Article Text

Abstract
Background Contextual factors, especially where people live, has been linked to various health outcomes, therefore, there is an increasing focus on its implication for policies and implementation of health interventions. Polygyny is a widespread practice in sub-Saharan Africa that also reflects socioeconomic and sociocultural features. This study investigated the association between polygynous context and risk of undernutrition.
Methods Recent Demographic and Health Surveys involving 350 000 mother–child pairs from 32 sub-Saharan African countries conducted between 2010 and 2018 as of March 2020, were analysed using relevant descriptive and 3-level multilevel logistic regression modelling. Undernutrition among under-5 was defined as underweight, stunting and wasting using the WHO Multicentre Growth Reference Study. Odd Ratio (OR) at 95% credible interval was used to report the associations.
Results The prevalence of contextual polygyny varied widely across the 32 sub-Saharan African countries, the lowest (0%) found in one of the regions in South Africa and the highest (52%) in one of the regions in Uganda. Underweight, stunting and wasting were lowest in Uganda (3.5%, 9.3%–1.27%, respectively), stunting was highest in Mozambique (37.1%) while wasting was highest in Niger (7.7%). Furthermore, the results showed that the contextual prevalence of polygynous practice exacerbates the risk of underweight (1.003 (0.997–1.008)) and wasting (1.014 (1.007–1.021)) among under-5 children, even when gender inequality and sociodemographic indicators were adjusted for. Polygyny was negatively associated with stunting though not significant; multiple births had the strongest and positive association with the risk of undernutrition among under-5 children in sub-Saharan Africa.
Conclusions This study further corroborates the strong influence of contextual factors on health outcomes—which is undernutrition in this study. In addition to specific interventions aimed at reducing the prevalence of undernutrition, broader strategies that will address contextual issues are required.
- child health
- health policy
- nutrition
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Undernutrition remains a major public health issue in many parts of sub-Saharan Africa.
Evidence has shown that contextual factors influence health outcomes, and sometimes, they have greater impact than individual-level factors in shaping health outcomes.
What are the new findings?
Contextual prevalence of polygyny is significantly associated with risk of underweight and wasting among under-5 children.
Socioeconomic development and cultural norms are the likely underlying factors for the observed associations.
What do the new findings imply?
In order to effectively tackle underweight and wasting in sub-Saharan Africa, multifaceted interventions aimed at improving socioeconomic development and equality, especially those linked with polygyny, should be prioritised.
Background
Improving the health and well-being of under-5 children has been one of the long-standing global health priorities, especially during the Millennium Development Goal era1–3 and the current Sustainable Development Goals (SDGs). Besides, child nutrition and growth have remained some of the most popular fields in maternal and child health research and policymaking, both in health and development dimensions.4 Evidence has shown over the years that early development of children, especially within the first 5 years of life, has short-term and long-term impacts on health and development in adulthood.4 5 Increased susceptibility to infectious diseases and non-communicable diseases, and cognitive development have been linked to early-stage development, thus, there are emphases on nutrition and growth during these critical periods.6–8
Undernutrition is the term used to describe an individual who is unable to maintain good health and well-being due to insufficient intake of energy and nutrients.9 10 Different indicators and proxy measures are being used to assess and measure nutritional status in research. However, the most commonly used ones are the anthropometric measures such as weight, length in combination with age and sex.11 12 Currently, undernutrition is estimated to contribute nearly 45% of death among under-5 children globally; with about 155 million stunted and 52 million wasted.9 10 The impact of undernutrition is more pronounced in low-income and middle-income countries especially in South Asia and sub-Saharan Africa. According to the most recent estimates by the WHO, more than one-third and one-quarter of children that experience stunting and wasting, respectively, live in Africa.9 13–15 Furthermore, undernutrition is largely a medical and social disorder, therefore, its causes are multifaceted. Poor dietary intake, poor hygiene, infections and diseases that affect children, food insecurity, economic deprivation, and other social and cultural norms have been identified as direct and indirect causes of undernutrition in children.16–18
Meanwhile, the concept of polygyny and how it is linked to health and development outcomes have been in the literature for a while.19–24 Polygyny is when a man marries more than one wife at the same time; it is a common feature in many sub-Saharan African countries.25 26 The implication of this practice for individuals and children in such unions has been explored, especially for children, where significant health and nutritional deficiencies have been observed. Survival disadvantage is, therefore, phenomenal among children from polygynous families.23 27–29 One of the underpinning theories that has been used to explain the link between child health outcome and polygynous families is dilution and scarcity of resources in setting where such are usually practised.24 29
Previous researches have shown that settings in which polygyny is predominantly practised are usually different from where it is seldomly practised in terms of demographics, sociocultural and socioeconomic parameters.22 30 31 Existing literature on the short-term and long-term implications for children that grew up in polygamous family has treated polygyny as an individual or at most family characteristics. In the real sense, the concept and practice of polygyny transcend beyond individual or family characteristics; the practice is deeply rooted in sociocultural norms and constructs and dominant in settings where this is popularly practised.30–33 Therefore, the contextual prevalence of polygynous practice may also be useful to understand the pattern of undernutrition in settings where it is commonly practised.
In this paper, considering the interlinkage between contextual prevalence of polygyny, sociocultural and economic factors, we hypothesised and tested the following hypotheses: first, that undernutrition is positively associated with the contextual prevalence of polygyny irrespective of individual family structure. Second, indicators for sociocultural and socioeconomic development will explain this association. Third, we also hypothesised that the prevalence of contextual polygyny will constrain the risk of undernutrition between families practising polygyny and monogamy.
Methods
Study design
This study is based on secondary dataset from the Demographic and Health Surveys (DHS) of 32 African countries conducted between 2010 and 2018. DHS is national representative data on demographic, environmental, socioeconomic, nutritional and health indicators from about 90 low-income and middle-income countries. Identical data are usually collected across all countries with very high response rates, 98% on average. Consequently, the datasets can be easily matched and used suitably for multilevel analysis across multiple countries.
The sampling approach used by DHS across all countries involves three-stage stratified cluster design. DHS uses the existing sampling frame in each country, usually the census enumeration, stratifies them either by geographical regions or urban and rural, and randomly select clusters with probability proportional to size of household listing. Finally, 20–30 households are randomly selected from the clusters; face-to-face interviews are conducted with family heads and eligible women to collect data on their birth history and other relevant data. Details of the data collection procedure have been published elsewhere.34
Data collected are based on recall by household heads and women. The dataset used for this study was limited to births that occurred within 5 years to the most recent survey. As this helps us to reduce possible recall error, this step is also important because of our outcome variables; underweight, stunting and wasting as indicators for undernutrition. The dataset used for this study consisted of 315 751 mother–child pairs within 5 years preceding the survey (see table 1 for detailed information on countries, survey year and key variables used in this study) The flow chart as required by Strengthening the Reporting of Observational Studies in Epidemiology is in figure 1 and the checklist is included as supplemental material.
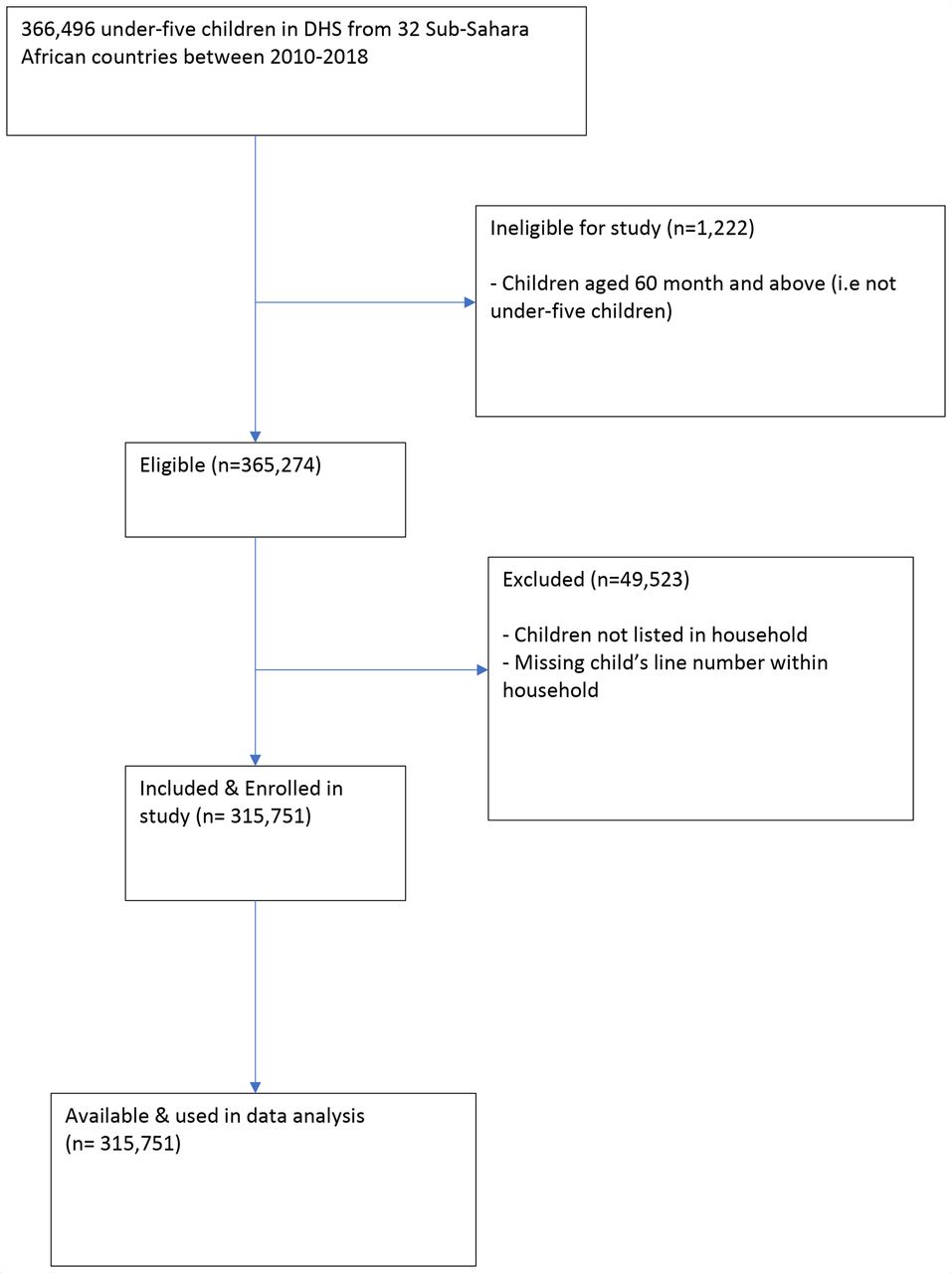
The Strengthening the Reporting of Observational Studies in Epidemiology flow chart. DHS, Demographic and Health Surveys.
Brief description of regional-level variables
Outcome variable
Following the WHO Multicentre Growth Reference Study—which provides a single and comparable standard for the description of children’s (under 5 years) physiological growth,35 underweight children were categorised as weight-for-age z-score below −2 SD with stunt children categorised as height-for-age z-score below −2 SD. Also, children whose z-score of weight-to-height was less than −2 SD from the median of the WHO reference group were categorised as experiencing wasting. Therefore, underweight, stunting and wasting were defined as a binary outcome; a child takes a value of 1 if z-scores are below −2 SD and 0 if otherwise.
Determinant variables
Based on our hypotheses, polygyny was the key determinant variable in this study. Therefore, subnational regions, which are usually political, administrative and geographical districts, as defined by each country, were used as a contextual unit of focus in the multilevel analysis. Using the child-recode dataset, aggregate (%) of women’s report of each regional-level variable was computed as explained in table 1.
Individual-level variables
The key individual-level variable in this study was family structure because of its link to the third hypothesis of our study; it was computed from three questions from the surveys. Mothers were asked about their marital status (currently married, divorced, separated, widows and never married). Currently married women were subsequently asked if they were cowives and finally, all unmarried women were asked if they were cohabiting. These responses were used to compute family structure. In addition to this, a set of robust individual (mother and child) level standard variables, informed by previous undernutrition research, were included as controls. Mother’s level variables included completed years of education by mother; mother’s wealth factor as constructed by the DHS; if the mother is a Muslim or not and age at birth of the focal child. The child’s level variables included preceding birth interval, gender, birth order and if a child is the first-born or not.
A cross-level interaction variable was computed using the regional prevalence of polygyny with family structure; this was to operationalise the third hypothesis; to test if the contextual prevalence of polygyny conditions the relationship between family structure and undernutrition as measured by underweight, stunting and wasting. Finally, we also controlled for country-specific variables such as study year and Human Development Index (HDI).
Statistical analyses
Descriptive analyses were conducted involving both dependent and independent variables; they were presented in percentages and means as shown. We applied household weight to the dataset to account for over or under sampling, and to make the data representative of each country. Missing responses were less than 5% and were removed from the analysis. A box plot was used to graphically show the variation in regional prevalence of polygyny across the 32 sub-Saharan African countries as shown in figure 1. By leveraging the hierarchical nature of our dataset, multivariable multilevel logistic regression was used to examine and test our hypotheses (see equation I).
logit (Dtijk)= β1Xijk + β2Yjk + β3Zk+uj + νk
Dtijk is the odd that an under-5 child (I) in a family (j) in region (k) experienced undernutrition (measured by underweight, stunting and wasting). Xijk is the child-level covariates, Yjk is the family-level covariates and Zk is the regional-level covariates, uj is the random effect at family-level and νk is the regional-level random effect.
Prior to the multilevel analysis, we assessed multicollinearity with the Variance Inflation Factor (VIF). In the multilevel analysis, we built six different logistic models to test our hypotheses systematically; a 3-level model for binary outcome reporting undernutrition (as underweight, stunting and wasting) was specified in each model. Model I was an empty model that is, without any independent variable; this allowed us to ascertain if the variance at family (level 2) and subregional (level 3) level is significant. Model II was specified to examine the relationship between the contextual prevalence of polygyny and undernutrition (as measured by underweight, stunting and wasting) while controlling family structure and the control variable. In models III and IV, we included socioeconomic development indicators (rurality and access to electricity) and regional-gender inequality, respectively, to examine how they affect model II. Model V involved a combination of the variables in models III and IV. Finally, in model VI, which also was the full adjusted model, we included the cross-level interaction variables between family structure and contextual prevalence of polygyny while country-level variables (study year and HDI) were included in the adjusted variables.
OR at 95% credible interval was used to report the associations between the variables. We also explored measures of variation using the intraclass correlation, also called variance partition coefficient (VPC). This allowed us to measure the percentage of undernutrition in sub-Saharan Africa related to family or regional level factors. All the analyses were performed using the ‘runmlwin’ command in Stata36 and using the Bayesian Markov Chain Monte Carlo procedure.
Patient and public involvement
Patients and the public were not involved in the design and conduct of this research.
Results
Descriptive
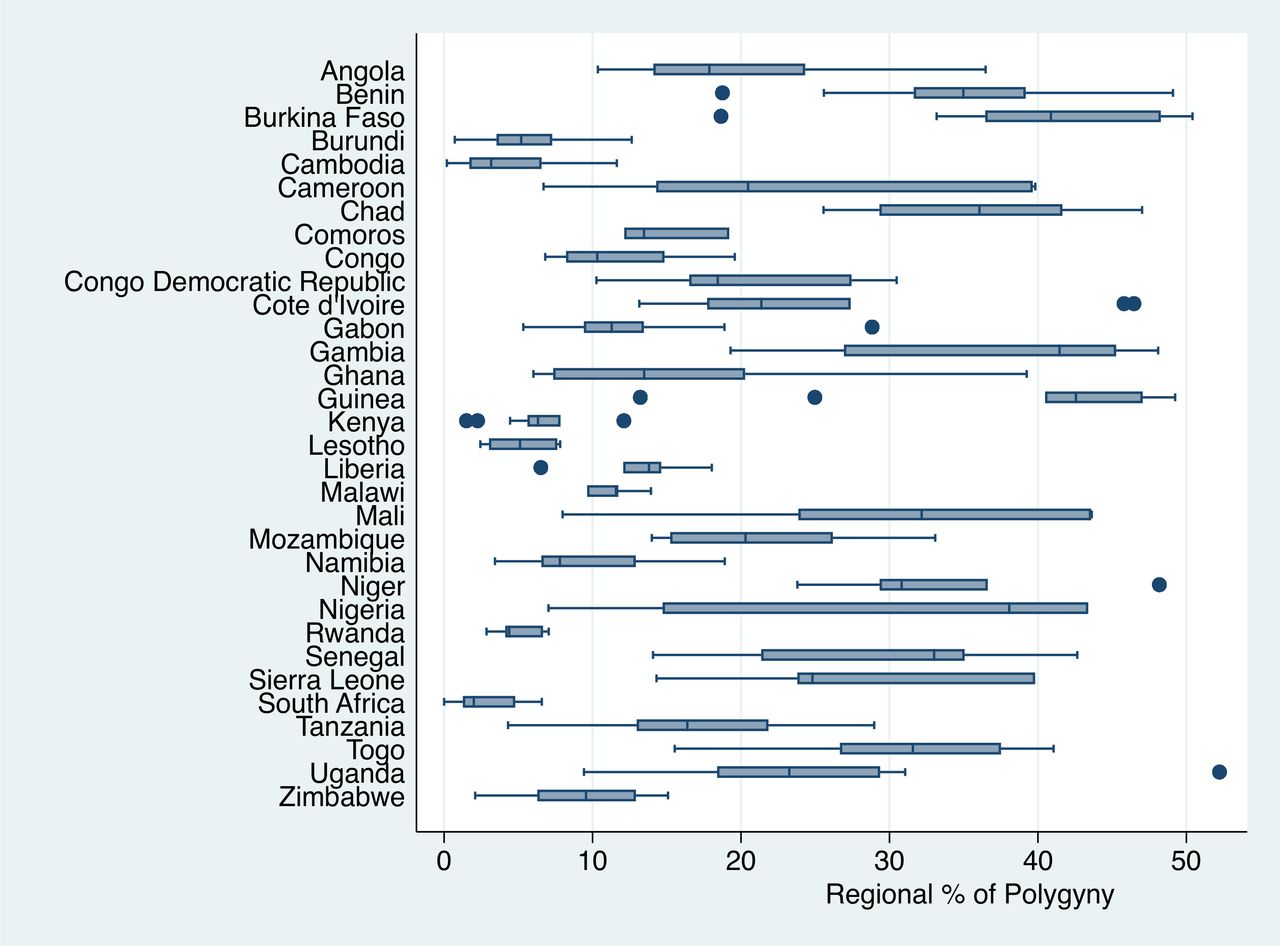
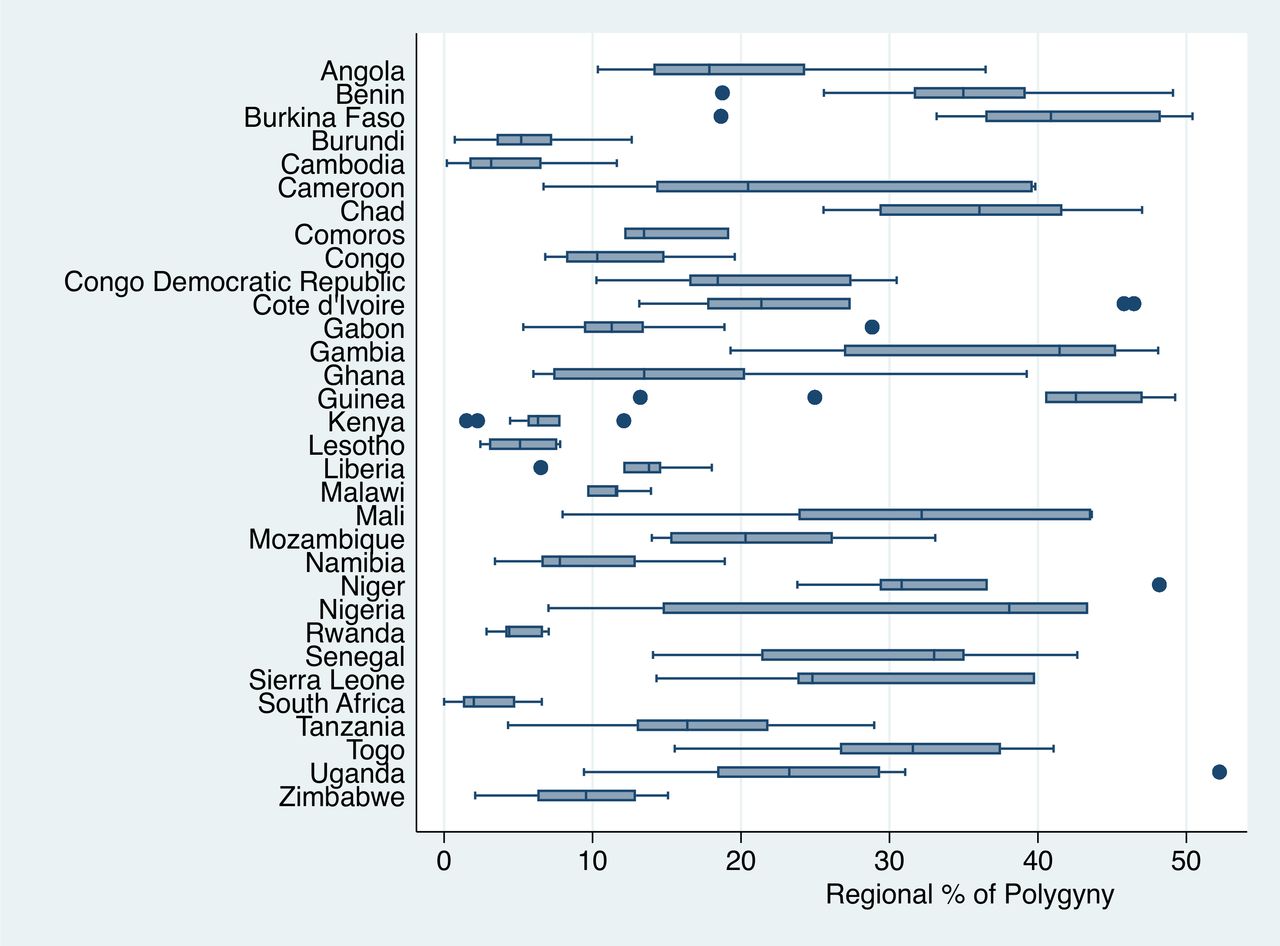
The analyses involved 315 751 mother–child pairs (level 1), ranging from 2685 in Lesotho to 28 818 in Nigeria. Of the 315 751 under-5 children, 32 755 (10%) were underweight, 60 513 (19%) were stunted and 13 699 (4.3%) were wasted. Table 2 shows the individual country’s contribution to this prevalence. As shown in figure 2, there was wide variation in the prevalence of polygyny in sub-Saharan African countries. Countries such as Cameroon and Mali had about 7% regional prevalence of polygyny in one region and as high as about 40% in another region.
{kind=link}
{kind=link}
Distribution of contextual percentage of women in polygyny across the 32 sub-Saharan African countries.
Description of DHS data by countries, survey year and percentage of undernutrition indicators
Further descriptive characteristics (at individual, family and country-level) of under-5 were presented in table 3. From the pooled sample, the average prevalence of women in polygynous union by region was 22.2%, most of the mother–child pairs lived in rural regions (69.6%) and monogamous families (52.4%). Only a few had access to electricity (28%), and approximately 20% lived in polygynous families. Mother–child pairs characterised by contextually poor socioeconomic development indicators and gender inequity were more concentrated in highly polygynous settings (see table 3). In these contextual differences, family structure, household size, maternal age at birth and maternal wealth were functions of the prevalence of polygyny.
Descriptive statistics with the pooled sample of characteristics of DHS data in sub-Saharan Africa
Multilevel analysis
Tables 4–6 provide estimates from the multilevel logistic regression models on the risk of undernutrition. In model I from each table, there were significant variations in the regional prevalence of underweight (1.584 (1.467–1.709)), stunting (1.43 (1.352–1.515)) and the highest regional variance in wasting (1.637 (1.504–1.782)) across the subnational region.
Multilevel analysis result on the risk of underweight among under-5 children in sub-Sahara
Multilevel analysis result on the risk of stunting among under-5 children in sub-Sahara
Multilevel analysis result on risk of wasting among under-5 children in sub-Sahara
Model II across the three tables aimed to test the first hypothesis with undernutrition. When individual family structures and sets of control variables at family and child levels were adjusted for, under-5 children living in regions with a higher prevalence of polygyny were significantly more likely to experience undernutrition. Each unit increase in regional prevalence of polygyny was associated with 0.7% increased risk of underweight (p<0.01) and 1.4% increased risk of wasting (p<0.001). The association in stunting was not significant.
Models III and IV examined the second hypothesis. We found that contextual socioeconomic development indicators explain the relationship between undernutrition and contextual prevalence of polygyny. As an extension from model I, we observed a reduced strength of association between underweight (from 0.007 to 0.005) and contextual prevalence of polygyny but increase for wasting (from 0.014 to 0.015). Also, the relationship between the contextual prevalence of polygyny and underweight was attenuated (from 0.007 to 0.006) when gender inequality was controlled for in model IV; similar observation was made with wasting (from 0.014 to 0.013). When the indicators for both gender inequality and socioeconomic development in model V were simultaneously adjusted, an increased risk of underweight (although insignificant) was found, while the strength of association remained the same for wasting.
The fully adjusted model (model VI) included an interaction term while simultaneously controlling for all other variables including study year and HDI. The results showed that at the inclusion of the interaction term, the increased risk of underweight and wasting observed among under-5 children from polygynous family became negative (0.954 (0.833–1.092) and 0.799 (0.645–0.989), respectively). In addition, we found a positive interaction between the contextual prevalence of polygyny and family structure. Under-5 children in polygynous families (vs monogamous) in regions with low (1%) prevalence of polygyny will have 4.6% reduced risk of underweight and 20% reduced risk of wasting. On the other hand, under-5 children from regions with a high prevalence of polygyny (52%) will likely experience 27% and 36% increased risk of underweight and wasting, respectively.
Concerning stunting, the first hypothesis was null, as the prevalence of polygyny was negatively associated with stunting; so other hypotheses were not explored (see table 3). Finally, we found that some family and child-level variables are independently associated with the risk of undernutrition as measured by underweight and wasting. Under-5 children born as twins had the strongest relationship with both underweight (138%) and wasting (75%). Also, children from higher wealth quartile households had a 52% lower risk of underweight and 29% decreased risk of wasting. Furthermore, children born to mothers under 20 years were more than 10% likely to experience underweight and 41% more likely to experience wasting. Also, female children were less likely to experience underweight and wasting. The multicollinearity test revealed that none of the independent variables were highly correlated (VIF mean=1.35, maximum=1.53, minimum=1.31). Finally, according to the VPC, 22.8%, 21.9% and 25% of variation in underweight, stunting and wasting could be attributed to regional-level factors while, 40.8%, 44.1% and 42.5% were attributed to family-level factors.
Discussion
The overarching aim of this study was to investigate the contextual prevalence of polygyny in 32 sub-Saharan African countries and its association with increased risk of undernutrition as measured by underweight, stunting and wasting—based on the WHO’s classification. We found compelling evidence that showed that contextual prevalence of polygyny is strongly associated with undernutrition in sub-Saharan African countries and this association was influenced by socioeconomic and sociocultural indicators.
In the descriptive result, wide variations in the regional prevalence of polygyny across sub-Saharan Africa was reported. Countries such as South Africa, Burundi, Cambodia, Rwanda and Malawi had the lowest and smaller variation in regional prevalence of polygynous practice. Guinea, Burkina Faso and the Gambia had the highest (with average above 40%). Countries such as Nigeria, Mali and Cameroon were sub-Saharan African countries with the widest variation in regional prevalence of polygyny (see figure 2). Previous research on the prevalence and distribution of polygynous marriage in Africa has reported similar findings. Polygyny belt was the term used to describe the regions of Africa (spanning from Senegal to Tanzania) with the highest prevalence of polygyny by one of the early researchers on the practice of polygyny in Africa.22 More recent studies37 38 have similarly reported wide variation in the practice in Africa with Guinea as the highest.
Similarly, the prevalence of undernutrition varied across the 32 sub-Saharan African countries included in this study. While the prevalence of stunting was found to be highest among these measures (table 2), countries such as Senegal, Burkina Faso and Mali had a high prevalence of these three measures. Conversely, Namibia, Uganda and Mali were countries with the lowest averages. The most recent estimate of nutrition in the WHO Africa region also supports some of these findings.15 39 One-third and one-quarter of the global prevalence of under-5 stunting and wasting are attributable to Africa; the recent estimate also showed that it is only in Africa that the prevalence of stunting has increased.13 The findings have enormous implications on the prospects for Mali, Senegal and Burkina Faso to achieve SDG-2 by 2030. As such, much concerted effort may be required from the central government and partner organisations to review existing child nutrition policies and incorporate family structure responsive measures.
We found that the contextual prevalence of polygyny is associated with increased risk of undernutrition (underweight and wasting); decreasing but insignificant association was observed in stunting of under-5 children. Previous studies have established link between living in polygynous families and child health outcomes, however, with more focus on child mortality.29 38 40 41 Studies have also reported that being born into polygamous families increases the likelihood of nutritional deficiency among under-5 children.28 42 43 These studies corroborate the result of this study as about 4.0% increased risk of underweight and about 2.0% increased risk of wasting were observed among under-5 children that grew in polygynous families. The findings suggest that overcoming undernutrition is sometimes beyond the capacity of households. Thus, investment in agriculture and expanding economic spheres of households through employment opportunities backed by commitment by leadership at the country level can facilitate the mitigation of undernutrition in sub-Saharan Africa.44 45 Adoption of horizontal approach45 whereby policies and programmes are implemented at community level, may be much beneficial.46 The horizontal approach helps to implement nutrition health promotion programmes and boost agricultural supply while accounting for the sociocultural peculiarities of communities.
Furthermore, we found contextual socioeconomic disadvantage (rurality and access to electricity) and social norms (gender inequalities) to explain some of these associations, especially for underweight. The practice of polygyny is usually rooted in sociocultural beliefs and norms. It is common in socioeconomically deprived settings with features such as rurality, low educational level and lack of improved water and electricity.29 31 33 37 Therefore, our findings linking regional prevalence of polygynous practice to undernutrition could be underpinned by the fact that the practice is common in socioeconomically deprived areas and other sociocultural constructs that might encourage polygyny.30 31 However, one of the findings from the study is that stunting has a negative association with the contextual prevalence of polygyny. The recent estimate by the WHO reported that Africa is the only region where stunting was increasing; from 50% to 60% between 2000 and 2016. This is projected to further increase by another 17% before 2050.13 40
As social development marked by urbanisation, migration, increased women’s education, reduced agrarian and declined patrilocal contexts occur across African countries, we expect that polygyny and its implication on child health outcome will subsequently attenuate. This suggests that there might be other family and contextual factors such as feeding practices or cultural norms surrounding child upbringing that facilitate the increasing prevalence of stunting in sub-Saharan Africa. We acknowledge that our analyses might not fully capture socioeconomic development indicators and contextual norms that might be drivers for stunting. One of our previous studies showed an insignificant association between stunting, as an indicator for malnutrition, and Gross Domestic Product.46 It is also noteworthy to mention that there are discussions on the misuse and inadequate sensitivity of stunting to accurately measure short-term nutrition deficiencies especially in low-resource settings.12 45 47
When we included a cross-level interaction term between the regional prevalence of polygyny and family structure, our findings showed that the increased risk of undernutrition associated with under-5 children from polygynous families disappeared and switched to a negative association. More importantly, we found that the difference in elevated risk of undernutrition between polygamous and monogamous families was amplified in settings where polygyny is predominantly practised; 7-fold and 11-fold risk of underweight and wasting, respectively.
It is noteworthy that undernutrition is multifaceted and affected by a number of factors. For sub-Saharan Africa to overcome undernutrition, this study has pointed to the need for governments and nutrition-inclined organisations in sub-Saharan Africa to motivate households, especially polygynous households to consume nutritious meals. To achieve this, sensitisation programmes at the household levels may be required. Although contextual and other forms of variations exist between and within countries, the mass media, especially radio can be used to reach the masses with undernutrition education. This strategy may be effectual because evidence indicate that radio has a wide coverage and is commonly used across sub-Saharan Africa.47 48 Moreover, the health sectors can collaborate with local government authorities to fashion culturally sensitive undernutrition programmes to conscientise the populace about the repercussion of undernutrition and the need to ensure childhood nutrition.
Strengths and limitations
This study involved large datasets from about 350 000 mother–child pairs from 32 sub-Saharan African countries. The DHS data are usually nationally representative; therefore, findings from such analyses allow generalisability. Also, we were able to assess undernutrition using the three commonly used indicators: underweight, stunting and wasting. Although data quality concerns for anthropometric measures in the DHS data have been raised in the past when compared with National Nutrition Survey. DHS is readily available and more importantly, it provides the richest socioeconomic context, central to our study. Furthermore, we used a Bayesian approach to compute estimates in our model. On the one hand, DHS data are based on a cross-sectional design, therefore, associations observed do not mean causality. Also, the data were from surveys ranging from 2010 to 2018; thus, indicating limitation on the comparability of our data. The survey year from each country was different, however, we controlled for it in our multilevel analysis.
Conclusions
The contextual prevalence of polygyny is associated with underweight and wasting risk of indicators for undernutrition except for stunting. Polygyny at the contextual level has proven to be a major determining factor of undernutrition in sub-Saharan Africa. Efforts to end undernutrition in sub-Saharan Africa need to prioritise family structure of children. This emphasises the impact of contextual factors in tackling undernutrition problem in sub-Saharan Africa. The study underscores the need for governments of sub-Saharan Africa to situate undernutrition interventions within contextual parameters as well. These efforts may accelerate the prospects of sub-Saharan African countries in achieving SDG-2 which seeks to achieve zero hunger by 2030. For African countries to achieve SDG-2, more research should be carried out on drivers for stunting in sub-Saharan Africa.
Acknowledgments
The authors thank the MEASURE DHS project for their support and for free access to the original data.
References
Footnotes
Handling editor Seye Abimbola
Twitter @aosanjorin, @edward_ameyaw, @vkchattu, @@realSanniYaya
Contributors SY contributed to the study design and conceptualisation. SSA and SY wrote the first draft of the article and analysed the data. OAU, EKA, BOA, VKC, GB, A-AS and EKMD provided technical support and critically reviewed the manuscript for its intellectual content. SY had final responsibility to submit for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests SY is an editorial board member of this journal.
Patient consent for publication Not required.
Ethics approval DHS conforms to the US Department of Health and Human Services regulations for the respect of the rights of human subjects. Additionally, Institutional Review Boards (IRBs) of partner organisations in each of the 32 countries reviewed and approved the survey protocols. Since the data were publicly accessible, no further ethical approval was required for our study. Details about data and ethical standards for DHS are available at: http://goo.gl/ny8T6X.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data for this study were from the Demographic and Health Surveys (DHS) and available here: http://dhsprogram.com/data/available-datasets.cfm.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.