Article Text

Abstract
Introduction The 2018 Astana Declaration reaffirmed global commitment to primary healthcare (PHC) as a core strategy to achieve universal health coverage. To meet this potential, PHC in low-income and middle-income countries (LMIC) needs to be strengthened, but research is lacking and fragmented. We conducted a scoping review of the recent literature to assess the state of research on PHC in LMIC and understand where future research is most needed.
Methods Guided by the Primary Healthcare Performance Initiative (PHCPI) conceptual framework, we conducted searches of the peer-reviewed literature on PHC in LMIC published between 2010 (the publication year of the last major review of PHC in LMIC) and 2017. We also conducted country-specific searches to understand performance trajectories in 14 high-performing countries identified in the previous review. Evidence highlights and gaps for each topic area of the PHCPI framework were extracted and summarised.
Results We retrieved 5219 articles, 207 of which met final inclusion criteria. Many PHC system inputs such as payment and workforce are well-studied. A number of emerging service delivery innovations have early evidence of success but lack evidence for how to scale more broadly. Community-based PHC systems with supportive governmental policies and financing structures (public and private) consistently promote better outcomes and equity. Among the 14 highlighted countries, most maintained or improved progress in the scope of services, quality, access and financial coverage of PHC during the review time period.
Conclusion Our findings revealed a heterogeneous focus of recent literature, with ample evidence for effective PHC policies, payment and other system inputs. More variability was seen in key areas of service delivery, underscoring a need for greater emphasis on implementation science and intervention testing. Future evaluations are needed on PHC system capacities and orientation toward social accountability, innovation, management and population health in order to achieve the promise of PHC.
- health policy
- health systems
- review
- public health
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known?
Improving primary healthcare (PHC) performance will be essential for achieving universal health coverage, but evidence about how to do so is lacking or fragmented, and there is a pressing need to prioritise research efforts, build the field of research around targeted questions and better understand how to ensure the core service delivery functions of PHC.
What are the new findings?
Some areas of PHC system performance are well-researched, such as PHC policies, health financing and health workforce, but we lack a sufficient evidence base in a wide enough range of countries about how to adapt these strategies to new contexts.
Major research gaps exist in understanding social accountability, effective information and quality management systems, fund flows and how to improve facility and district management.
Our country-specific review of 14 countries with improving systems in 2010 generally found continued progress over the last decade in the scope of services, quality of services, access for marginalised populations and progressive health financing initiatives.
What do the new findings imply?
As countries implement new PHC strategies, they should be designed with rigorous evaluation and measurement across a wider array of countries in order to share and grow knowledge and learning about translating PHC research to universal health coverage implementation.
Introduction
In recent years, primary healthcare (PHC) has re-emerged as an important strategy in both improving population health and in making healthcare systems more effective, responsive and efficient. In 2016, 193 countries adopted the Sustainable Development Goals (SDGs), making the achievement of universal health coverage (UHC) a principal goal for the global health community through 2030.1 Multiple global, national and subnational organisations recognise that strong PHC systems will be essential to achieving UHC.2–7 Additionally, the global health community has just celebrated the 40th anniversary of the Alma-Ata Declaration with the issuance of the 2018 Astana Declaration, which reconfirmed the central role of PHC to improving health and defined PHC as a triad of multisectoral policies to promote health, engaged communities to promote health and integrated clinical and public health services to deliver better primary care.8
Despite this increased focus on the centrality of PHC, the performance of PHC systems globally, and in particular in low-income and middle-income countries (LMIC), is poor. Significant improvements in PHC systems and service delivery are needed in order to meet the SDGs and achieve UHC. Efforts to do so, however, are hampered by the state of PHC research in LMIC which is currently fragmented, underfunded and under-prioritised. While a plethora of research exists on different facets of PHC globally, there is a need to prioritise disparate research efforts, build the field of research around targeted questions linked to the provision of equitable care and better understand how to ensure the core service delivery functions of PHC that are linked to desired outcomes.
Several notable publications over the last decade have attempted to describe the state of PHC knowledge, and, more specifically, to identify interventions that have successfully improved outcomes and identified emerging or remaining knowledge gaps. However, these reviews did not employ a systematic approach, described middle- and high-income countries rather than LMIC or focused narrowly on the functions of PHC.9 10 Thus, just as researchers, policymakers and other stakeholders in LMIC are re-focusing improvement efforts on PHC, there is an urgent need to better understand the state of recent research on PHC in LMIC, and to map remaining gaps in that research.
To meet this need, we conducted a scoping review of the recent literature to assess the state of global knowledge on PHC in LMIC and understand where further PHC systems research efforts are most needed. This scoping review was completed as the foundational document for a priority setting exercise conducted in July 2017 (described more fully elsewhere in this online supplementary files).11 The goal of that exercise was to identify specific content areas for which more in-depth research into measurement and improvement strategies is likely to lead to significant impact on PHC service delivery, outputs and outcomes. The results of the priority-setting exercise formed the basis for a new PHC research consortium in LMIC.11
Methods
We conducted the scoping review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews guidance.12 A scoping review was deemed to be appropriate given that the purpose of this review was to explore broadly the evidence on primary healthcare research in LMIC, a topic that is diverse, wide-ranging and methodologically complex. A further justification for this approach was that PHC has a wide and heterogeneous evidence base, and a paucity of existing summative systematic reviews. Additionally, the review sought to assess the extent, range and nature of the evidence, elements that are well suited to exploration using a scoping review methodology.12
Scoping the review
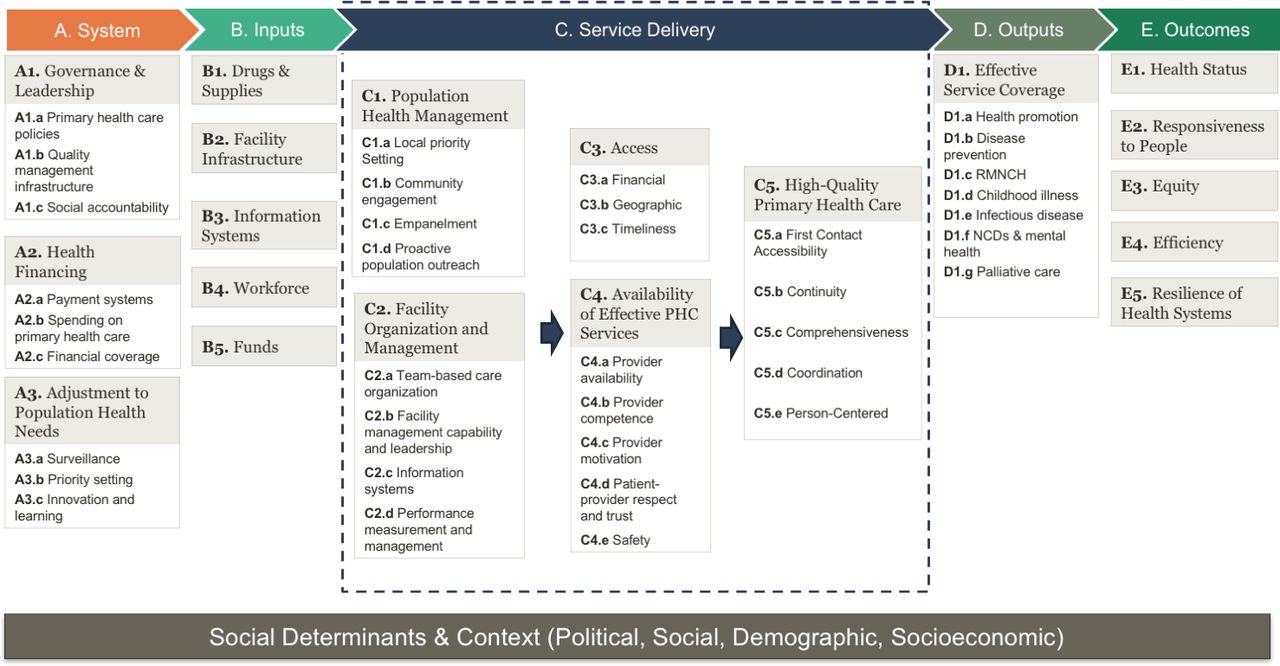
We anchored our review in the conceptual framework of the Primary Healthcare Performance Initiative (PHCPI) -- a collaboration between the World Health Organization (WHO), the World Bank Group and the Bill & Melinda Gates Foundation, in partnership with Ariadne Labs and Results for Development Institute.7 13 14 PHCPI aims to catalyse improvement in PHC in LMIC through better measurement and evidence-based improvement strategies. The PHCPI conceptual framework (figure 1) describes the necessary components of a high-functioning PHC system.14 As defined by the WHO, PHC includes three components: primary care services and integrated health services, empowered people and communities and multisectoral policy and action.15 PHCPI focuses on PHC overall, with a particular focus on integrated health service delivery and people-centred care.13
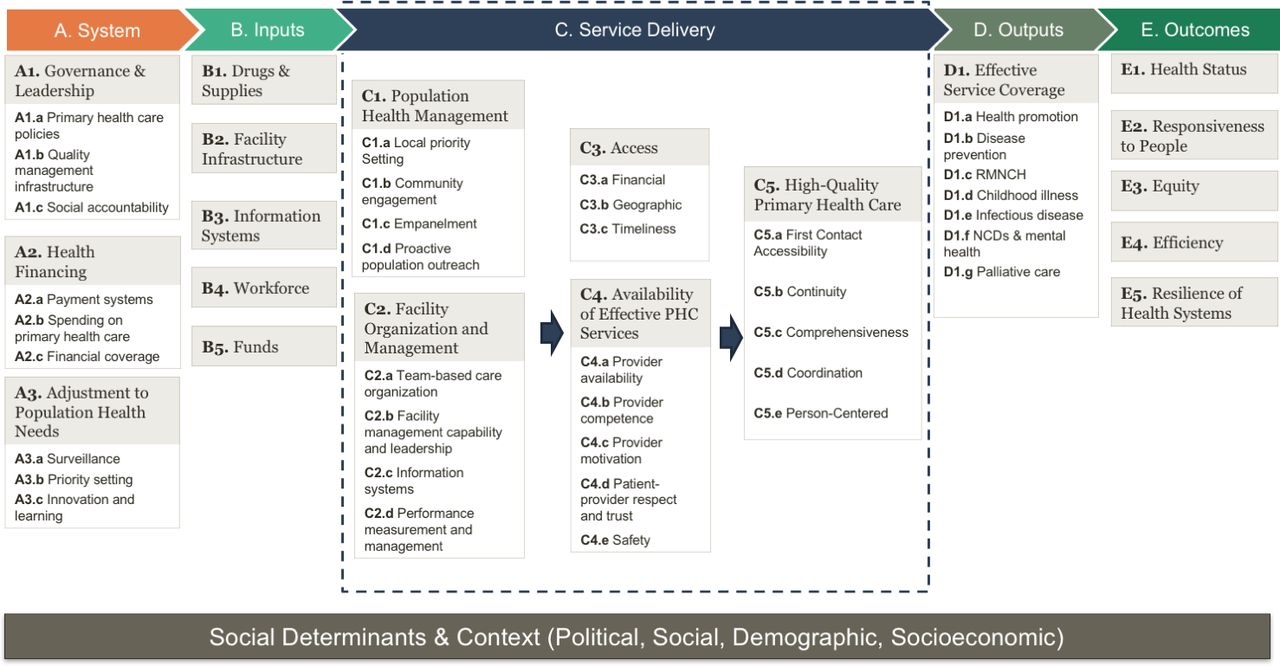
PHCPI conceptual framework. PHCPI, Primary Healthcare Performance Initiative.
PHCPI defines a PHC system as the totality of the system, inputs and service delivery components that contribute to high-quality primary care services and achieve the four functions of PHC described by Barbara Starfield - first contact accessibility, continuity, comprehensiveness and coordination - as well as person-centredness.14 16 This conception of PHC systems guided our search strategy.
For this review, we focused specifically on the 13 topics within the system, inputs and service delivery domains of the framework, recognising that by design, improvements in these areas should lead to improvements in outputs and outcomes and that the levers for PHC improvement are generally within these domains. Definitions for each of these specific topic areas are included elsewhere.17
Beginning with a search guided by the PHCPI conceptual framework, we then conducted a country-specific review of 14 countries identified as high or rapidly improving performers in the last systematic summary of PHC literature, so as to more deeply examine the global literature in the context of these countries.2 We therefore limited our research on these countries to the past 7 years, since the 2010 summary was published, so as to provide updated summaries of these countries’ literature and gain insights into the current state of their PHC systems and trajectories since that publication (full results of this search are presented in online supplementary file 3).
Supplemental material
Information sources
Our scoping review process included four main components. The first was a search of the peer-reviewed literature in PubMed. We limited the date range of included studies to 1 January, 2010 to 20 March, 2017. The former date was selected such that our review could build off of the last review of PHC initiatives in LMIC, as discussed above.2 The latter date was selected to align with a priority setting meeting that occurred in July 2017, for which the extended results of this review (presented in online supplementary file 3) were a foundational resource.11
This first component of the systematic review included two separate searches. We started with a generic search for all review publications in PubMed that included the term ‘primary care’ OR ‘primary healthcare’ AND a set of search terms used to identify all articles from a low-income or middle-income country (online supplementary file 1). Next, to focus on the topics of interest from the PHCPI conceptual framework, we conducted a search of review articles using the terms ‘primary care’ OR ‘primary healthcare’, AND the search terms from above to specify articles about LMIC, AND a set of key terms from the targeted areas of the PHCPI conceptual framework. These latter terms are also included in the online online supplementary file 1.
Supplemental material
The second main component of our scoping review was a search to explore primary healthcare performance in 14 countries profiled in Kruk et al 2010.2 As described above, this was the most recent review of the state of primary healthcare in LMIC. Among other data, Kruk et al described 14 countries that had implemented primary healthcare initiatives at a large scale or were fragile states that had made substantial progress in promoting primary healthcare as the first point of contact. These countries included: Costa Rica; Cuba; Brazil; Bolivia; Mexico; Niger; Ghana; The Gambia; Thailand; Sri Lanka; Kerala, India; Iran; Afghanistan and Liberia.2 Although this list is far from representative of all progress or innovation in PHC in LMIC, it has considerable overlap with countries profiled in the World Health Report 2008, Shi et al’s9 2012 examination of primary care functions as assessed using the primary care assessment tool, and countries profiled by PHCPI.18 19 This component of the review was conducted using search terms of ‘primary care’ or ‘primary healthcare’ in addition to each of the country names.
For the third main component of our search, we reviewed all articles labelled as ‘low- or middle-income countries’ in the PHC evidence portal, part of the McMaster University Health Systems Evidence portal for collecting and making a standardised rating of systematic reviews of health interventions.20 21
Finally, in the fourth component of our review, we conducted a search of all publications in PubMed from 1 January, 2010 to 31 May, 2017, by the 17 individuals who had confirmed participation at the Primary Healthcare Measurement and Implementation Research Consortium Priority Setting Meeting.11
Selection of data sources
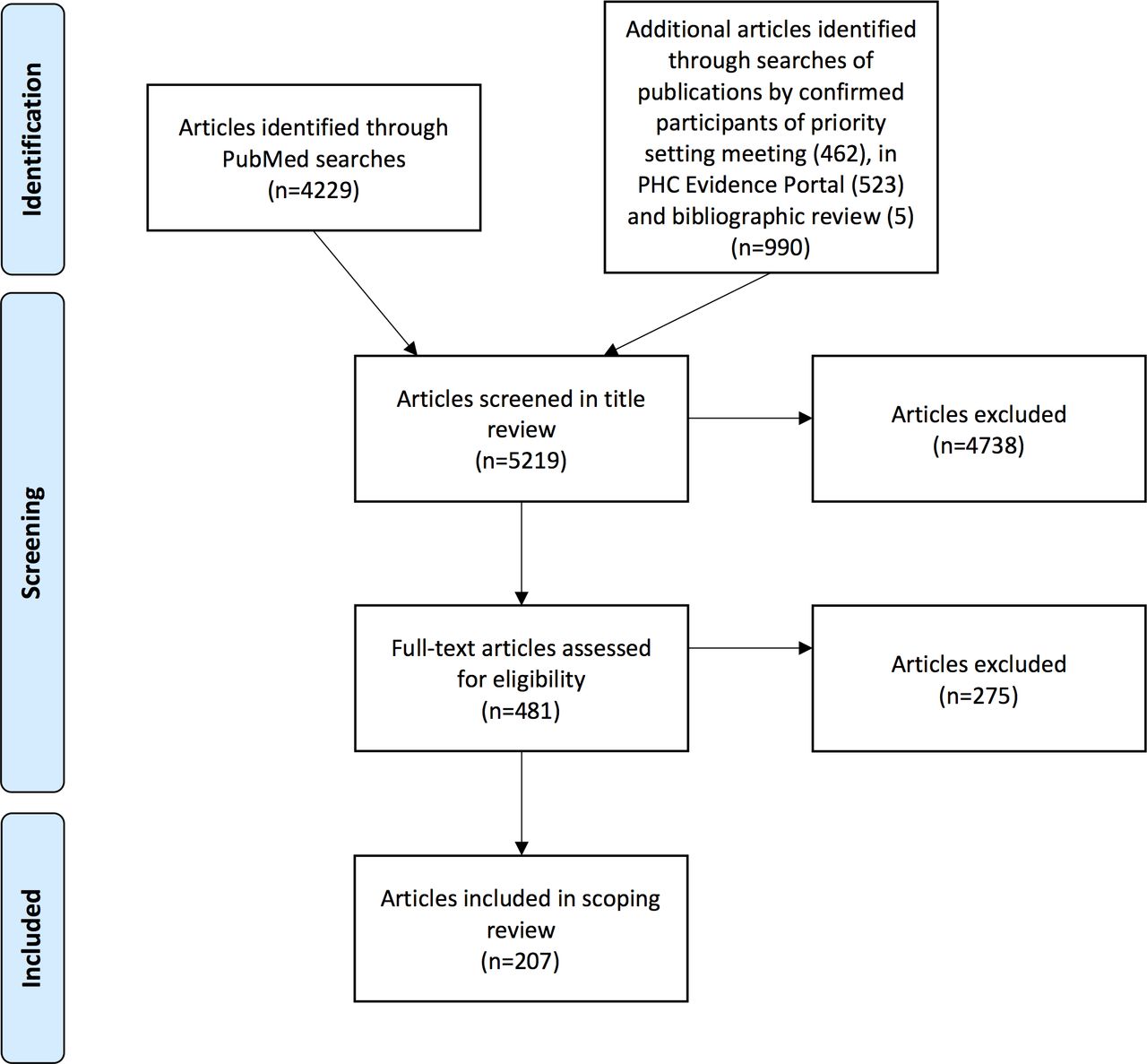
To select articles for inclusion from these searches, at least one author reviewed titles using the inclusion criteria that the article focused on the primary care setting in a low-income or middle-income country, addressed a topic relevant to the PHCPI framework, and that the publication was available in English. A subsequent full-text review was conducted by at least one author with the following criteria: (1) the article focused on primary healthcare, not on vertical, disease-specific issues; (2) the intervention or method of study was related to strengthening primary healthcare systems or functions, even if disease-specific outcomes were assessed; (3) the article concerned a large population area, not a small-scale pilot; (4) the article connected to the PHCPI framework and/or one of the countries of focus; (5) the article was a research or review article that included qualitative or quantitative data or described a new methodology and (6) the article was available in English. For the articles from the PHC evidence portal, they needed to also meet the criteria that they included evidence from at least three LMICs to ensure that the focus was primarily on LMIC as opposed to high-income countries. During the full-text review, additional articles were included through a bibliographic search (figure 2).
{kind=link}
{kind=link}
Summary of search, selection and inclusion process.
Data charting and analysis
To extract the content from the full set of identified articles, every article was tagged for its relevance to the PHCPI conceptual framework (figure 1) using Mendeley V.1.19 (Elsevier, Amsterdam, Netherlands). Articles could include multiple tags, and for each tag, one author extracted and summarised the relevant information. Finally, authors reviewed all extractions for each topic and generated evidence highlights and gaps. The full list of included articles is presented in the online supplementary file 2, and full summaries are presented in the online supplementary file 3.
Supplemental material
Patient and public involvement
Patients were not involved in this study.
Results
We retrieved a total of 5219 articles using the search strategy, of which 481 were accessed in full text, and 207 met the inclusion criteria and were included in the scoping review (figure 1). The list of all included studies are included in the online supplementary file 2.
Publication descriptions
Of the included articles, 70% were published between 2014 to 2017, with more than one-quarter of the articles published in 2016 alone (table 1). Despite parts of our search strategy focusing specifically on review articles, the majority of identified articles were primary research (61.4%), and 66.9% of these analysed quantitative data. Systematic reviews comprised 17.4% of the total identified articles.
Selected characteristics of reviewed publications
Findings
Table 2 presents our synthesised findings from this scoping review. We found that a number of areas of PHC system performance are well-studied. The four topics with the highest volume of research were workforce, payment systems, provider competence and PHC policies, together accounting for two-thirds of the total included studies (table 2). Effective, integrated and comprehensive PHC policy and governance systems appear to be associated with better long-term system performance.22–26 Good evidence exist that insurance programmes can increase access to PHC by decreasing financial barriers and preventing catastrophic losses; whereas, user fees act as an additional barrier to access.26–30 More public spending on PHC appears to be associated with more equitable outcomes. In addition, fee for service (FFS) payment systems alone do not appear to be associated with better outcomes. Capitation appears to be show modest improved outcomes, as does pay for performance on top of FFS (though the benefits are often transient).
Synthesised key findings and gaps; red = low evidence (0 to 6 articles), yellow = moderate evidence (7 to 13 articles), green = high evidence (14+ articles)
Financial limitations are not the only access barriers to care access. We found evidence that gaps in medication and other supplies not only impede care delivery but also decrease access as patients may avoid or bypass facilities that lack necessary resources, and quality of care.31–33 However, even in areas with a high volume of evidence there are remaining research questions or little information on implementation, social accountability mechanisms for PHC, adjustment to population health needs or adaptation to other contexts.
The evidence for the core PHC functions (first-contact access, continuity, comprehensiveness, coordination and person-centredness) was moderate-to-strong in LMIC. Comprehensiveness, access and person-centredness in particular had strong evidence of linkages to important improved outcomes. Coordination and continuity were less-studied, but still associated with moderate improvements. Related domains in trust and provider competence clearly showed both the association with improved outcomes when both are high, as well as even stronger relationships to poor outcomes when both are low.
There were a number of topics that had a moderate evidence base that was often concentrated on a few specific service delivery topics or geographical areas. For instance, there is evidence that empanelment and multidisciplinary teams serve as a useful base on which to build PHC strategies and to attend to population health concerns in limited countries.24 34–39 Management appears to play an important role in mediating or improving facility outcomes, but there is little information available on how to measure it systematically or improve it.40 Motivating providers through both explicit (ie, financial) and implicit ways appears to be important to maintaining and improving clinical outcomes. Additionally, in contexts lacking sufficient clinicians, the evidence shows that task shifting to community health workers or other health workers can provide increased patient access to care and increased coverage to effective interventions. Task shifting was shown to be most successful when supported by policies, training and proper integration of community health workers into the existing workforce.34 41–43 However, evidence is lacking on the best ways to use these strategies in various LMIC contexts, and the extent to which task shifting can work for more complex condition or in people with multiple comorbidities.
We found the least volume of evidence on funds, information systems and timeliness. For funds in particular - a topic defined as the availability, control and management of funds at the facility level - our search returned no articles.17 Very little information was available as well for how PHC systems can learn and innovate in a reliable manner, and better engage populations in their work. Much more research is also needed on patient safety in PHC settings in LMIC.
Country-specific findings
Our review of 14 countries in Kruk et al’s (2010) paper described progress in many of the reviewed countries (table 3). Of the nine countries with sufficient evidence, all had either stable or improving outcomes since 2010. Eight (57%) of the 14 countries reviewed were categorised as ‘Low’ for the quantity of the evidence, with six of those eight having three or fewer articles published during the period of review. Five of those six were ultimately categorised as an ‘Indeterminate’ trajectory given the dearth of evidence. Only three countries (21%) were qualified as ‘High’ quantity of evidence. It is notable that 33% of all country-specific articles focused on Brazil exclusively, which generates a disproportionately high amount of high-quality PHC evidence. No country previously identified had clearly worsening outcomes. The full summaries of the country update are in online supplementary file 4.
Supplemental material
Summary of the quantity of evidence and the trajectory of 14 PHC systems (2010 to 2017); red = low evidence (0 to 6 articles), yellow = moderate evidence (7 to 13 articles), green = high evidence (14+ articles)
Discussion
We conducted a scoping review of the recent literature on PHC in LMIC (2010 to 2017), based on the structure of the PHCPI conceptual framework. We profile 207 articles in this review, which reveal a heterogeneous focus of the recent literature. We found a few thoroughly researched components of PHC particularly in the areas of PHC policy, payment and workforce - including provider competence and motivation. Other key PHC components--particularly population health management, facility management and effectiveness and quality of service delivery--suffer from much smaller, less rigorous evidence bases.
From the substantial literature on PHC policies, financing, workforce, performance measurement and quality, we found that clear policies that promote more system focus and public spending on PHC are related to better outcomes and equity.22 24 44 These policies should focus on integrating care delivery with other policies that promote health at the community level. While no obviously better finance system exists for PHC, user fees are clearly detrimental to utilisation and access.29 45 Furthermore, it appears that FFS alone is not associated with improved outcomes compared with other financing mechanisms. We also found that community-based PHC systems that engage populations (in both public and private sectors), proactively track and reach out to identified population and utilise well-managed multidisciplinary teams are often successful.36 46–48 A focus on motivating providers through both extrinsic and intrinsic mechanisms leads to better, less burned out providers and possibly to better outcomes.49 50 In particular, understanding and improving hybrid payment schemes for PHC, especially among private providers, is a major priority area for further research. Achieving key PHC functions like comprehensiveness, first contact access and person-centredness leads to improved outcomes from the patient perspective. Evidence suggests that provider competence and safety across most PHC systems in LMIC is poor, and major preclinical and ongoing training plans are needed to improve both technical quality and experiential quality, especially in the areas of communication and trust.51–53
Major research gaps exist in understanding social accountability and innovation systems as they relate to PHC. More research is needed on optimising the use and deployment of effective information and quality management systems on the frontlines of PHC delivery, as well as discerning the successful and timely flow of funds to both public and private providers within a system. Better understanding of how to measure and improve management at the facility level is also critical, along with how that management can supervise and motivate multidisciplinary teams. In particular, given their centrality to PHC performance, future research may consider prioritisation of PHC policies that promote uptake of successful community-based PHC, as well as financing mechanisms that can adequately pay for them.
Most of the 14 countries and regions identified previously as rapidly improving or high performing were found to either be stable or improving, though notably evidence is limited in understanding the trajectory of over a third of these countries. Since 2010, our review shows that there has been further progress in the scope of services, quality of services, access for marginalised populations and progressive health financing initiatives. In some of the higher-performing health systems such as Brazil, Ghana, Mexico, Sri Lanka and Iran, many recent challenges mirror higher income systems (eg, chronic care provision, effective empanelment, patient satisfaction scores, epidemiological transition and ageing populations).
As more countries seek to create and improve PHC systems, they should implement interventions and policies in ways that allow for rigorous measurement. Such programme evaluation can help guide countries’ implementations, particularly if they commit to a staged rollout. Understanding what specific strategies and tradeoffs work in each country’s context to successfully implement and sustain PHC systems on a small scale first can help those countries scale up their PHC systems more effectively and efficiently. Moreover, while sharing lessons learnt between countries is a worthwhile endeavour, publishing rigorous data as well as qualitative information will allow us to draw useful conclusions about successful (and unsuccessful) strategies across multiple, varying contexts.
While some areas of PHC still lack health systems and implementation research, we found that many of the components of the PHCPI conceptual framework already have at least a moderate amount of recent evidence on fundamental questions. The renewed interest in PHC through both the Astana Declaration, multilateral efforts such as PHCPI and a realignment of donor funding away from vertical programme creates an urgent need for prioritised research around implementation, adaptation and sustainability of PHC.8 19
Limitations
With a topic as broad as PHC, conducting a comprehensive literature search is impracticable, if not impossible. Despite our best efforts, we have inevitably missed relevant evidence, particularly due to the limits of our searches (eg, PubMed, English-language). Because we were interested in PHC as systems of care, we excluded articles focusing only on vertical, disease-specific topics that often relate or intersect with PHC. However, due to the prevalence of vertical funding and reporting structures in global health--particularly in sub-Saharan Africa--those excluded articles likely contained evidence relevant to PHC systems that we were thus unable to consider. Specifically, articles on vertical maternal and child health programmes likely included relevant information that we excluded due to the focus of the articles. Our exclusion of articles about smaller pilots or localities may have caused us to miss important descriptions of local reforms. Additionally, while many elements of a health system have implications for PHC, we intentionally limited our searches by using the terms ‘primary healthcare’ or ‘primary care’, which may have led to the exclusion of literature addressing broader systemic topics such as governance, district health system oversight and insurance mechanisms that did not explicitly link to PHC. We also did not include grey literature in our search strategy due to time and scope constraints.
Although some grey literature was identified through bibliographical reviews, there is a substantial knowledge base outside of the peer-reviewed literature that was therefore not encompassed in this scoping review. Additionally, evidence from countries with complex and multilayered PHC policies and investments such as Ethiopia, Nigeria, South Africa and India is somewhat limited. Many of these large countries exist in a federal model for which regional or state-based research might have been missed. We limited our countries of focus to those that were identified in a previous review which has biased our regional representation and limited our ability to make conclusions about the geographical spread of the evidence. Finally, with such an expansive literature, sensemaking necessarily results in occasional overgeneralisations and simplifications.
Conclusion
The literature on PHC in LMIC between 2010 and 2017 contains strong evidence on some of the important aspects of PHC systems, especially issues of financing and policies, workforce and core PHC functions. It contains less evidence on other PHC-system components, including population health management, facility management, safety and improving service-delivery quality. However, even where there is evidence for successful strategies for building PHC systems (eg, empanelment, facility management), there is still a glaring lack of evidence about the best ways to adapt, implement and sustain those strategies across various contexts. With the resurgence of interest in PHC in recent years, countries have an opportunity to design their implementation and scaling up of PHC to incorporate rigorous measurement and evaluation, which will improve the quality of these PHC interventions and offer further evidence for research work. Building a prioritised research agenda off these recent findings is an important next step toward catalysing these necessary improvements within and across LMICs to address current and emerging challenges.
Acknowledgments
The authors would like to acknowledge Brooke Huskey and Emily Benotti for their assistance in article extractions as well as Etienne Langlois, Abdul Ghaffar and Atul Gawande for their critical input on the design and structure of this scoping review.
References
Footnotes
Handling editor Stephanie M Topp
Contributors AB and LRH conceptualised the paper. AB, HLR, LRH, JF and DS wrote the initial version of this report for the priority setting meeting in 2017, and AB, JF and AK adapted it to a manuscript. HW and JV provided critical revisions. All authors contributed intellectual content, edited the manuscript and approved the final version for submission.
Funding Funding for this research was provided by the Bill & Melinda Gates Foundation.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.