Article Text

Abstract
Background Effective maternal service delivery for adolescent mothers is essential in achieving the targets for maternal mortality under the Sustainable Development Goals. Yet little is known about levels of maternal service coverage in adolescents compared with adult mothers.
Method We used data from 283 Demographic and Health Surveys or Multiple Cluster Indicator Surveys for 105 countries between 2000 and 2019 to estimate the levels and trends of inequality in coverage of five maternal health services between adolescent girls (aged 15–19) and adult mothers (aged 20–34), including receiving four or more antenatal care visits, delivering with skilled birth attendants and receiving a postnatal check-up within 24 hours of delivery.
Results We analysed data from 0.9 million adolescent girls and 2.4 million adult mothers. Using the most recent data, we found adolescent girls had poorer coverage across all indicators, with receipt of four or more antenatal care visits 6.5 (95% CI 6.3 to 6.7) percentage points lower than adult mothers, delivery with skilled birth attendants 3.6 (95% CI 3.4 to 3.8) lower and having a postnatal check-up within 24 hours of delivery 3.2 (95% CI 2.8 to 3.6) lower. The coverage was 54.2% (95% CI 53.9 to 54.5) among adolescents for four or more antenatal care visits, 69.7% (95% CI 69.4 to 70.0) for delivery with skilled birth attendants and only 30.0% (95% CI 29.3 to 30.7) for receiving a postnatal check-up within 24 hours of delivery. Country-specific coverage of the maternal services increased over time in most countries, but age-related differences persisted and even worsened in some, particularly in the Western Pacific (eg, Vietnam, Lao, Cambodia and Philippines).
Conclusion Even though their pregnancies are of higher risk, adolescent girls continue to lag behind adult mothers in maternal service coverage, suggesting a need for age-appropriate strategies to engage adolescents in maternal care.
- maternal health
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Girls aged 15–19 years constitute 15% of the female population of reproductive age and account for more than one in ten global births.
To achieve the Sustainable Development Goals target of reducing the maternal mortality rate to less than 70 per 100 000 live births by 2030, adolescent girls are a priority group.
What are the new findings?
The latest data suggest that less than two-thirds of mothers aged 15–34 years old received four or more antenatal care visits and had their initial visit in the first trimester; less than three-quarters of adolescent mothers delivered in health facilities and with a skilled birth attendant; and only 30% received a postnatal check within 24 hours of childbirth.
For all types of maternal services, adult mothers were better covered. The difference between adult and adolescent mothers was especially large in antenatal care.
Although most countries made progress in maternal care coverage between 2000 and 2019, the differences between adult and adolescent mothers persisted and even worsened in some countries, particularly evident in the Western Pacific (eg, Vietnam, Lao, Cambodia and Philippines).
What do the new findings imply?
Adolescents continue to lag behind adult mothers in maternal service use. More efforts (eg, adolescent friendly maternal care, comprehensive education, increased media exposure) are needed to develop age-appropriate strategies to engage adolescents in maternal care.
Introduction
Although maternal mortality ratios have dropped by 45% worldwide across the Millennium Development Goals (MDGs) era, progress was insufficient in many countries to reach the MDG target of reducing maternal mortality by three quarters between 1990 and 2015.1 With the Sustainable Development Goals (SDGs), a more ambitious target has been set to reduce the maternal mortality rate to less than 70 per 100 000 live births by 2030.2
Girls aged 15–19 years old are 15% of the female population of reproductive age3 and account for more than one in ten global births with 95% of these occurring in low-income and middle-income countries (LIMCs).4 5 Maternal conditions are the second leading cause of death among adolescent girls worldwide, with earlier work suggesting a slightly higher risk of death among adolescents 15–19 years old relative to mothers aged 20–24 years old.6 For these reasons, adolescent mothers will remain a priority group in the SDGs era.
Most available analyses of country-level data have not considered age stratification, resulting in a limited understanding of the effects of age on maternal care. Three peer-reviewed age-disaggregated studies of antenatal and delivery care used single data years and covered 21 sub-Saharan African (SSA), 13 west African, and a mixture of 15 developing countries from Asia, Latin America, and Africa, but the findings were inconclusive.7–9 The Countdown group reported the coverage of antenatal and delivery care by maternal age in Countdown countries (75 countries where more than 95% of all maternal deaths occur), but it did not analyse the changes in inequality between adolescents and adult mothers over time.10 The current paper uses household survey data from 105 countries between 2000 and 2019 to provide by far, the most comprehensive picture of levels and trends in antenatal, delivery and postnatal care coverage among adolescents (15–19 years old) and adult mothers (20–34 years old).
Method
Data source
Data were drawn from the Demographic and Health Surveys (DHS) and Multiple Indicator Cluster Surveys (MICS). Our study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines. DHS and MICS allow for direct comparison as their survey design and implementation quality are sufficiently similar across countries and over time.11 DHS and MICS usually use a two-stage stratified cluster sampling approach, with the selection of geographically defined units such as villages in the first stage, followed by the selection of specific households or persons to be interviewed in the second stage.12 13
For each sampled household, women aged between 15 and 49 years were surveyed regarding their maternal service use during the 3 years before the survey, including antenatal care, delivery care and postnatal checkups. We followed previous practice7 and limited our analysis to births within the 3 years before the surveys to mitigate recall bias and enhance data comparability. Because previous studies show that birth order is an important determinant of maternal service use,14 15 we included only first births in our analysis.
Following previous work, we defined adolescent mothers as those 15–19 years old and adult mothers as those 20–34 years old.7 With our focus on primigravidas, we did not include mothers aged 35 and older, given that more than 90% of these mothers are multiparas, particularly in LIMCs7 16; for all countries with available data since 2010, both the mean and the median of age at first birth were 20 years old, with IQR between 17 and 22. We used data from 283 DHS or MICS surveys for 105 countries between 2000 and 2019. Our analysis involved a total of 928 736 adolescents and 2 412 973 adult mothers.
Maternal service indicators
We adopted the following indicators to consecutively and comprehensively cover the continuum of pregnancy and childbirth: (1) receiving four or more antenatal care visits during pregnancy from a skilled provider such as doctor, nurse, midwife and auxiliary nurse/midwife; (2) delivery with skilled birth attendants including physician, nurse and midwife, either in a health facility or at somewhere else (eg, at home); and (3) receiving a postnatal check-up within 24 hours of delivery from any type of health provider, including a skilled provider, community health worker or traditional birth attendant. Receiving four or more antenatal care visits and delivery with skilled birth attendants have been widely adopted as service indices in previous studies.7 8 14 15 Given that almost half of postnatal maternal deaths occur within 24 hours of delivery, receiving a postnatal check-up within 24 hours is a further important indicator of coverage.17
In addition to the above three indicators, we also analysed the timing of the first antenatal visit and delivery in a health facility, with the findings in the online supplementary appendix.
Supplemental material
In November 2016, the WHO issued a new series of recommendations for a positive pregnancy experience which included the timing of first antenatal care to before 12 weeks of gestational age,18 and the indicator has been widely adopted.7 8 Delivery in a health facility has also been closely monitored in previous studies.7–9 Therefore, we also investigated age-related differences in these two indicators.
Measurements of inequality
We adopted two commonly used inequality measurements.19 Absolute inequality refers to the difference in service coverage between adult and adolescent mothers. A value larger than zero indicated that coverage was higher among adult mothers than adolescents. Relative inequality was defined as the ratio in maternal service coverage between adult mothers and adolescents. A value larger than one means that maternal service was greater among adult mothers.
Statistical analysis
Our study examined maternal service coverage and inequality at the aggregate and the country levels. For analyses at both the aggregate and country levels, we assessed maternal service coverage in the two age groups and age-related inequalities between them using the latest DHS/MICS since 2010. For analyses at the country level, we also tracked the changes in coverage and inequalities over time for countries with available data in multiple survey years.
Among the 105 countries involved in the study, 87, 87 and 52 countries collected data on four or more antenatal care visits, skilled birth attendants and postnatal checkups within 24 hours of delivery, respectively, in 2010 or afterwards (see table 1). For each country, we generated point estimates of service coverage for each age group following the DHS/MICS guidelines,20 21 taking into account sampling weight, clustering and stratification variables.22 Then we calculated the difference and ratio measures based on the levels of coverage among adolescents and adult mothers. Consistent with previous studies,23 24 we generated SE for service coverage and inequality using bootstrap method by drawing 1000 samples.
Estimates of overall levels of maternal service coverage, levels by maternal age and absolute inequality between the two age groups, using the most recent available survey data since 2010 for 105 countries*
For trend analysis at country level, we excluded countries with the latest and the earliest surveys less than 5 years apart, so that we ensured a decent timeframe between the two surveys. We identified 59, 70 and 32 countries with trend data on four or more antenatal care visits, skilled birth attendants and postnatal check-ups within 24 hours of delivery respectively. We generated point estimates, inequalities and their 95% CI for each country in both survey years using the same method as in the latest estimates above. We investigated whether the coverage and inequality changed significantly between the surveys using a bootstrap test, drawing samples from each of the two survey years and estimating the difference between the means of the two samples, repeating the process for 1000 times to generate the p value for the difference in means.25 As the number of years between the two rounds varied across countries, we also calculated the annual rate of change as the total change in absolute inequality divided by the number of years between the two surveys. We used STATA (V.14.2) for all analyses. We ascertained statistical significance with 95% CI.
This study used publicly accessible secondary data and obtained an Institutional Review Board (IRB) exemption from the IRB at Harvard.
Patient and public involvement statement
Neither the patients nor the general public were involved in the design of this study.
Results
Aggregate-level coverage and inequality of maternal services since 2010 (latest available surveys)
Table 1 presents the maternal service coverage and age-related differences. For all mothers aged 15–34 years old, 59.4% (95% CI 59.2% to 59.5%) had four or more antenatal care visits; 72.5% (95% CI 72.3% to 72.7%) delivered with skilled birth attendants; and 32.7% (95% CI 32.4% to 33.0%) received a postnatal check-up within 24 hours of delivery. Coverage for all indicators was greater in countries with a higher income level and was also higher among non-sub-Saharan African (non-SSA) countries or non-Countdown countries.
For all maternal service indicators, absolute inequality between adult mothers and adolescents indicated that adult mothers fared better than adolescents. Receiving four or more antenatal care visits had the largest absolute inequality by age at an average of 6.5 (95% CI 6.3 to 6.7) percentage points. Absolute inequalities for delivery with skilled birth attendants and receiving a postnatal check-up within 24 hours of delivery were 3.6 (95% CI 3.4 to 3.8) and 3.2 percentage points (95% CI 2.8 to 3.6), respectively. The results were consistent across all regions, income groups, SSA categories and Countdown categories.
Results on the timing of receiving first antenatal care and delivery in a health facility are presented in online supplementary appendix table 2, which were similar to the results on four or more antenatal care visits and delivery with skilled birth attendants. Relative inequalities showed consistent results (online supplementary appendix table 3).
Country-level coverage and inequality of maternal services in the latest surveys since 2010
Of the 87 countries with available data on four or more antenatal care visits since 2010, there were 19 countries with coverage greater than 90% among mothers 15–34 years old. These 19 countries were scattered along different regions, income groups and Countdown categories. The coverage was significantly higher among adult mothers in 63 countries across different categories (regions/income groups/Countdown), including four of the five studied Western Pacific countries (Cambodia, Lao, Philippines and Vietnam). Vietnam had the largest absolute inequality of 22.1 percentage points (95% CI 21.2 to 23.0) in 2013. Four countries had coverage significantly higher among adolescents, including Albania, Algeria, Iraq and Tajikistan (online supplementary appendix table 4 and figure 1A). Similar findings were found in mothers receiving their first antenatal care in the first trimester (online supplementary appendix table 5 and online supplementary appendix figure 1A).
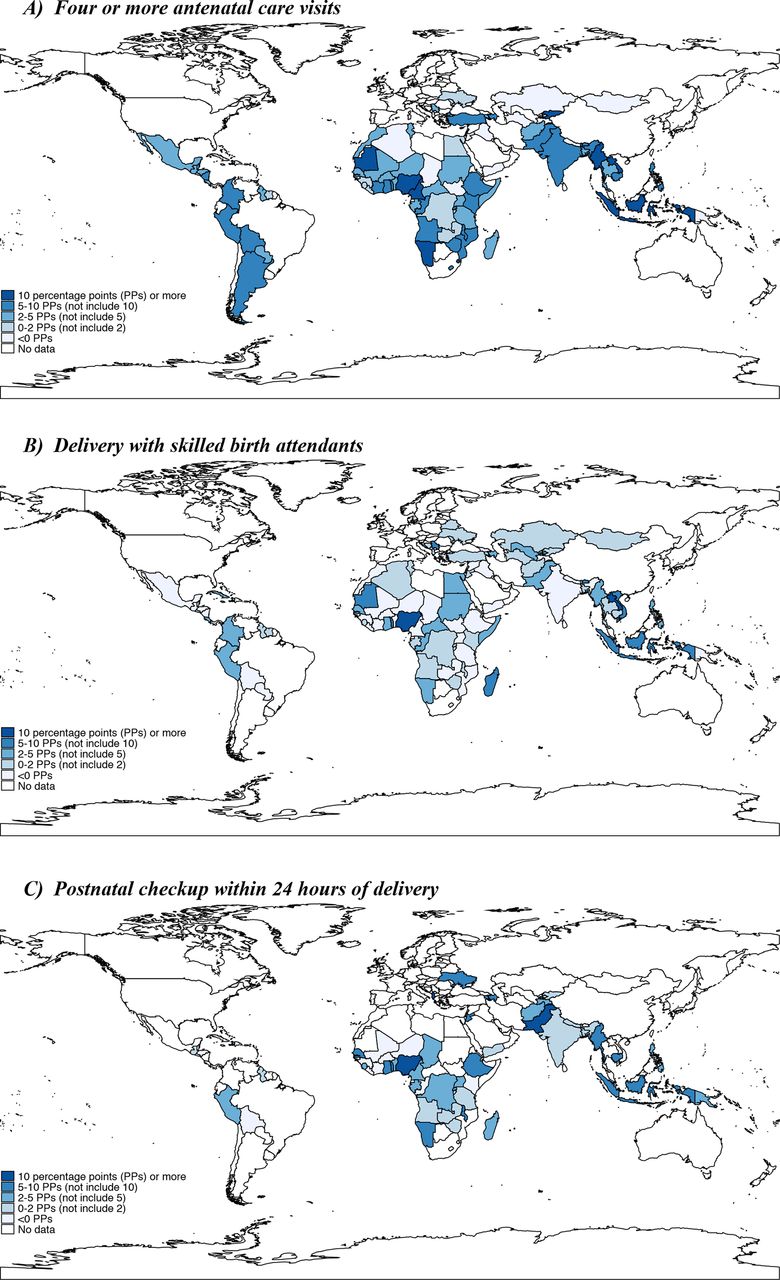
Absolute inequality in maternal service coverage between adolescent mothers 15–19 years old and adult mothers 20–34 years old for the most recent years of data available. (A) Four or more antenatal care visits. (B) Delivery with skilled birth attendants. (C) Postnatal check-up within 24 hours of delivery. Data sources: Demographic and Health Surveys and Multiple Indicator Cluster Surveys).
Among the 87 countries with data available on delivery with skilled birth attendants, there were 36 countries with coverage among mothers 15–34 years old greater than 90% in the latest years, which were scattered along various regions, income groups and Countdown categories. Four countries, all low-income countries in SSA, had a coverage of less than 30% (Chad, Ethiopia, Niger and South Sudan). There were 33 countries with delivery by skilled birth attendants significantly greater among adult mothers, including four of the five studied Western Pacific countries (Cambodia, Lao, Philippines and Vietnam). Age-related service gaps were most notable in Nigeria (16.1 percentage points (95% CI: 15.3 to 16.9)), Laos (11.6 percentage points (95% CI 9.9 to 13.3)) and Indonesia (9.9 percentage points (95% CI 9.4 to 10.4)). Twenty countries had greater delivery by skilled birth attendants among adolescents: all were Countdown countries and none were located in the Western Pacific (online supplementary appendix table 6 and figure 1B). We found a similar pattern in the coverage of delivery in a health facility (online supplementary appendix table 7 and online supplementary appendix figure 1B).
Among the 52 countries with available data on whether mothers received a postnatal check-up within 24 hours of delivery, the coverage in the latest year among mothers 15–34 years old was greater than 90% in only one country (Peru). There were eight countries from different regions, income groups and Countdown categories with coverage less than 30%. There were 29 countries across different categories with a significantly higher proportion of adult mothers receiving a postnatal check-up within 24 hours of delivery than adolescents, including both of the studied Western Pacific countries (Cambodia and Philippines). Burkina Faso, Congo, Honduras and Maldives were the only countries with significantly greater coverage among adolescents (online supplementary appendix table 8 and figure 1C).
The results using relative inequality were largely consistent with those for absolute inequality (online supplementary appendix figure 2).
Country-level coverage and inequalities in maternal service over time
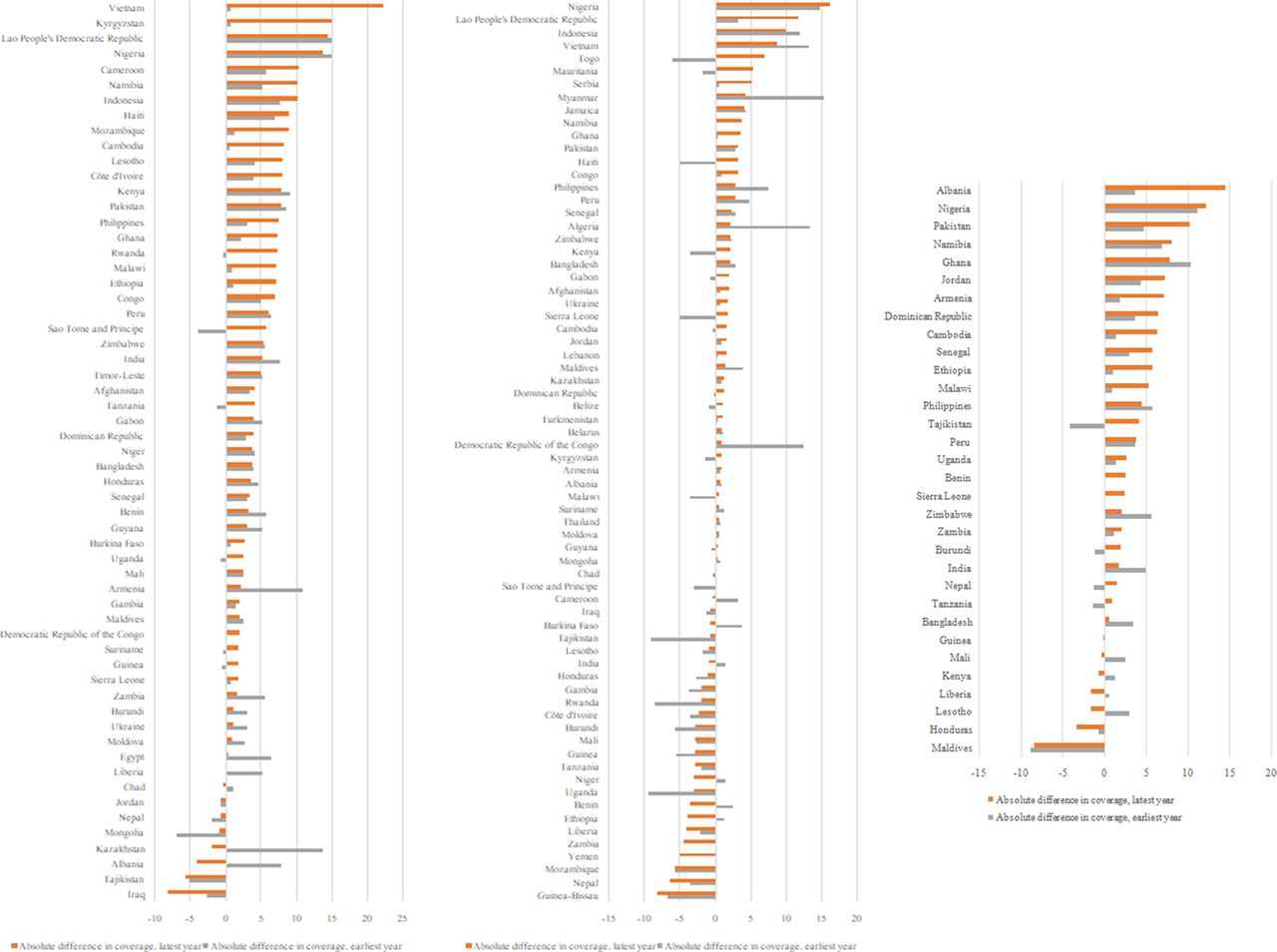
Among the 59 countries with available data for receiving four or more antenatal care visits in multiple rounds, 33 countries across different regions, income groups and Countdown categories increased their coverage among mothers 15–34 years old by more than 10 percentage points. By contrast, coverage in seven SSA countries fell by more than five percentage points (Guinea, Benin, Malawi, Tanzania, Zambia, Senegal and Namibia) (online supplementary appendix table 4). Twelve countries (eight in Africa, one in Europe and three in the Western Pacific) had significantly greater absolute inequality by age emerge over time, mostly due to a faster increase in the coverage of four or more antenatal care visits among adult mothers. Five countries (Albania, Armenia, Egypt, Kazakhstan and Liberia) had significantly reduced inequality, due to greater increase in coverage among adolescents. Tajikistan was the only country where the coverage of four or more antenatal care visits was significantly higher among adolescents in both survey rounds (online supplementary appendix table 9 and figure 2A). We found generally similar results on receiving first antenatal care in the first trimester (online supplementary appendix tables 5‒10).
{kind=link}
{kind=link}
Absolute inequality in percentage points in maternal service indicators between adult mothers and adolescents, latest data versus earliest data. (A) Four or more antenatal care visits. (B) Delivery with skilled birth attendants. (C) Postnatal check-up within 24 hours of delivery. Data sources: Demographic and Health Surveys and Multiple Indicator Cluster Surveys.
Among the 70 countries with available data on skilled birth attendants, 36 countries from various regions, income groups and Countdown categories increased skilled birth attendants coverage by more than 10 percentage points, while Benin, Senegal and Myanmar had skilled birth attendants coverage reduced by more than 5 percentage points (online supplementary appendix table 4). The inequality enlarged in three countries (Lao, Mauritania and Serbia) as adolescents increasingly lagged behind adult mothers. Six countries (Algeria, Burkina Faso, Democratic Republic of the Congo, Myanmar, Philippines and Vietnam) had reduced inequality, mainly due to greater improvements in adolescents (online supplementary appendix table 11 and figure 2B). Similar findings were found in the coverage of delivery in a health facility (online supplementary appendix tables 5‒12).
Of the 32 countries with available data on whether a woman received a postnatal check-up within 24 hours of delivery in multiple survey rounds, 21 countries across different categories had an increase in coverage over time by more than 10 percentage points, while three countries (Armenia, India and Senegal) had the coverage decreased by more than 5 percentage points (online supplementary appendix table 6). Six countries (Albania, Armenia, Cambodia, Ethiopia, Malawi and Pakistan) had absolute inequality increase between the two age groups mainly due to greater improvements in adult mothers. None of the countries analysed had the absolute inequality by age in the coverage of receiving a postnatal check-up within 24 hours of delivery significantly reduce over time (online supplementary appendix table 13 and figure 2C).
Discussion
We used 283 national household surveys from 105 countries to provide a comprehensive picture of age-related differences in maternal service coverage since the commencement of the MDGs. We found that less than two-thirds of mothers received four or more antenatal care visits and had a first antenatal visit in the first trimester; around three-quarters of mothers delivered in health facilities and with a skilled birth attendant; but only one-third of mothers received a visit within 24 hours of childbirth. Adolescents fared less well in all studied maternal service indicators than adult mothers. At the country level, we found most countries had made remarkable progress in maternal care coverage across the MDGs era, but adolescents were still lagging behind adult mothers in most countries. Age-related differences in coverage were particularly evident in the Western Pacific (eg, Vietnam, Lao, Cambodia and Philippines). Over time, the differences in coverage by age not only persisted but even increased in many countries.
High-quality antenatal and delivery care are particularly important for adolescent mothers given their higher rates of iron deficiency anaemia and pre-eclampsia, as well as other comorbidities and complications of delivery compared with adult mothers.26–28 We found that even in countries where there had been remarkable progress in service coverage (eg, Cambodia, Laos), adolescents continue to face barriers to antenatal and delivery care. These may arise from limited financial resources, limited access to healthcare facilities, lack of knowledge or poorer quality of maternal services in rural areas where adolescent pregnancies are more prevalent.4 6 Sociocultural norms may be a further contributor—pregnant unmarried adolescents are likely to face social stigma or even judgemental attitudes from health workers.29–31 In some places, married adolescents living in traditional extended family arrangements may have limited power to make their own decisions about antenatal care and the place of delivery.29
The finding of low rates of postnatal care among both age groups is consistent with previous reports.32 33 Postnatal care is neglected in many developing countries with its significance not well recognised until 2014 when WHO explicitly recommended that a mother and her newborn should receive a visit within 24 hours of the birth.34 This neglect has led to poor provision and quality of postnatal care, particularly in rural areas.17 35 Families tend not to return for postnatal care visits if antenatal and/or delivery care was poor,36 37 raising the possibility that improving antenatal care coverage and quality may promote better use of postnatal care.
This study has some limitations. First, we were only able to include 105 developing countries with available data. The estimates were therefore not representative at the global, regional or income group levels. With more data available in the future, the aggregate-level analysis could be strengthened. Second, all maternal service indicators were self-reported and so subject to misreporting. Moreover, mothers may not be able to distinguish skilled birth attendants from traditional, raising a possibility of misclassification and misspecification of coverage. Third, our study is limited to descriptive analysis of the age-related inequalities in maternal service coverage. Socioeconomic determinants of inequalities are not the focus of this study, but will be addressed in the future. Fourth, our study only focused on service coverage, not the quality of services provided.
Adolescents have the potential to benefit from broader interventions in maternal care as well as age-targeted initiatives. Previous studies have demonstrated that task shifting to community health workers (CHWs) has been a cost-effective strategy to address geographical barriers and shortages in health workers, particularly in rural and disadvantaged populations.38 39 It is essential that such CHWs are provided with the necessary training for engaging with adolescents including the adoption of non-judgemental perspectives and a capacity to maintain confidentiality in consultations. Financial instruments can also encourage use and service provision in poorer, rural areas, with potentially great benefits in younger mothers who commonly come from poorer households. Burundi, for example, removed user fees for all pregnant women and the policy was found to promote coverage of maternal services for both adolescent and adult mothers.40
Designing age-specific interventions could also increase maternal service coverage. Tajikistan introduced a series of laws on reproductive health as well as national strategies for youth health. The country scaled up a Youth Friendly Service by integrating it into an extensive network of reproductive health and dermato-venerology centres.41 Our study found a high adolescent coverage of maternal care in Tajikistan and reductions in inequality compared with adult mothers over time. Interventions such as education of adolescent mothers and their partners, training of health workers on adolescent friendly maternal care, increased media exposure and providing greater household income are also likely to promote coverage of maternal care for adolescent mothers.42 43 Such examples highlight a need for further study on the effectiveness of financial actions including extended health insurance and removal of user fees for young and poor mothers. There is also a need to engage with young mothers to develop and test adolescent targeted interventions, including those around adolescent health literacy, stigma and lack of knowledge about maternal care services.44
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Handling editor Sanni Yaya
Contributors ZL and CL conceptualised the analysis, developed the analysis plan. ZL conducted data analysis under CL’s supervision. ZL wrote the first draft of the report. ZL had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. All authors interpreted findings, critically reviewed the report for important intellectual content, contributed to manuscript writing, and approved the final version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. All data is publicly available via the links of https://dhsprogram.com/data/available-datasets.cfm and http://mics.unicef.org.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.