice between 1990 and 2017, and it varied across countries with different SDI values and was also different between females and males. Age-standardised TBL cancer burden was more concentrated in higher socioeconomic development countries, but the development of healthy inequality showed a downward trend in males while showing an upward trend in females.
Conclusion The magnitude and temporal trends of TBL cancer burden varied across countries and sex. This study highlighted the importance of crafting health policy to adapt to local conditions to manage the global burden of TBL cancers.
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Tracheal bronchus and lung cancer impose a formidable burden worldwide and, although this increasing burden is largely due to population growth and ageing, age-standardised disability-adjusted life year rates are also rapidly increasing in some countries.
What are the new findings?
The global burden of tracheal, bronchus and lung (TBL) cancers in terms of age-standardised rates has declined, but the distribution of TBL cancer burden was uneven, with higher Social Demographic Index (SDI) countries bearing a larger disease burden.
The global burden of the diseases is shifting from higher SDI countries to lower SDI countries.
What do the new findings imply?
The importance of ensuring health policy adapts to local conditions to manage the global burden of TBL cancers.
Introduction
As a highly severe disease, tracheal, bronchus and lung (TBL) cancer has been the focus of governments and healthy organisations.1–3 In recent decades, the global incidence and mortality associated with lung cancer has grown. The reasons are complex, but related with both ageing and population growth, as well as changes in the prevalence and distribution of the main risk factors, along with industrialisation, urbanisation and environmental pollution globally.4 According to the newest version of Global Cancer Statistics, which provides a status report on cancer incidence and mortality with a focus on 36 cancers across 185 countries, lung cancer remained the leading cause of cancer incidence and mortality worldwide, with 2.1 million new lung cancer cases and 1.8 million associated deaths predicted in 2018.5
Apart from the incidence and mortality rate, the disease burden of TBL cancer is also a concern for policy-makers. Disease burden can be quantified by disability-adjusted life years (DALYs), which is defined as the sum of years of healthy life loss due to premature life lost (YLL) and disability (YLD).6 The advantage of the DALY metric lies in its aggregative nature, which enables comparisons of different diseases across time and region. The impact of socioeconomic development on the healthy burden of TBL cancer is complicated. On one hand, increasing disease magnitude is most striking in emerging economies, which is often ascribed to the so-called westernisation of lifestyle. On the other hand, far more complete cancer screening systems and better healthcare resources are available in developed countries.5 7 Thus, countries with higher socioeconomic status may have a higher cancer incidence but longer survival years with cancer.
We assessed whether DALYs owing to TBL cancer was more concentrated in high-income countries, and attempted to determine national-specific trends of the cancer burden based on socioeconomic status. Published studies have revealed little about socioeconomic disparities and gender inequality around the health burden of the disease.8 9 Further, most of these studies are cross-sectional and restricted by the sample size as well as district level design, and thus do not truly estimate worldwide inequality or global cancer trends. Fortunately, a continuously updated global survey, Global Burden of Diseases study (GBD) 2017, provides a systematic review of 359 diseases in 195 countries, including the incidence, prevalence, mortality and health burden of TBL cancers at global, regional, national levels from 1990 to 2017.6 Thus, in this study, we aimed to explore the global and national trends of the TBL cancer burden by using data provided in the GBD 2017.
Methods
Estimation flow of incidence, prevalence, deaths, YLL, YLD, DALYs, population and Social Demographic Index in GBD 2017 study
Global TBL cancer incidence, prevalence death data were estimated from Bayesian hierarchy model, using pooled data obtained from an extensively systematic review at global, regional, national level, and YLLs, YLDs, DALYs number were further calculated based on them with the so-called DISMOD II model.6 10 DALYs were obtained using the following algorithm: DALY number = (Standard life expectancy - Age of death)×Number of death + (Number of prevalent cases×Disability wt).11 In order to remove the influence of population size, crude DALY rate (also known as all ages rates) was calculated by the following algorithm: crude DALY rate=DALY number/population; and the age-standardised DALY rates (ASDR) were obtained by further removing the influence of age structure:

where agei represent the i-th age range with a span of 5 years old. Similar calculation methods were used to calculate crude incidence rates, age-standardised incidence rates (ASIR).10 Social Demographic Index (SDI), as an indicator of national socioeconomic status, is a summary index of total fertility rate of individuals under the age of 25, mean education for those age 15 and older, and lag distributed income per capita.12 The SDI ranges from 0 to 1, with a higher value implying a higher level of socioeconomic development. One hundred and ninety-five countries or territories were further divided into the following five quintiles in the GBD 2017 study based on national SDI value: High SDI quintile, High-middle SDI quintile, middle SDI quintile, Middle-low SDI quintile and Low SDI quintile.
More information about data sources, methodology, estimation flow for incidence, prevalence, death, YLL, YLD, DALY, population and SDI estimation are available in the online supplemental material of the most recent GBD study.12 13
Supplemental material
Data identification and extraction
The 10th version International Classification of Diseases codes C33, C34–C34.92, Z12.2, Z80.1–Z80.2, Z85.1–Z85.20 were mapped to TBL cancer GBD 2017 study. Global, regional, national DALY, YLL, YLD, incidence, prevalence, death data owing to TBL cancer, national SDI value, and global and national population was extracted from the study’s open source database for the years 1990 through 2017 (http://ghdx.healthdata.org/gbd-results-tool).
Descriptive and comparative study
A series of descriptive studies were conducted to evaluate the global and national status, percentage change between 1990 with 2017, and age distribution of TBL cancer. Multiple indicator-level differences by sex and SDI quintiles of TBL cancer were compared. Correlation analysis was used to evaluate the relationship between socioeconomic development with cancer burden, and Spearman’s correlation coefficient ρ was calculated and used to evaluate how good the correlation was due to the non-normal distribution of national SDI value.
Trends analysis
Joinpoint regression programme was used to analyse trends in age-standardised cancer burden. The software describes changes in data trends by connecting several different line segments on a log scale at ‘joinpoints,’ and can identify points where a statistically significant change over time in the linear slope of the trend has occurred.14 The analysis started with the minimum number of joinpoints (eg, 0 joinpoint, which is a straight line), and tests whether one or more joinpoints are statistically significant and should be added to the model. The statistical significance test used a Monte Carlo Permutation method. Furthermore, the annual percentage change (APC) was tested to determine whether it is different from the null hypothesis that the APC is zero. In the final model, each joinpoint indicated a statistically significant change in trends (increase or decrease) and each of those trends was quantitatively described by an APC.15 The average APC (AAPC) was a weighted average of the APCs, with the weights equal to the length of the joinpoint segment.15 To have a summary measure of the trend over the complete study period, AAPC and the related 95% uncertainty interval were also computed for the complete study period (1990–2017). For all analyses, a p<0.05 was considered statistically significant.
Measures of health inequality
We use Concentration Index (CI), which is recommended by WHO,16 to measure the severity of socially economic dimension health inequality. In order to compute CI, all 195 countries or territories were first ranked from the most disadvantaged to the most advantaged according to national SDI values, so that we can get the weighted ranks of each country or territory, which is approximately the ratio of cumulative population to global population (actually, weighted ranks are in the midpoint of each groups). CI is the numerically integrating of the area under the Lorenz concentration curve fitted between the cumulative proportion of DALY number ((national ASDR * national population)/global population, as Y axis) with weighted ranks of each country (as X axis). It ranges from −1 to 1, with a negative (positive) value of the CI means that health burden is more concentrated in countries with low (high) levels of socioeconomic development.16 National population, national ASDR, national SDI and global population data were used to compute the CI. In order to know the trends of the global health inequalities and further compare the gender specific healthy inequality, gender-specific CI in years 1990, 1995, 2000, 2005, 2010, 2015 and 2017 were calculated. After all, Bootstrap method was used to computed the 95% CI of CI.
Patient and public involvement
Patients and the public were not involved in this study.
Results
Temporal trends and multiple index differences of TBL cancer between males and females
The impact of ageing and population growth on both TBL cancer morbidity and mortality has been mentioned in other studies.5 Results here align with this finding, with evidence showing that ageing and global population growth accounted for the dramatic increase in the number of new cancer cases, deaths and disease burden worldwide (table 1 and figure 1B). After removing the influence of population size and age structure, global TBL cancer incidence increased by 3.0%, with 26.3 new cases per 100 000 persons in 1990 vs 27.1 new cases per 100 000 persons in 2017. Mortality dropped by 7%, with 25.5/100 000 in 1990 vs 23.7/100 000 in 2017. Correspondingly, the global burden of TBL cancer in terms of age-standardised rates decreased by 15.3%, from 594.0 per 100 000 in 1990 to 503.1 per 100 000 in 2017. Moreover, the composition of DALYs has slightly.
Multiple index change of TBL cancer from 1990 to 2017

Proportion of risk factors for global TBL cancer in 2017 (A). And the proportions of DALY number increased from 1990 to 2017 attributed to population growth, ageing of the people, decrease of incidence rates and other factors (B). DALY, disability-adjusted life year; TBL, tracheal, bronchus and lung.
changed, with an increasing proportion of YLDs and a decreasing proportion of YLLs. Although YLDs have increased by 9.8% in the last 27 years, it still accounted for less than 2% of the DALYs (table 1). In general, TBL cancer was more severe in males than in females, and they showed different development trends in multiple disease indicators (figure 2C). From 1990 to 2017, the age-standardised incidence, death and DALY rates among males showed a decreasing trend, with the incidence decreasing from 42.5 to 40.0, the death rates decreasing from 41.6 to 35.4, and the DALYs decreasing from 937.6 to 734.1. During the same period, female-specific age-standardised incidence, death and DALY rates showed an increasing trend, with the incidence rising from 13.0 to 16.3, the death rates rising from 12.5 to 14.0, and the DALYs incidence rising from 290.3 to 295.7 (figure 2C1,C3,C6). Although the proportion of risk factors for TBL cancer burden is different between men and women, smoking ranked the first in both of them (62% in males vs 46% in females). Occupational risks caused burden ranked the second in men (14%), while particular matter pollution (18%) ranked the second in women (figure 1A).

Globally, TBL cancer mainly affects people over the age of 40, and higher in males than females at multiple index levels (A1–6). National SDI has no statistical linear relationship with national TBL cancer burden in terms of ASDR at α=0.05 level (B1–6). The persistence of gender inequality in the global incidence, prevalence, deaths, heathy burden of TBL cancer in terms of age-standardised rates from 1990 to 2017 (C1–6). AAPC, average annual percentage change; ASDR, age-standardised DALY rates; DALYs, disability-adjusted life years; SDI, Social Demographic Index; TBL, tracheal, bronchus, and lung; YLD, years lived with disability; YLL, years of life lost.
Globally, TBL cancer mainly affects people over the age of 40, and the cancer incidence, mortality, healthy burden increases rapidly with age. At the age of 80, TBL cancer incidence and mortality reached the peak and then slowly decline among males, whereas incidence and mortality continue to rise after the age of 80 among females (figure 2A1,A3). Males and females showed a similar age distribution in age-standardised TBL cancer burden and, although males bear a much higher burden than females, both males and females reach the peak between the age range of 70–75 and are symmetric distributed (figure 2A6). DALYs were composed of YLDs and YLLs, with YLLs accounting for more than 98% of DALYs, and there was a similar distribution with DALYs, while YLDs could not be displayed on the same scale (figure 2A4,A5).
Joinpoint trends of cancer burden in different SDI quintiles
We use joinpoint regression modelling to estimate the temporal trends of TBL cancer burden in global and different SDI quintiles. During the past 27 years, the global burden of TBL cancer in terms of ASDR decreased by 15.3%, with an AAPC of −0.6% (−0.7, –0.5). However, the trend was not constant; it fluctuated twice. The first joinpoint occurred in 1994, when the global burden of lung cancer shifted from rising to falling rapidly; and the second joinpoint occurred in 2009, when the decline rate significantly slowed (figure 3 global/both). Among males, the global TBL cancer burden showed a similar decreasing trend with total burden, which dropped by 21.7%, with an AAPC of −0.9% (−1.1, 0.6) (figure 3 global/male, table 2); among females, no statistically significant upward or downward trend was observed from 1990 to 2017 (AAPC=0.02%, p<0.05) (figure 3 global/female, table 2).
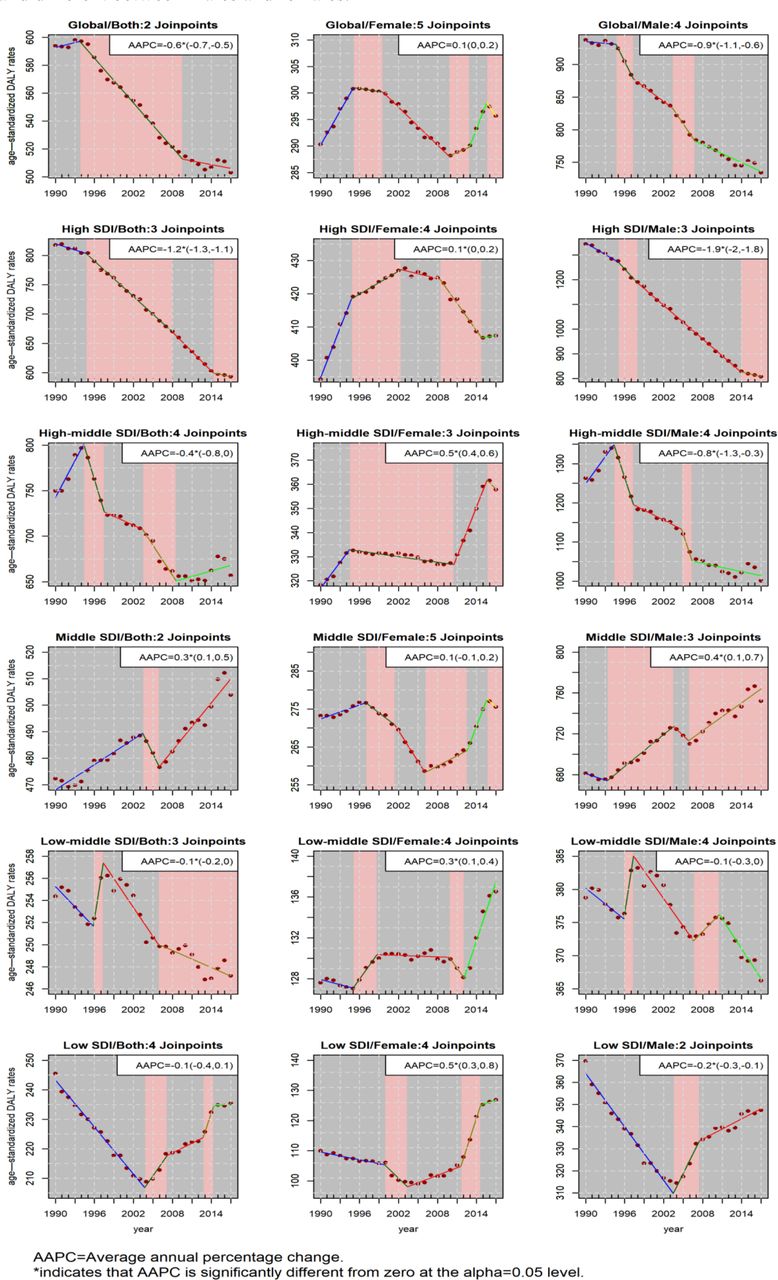
Joinpoint regression results of global, superregional gender-specific age-standardised burden of TBL cancer burden. Temporal trends varied across countries with different SDI values and different between males and females. DALY, disability-adjusted life year; SDI, Social Demographic Index; TBL, tracheal, bronchus and lung.
Joinpoint regression results of global, super-regional gender-specific TBL cancer burden in terms of ASDR in different jointpoint segments
The temporal trend of cancer burden varies among different SDI quintiles, and most of the quintiles showed a decreasing trend. High SDI quintiles rank first with −1.2% of the AAPC, followed by high middle SDI countries (AAPC=−0.4%), low middle SDI quintiles (AAPC=−0.1% (−0.2, 0.0)) and Low SDI countries (AAPC=−0.1% (−0.4, 0.1)). In contrast, middle SDI quintiles showed an increasing trend, with an AAPC of 0.3% (0.1, 0.5) (figure 3, first column). Male-specific TBL cancer burden in different SDI quintiles showed a similar decreasing trend to the total burden, likely because males accounted for most of the burden in each SDI country (figure 3 third column, table 2). Compared with males, the development trend of females has gone through more fluctuations and showed an overall upward trend during the past 27 years (table 2). Based on AAPC value, the quintile rank as follows: low SDI quintile (AAPC=0.5%), high-middle SDI quintile (AAPC=0.5%), low-middle SDI quintile (AAPC=0.3%), middle SDI quintile countries (AAPC=0.1%), high SDI quintile (AAPC=0.1%) (figure 3, second column).
Cross-national health inequality
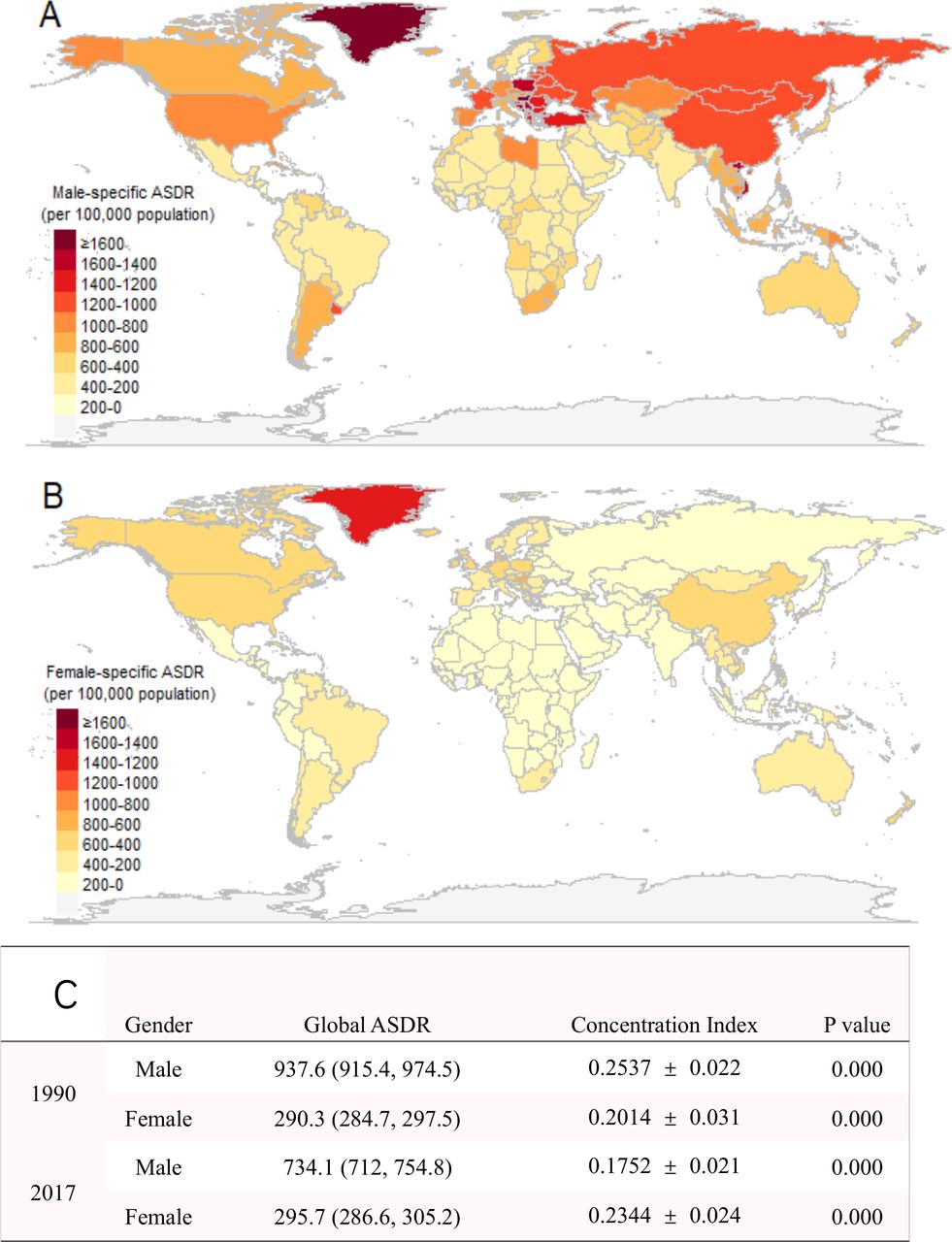
Great disparity in ASDR of TBL cancer was found among 195 countries or territories. In 2017, the most burdened country (or territory) was Greenland, with an ASDR of 1584.9 (1458.6, 1709.4) per 100 000 population, 13 times higher than the least burdened country Malawi, which is 121.9 (103.3, 143.5) per 100 000 population in the same year.Beside that, there are 3/195 country or territories (Hungary, Montenegro, Serbia) with ASDR more than 1000 per 100 000 worldwide, 51/195 country or territories with ASDR more than 500 per 100 000, and 93/195 country or territories with ASDR between 200 with 500 per 100 000, respectively. In addition, gender differences vary greatly at the national level as well. The country (or territory) with the largest absolute gender difference was Georgia, which male-to-female difference was 1153.2 per 100 000 in 2017. But in terms of male/female ratio, Belarus ranked first, with male-specific ASDR 10 times higher than female. However, no matter from the perspective of absolute difference of M/F ratio, Sweden is the country with the smallest gender gap (online supplemental table).
However, the cross-national comparison above is not social economic related. We also conducted a health inequality analysis on the socioeconomic dimension. The correlation analysis showed that in 2017, there was no significant hierarchical correlation between national SDI with national ASDR due to TBL cancer at α=0.05 level (figure 2B1–6). But CI showed a different result. As can be seen in figure 4C, we found a positive CI, both in males and females, at 1990 and 2017 years. This means that TBL cancer burden was unequally distributed and there was more disease burden concentrated in higher SDI countries. Compare 1990 with 2017, 47/195 country or territories showed upward trend, and 148/195 country or territories showed downward trend (online supplemental table). Further, trends of health inequality were as follows: among males, the unfairness alleviated gradually from 0.2537±0.022 (p=0.00) to 0.1752±0.021 (p=0.00); while among females, on the contrary, CI increased from 0.2014±0.031 (p=0.00) in 1990 to 0.2344±0.024 (p=0.00) in 2017.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Global distribution of gender-specific TBL cancer burden in term of national age-standardised DALY rates (ASDR) in 2017 (A,B), and changes of gender-specific cross-national healthy inequality from the perspective of concentration index (CI) compare 2017 with 1990 (C).
Discussion
TBL cancers impose a formidable burden worldwide and, although this increasing burden is largely due to population growth and ageing, ASDR are also rapidly increasing in some quintiles.5 Our results demonstrated that, to some extent, the magnitude burden of TBL cancers were positively related to the countries’ socioeconomic status, and the overall impression of the diminution burden in terms of age-standardised rates masked the huge spatial, temporal and populational disparities. These findings are of substantial import, suggesting that the possible causes for the transfer of global disease burden and successful TBL cancers control strategies must adapt to local conditions. Economic globalisation accelerates the free flow of production factors worldwide, and the risk factors of TBL cancers are shifting and concentrating in lower income countries.4 This pattern, in turn, has resulted in a decreasing burden over the past 27 years in high SDI quintiles and an increasing burden in middle-SDI or low-SDI countries. Moreover, the decline in between-countries health inequalities owing to TBL cancers (measured by CI) not only reflect a narrowing gap related to socioeconomics, but also the transferring of the disease burden.
Tobacco control may be the main reason for the diminishing burden in high SDI countries. A study previously estimated that there is a 20-fold variation in lung cancer incidence rates by region, which largely reflects the maturity of the tobacco epidemic and differentials in the historic patterns of tobacco exposure, including intensity and duration of smoking, cigarette types and degree of inhalation.5 Diminishing smoking prevalence in high SDI countries, including the UK, the USA, Finland, Australia, New Zealand, the Netherlands, Singapore and Germany, followed by a decline of lung cancer rates in the same generations, was first observed in 2000.17 At present, tobacco is more prevalent in developing countries. According to the WHO Report on the Global Tobacco Epidemic 2019, there are an estimated of 1.1 billion smokers worldwide, around 80% of whom live in low-income and middle-income countries. Governments should take more effective measures to reduce the prevalence of tobacco to stop the increasing smoking trends in these countries.
The transfer of environmental pollution may be another reason for the diminishing burden in higher-SDI countries and the rising burden in lower SDI countries. The rise of emerging economies is often accompanied by increasing environmental pollution and long-term exposure to carbon monoxide, nitrogen oxides, ozone, particulate matter air pollution, which are related to increased TBL cancer risk.18 19 The economy of high-middle SDI countries, such as China, began to accelerate in the last 20th century, and a corresponding peak in TBL cancers was observed at the same time. With the improvement of environmental quality, the disease burden now shows a corresponding downward trend. Similar patterns occur in low-SDI to middle-SDI countries, when high-polluting industries further transfer to to less developed areas.
Our research reveals that a great difference between male and female in the incidence, prevalence, mortality and disease burden due to TBL cancer had been existing during the past 28 years. This result is consistent with published literature, those men bear larger TBL cancer burden than women.4 8 Apart from the differences in genetic background and hormone secretion between male and female, the great difference in smoking prevalence may be the main reason that caused the disparities.20 21 The general increasing trend of a female-specific burden is particular noteworthy, even though it accounts for less than 1/3 of the total TBL cancer burden. Compared with males, the female-specific burden experienced more complex fluctuation trends, and showed a bigger socioeconomic inequality. Smoking ranked the first among all causes for female-specific TBL cancers and became increasingly popular among females, which may be the main reason for the increasing burden in this group.22 23 Furthermore, the socioeconomic inequality associated with the female-specific TBL cancer burden is consistent with the idea that economic development and social-cultural processes related to gender empowerment have affected the diffusion of smoking in different ways for females.24 Passive smoking and environmental pollution, especially indoor environmental pollution, also cause a considerable proportion of TBL cancer burden.20 25 However, more information is need to assess the relationship between the change of trends and the prevalence of risk factors in global and different SDI countries.
One published study which focuses on the same topic has discussed the uneven distribution of the incidence, death and DALY number of TBL cancer from the perspective of geography, SDI quintiles and genders.13 In order to further quantify the inequality and described the situation improved or not, we quantify the healthy inequality from the perspective of socioeconomic-related or non-socioeconomic-related dimension by CI and gini coefficient, and further found that, compare 2017 with 1990, the severity of healthy inequality decreased in males while increased in females. In addition, the published study has developed a method, which is different from us, to quantify the trends of the disease from 1990 to 2017, but did not find the turning point as it regarded the past 27 years as a whole.
It is worth mentioning that the development trend was not consistent between ASIR with ASDR in TBL cancer during the past 27 years. As estimated in GBD 2017 study, global ASIR increased by 3% while the ASDR decreased by 15.3% compare 2017 to 1990. This contradictory result may reflect both the spread of risk factors and the progress of protective factors, especially the popularity of early lung cancer screening and the emergence of lung cancer targeted drugs, which had further extending the average life expectancy of patients.21 26
The GBD 2017 study has some key limitations, including statistical assumption and data sources, which have been described in detail elsewhere.6 27 Due to using aggregate data at the national level instead of at the district level, bias might come from geographical variations in DALY estimates. Though a global view of socioeconomic inequality in TBL cancers burden has been provided in this study, the conclusions may not applicable to a specific district. Given the availability of annual updates to the GBD study, the long-term trends in socioeconomic disparity in global burden of TBL cancers, as a reflection of health policy effectiveness, could be further explored.
In summary, this study revealed that the global burden of TBL cancers in terms of age-standardised rates has declined, but the distribution of TBL cancer burden was uneven, with higher SDI countries bearing a larger disease burden. Countries with different socioeconomic statuses shared a different TBL cancer development trend. It appeared that in recent years, ASDR caused by TBL cancer in high-SDI countries have been decreased while the burden in low-SDI countries is still increasing, which may be related to the prevalence of tobacco in low-income countries and the global transfer of high polluting enterprises.19 28 29 Males had a higher disease burden than females, but the general increasing trend of TBL cancers among females was notable. These findings may raise public awareness on the huge socioeconomic disparities in TBL cancers. Because TBL cancers are among the deadliest diseases, prevention is far more important than treatment for the management of the global TBL cancers burden. This study highlights the importance of ensuring health policy adapts to local conditions to manage the global burden of TBL cancers.
Acknowledgments
We thank International Science Editing (http://www.internationalscienceediting.com) for editing this manuscript.
References
Footnotes
Handling editor Sanni Yaya
ZW and LH contributed equally.
JZ and JZ contributed equally.
Contributors ZW wrote the manuscript. JL analysed the data. JZh conceived the study and provided guidance. All other authors contributed to the analysis and reviewed the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All data is publically available. Data are available on request.