Article Text

Abstract
Introduction Our study aimed to identify factors that influence access to eye care and eye health outcomes for remote Indigenous Australians living with diabetes.
Methods In collaboration with Indigenous Community-Based Researchers (CBR) and Aboriginal Community Controlled Health Services (ACCHS), a qualitative, participatory action research approach was taken, drawing on Indigenist and decolonising methodologies. The study was undertaken in four remote communities, in the Katherine region, Northern Territory and north-western New South Wales, Australia. Interviews and focus groups were undertaken with Indigenous adults aged ≥40 years living with diabetes (n=110), and primary care clinicians working in ACCHSs (n=37). A series of interviews with CBRs (n=13) were undertaken before and after data collection to add cultural insights and validation to participant accounts. Data were analysed inductively using grounded theory, in-depth discussion and NVivo V.11.
Results More than one-third of all patients had little to no knowledge of how diabetes affects eye health. Limited access to health information and interpreters, language barriers, distrust of health providers and services, and limited cultural responsivity among non-Indigenous clinicians, were identified as determining factors in eye health and care.
Discussion We outline a need to address gaps in trust and communication, through increased access to and resourcing of Indigenous language interpreters and cultural brokers, understandable and culturally sensitive diabetic eye health information and cultural responsivity training for non-Indigenous clinicians. Centring Indigenous cultures in healthcare practice will enable a shared understanding between clinicians and Indigenous patients, and subsequently more equitable eye health outcomes.
- eye diseases
- diabetes
- health systems
- public health
- qualitative study
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Vision and impairment and blindness among Indigenous Australians is largely preventable and treatable, yet uptake of primary and tertiary eye care remains fragmented.
What are the new findings?
Our study presents a novel analysis of Indigenous patient perspectives specifically related to diabetic eye health.
Culture, communication and trust are key determinants of access to and uptake of eye care, and prevention of diabetic eye diseases.
What do the new findings imply?
Our findings highlight the need for increased health promotion activity to be undertaken in Indigenous language speaking communities: through access to Indigenous interpreter services, and translation of key health promotion messages targeting diabetic retinopathy.
Shared health knowledge can help bridge the communication gap, support Indigenous patients to make informed health decisions and enable culturally safe access to eye care services.
Introduction
Aboriginal and Torres Strait Islander (hereafter Indigenous) Australians collectively experience some of the worst health outcomes globally.1 The difference in health and socioeconomic outcomes between Indigenous and non-Indigenous Australians is often referred to as ‘the gap’, reflecting inequities that continue to persist at unacceptable levels.2 Chronic diseases, including type II diabetes, account for 70% of Indigenous deaths, and three-quarters of the gap in mortality rates between Indigenous and non-Indigenous Australians.2 National population health data (2014) show one in three (38%) Indigenous Australian adults over 55 years reported having diabetes (recorded HbA1c >6.5%), a rate 25% higher than non-Indigenous Australians.3 Furthermore, rates of diabetes and chronic kidney disease are noticeably higher in very remote areas compared with other regions.4
The high prevalence of diabetes among Indigenous adults is associated with a risk of developing vision impairment.5 Vision impairment and blindness are three times higher among Indigenous when compared with non-Indigenous Australians, with 90% of conditions being preventable or treatable.6 The two leading causes of blindness among Indigenous Australians include cataract (40%) and diabetic retinopathy (20%).6 Diabetes is associated with an approximate twofold increase in cataract detection rates,7 with previous studies noting glycaemic control as an associated risk factor.8 Diabetic retinopathy remains asymptomatic until later stages, reinforcing the need for annual screening and early intervention to prevent irreversible vision loss. Despite this, only 33% of Indigenous adults with diabetes undergo eye screening within the recommended time frames.9
A 2016 national survey reported cataract surgery coverage rates among Indigenous Australians (61.4%) were significantly lower than coverage rates among non-Indigenous Australians (87.63%)6 (p 19). Outreach services in rural and remote Indigenous communities are limited and therefore attendance rates are an important factor to achieve guideline targets.10 Issues related to low attendance of ophthalmic treatment, such as fear of cataract surgery,11 inadequate patient information and coordination, and poor approachability of public hospitals,12 suggest the need for improved access to eye care services. There is little evidence detailing Indigenous patient perspectives of diabetic eye health and care, including the sociocultural influences that impact access, uptake of treatment and attendance to eye care services.
Data were collected as part of a broader research project named the Patient Experience in Eye Care study,13 which was undertaken in close collaboration with Aboriginal Community Controlled Health Services (ACCHS) in the Northern Territory (NT) and New South Wales (NSW), Australia. ACCHS are governed by an Indigenous board, and aim to deliver holistic and culturally responsive primary health services that are primarily managed and provided by Indigenous staff. Culturally responsive care can be defined as an extension of patient-centred care that includes paying particular attention to social and cultural factors in managing therapeutic encounters with patients from different cultural and social backgrounds.14 The study aimed to understand factors influencing accessibility and uptake of ocular treatment, and eye health outcomes for remote Indigenous Australians living with diabetes. To explore the broader influences on health inequity and their sociocultural and structural determinants, factors both internal and external to health systems were analysed. This article focuses on diabetes and related eye diseases, and the way health literacy, cultural perceptions of health and illness, and trust have an impact on informed decision-making and clinical outcomes; however additional aspects that are not reported here were also explored as part of the broader study.
Methods
A detailed account of the methodology is documented elsewhere,13 however, a summary is provided here for context. The study was undertaken in four rural communities, two in the Katherine Region, NT, and two in north-western NSW; and was grounded in the principles of Indigenist15 16 decolonising,17 and participatory action research (PAR)18 methodologies. PAR methods originated in emancipatory movements of resistance, agency and political contestation to colonisation,19 and incorporate theories of community empowerment highlighted by scholars such as Paolo Freire20 and Frantz Fanon.21 Working within such principles aimed to privilege the voices, experiences and lives of Indigenous people and sought to place Indigenous interests, experiences and knowledge at the centre of the research approach.15 The study used qualitative methods and was conducted over four phases: (1) community consultation and design of methods, (2) interviews and preliminary analysis, (3) design and conduct of focus groups based on the results of phase 2, and (4) report back of findings to the ACCHS in each community.
Patient and public involvement
Nine Indigenous community members collaborated as Community-Based Researchers (CBR) on the study (including co-authors TF, GB and RS). CBRs contributed to the design of the study and data collection tools, recruitment of participants, conduct of interviews and focus groups, translation of Indigenous language transcripts to English, collaborative analysis of data and report back of findings to ACCHSs and community members. CBRs provided valuable cultural insights to the research findings. As PAR methods focus on change through understanding history, culture and local context,18 an important part of the research process involved using participant data and CBR insights to develop strength-based strategies to overcome identified concerns. These strategies were shared with participating ACCHSs at the end of the study via a presentation by CBRs and a site report, with the aim of improving access to eye care services for Indigenous patients. Furthermore, patient perceptions from phase 2 were used to shape focus group discussion guides used in phase 3. Patients were not directly involved in the initial study design.
Setting and sample
Participants comprised two groups: Indigenous patients aged 40 years or more with a clinical diagnosis of diabetes, and primary care clinicians working in ACCHS. Purposive sampling using data from a file audit conducted within the ACCHS in each community22 was used to recruit patients. Purposive sampling was also used to recruit clinicians who were involved in primary, chronic disease, or eye care within the ACCHS.
Data collection and analysis
Participants took part in either an interview or a focus group or both, all of which were conducted face to face. Patient interviews explored experiences accessing eye care services and eye health knowledge. One specific interview question asked patients to explain their understanding of how diabetes affects eye health, a subsection of which forms the focus of this article. Clinician interviews explored perceptions regarding barriers and enablers to diabetic eye care. Focus groups gave the opportunity to further explore themes identified in earlier interviews. Two of eight patient focus groups were conducted in an Indigenous language. Separate male and female patient focus groups were conducted to respect gender-sensitive social norms in Indigenous cultures. Recorded interviews and focus groups were transcribed and, where necessary, translated to English. Transcripts were analysed using grounded theory, inductive coding techniques23 and NVivo V.11 (QSR International, 2015) software, to allow for themes to organically arise. Coded data were presented visually and used as a basis for discussion and analysis in sessions with CBRs, who provided crucial cultural and contextual insights. Themes identified during interviews and focus groups were also used as a basis for a series of in-depth interviews conducted with CBRs, to add further texture and validation. An additional layer of analysis was applied to interview data generated from patients specifically being asked how diabetes affects eye health. Based on the clinical information required for informed decision-making regarding prevention and treatment of diabetic eye disease,24 these particular data were also grouped into three knowledge categories (limited, some, good).
Results
Population demographics outlined in table 1 have been rounded to protect anonymity of study sites. Sampled communities (table 1) each had a sizeable Indigenous population, an ACCHS and outreach eye care services. They varied by degree of remoteness and geographic access to health services. Participant samples are outlined in table 2. Patients were between 40 and 89 years of age with an equal distribution between males and females. Clinicians were employed in a number of primary care roles, including primary healthcare workers, eye health coordinators, nurses, general practitioners, diabetes educators and clinic managers.
Community remoteness (Australian Government Department of Health, ASGC-Remoteness Area rating) and demographics, Australian Bureau of Statistics (ABS) 2011 Census data
Interview and focus group discussion (FGD) samples
Effective communication (or its absence) was identified as a key determinant of eye health outcomes, and is explored through three themes: access to health knowledge, cultural perceptions of health, illness and prevention, and trust in clinicians and health services. Within each theme, factors that impede positive eye health outcomes are discussed, as well as strength-based strategies developed through the research process that were presented by CBRs back to ACCHSs with the aim to address diabetic eye care barriers.
Communication and access to health information
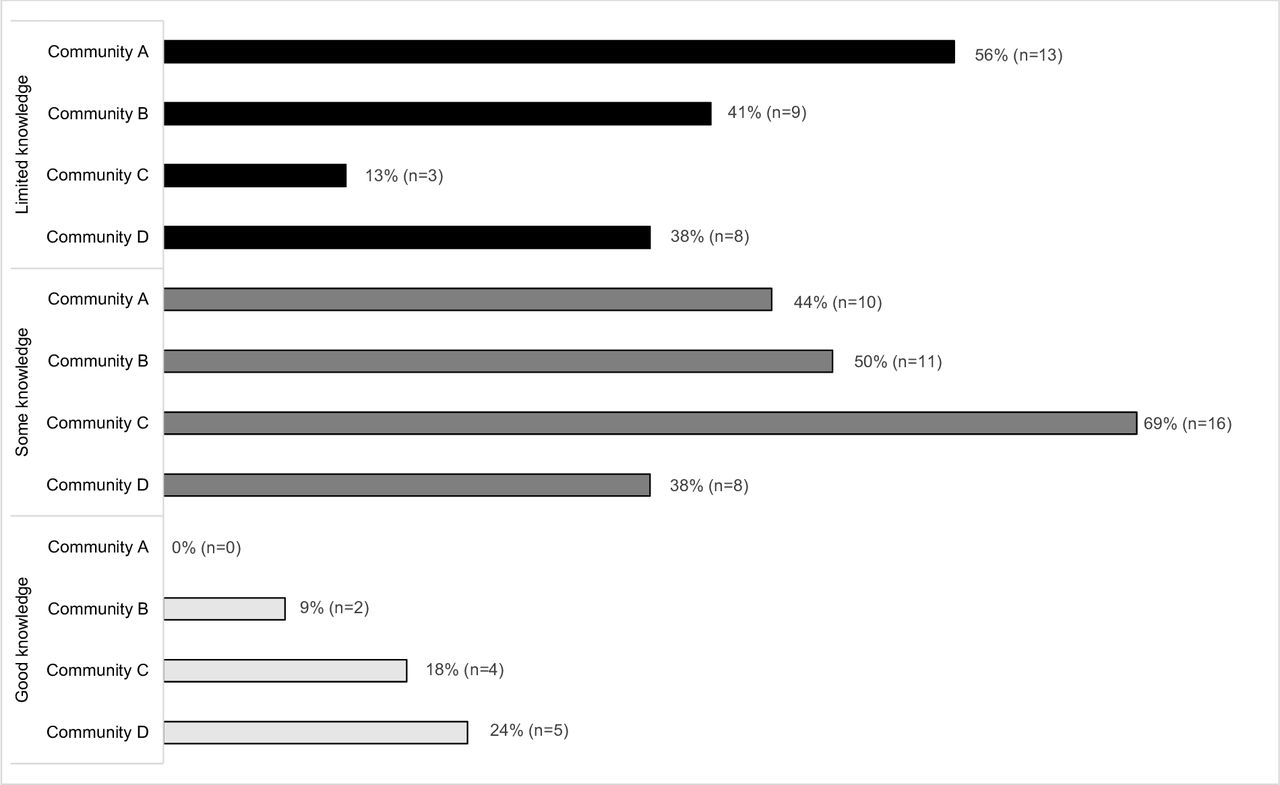
Table 3 shows the results of the analysis applied to a specific subset of interview data investigating patient knowledge of diabetic eye disease. Patient knowledge was grouped into three categories: limited knowledge, some knowledge and good knowledge. Figure 1 shows the number of patients in each knowledge category disaggregated further by community. Over one-third of all patients interviewed (n=89) either did not know diabetes could have an effect on eye health (19%) or were unsure how it could do so (18%), limiting the space whereby informed decisions around prevention and treatment can be made. ‘Good knowledge’ was associated with communities C and D in which English predominated.

{kind=link}
Knowledge and perceptions of how diabetes affects eye health (% of total sample of Indigenous patients)
Diabetes can change your eyesight. It’s important to get checked in case there is blood vessels behind the eye that have bursted because diabetes causes blindness. (Male patient, Interview, Community C)
From what I understand you can get bleeding behind the eyes and pressures and everything. You got to have the right pressures and they check all that for me when I go to make sure everything's right. (Female patient, Interview, Community D)
Patients with ‘limited knowledge’ of diabetic eye care were for the most part located in communities A and B where Indigenous languages are predominantly spoken (figure 1).
No I don't think diabetes affects the eyes. There's no other reasons why I should go back [for an eye check] again now, because I've got what I want [cataract surgery] and I'm happy with that. (Male patient, Interview, Community A)
Well I’m a diabetic but I don’t think it affects my eyes. (Male patient, Interview, Community B)
In the NT, 60% of Indigenous Australians speak an Indigenous language at home.25 Of these Indigenous language speakers, the highest proportion (32%) reside in the Katherine Region where communities A and B are located.26 Conversely, less than 1% of Indigenous Australians in NSW speak an Indigenous language at home.25
The in-depth thematic analysis of the overall data set revealed sociocultural determinants and influences, which gave further texture to limited patient knowledge of diabetic eye care identified in interviews. Language was reported as a key barrier to effective face-to-face communication between patients and clinicians, and to understanding and accessing meaningful health information. In focus groups, patients identified the significance of communication and language barriers, in addition to a lack of Indigenous language interpreters.
The doctors come up sometimes and they do not use our words, they use the medical words and we don’t understand. (Female patient, Focus group, Community A)
Interpreters should be there, [the hospital] got to use them all the time. That goes for young people that don’t read and write and don't understand English. And same with our old people, you know? They need interpreters. (Female patient, Focus group, Community A)
People don’t understand English. The hardest is medicine language. We need interpreters. (Female patient, Community B)
Not knowing English and White people that’s the problem for us Aboriginal people aye? It doesn’t feel good for us Aboriginal people, you know. (Male patient, Focus group, Community B)
Clinicians, however, attributed difficulties in understanding clinical information not to linguistic misunderstandings, but to a lack of patient interest, engagement and prioritisation of health.
C1: I really don’t think language is a barrier, that’s the main point.
C3: I’ve found that [language] is not a barrier when they are wanting us to understand and follow through with something that is important to them. It just doesn’t seem to be a priority in their thinking or their planning in their daily behavior. (Clinicians, Focus group, Community B)
An Indigenous health worker outlined the importance of using visual materials, and practical teaching and learning principles to give patients access to biomedical information. Yet, few systemic initiatives, including regular use of interpreters, were in place at the time of data collection in 2016.
It’s not just about being on medication it’s about everything else. Some patients think that when they get blurry vision that they need glasses, it isn’t associated with diabetes. Looking at the social determinants of health is not incorporated in the training people do to work in chronic disease—there is a strong focus on the biological side, lifestyle and genetic factors. Tell me what to do I won’t do it, show me what to do and I’ll be able to do it. The show and tell factor is powerful, showing them images and telling them what’s happening and how that links to real life outcomes. (Indigenous health worker, Community A)
While differences in language were an issue in communities A and B, a broader theme reflecting poor communication between patients and clinicians was apparent across all study sites. In communities C and D, communication barriers were linked to limited biomedical/scientific literacy,27 and ability to understand healthcare terms among patients. Where clinicians had assumed patients had a degree of scientific literacy, a breakdown in communication occurred, which in some cases resulted in missed opportunities to prevent and treat eye disease. One patient described that she had only understood her diagnosis of diabetic retinopathy after being shown a retinal image of her eye.
A lot of our people have got no idea what they’re [clinicians] talking about. Even me when I first got diabetes, I had no idea what they were talking about. And finally when they showed me I saw it. ‘All the white stuff is bleeding at the back of your eyes’ they said. Only after going through that I wished I had looked after my diabetes more because in the end I will probably go blind. (Female patient, Focus group, Community D)
In some instances poor communication, and exclusion from decision-making processes, led patients to refuse cataract surgery, despite moderate to severe vision impairment.
No I didn't like the idea of it [cataract surgery]. I’m frightened of losing my eyesight. They [ophthalmologist] didn’t tell me about what was going on. They more had a yarn [talk] amongst themselves to talk about the thing at the back of my eye. (Male patient, Interview, Community D)
This patient voiced that had he received a ‘better explanation’ he would have considered undergoing cataract surgery.
At the time of data collection there were no Indigenous language initiatives promoting understanding of diabetic eye disease in communities A and B. Drawing on patient and clinician perspectives several strategies were developed in collaboration with CBRs to address identified barriers that hindered access to health information, including both ‘upstream’ (policy/health systems/providers) and ‘downstream’ (patient knowledge/education/behaviour) strategies. Upstream strategies proposed enhanced resourcing of the NT Aboriginal interpreter service and workforce; and supporting locally available services in the region such as Indigenous language centres, to run Indigenous language training sessions with clinicians working in language-speaking communities. Downstream strategies proposed training and supporting Aboriginal Health Workers (AHWs) to use readily available retinal cameras to provide visual and real-time eye health information to Indigenous patients with diabetes.
I find the camera an important educational tool. If you can show them an image of their eyes now and then an image of what could happen if their eyes worsen and say to them if you don't look after your eyes they seem quite interested. (Indigenous health worker, Interview, Community A)
Using retinal camera images, and deidentified themes from interviews and focus groups, CBRs suggested developing a diabetic eye health ‘story’ that would involve bridging scientific and cultural understandings of diabetic eye disease. Patients highlighted the importance of getting elders involved, as well as training young people as ‘apprentices’ so they may learn and pass down health information. CBRs suggested the diabetic eye health story could be developed and delivered in the context of Indigenous cultural camps, allowing people to reconnect with ancestral lands, culture, language and traditional foods.
Cultural perceptions of health, illness and prevention
Cultural perceptions of health, illness and prevention influenced patient decision-making, particularly in community B where a strong belief in the materialisation of illness through metaphysical sorcery shapes patient decision-making.
A mulungwa is a person who does sorcery and can make people sick. If people make trouble they sneak up on their house and curse them. They can make your whole body sick. (CBR, Community B)
For black fella side [Indigenous culture], every time you’re sick people don't know if something has been done to them. Black fella way, sorcery or whatever you know, makes them sick. (Male patient, Focus group, Community B)
This suggests perceived sorcery may be a reason for not seeking early care in community B. Such beliefs have implications for the prevention and early presymptomatic detection of diabetic retinopathy.
They wait until they really sick. That happens [to] a lot of people. They end up in hospital, maybe family take them. That's where they find out what's really happening. (Male patient, Focus group, Community B)
However, patients readily understood the aetiology of diabetes as a Western disease associated with the introduction of Western foods and best treated using Western medicines. Yet poor access to health-related information reduced the opportunity to prevent diabetic morbidity. Some patients linked the prevalence of chronic disease to the ongoing process of colonisation, and dispossession or exclusion from ways of understanding it.
How are we going to know? People just eat whatever. Now it’s already spread all over here and the Torres Strait. We didn’t know anything. My parents they never had sickness like that. Then we say ‘Now it’s too late. We can’t read. We don’t like White people.’ (Female patient, Focus group, Community A)
Even if you drink alcohol the same, a lot of sugar! Aye? Coke, anything. Anything like that is White people’s poison. They don't tell you that you drinking poison you know. They put it in the shop there, they don't tell you, big one sugar. (Male patient, Focus group, Community B)
Non-Indigenous clinicians exhibited frustrations communicating biomedical concepts to patients. While some suggested the need to take an approach that considers cultural and historical perceptions, others associated access to health information with individual ability.
It’s their psyche, their traditional and historical beliefs, that’s why I think the approach has to come from that side rather than from us pushing a more Westernized approach. (Clinician, Focus group, Community B)
You have to give [health information] in a language that is understood, and for each person’s ability to be able to understand…that’s a big barrier. (Clinician, Focus group, Community B)
Patient experiences reflected a lack of cultural safety, highlighting the need for non-Indigenous clinicians to be supported in developing their cultural literacy and responsivity skills, and cultural humility more generally. CBRs proposed that a disjuncture in cultural and clinical understandings of diabetic eye disease may be prevented with the introduction of specific Indigenous cultural brokerage roles; that aim to bridge cultural and language gaps, through a combination of interpreting, clinical appointment coordination assistance and family/community engagement. A non-clinical role such as this would support, rather than replicate the work performed by Indigenous health workers or eye health coordinators who are often overburdened by clinical and administrative responsibilities, limiting their capacity to provide cultural brokerage.28
Trust and distrust
We defined patient trust as confidence in a clinician’s competence including social and communication skills, technical knowledge, honesty, confidentiality and empathy.29 Overall, patients had a low level of confidence in the competence of clinicians (particularly general practitioners and ophthalmologists) to provide them with the care and treatment needed to achieve positive clinical outcomes. Such perceptions resulted in avoidance of primary and tertiary health services. A common association with patient distrust was perceived fear of losing an eye or vision during cataract surgery.
People want to go down there [to the ACCHS] but they’re scared, especially old people. Everyone there, you feel uncomfortable around White people you know? (Female patient, Focus group, Community B)
You might never see again. Taking your old eye out and putting in a glass one. (Female patient, Interview, Community C)
I don't know why they can't tell us, it’s like you’re a guinea pig or something! If you have an operation you go blind, we can't believe that doctor mob. Me, I don't believe all doctors. (Male patient, Interview, Community B)
Other negative clinical outcomes shaped by distrust of clinicians and health services included patient compliance with prescribed medication for type II diabetes such as metformin. This discussion, within a community-based focus group, is illustrative of their concerns.
P2: Each doctor and nurse they change your tablets. Never know if it’s gonna fix you or bugger you or slow you up.
P1: They’ve got money, they’ve got investments in pharmaceuticals, that’s why they must prescribe you a lot of drugs.
Group: Agrees. (Male patients, Focus group, Community D)
Conversely, trust was associated with interpersonal communication and connections, emphasising the need to be understood and treated with empathy. This was widely reported in relationships with Indigenous health workers but was reported as rare with non-Indigenous clinicians.
It doesn’t always have to be an interpreter, just someone who can relate. Because it’s really important that we can get that message across to our client and vice versa. We certainly can—having the right people on the clinic days really takes that fear away. [Patient’s feel] someone’s there with me, you know, I feel really good. (Indigenous health worker, Interview, Community A)
To address issues of distrust, we identified that rapport between clinicians and patients must be structurally enabled and supported. The majority of patients across all communities voiced the importance of having family involved in their care, particularly when needing to travel outside of their community to attend hospital.
If you have someone there saying come on I’ll help you that may make it easier. You need to have it done…Family members too, help you open up a bit more. (Male patient, Focus group, Community C)
To improve trust and reduce fear, particularly around cataract surgery, patients from community B suggested that a representative from the ACCHS meet with their family members prior to travelling to town centres for secondary and tertiary care.
They [old people] can’t understand by themselves, we got to have family there to try and help. You need to be checked up. You got to go to the clinic, why can’t you? Maybe that old lady turns around and says ‘No I’m alright, I know what I’m doing!’ But we family trying to tell you about your health! (Female patient, Community B)
Patients, clinicians and CBRs proposed the need for more Indigenous liaison officers to increase cultural safety and trust in hospital settings. Indigenous liaison officers provide advocacy, and non-clinical support within acute care health settings, such as hospitals and multipurpose (mainstream) services.
You know how shy Aboriginal people are mate…the old people, they should have someone there like an Aboriginal liaison officer with medical knowledge to answer those questions for people who don’t understand. (Male patient, Community D)
Discussion
There is no pan-Indigenous understanding of health and illness.30 However, some commonalities between approaches include a collective perspective, and recognition that individual well-being is contingent on social, spiritual and collective well-being, and is often linked to social obligations to community and land.31 In comparison, Western biomedical understandings of health and illness place emphasis on identifying and treating standard disease entities within individual bodies, and tend to individualise the problem of poor health,32 despite widespread recognition that the social (and structural) determinants of health shape disease causation more than individual agency. The epistemological differences between these systems both directly and indirectly contribute to persisting poor eye health outcomes for Indigenous Australians.13
Previous studies have reported sociocultural and linguistic barriers result in potential misdiagnosis,33 heightened patient fear,34 limited clinic attendance and difficulties in managing treatment.35 The perspectives of Indigenous participants in our study revealed the wider societal inequities and racism that underpin current eye health disparities between Indigenous and non-Indigenous Australians with diabetes. Poor access to biomedical health information, cultural marginalisation and distrust are all linked to the ongoing disjuncture in communication between Indigenous patients and non-Indigenous clinicians.36 This disjuncture is reflective of a deeper and repressive history related to the denial of Indigenous language rights and cultural sovereignty, and the ongoing fight for equality, justice and recognition in the context of dominant Western neoliberal values and systems that normalise racism and assimilation. Understanding the structural determinants that produce miscommunication and distrust assists in establishing how these might translate into poorer clinical outcomes, and more importantly how they might be addressed.
Health literacy describes the capacity of an individual or group to understand and navigate concepts regarding health, well-being and access to healthcare services; it is multidimensional, particularly in cross-cultural contexts where the world view and language of the patient differs from that of the health system.37 The association between ‘limited knowledge’ as defined in table 3, and communities A and B where Indigenous languages predominate, suggests little is being done to create a shared understanding between clinicians and patients. English language proficiency was clearly a barrier in community B, yet this was poorly acknowledged by clinicians, and often deflected as an issue of individual responsibility. None of the (non-Indigenous) clinicians working in community B spoke the primary Indigenous language in the community. Furthermore, the assumption that patients hold a degree of scientific literacy in the context of limited English literacy results in exclusion from decision-making processes, and in some cases from accessing healthcare altogether, leading to late detection of eye diseases, and refusal of or non-attendance to treatment and surgery. Access to clinical information influences the way patients determine whether or not to seek care and creates the space in which informed health decisions are made. From a structural perspective, our study reveals a need for better interpreter services, particularly in Indigenous language-speaking communities. Minimal resources have been allocated to improving access to Indigenous interpreter services, inhibiting regular use.38 From a grassroots perspective, health promotion focused on knowledge gaps with respect to diabetic retinopathy is needed, and may be adapted from existing resources.39 Participants indicated health promotion resources should be delivered in non-text-based form, incorporating Indigenous ways of being, knowing and doing as reported in other settings.40 41 This may be facilitated through existing Indigenous cultural camps supporting the notion that connection to ‘country’ (ancestral lands) is inherently linked with well-being,42 while creating a culturally safe space to share experiences and information around diabetes, treatment and surgery. Such approaches can contribute to closing the communication gap36 in Indigenous eye health.
Evidence from our study suggests that exclusion from biomedical health information, combined with cultural perceptions that delay care-seeking behaviour, may perpetuate eye disease among patients with diabetes. This presents a complex conundrum of Indigenous ‘culture’ as potentially health hindering, due to its marginal positioning in relation to the dominant biomedical and neoliberal cultural norms of the health system at large, resulting in exclusion from health information, care and treatments.43 Previous studies44 45 have outlined how cultural understandings of diabetes among Indigenous Australians, particularly in the context of exclusion from biomedical health information, can have negative implications for prevention and treatment. Vass et al37 outline that while language and world view differences could be considered barriers to improving health literacy, effective methodologies for improving health literacy are in fact based in a better understanding of these two key elements. Part of this is acknowledging that differentiation from norms dominant in Australian society, enacted through the right to speak Indigenous languages and live by divergent cultural values and laws (a determinant of strength and well-being), to differing degrees can compromise access to the Australian public health system (a determinant of ocular and diabetic morbidity).
Distrust of biomedical health systems among Indigenous Australians is well documented, and associated with evidence that links racist policies, such as those that produced the Stolen Generations, to hospitals and health services.46 47 At an interpersonal level, miscommunication or lack of communication regarding treatment, symptoms or results may lead patients to perceive clinicians as intentionally misleading48 or untrustworthy, hiding medical information from them,49 which in turn prevents them or their families from making informed decisions, and subsequently disallowing cultural laws and processes to be undertaken.50 These perceptions reinforce the crucial need to resource and enable the Indigenous health workforce as providers of clinical care, and of cultural support and brokerage.51 In addition, structural factors, such as the transient nature of remote area health staff and specialists,52 53 may have further inhibited trust building.
A genuine acknowledgement of the need to decolonise health systems is required at the macro (policy, policymakers), meso (health systems, health governance), and micro (clinicians, health service staff) levels, in order to create a basis for transformative structural change. The National Aboriginal and Torres Strait Islander Health Plan (2013) identified working towards achieving a ‘culturally respectful and non-discriminatory health system’ by 2023, as a key priority.54 In a context where English language and Western biomedical concepts dominate, working towards a non-discriminatory health system requires creating a shared space for understanding health and well-being. Cultural responsiveness is key to decolonising health spaces, and highlights the need for an applied recognition of the longer term and deeper historical, political and sociocultural influences on Indigenous health and well-being.14 55 56 Rather than solely learning about Indigenous cultures, cultural responsivity training uses the clinician’s own culture as a resource; highlighting the way dominant cultural values, beliefs and norms shape their delivery of care to Indigenous patients.14
At present, cultural responsivity training is not a core component of the Australian medical and nursing undergraduate syllabi, a factor that stunts improved cross-cultural communication and equity in health. A culturally responsive and non-discriminatory health system must involve trust building. This study highlights that trust building is rooted in strong communication, respect and empathy regarding historical and cultural realities, and must build on the improved engagement of Indigenous Australians as leaders, clinicians, cultural brokers and interpreters in clinical spaces.
Conclusion
Evidence from our study highlighted how culture, access to biomedical information and trust impact communication in the delivery of diabetic eye healthcare, as well as the need to create a shared dialogue to overcome disparate understandings of health and illness. Barriers to shared understandings, knowledge and health literacy between clinicians and Indigenous patients perpetuate poor diabetic eye health outcomes. Our findings identified strategies for the prevention and treatment of diabetic eye disease; through identifying the need to create a shared understanding of illness, treatment and well-being. Health inequities will not be adequately addressed until the structural determinants of ill health receive serious and sustained attention. Enabling access to culturally safe and responsive services, and support roles such as cultural brokers and interpreters, will contribute towards closing the communication gap and supporting equitable eye health outcomes.
Acknowledgments
We acknowledge Dr Anthea Burnett and CBRs Francis Hayes, Aaron Joshua, Wendy Fernando, Kelvin Brown, Brian Donnelley and Bridgette Jerrard for their contribution to the collection and analysis of data presented in this paper. We also acknowledge the support and contribution of the ACCHSs in each of the study sites.
References
Footnotes
Handling editor Seye Abimbola
Correction notice This article has been corrected since it was published. The article type has been updated.
Funding This study was funded by the Australian Government Department of Industry's Cooperative Research Centre initiative under the Vision CRC.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Due to Human Research Ethics Committee and intellectual property requirements data is not available.